

Abstract
Objective
Recent years have witnessed an expansion of Internet- and mobile-phone-based interventions for health promotion, yet few studies have focused on the use of technology by individuals with mental illness. This study examined the extent to which patients at an inner-city community psychiatry clinic had access to information and communications technology (ICT) and how they used those resources.
Methods
Patients of an outpatient, inner-city community psychiatry program (N = 189) completed a survey that included questions about demographics and ICT use which were adapted from an existing local population-based health survey (community sample, N = 968). Frequencies of ICT use were assessed for the clinic sample and questions common to both the surveys completed by the clinic and community samples were compared using logistic regression.
Results
Among clinic cases, 105 (55.6%) reported owning or using a computer, 162 (85.7%) reported owning or using a mobile phone, and 112 (59.3%) reported using the Internet. Among those who used mobile phones, the majority reported using them daily; 42% of those who used the Internet reported using it several times per day. Differences in frequency of Internet use between samples were not significant, but clinic participants used the Internet more intensively to email, instant message, access health information, and use social media sites.
Conclusions
A majority of patients in this community psychiatry clinic sample use ICT. Greater access to and use of the Internet by those with mental illness has important implications for the feasibility and impact of technology-based interventions.
Keywords: Internet, mobile phones, mental disorders, ehealth, mhealth, mental illness
Technology use is now an integral part of nearly all aspects of our daily lives. Within the medical field, the use of interactive technology has the potential to improve patient care and quality of life,1–6 and there is some movement toward reimbursement being provided for technology-based treatments.7 Recently, interest in the role of technology in the management and treatment of individuals with serious mental illness has been growing. A number of studies have investigated the effect of technology-based interventions in individuals with disorders such as panic disorder, depression, and social phobia and have found them to be beneficial.8–11 Others have investigated the value of mobile interventions among those with schizophrenia and bipolar disorder with promising results.12–15 One factor that affects the ability to implement any technology-based intervention is the target population’s access to and use of technology. To date, only a small number of studies have examined access to and use of information and communication technology (ICT) in individuals with serious mental illness.12,16–18
The objective of this study was to examine the extent to which patients at an inner-city community psychiatry clinic had access to ICT and how they used those resources. Specifically, we assessed frequency of access to mobile phones, computers, and the Internet, the location of computer and Internet use, and the nature of Internet and mobile phone use among this population. To identify the extent to which mental illness may act as a barrier to computer and Internet use, we compared ICT use profiles of the participants recruited from our clinic to previously collected information on ICT use in a representative population sample who reside in the geographical area where the clinic is located.
METHODS
Samples
The clinic sample was drawn from the Johns Hopkins Hospital Community Psychiatry Program. The program serves approximately 1,200 patients, the majority of whom have a serious mental illness and reside in the East Baltimore area. Of the patients attending the program, 60% have an affective disorder (bipolar disorder types I and II, major depressive disorder) and 30% have a psychotic disorder (schizophrenia, schizoaffective disorder), while approximately 40% have a comorbid substance use disorder. Sixty percent of the clinic population is female and the mean age is 42 years. Following IRB approval, all English-speaking patients attending the program over a 4-week period in 2011 were invited to participate in the study by completing a short survey. Given the nature of the data being collected, the IRB waived the need for written consent and no incentive was offered for participation. Overall, 274 individuals from the community psychiatric clinic were invited to participate in the study, 214 of whom agreed. Of those who did not agree to participate, two reported that they did not use any form of technology, 10 reported that they did not have time to complete the survey, and 1 reported not being able to read or write. The others who did not participate did not volunteer a reason. In the surveys that were collected, no responses were checked in 6 (3%) and information on age, gender, and/or education were not provided in 19 (9%); these 25 surveys were not included in the analyses. Thus, 189 of the 214 participants (88%) did provide information on all basic demographic characteristics and comprised the clinic sample.
The community sample comprised 1,000 head-of-household participants enrolled in the Windows to Health epidemiological study. The study was conducted between January 2010 and November 2011 in a stratified random sample in neighborhoods of Baltimore by researchers at the Johns Hopkins Bloomberg School of Public Health (C. D. Furr-Holden, unpublished data). Participants in this study were recruited using a mailed flyer and invited to participate in a 15-minute interview about health and complete a follow-up contact sheet that included questions about ICT use. Total participation time was estimated to be 25 minutes and subjects received $10. Of the 1000 survey responses, only 32 did not provide complete information on age, gender, or education and were not included in analyses. Thus, 968 of the 1,000 responses (96.8%) had complete data on these basic demographic characteristics and comprised the community sample.
Survey Instruments
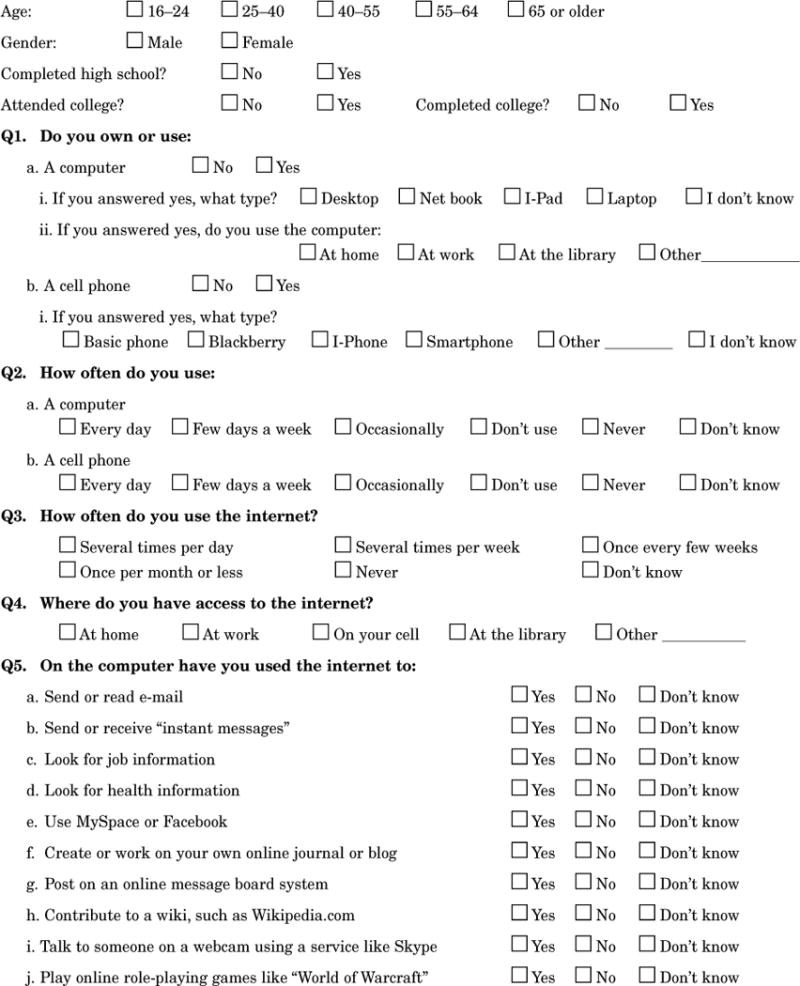
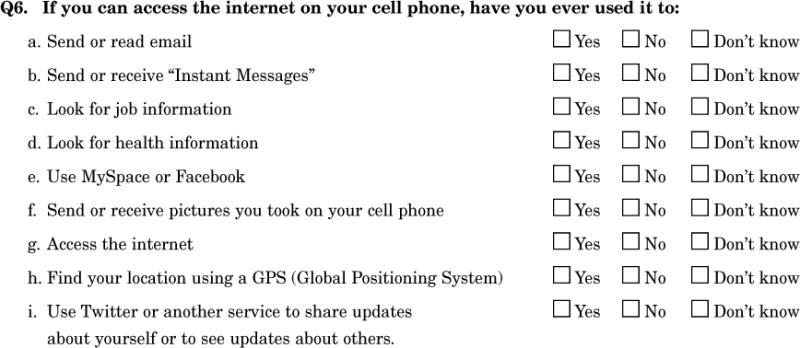
Both surveys included questions about use of ICT as well as questions about age, gender, and education; race and ethnicity were not assessed. The questionnaire used for the clinic sample was adapted from the section of the community sample questionnaire that inquired about technology use. Internet use was assessed in the clinic participants with a series of questions about their use of the Internet on the computer or cell phone and in the community sample with questions about the place where they used the Internet and their reasons for using the Internet. (See Appendix for the survey completed by the clinic sample).
Both surveys ascertained overall Internet and computer use as well as frequency and location of use. The frequency of Internet use variable was dichotomized into “Never” and “Any” use. Participants were rated as having used computers if they specified a location in response to a question about location of computer use.
Analyses
The characteristics of the clinic and community samples’ computer and Internet use were compared using bivariate and multivariate binary logistic models. Multivariate models were adjusted for the socio-demographic variables of age, gender, and education.
A sensitivity analysis using multiple imputation with iterative chained equations was run to determine the impact of missing data on the results of the analyses.19 All analyses were conducted using STATA 12 software.
RESULTS
Socio-demographic Characteristics of Participants
The socio-demographic characteristics of the clinic and community participants are presented in Table 1. Neither age distribution nor gender differed by sample. Education levels differed significantly between the samples; compared to the community sample, the clinic sample had a lower educational attainment level overall. In the clinic sample, 32.8% did not complete high school compared to 19.1% of the community sample, and only 9.5% of the clinic sample indicated that they had completed college compared to 25.3% of the community sample. Comparison of cases with complete data on age, gender, and education with those missing data in one or more of these areas (and so not included in the analyses) revealed no significant differences in demographics in either the community or clinic samples (data not shown).
Table 1.
Characteristics of the 189 clients of an inner-city mental health clinic with serious mental disorders and 968 community participants from the same catchment area*
| Clinic sample | Community sample | ||||||
|---|---|---|---|---|---|---|---|
| N = 189 | N = 968 | Odds ratio | |||||
| n | (%) | n | (%) | OR | 95% CI | p | |
| Age, years | |||||||
| 16–24 | 24 | (12.7) | 107 | (11.1) | 1 | — | — |
| 25–40 | 49 | (25.9) | 241 | (24.9) | 0.91 | 0.53–1.55 | 0.72 |
| 40–55 | 71 | (37.6) | 285 | (29.4) | 1.11 | 0.66–1.86 | 0.69 |
| 55+ | 45 | (23.8) | 335 | (34.6) | 0.60 | 0.35–1.03 | 0.06 |
| Gender | |||||||
| Male | 68 | (36.0) | 388 | (40.1) | 1 | — | — |
| Female | 121 | (64.0) | 580 | (59.9) | 1.19 | 0.86–1.65 | 0.29 |
| Education | |||||||
| Did not complete high school | 62 | (32.8) | 185 | (19.1) | 1 | — | — |
| Completed high school | 61 | (32.3) | 352 | (36.4) | 0.52 | 0.35–0.77 | < 0.01 |
| Attended college | 48 | (25.4) | 186 | (19.2) | 0.77 | 0.50–1.18 | 0.23 |
| Completed college | 18 | (9.5) | 245 | (25.3) | 0.22 | 0.13–0.38 | < 0.01 |
Numbers and analyses reflect cases with complete data for age, gender, and education.
CI: confidence interval
Technology Use in the Clinic Sample
Of the 189 respondents in the clinic sample, 105 (55.6%) reported owning or using a computer, 162 (85.7%) reported owning or using a mobile phone, and 112 (59.3%) reported using the Internet. Of the 105 respondents who owned or used computers, 66 (62.9%) reported owning a desktop computer, 52 (49.5%) a laptop computer, 6 (5.7%) a netbook, 5 (4.8%) an iPad, and 5 (4.8%) did not know the type of computer (categories were not mutually exclusive). Among the 162 respondents (85.7%) in the clinic sample who used a mobile phone, 120 (74.1%) reported using their phone every day, 17 (10.5%) a few days a week, 16 (9.9%) occasionally, and 9 (5.6%) responded “Don’t know,” “Never,” or did not answer the question.
Among the 112 respondents in the clinic sample who reported using the Internet, 47 (42%) reported using it several times per day, 37 (33%) reported using it several times per week, 12 (10.7%) reported using it once every few weeks, and 16 (14.3%) reported using it once per month or less. Respondents were also asked to indicate types of Internet use on computers and on mobile phones. With regard to overall Internet use (either on a computer or a mobile phone), among the 112 Internet users, 98 (87.5%) reported using the Internet for email, 88 (78.6%) for instant messaging, 80 (71.4%) for looking up job information, 85 (75.9%) for looking up health information, and 77 (68.8%) for Facebook or MySpace.
Comparison of Technology Use Between Clinic and Community Samples
Table 2 presents comparisons of technology use between the clinic and community samples. Frequencies were calculated only for cases with complete data, and adjusted analyses controlled for age, gender, and education. While computer and Internet use were less common overall in the clinic sample, the difference between the clinic and community samples reached statistical significance only with regard to computer use (adjusted odds ratio [aOR] 0.39, p < 0.01). In addition, compared to community participants, participants in the clinic sample reported using computers less commonly in all settings except at home.
Table 2.
Computer and Internet use in 189 clients of an inner-city mental health clinic with serious mental disorders and 968 community participants from the same catchment area
| Clinic sample | Community sample | ||||||
|---|---|---|---|---|---|---|---|
| N = 189 | N = 968 | Adjusted odds ratioa | |||||
| n | (%) | n | (%) | aOR | 95% CI | p | |
| Computer useb | |||||||
| Yes | 105 | (55.6) | 717 | (74.1) | 0.39 | 0.26–0.57 | < 0.01 |
| No | 84 | (44.4) | 251 | (25.9) | 1 | — | — |
| Location of computer use (for respondents who used computer)c | |||||||
| Home | 85 | (81.0) | 546 | (76.2) | 1.45 | 0.84–2.53 | 0.18 |
| Work | 16 | (15.2) | 261 | (36.4) | 0.29 | 0.16–0.53 | < 0.01 |
| Library | 36 | (34.3) | 411 | (57.3) | 0.33 | 0.21–0.51 | < 0.01 |
| Other | 3 | (2.9) | 226 | (31.5) | 0.06 | 0.02–0.18 | < 0.01 |
| Internet used | |||||||
| Yes | 112 | (59.3) | 667 | (68.9) | 0.82 | 0.55–1.23 | 0.35 |
| No | 62 | (32.8) | 300 | (31.0) | 1 | — | — |
| Frequency of Internet use (for those using the Internet) | |||||||
| Once per month or less | 16 | (14.3) | 64 | (9.6) | 1 | — | — |
| Once every few weeks | 12 | (10.7) | 62 | (9.3) | 0.78 | 0.34–1.82 | 0.57 |
| Several times per week | 37 | (33.0) | 134 | (20.1) | 1.22 | 0.62–2.43 | 0.56 |
| Several times per day | 47 | (42.0) | 407 | (61.0) | 0.57 | 0.30–1.10 | 0.09 |
| Location of Internet use (for those using Internet)e | |||||||
| Home | 83 | (74.1) | 511 | (76.6) | 1.15 | 0.70–1.90 | 0.58 |
| Work | 17 | (15.2) | 247 | (37.0) | 0.34 | 0.19–0.60 | < 0.01 |
| Mobile | 36 | (32.1) | 327 | (49.0) | 0.45 | 0.29–0.72 | < 0.01 |
| Library | 35 | (31.3) | 399 | (59.8) | 0.25 | 0.16–0.40 | < 0.01 |
| Other | 9 | (8.0) | 197 | (29.5) | 0.18 | 0.09–0.37 | < 0.01 |
| Types of Internet use (for those using Internet)e | |||||||
| 98 | (87.5) | 528 | (79.2) | 3.06 | 1.56–6.02 | < 0.01 | |
| Instant messaging (IM) | 88 | (78.6) | 288 | (43.2) | 5.95 | 3.50–10.12 | < 0.01 |
| Job information | 80 | (71.4) | 427 | (64.0) | 1.48 | 0.90–2.43 | 0.12 |
| Health information | 85 | (75.9) | 446 | (66.9) | 2.00 | 1.21–3.32 | 0.01 |
| Facebook/MySpace (FB) | 77 | (68.8) | 345 | (51.7) | 2.80 | 1.71–4.59 | < 0.01 |
Adjusted odds ratios (aORs) are from separate binary logistic regression models, each adjusting for age, gender, and education. Numbers and analyses reflect cases with complete information for age, gender and education.
Defined as answering in the affirmative to use of computer in any location
Categories are not mutually exclusive and are also conditioned on those using the computer.
Defined as use of the Internet at any frequency other than “Never.” Fifteen participants in the clinic sample and 1 participant in the community sample did not provide this information.
Categories are not mutually exclusive and are also conditioned on those using the Internet either on the mobile phone or through a computer.
CI: confidence interval
There was a trend toward less frequent use of the Internet by clinic sample participants that was strongest when comparing the frequency of Internet use at several times per day vs. once per month or less (aOR 0.57, p < 0.10). However, of those participants in the clinic sample who reported using the Internet, their use of it was more intensive than the community sample participants’ use. They were more likely to use it for email, instant messaging, health information, and social media. The difference across samples with regard to use of the Internet for job information did not reach a statistically significant level (aOR 1.48, p = 0.12).
Analyses of the relationship between demographic characteristics and technology use found that older age was associated with less use of computers (χ2 = 142.6, df = 3, p < 0.01) and the Internet (χ2 = 224.57, df = 3, p < 0.01). However, the association between age and computer use varied across the clinic and community samples (χ2 = 11.86, df = 3, p = 0.01), being stronger and more statistically significant in the community sample (χ2 = 155.36, df = 3, p < 0.01) than in the clinic sample (χ2 = 11.52, df = 3, p = 0.01). In contrast, higher education was associated with greater use of computers (χ2 = 109.13, df = 3, p < 0.01) and the Internet (χ2 = 116.03, df = 3, p < 0.01), and this association did not vary across samples. There was no association between gender and use of computers or the Internet.
Analyses after Imputing Missing Data Using Multiple Imputation
Analysis of multiple-imputed adjusted models affected results only for overall Internet use. When the data from the 189 cases for which complete data were available were analyzed, the adjusted OR of 0.82 did not reach significance (p = 0.35). However, using multiple imputation, the adjusted OR of 0.65 had a p value < 0.04, indicating less use of the Internet in the clinic sample at a statistically significant level.
DISCUSSION
Clinical Implications
The results of this study are encouraging as they suggest widespread use of ICT among individuals with serious mental illness attending an inner city outpatient psychiatry program. Furthermore, it would appear that access to and use of the Internet among this particular population is increasing. A study by Borzekowski et al. that collected data in 2007 found that only 36% of outpatients with a serious mental illness had ever used the Internet.16 Our study, performed in 2011, found that 112 individuals (59.3%) among a similar psychiatric clinic sample had used the Internet. While this was still lower than use in the community comparison group (68.9%), this 64.7% increase in Internet use between 2007 and 2010/2011 among samples of outpatients with serious mental illness far outpaces the <10% change in Internet usage among the general population of the United States during the same period.17 Of those clinic subjects who used computers and the Internet, the majority had access in their own homes, as was the case also in the comparison group. It is important to note that, at the time the survey was done, the academic clinic involved did not use electronic medical records or any form of digital contact or computer-based evaluation with patients, thus no exposure at the clinic might have influenced participants’ reported ICT use. Greater access to and use of the Internet by those with a serious mental illness has important implications for the feasibility and impact of implementing Internet-based therapeutic interventions and could potentially allow greater numbers of individuals to access care.
Three quarters of Internet users in the clinic sample used it to access health information. This finding is similar to that found in a recent U.S. poll in which 80% of Internet users in the United States reported using the Internet to obtain health information.20 Much recent research on emerging interactive technologies (eHealth) has highlighted its potential benefits for health improvement,21 and has postulated that disseminating health information via the Internet would be a cost-effective way to reach a large number of individuals.22 Finding that those with a serious mental illness use the Internet to gather health information offers an excellent opportunity to further improve their wellbeing. Studies have repeatedly found that the uptake of routine medical screenings, such as mammography and colorectal screening, is very low among those with serious mental illness.23–25 Developing medical information websites that provide information on and promote heath screening may be an effective way of reaching this population. Borzekowski et al.16 found that the Internet-based health information sought by those with serious mental illness is predominantly related to mental health issues, so that incorporating health screening information into mental health information websites could be particularly effective. However, while the Internet may increase access to health information, Khazaal et al. have stressed the importance of educating patients on how to identify reliable websites.26 Only 25% of people regularly check the accuracy of the information they obtain online.27 Therefore, clinicians should be aware that patients may be obtaining information about both their diagnoses and their treatment from the Internet and address this possibility with them to ensure that the information they have obtained is accurate.
Use of the Internet as a social communication tool was very common among the clinic sample in this study at rates significantly higher than in the comparison group. Evidence from the communication literature may provide insight into this finding. Compared to face-to-face (FtF) communication, computer-mediated communication (CMC) allows users greater control over self-presentation and allows users to express themselves more clearly without the need to attend to “noise” such as sensations, conversational demands, unwanted cues, or concerns about appearance or behavior.28,29 In an early study of the use of CMC in a population of young people with mental illness, Zimmerman compared content of weekly 30-minute sessions of FtF and CMC conferencing and found evidence of lower stress and greater expression of feelings in the CMC group, concluding that CMC may provide special benefit for adolescents with emotional disorders.30 Likewise one could speculate that, for those who experience the negative symptoms of schizophrenia, CMC would be less stressful than FtF. The high rates of use of the Internet as a social communication tool in this study appear to support the hypothesis that, among those with a serious mental illness, the Internet has the potential to be a comfortable social outlet that could allow them both to find support and to develop a social network to which they may not otherwise have access.
The 85.7% rate of mobile phone use in the clinic sample is comparable to the 82% use of mobile phones found among American adults,31 demonstrating that participants in this sample do not lack access to mobile phones. A number of researchers have studied mobile health (mHealth) interventions for those with a serious mental illness. Depp et al. reported on three studies that used mobile phones to augment psychosocial interventions among patients with bipolar disorder and schizophrenia, concluding that patients found mHealth interventions useful and acceptable.13 Granholme et al. investigated the use of mobile phones for assessing and improving medication compliance, auditory hallucinations, and socialization among a group of patients with schizophrenia and schizoaffective disorder and found that the intervention was feasible.14 Spaniel et al. found that using mobile phones to detect and treat early psychotic symptom re-emergence was an effective intervention.32 Individuals with serious mental illness have expressed interest in using mobile phone-based interventions as part of their treatment,12 and community surveys have found that people find this an acceptable method of monitoring and managing depression, anxiety, and stress.32 The rate of mobile phone access and use found in the present study provides additional support that such interventions are feasible.
Limitations
The findings of this study should be considered in the context of its limitations. Compared to the community sample, the clinic sample was non-random and received no compensation. The receipt of compensation among the community sample could partially explain the difference in completion rates (88.3% in the clinic sample vs. 96.8% in the community sample). The lack of compensation in the clinic population may also have influenced the decision by some not to participate. In addition, in non-random samples, responses may be subject to a selection effect and findings based on self-report surveys are prone to social desirability, recall, and nonresponse biases. A larger proportion of clinic participants used the answer option “Don’t Know” or left responses blank compared to the community sample. This differential pattern of responding, whether due to recruitment or other reasons, represents nonresponse bias and could potentially impact the comparison. However, results of the analyses with multiple imputed data were for the most part consistent with findings from complete case analyses, with the notable exception of comparison of Internet use which became statistically significant in analyses with imputed data. Also, ICT in the community sample was ascertained with a somewhat different instrument, and ICT use was not the focus of the assessment in that sample. No information on the specific diagnoses of clinic participants was collected; however, the clinic is designed to serve individuals with serious mental illness and therefore the distribution of illness and severity in this sample is likely to be representative of a population with serious mental illness.
CONCLUSION
In the context of these limitations, the results of our study indicate that a sample of patients attending an inner city community psychiatry outpatient program are accessing and using ICT in significant numbers. This provides us with opportunities to develop and extend monitoring and treatment interventions and to disseminate pertinent health information to this population. For individuals with serious mental illness these technologies also create opportunities for them to expand their social network in a way that may be more accessible given their symptoms and other challenges.
Acknowledgments
Support for this study provided by National Institute of Mental Health Child Mental Health Services, Service System Research Training Fellowship T32MH019545-21 awarded to Michelle Colder Carras, B.A., and an anonymous donation to the Bloomberg School of Public Health, Department of Mental Health.
Appendix: Technology survey completed by the clinic sample
Footnotes
The authors declare no conflicts of interest.
Contributor Information
MICHELLE COLDER CARRAS, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
RAMIN MOJTABAI, Johns Hopkins Bloomberg School of Public Health and the Johns Hopkins University School of Medicine.
C. DEBRA FURR-HOLDEN, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
WILLIAM EATON, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
BERNADETTE A.M. CULLEN, Johns Hopkins Bloomberg School of Public Health and the Johns Hopkins University School of Medicine.
References
- 1.Houston TK, Ehrenberger HE. The potential of consumer health informatics. Semin Oncol Nurs. 2001;17:41–7. doi: 10.1053/sonu.2001.20418. [DOI] [PubMed] [Google Scholar]
- 2.Klersy C, De Silvestri A, Gabutti G, et al. Economic impact of remote patient monitoring: An integrated economic model derived from a meta-analysis of randomized controlled trials in heart failure. Eur J Heart Fail. 2011;13:450–9. doi: 10.1093/eurjhf/hfq232. [DOI] [PubMed] [Google Scholar]
- 3.Liang X, Wang Q, Yang X, et al. Effect of mobile phone intervention for diabetes on glycaemic control: A meta-analysis. Diabet Med. 2011;28:455–63. doi: 10.1111/j.1464-5491.2010.03180.x. [DOI] [PubMed] [Google Scholar]
- 4.Gainsbury S, Blaszczynski A. A systematic review of Internet-based therapy for the treatment of addictions. Clin Psychol Rev. 2011;31:490–8. doi: 10.1016/j.cpr.2010.11.007. [DOI] [PubMed] [Google Scholar]
- 5.Van Gaalen JL, Hashimoto S, Sont JK. Telemanagement in asthma: An innovative and effective approach. Curr Opin Allergy Clin Immunol. 2012;12:235–40. doi: 10.1097/ACI.0b013e3283533700. [DOI] [PubMed] [Google Scholar]
- 6.Ybarra ML, Biringi R, Prescott T, et al. Usability and navigability of an HIV/AIDS Internet intervention for adolescents in a resource-limited setting. Comput Inform Nurs. 2012;30:587–95. doi: 10.1097/NXN.0b013e318266cb0e. quiz 596–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Centers for Medicare & Medicaid Services. Telemedicine. Available at www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Delivery-Systems/Telemedicine.html, accessed February 12, 2014 (archived by WebCite® at www.webcitation.org/6NKfW0N8I)
- 8.Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the Internet: Randomised controlled trial. BMJ. 2004;328:265. doi: 10.1136/bmj.37945.566632.EE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gruber K, Moran PJ, Roth WT, et al. Computer-assisted cognitive behavioral group therapy for social phobia. Behav Ther. 2001;32:155–65. [Google Scholar]
- 10.Kenardy JA, Dow MGT, Johnston DW, et al. A comparison of delivery methods of cognitive-behavioral therapy for panic disorder: An international multicenter trial. J Consult Clin Psychol. 2003;71:1068–75. doi: 10.1037/0022-006X.71.6.1068. [DOI] [PubMed] [Google Scholar]
- 11.Newman MG, Erickson T, Przeworski A, et al. Self-help and minimal-contact therapies for anxiety disorders: Is human contact necessary for therapeutic efficacy? J Clin Psychol. 2003;59:251–74. doi: 10.1002/jclp.10128. [DOI] [PubMed] [Google Scholar]
- 12.Ben-Zeev D, Davis KE, Kaiser S, et al. Mobile technologies among people with serious mental illness: Opportunities for future services. Adm Policy in Ment Health. 2013;40:340–3. doi: 10.1007/s10488-012-0424-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Depp CA, Mausbach B, Granholm E, et al. Mobile interventions for severe mental illness: Design and preliminary data from three approaches. J Nerv Ment Dis. 2010;198:715–21. doi: 10.1097/NMD.0b013e3181f49ea3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Granholm E, Ben-Zeev D, Link PC, et al. Mobile assessment and treatment for schizophrenia (MATS): A pilot trial of an interactive text-messaging intervention for medication adherence, socialization, and auditory hallucinations. Schizophr Bull. 2012;38:414–25. doi: 10.1093/schbul/sbr155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Oorschot M, Lataster T, Thewissen V, et al. Mobile assessment in schizophrenia: A data-driven momentary approach. Schizophr Bull. 2012;38:405–13. doi: 10.1093/schbul/sbr166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Borzekowski DL, Leith J, Medoff DR, et al. Use of the Internet and other media for health information among clinic outpatients with serious mental illness. Psychiatr Serv. 2009;60:1265–8. doi: 10.1176/ps.2009.60.9.1265. [DOI] [PubMed] [Google Scholar]
- 17.Pew Research Center. Pew Internet & American Life Project. Trend data (adults): Usage over time. Available at www.pewinternet.org/Static-Pages/Trend-Data-(Adults)/Usage-Over-Time.aspx, accessed February 12, 2014.
- 18.Clayton S, Borzekowski D, Himelhoch S, et al. Media and Internet ownership and use among mental health outpatients with serious mental illness. Am J Drug Alcohol Abuse. 2009;35:364–7. doi: 10.1080/00952990903108249. [DOI] [PubMed] [Google Scholar]
- 19.Rubin D. Multiple imputation for nonresponse in surveys. New York: Wiley; 1987. [Google Scholar]
- 20.S Health topics: Health information is a popular pursuit online, Pew Research Center’s Internet & American Life Project. 2011 Feb 1; Available at pewinternet.org/Reports/2011/HealthTopics/Summary-of-Findings/Looking-for-health-information.aspx, accessed February 12, 2014 (archived by WebCite® at www.webcitation.org/6NKg9eDnJ)
- 21.Ahern D, Phalen J, Eaton C. The Role of eHealth in patient engagement and quality improvement. In: Gibbons MC, editor. Health solutions for healthcare disparities. New York: Springer; 2008. pp. 75–92. [Google Scholar]
- 22.Strecher V. Internet methods for delivering behavioral and health-related interventions (eHealth) Annu Rev Clin Psychol. 2007;3:53–76. doi: 10.1146/annurev.clinpsy.3.022806.091428. [DOI] [PubMed] [Google Scholar]
- 23.Howard LM, Barley EA, Davies E, et al. Cancer diagnosis in people with severe mental illness: Practical and ethical issues. Lancet Oncol. 2010;11:797–804. doi: 10.1016/S1470-2045(10)70085-1. [DOI] [PubMed] [Google Scholar]
- 24.Werneke U, Horn O, Maryon-Davis A, et al. Uptake of screening for breast cancer in patients with mental health problems. J Epidemiol Community Health. 2006;60:600–5. doi: 10.1136/jech.2005.039065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Friedman LC, Puryear LJ, Moore A, et al. Breast and colorectal cancer screening among low-income women with psychiatric disorders. Psycho-oncology. 2005;14:786–91. doi: 10.1002/pon.906. [DOI] [PubMed] [Google Scholar]
- 26.Khazaal Y, Chatton A, Cochand S, et al. Internet use by patients with psychiatric disorders in search for general and medical information. Psychiatr Q. 2008;79:301–9. doi: 10.1007/s11126-008-9083-1. [DOI] [PubMed] [Google Scholar]
- 27.Fox S, Rainie L. Vital decisions: How Internet users decide what information to trust when they or their loved ones are sick. Pew Research Center’s Internet & American Life Project; May 22, 2002. Available at www.pewinternet.org/Reports/2002/Vital-Decisions-A-Pew-Internet-Health-Report/Summary-of-Findings.aspx, accessed February 12, 2014 (archived by WebCite® at www.webcitation.org/6NTxOIdyV) [Google Scholar]
- 28.Walther JB. Computer-mediated communication: Impersonal, interpersonal, and hyperpersonal interaction. Communication Research. 1996;23:3–43. [Google Scholar]
- 29.Caplan SE. A social skill account of problematic Internet use. Journal of Communication. 2005;55:721–36. [Google Scholar]
- 30.Zimmerman DP. Effects of computer conferencing on the language use of emotionally disturbed adolescents. Behavior Research Methods, Instruments & Computers. 1987;19:224–30. [Google Scholar]
- 31.Smith A. Mobile access 2010: Part Two: Internet use and data applications using mobile phones. Pew Research Center’s Internet & American Life Project; Jul 7, 2010. Availalble at www.pewinternet.org/Reports/2010/Mobile-Access-2010/Part-2.aspx, accessed February 12, 2014 (archived by WebCite® at www.webcitation.org/6NKgd2U63) [Google Scholar]
- 32.Spaniel F, Vohlídka P, Kozený J, et al. The Information Technology Aided Relapse Prevention Programme in Schizophrenia: An extension of a mirror-design follow-up. Int J Clin Pract. 2008;62:1943–46. doi: 10.1111/j.1742-1241.2008.01903.x. [DOI] [PMC free article] [PubMed] [Google Scholar]