

Abstract
Background:
Identifying risk factors that contribute to shoulder and elbow pain within youth baseball players is important for improving injury prevention and rehabilitation strategies.
Hypothesis:
Differences will exist between youth baseball players with and without a history of upper extremity pain on measures related to growth, shoulder performance, and baseball exposure.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 84 youth baseball players were divided into 2 groups based on self-reported history of throwing-related arm pain. Group differences for growth-related, shoulder performance, and baseball exposure variables were analyzed by use of parametric and nonparametric tests, as appropriate. Multivariate logistic regression was used to assess variables most predictive of pain.
Results:
The group of athletes with pain (n = 16) were taller and heavier, played more baseball per year, and had greater pitching velocity. Athletes with pain also had greater loss of internal rotation range of motion and greater side-to-side asymmetry in humeral retrotorsion (HRT), attributable to lower degrees of HRT within the nondominant humerus. Multivariate analysis revealed that player height was most predictive of pain, with a 1-inch increase in height resulting in a 77% increased risk of pain.
Conclusion:
Vertical growth that accompanies adolescence increases the risk of experiencing throwing-related pain in youth baseball players. Players who are taller, particularly those with faster pitching velocities, are at the greatest risk for developing pain and should be more carefully monitored for resultant injury. The degree of nondominant HRT may have a relationship to the development of pain, but further research is required to better understand the implications of this observation.
Keywords: baseball, shoulder range of motion, humeral retrotorsion, youth athlete, pediatric athlete, pitching velocity
Up to 50% of youth baseball players experience upper extremity pain during their season, and overuse injuries of the shoulder and elbow are a growing concern among sports medicine practitioners.17,18,32,35 Several exposure-related factors have been identified that may increase the risk of injury, including pitching with arm fatigue, pitching with pain, playing baseball more than 8 months each year, experiencing a high overall volume of pitching per game or season, throwing breaking pitches at a young age, and having inadequate rest between pitching outings.7–9,26,28 Despite the implementation of pitching volume and rest time requirements, youth athletes continue to develop overuse injuries at a high rate.8
Recently, greater focus has been placed on variations in physical factors, such as strength,35 range of motion (ROM),32 pitching velocity,25 or humeral retrotorsion (HRT),12,36 as potential contributors to increased risk of injury. However, a limited body of research is available specific to the youth athlete, despite being the largest group of the baseball-playing community.32 Improved understanding of which physical factors increase injury potential would allow for better screening and injury prevention strategies. Thus, the purpose of this study was to examine the relationship between physical characteristics, HRT, shoulder ROM, strength, pitching velocity, playing history, and upper extremity pain in youth baseball players.
Methods
Participants
This cross-sectional study involved male baseball players aged 8 to 14 years who were currently playing baseball. Participants were recruited from local Little League teams and private baseball academies. This cohort was a portion of participants from a larger study.11 All protocols were approved by the institutional review boards of all participating institutions, and written parental consent and child assent were obtained prior to data collection. Participants were excluded if they were female; participated in other repetitive overhead sports such as tennis, squash, or swimming; had any current shoulder problem that limited sports participation; had any history of humeral fracture; or had any known systemic disorder that may result in joint hypermobility (eg, Ehlers-Danlos syndrome).
Demographic and Sports Information
Demographic and baseball participation information was obtained by use of a customized questionnaire that players completed with the help of a parent or guardian. The information collected included age, height, weight, arm dominance (defined as arm used to throw a ball), baseball participation volume (months per year), whether the athlete was a pitcher, age of onset of baseball activity, other sports participation, any previous traumatic upper extremity injury (eg, fracture, dislocation), and shoulder or elbow pain associated with throwing. The presence of pain in the throwing arm was rated dichotomously (yes/no) from the statement “Shoulder or elbow pain with throwing in the past 30 days.” Use of this low threshold for pain classification was based on previous research identifying pitching with arm pain as a risk factor for future injury.25 Classifying participants in this manner allowed for further exploratory analysis of players in the early stages of the pathological cascade that may ultimately present as serious injury. After administration of the survey instrument, participants underwent a bilateral standardized measurement procedure, with the order of assessment of dominant or nondominant shoulder determined by a coin flip. The measurement team was unaware of questionnaire answers at the time of measurement.
Range of Motion Measurements
Glenohumeral external rotation (ER) and internal rotation (IR) ROM at 90° of abduction was assessed with previously described validated methods.12,22,39 The scapula was stabilized and the shoulder passively externally or internally rotated until resistance was felt by the examiner and motion no longer occurred at the glenohumeral joint. A digital inclinometer was then firmly placed along the ulnar aspect of the forearm to determine degree of rotation relative to vertical (Figure 1). The average of 2 trials was used for the final value. This measurement has been shown to have excellent intra- and interrater reliability, with intraclass correlation coefficient (ICC) values greater than 0.90 and a standard error of the mean (SEM) of 1.5° to 2.6°.12,19,23
Figure 1.

(A) Measurement of external rotation range of motion. (B) Measurement of internal rotation range of motion.
Shoulder Strength Measurements
While the athlete remained in the same position, the examiner determined shoulder ER and IR strength using the peak force, recorded as the average of 2 trials during a make test (ie, subject exerts maximal force against stationary dynamometer), measured with a hand-held dynamometer (MicroFET; Hogan Industries) applied just proximal to the ulnar styloid. The validity and reliability of hand-held dynamometry in the assessment of upper extremity strength have been previously documented, with ICC values ranging from 0.79 to 0.97.5,15,34
Humeral Retrotorsion
HRT was assessed in the same body position by use of the indirect ultrasonographic techniques described and validated by Myers et al.21 A 5- to 13-MHz linear array ultrasound transducer (GE LOGIQe; General Electric) was placed on the anterior aspect of the shoulder, perpendicular to the long axis of the humerus and aligned level to the treatment table with a bubble level. A second examiner then rotated the participant’s humerus so that the bicipital groove could be visualized directly with the apexes of the greater and lesser tubercles parallel to the horizontal plane (Figure 2). This examiner then placed a digital inclinometer firmly against the athlete’s ulna, and the forearm inclination angle relative to horizontal was recorded. By standardizing alignment of the proximal humerus and taking advantage of the consistent perpendicular arrangement of the ulna to the transepicondylar axis, this measurement procedure provides the relative difference between the proximal segment (humeral head) and distal segment (epidondylar axis), thus giving an indirect measurement of the degree of longitudinal twisting within the humerus (HRT). The average of 3 measurements was used for data analysis. The examiners underwent specific training for this measurement, and an independent reliability study conducted by the examiner team yielded excellent intraclass correlation, with ICC coefficients of 0.91 to 0.98 and an SEM of 1.8°. This degree of accuracy in the measurements is consistent with other reliability studies using this technique.1
Figure 2.
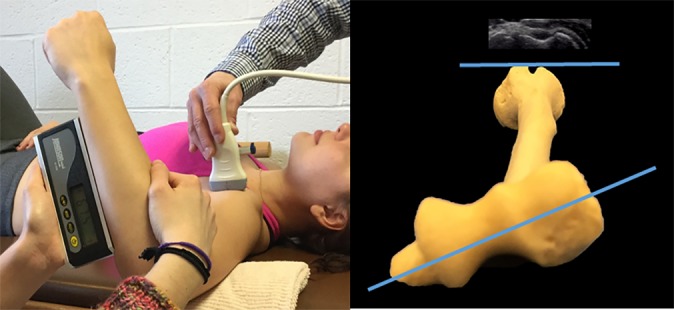
Measurement of humeral retrotorsion (HRT). The apexes of the greater and lesser tuberosities were identified via ultrasonography and aligned horizontally. The angle of the ulna relative to horizontal was measured representing the difference in alignment between the humeral head and transepicondylar axis (degree of HRT). Higher values indicate greater degree of HRT.
Pitching Velocity
Maximum pitching velocity was assessed with a Stalker Sport II (Stalker Radar) radar gun, which can measure pitch speeds from 5 to 150 mph and has an established accuracy of ±3%. After a sufficient amount of warm-up throwing, participants were positioned 46 feet from a stationary target and asked to perform 3 maximum-velocity throws. To standardize the throwing technique, each athlete was asked to pitch from a “stretch” position. The average of 3 throws was used for analysis.
Variables for Data Analysis
Shoulder total range of motion (TROM) was calculated by adding ER and IR values. Glenohumeral IR difference (GIRD), glenohumeral ER difference, difference in TROM (dTROM), and side-to-side difference in HRT (dHRT) were all calculated as dominant side value minus nondominant. Absolute values for dominant and nondominant HRT were also included in the analysis, as previous research has shown that these values (not just side-to-side asymmetry) may affect likelihood of injury.23,27,36 Strength ratios were calculated by use of a ratio of external rotator to internal rotator force (ER/IR) for the dominant limb of each participant. Additional demographic variables chosen for data analysis included age, height, weight, number of months per year playing baseball, and other participation factors.
Statistical Analysis
Participants were divided into 2 groups according to their subjective reports of shoulder or elbow pain: a pain group, who reported pain within the past 30 days, and a pain-free group. All statistical analyses were conducted with the Statistical Package for Social Sciences version 22.0 (SPSS Inc) and Stata version 12.0. Data were assessed for normality by use of the Kolmogorov-Smirnov test. Descriptive statistics were computed to summarize the demographic and clinical measures of the participants exhibiting shoulder or elbow pain and those who did not have pain. Bivariate analysis was conducted to compare between-group differences, using the t test for normally distributed variables and Mann-Whitney U test for nonnormally distributed variables (ie, height, weight, months of baseball, and dHRT). The level of statistical significance was set at P < .05.
We further conducted multivariate logistic regression using a forward-entry method in order to determine the variables that were most likely associated with the presence of shoulder or elbow pain. Variables were chosen based upon significance in bivariate analysis, literature review, and proposed relationship to injury in throwing athletes. Included variables were divided into 3 categories: growth-related variables, shoulder performance variables, and exposure variables. Three models were sequentially created by use of a forward-entry method, and variables were retained in the model if the P value was less than .05. In the first model, only growth-related variables were introduced. The second model was controlled for shoulder performance variables, and the third model was controlled for both shoulder performance and exposure variables. From these models, odds ratios were constructed along with correlation coefficients and pseudo R 2 values to evaluate the percentage of variance explained by individual variables and that accounted for by the model as a whole.
Results
Study Population
A total of 84 athletes were included in the analysis. Sixteen participants (19%) reported a history of shoulder or elbow pain with throwing.
Comparison of History of Pain to Pain-Free Group
The pain and pain-free groups were similar in age, dTROM, dominant HRT, and shoulder strength. The pain group had significantly greater height, weight, GIRD, side-to-side asymmetry in HRT (attributable to decreased nondominant HRT), pitching velocity, and baseball exposure (Table 1).
TABLE 1.
Differences in Variables by Groupa
| Variable | Pain Group (n = 16)b | Pain-free Group (n = 68)b | P Value |
|---|---|---|---|
| Age, y | 11.9 (12.4) ± 1.7 | 11.4 (11.5) ± 1.4 | .192 |
| Height, cmc | 161.7 (160.2) ± 12.3 | 148.2 (149.9) ± 11.4 | .001d |
| Weight, kgc | 51.5 (51.8) ± 17.7 | 40.5 (39.4) ± 10.8 | .018d |
| dTROM, deg | –0.5 (–1.0) ± 9.9 | –0.6 (–0.3) ± 7.9 | .964 |
| Glenohumeral IR difference, deg | –9.1 (–8.7) ± 6.9 | –5.2 (–4.7) ± 6.8 | .041d |
| Glenohumeral ER difference, deg | 8.5 (7.3) ± 8.1 | 4.5 (3.6) ± 7.8 | .069 |
| Dominant HRT, deg | 72.7 (70.1) ± 11.9 | 75.8 (76.5) ± 11.2 | .329 |
| Nondominant HRT, deg | 60.4 (59.9) ± 11.0 | 68.1 (66.9) ± 13.1 | .033d |
| dHRT, degc | 12.3 (10.9) ± 6.9 | 7.6 (8.8) ± 9.8 | .030d |
| ER/IR strength | 0.92 (0.92) ± 0.11 | 0.94 (0.95) ± 0.2 | .682 |
| Pitch velocity, mph | 55.4 (56.8) ± 9.5 | 50.1 (50.0) ± 6.9 | .012d |
| Months per year of baseballc | 10 (10) ± 1.9 | 8.9 (9) ± 1.9 | .040d |
| No. of pitcherse | 13 | 55 | .843 |
adHRT, side-to-side difference in HRT; dTROM, side-to-side difference in total range of motion; ER, external rotation; HRT, humeral retrotorsion; IR, internal rotation.
bValues expressed as mean (median) ± SD, except No. of pitchers.
cNonmormally distributed, analyzed with Mann-Whitney U test.
dStatistically significant, P < .05.
eChi-square test.
Multivariate Analysis
Participant height was the primary factor that predicted injury consistently across all 3 models. We chose to focus on the final model, as the model’s fit was adequate and it was adjusted for shoulder performance and exposure variables. According to our final model (P = .007) with an odds ratio of 1.77 (95% CI, 1.17-2.66), every additional inch of height increased the rate of shoulder or elbow pain by 77%, other factors being equal. Age was significant when only growth-related variables were assessed; however, it was not significant when we controlled for shoulder performance and exposure variables, suggesting that age might function as a moderating variable (Table 2).
TABLE 2.
Multivariate Logistic Regression Modelsa
| Model 1: Growth-Related Variables | Model 2: Growth and Shoulder Performance Variables | Model 3: Growth, Shoulder Performance, and Exposure Variables | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | OR | P | 95% CI | OR | P | 95% CI | OR | P | 95% CI |
| Age | 0.45 | .022b | 0.22-0.89 | 0.60 | .208 | 0.27-1.33 | 0.60 | .219 | 0.27-4.35 |
| Height | 1.55 | .004b | 1.15-2.08 | 1.79 | .005b | 1.19-2.69 | 1.77 | .007b | 1.17-2.66 |
| Weight | 0.99 | .951 | 0.96-1.04 | 0.99 | .723 | 0.96-1.03 | 0.99 | .878 | 0.96-1.03 |
| Difference in shoulder IR | 0.89 | .053 | 0.79-1.00 | 0.90 | .098 | 0.79-1.02 | |||
| Average maximum pitch velocity | 0.90 | .220 | 0.75-1.07 | 0.89 | .190 | 0.75-1.06 | |||
| Nondominant humerus torsion | 0.99 | .915 | 0.93-1.07 | 1.00 | .952 | 0.94-1.07 | |||
| Months per year baseball played | 1.23 | .287 | 0.84-1.79 | ||||||
| Pseudo R 2 | 0.2605 | 0.3265 | 0.3419 | ||||||
aIR, internal rotation; OR, odds ratio.
bStatistically significant, P < .05.
Discussion
The results of this study indicate that the vertical growth that accompanies physical development during adolescence may be an important risk factor for the development of shoulder or elbow pain in youth baseball players. Our multivariate regression analysis demonstrated that player height was most predictive of shoulder or elbow pain, with a 1-inch increase in height resulting in a 77% increased risk of developing throwing-related arm pain. Pain may serve as an important indicator of future injury, and thus recognition of these risk factors is important to prevent injury.16,25,35
Our results are in agreement with previous studies3,25 that found a relationship between increased height and injury within adolescent baseball players. Several hypotheses may account for this relationship. Increased player height and weight may contribute to faster pitching velocity among youth pitchers.31 Taller pitchers exert more torque through the upper extremity while throwing, as a result of longer lever arms and increased pitching velocity.3 We speculate that this leads to increased tissue loading, contributing to an environment of cumulative microtrauma, which creates pain and possible injury. Alternatively, increased height may be associated with more active physes, which may be more susceptible to damage when exposed to the torsional stresses associated with throwing. Hence, players experiencing rapid growth may need reduced throwing volumes. Considering these findings and previous literature outlining arm pain as a risk factor for injury in youth baseball players,16,25 we recommend that taller players be considered to have a higher baseline risk of injury. Close monitoring of these players for other established modifiable risk factors, such as increased pitching volume, inadequate rest, or playing for multiple leagues,3,8,16,17,25 is necessary because these players may have a lower tolerance for extrinsic stressors.
The results of our bivariate analysis are consistent with previous reports that identified shoulder performance variables, such as shoulder ROM,20,32,33,37 and exposure-related variables, such as playing baseball more than 8 months per year,25 as factors that may increase the risk of upper extremity injury. The contribution of deficits in shoulder ROM to upper extremity injury in baseball players is among the most widely studied risk factors, and several investigations have identified an association between loss of shoulder TROM, ER, and IR with increased injury.2,4,20,32,33,37,38 Although most experts would agree that maintaining proper shoulder mobility is important for injury prevention,29 the degree of tolerable IR deficits in throwing athletes is unclear. Currently, GIRD has been defined as a side-to-side deficit of 18° or more and is considered predictive of injury13; however, this value is mostly derived from collective analysis of studies within the adult population. Shanley et al32 performed a prospective investigation of ROM deficits as a predictor of upper extremity injury within adolescent (mean age, 14.9 years) and youth (mean age, 9.9 years) baseball players. Specifically within the adolescent population, a shoulder IR deficit of more than 13° was associated with a 6 times increased likelihood of injury.
Our results are similar to those of Shanley et al32 in that the pain group demonstrated a greater loss of IR motion than the pain-free group; however, the amount of motion loss was lower within our sample (9.1°) than the 13° threshold identified by Shanley et al.32 Differences in mean age (11.9 vs 14.9 years) or the lower threshold for classification (reports of pain vs actual injury) in our study may account for this observation. However, the results of our investigation and those of Shanley et al32 suggest that GIRD is an important risk factor for injury and that younger baseball players may have less tolerance for IR motion loss prior to the development of injury, compared with their adult counterparts. Further investigations, with larger sample sizes within both preadolescents and adolescents, are necessary to more fully understand the details of GIRD and injury within youth baseball players.
Recently, significant interest has arisen in identifying the effect that HRT may have on injury among baseball players. HRT is a longitudinal twist about the long axis of the humerus, with higher degrees of retrotorsion indicating a more posteriorly oriented humeral head. At birth, the humeral head is in marked retrotorsion, and it undergoes a process of derotation (less retrotorsion) during the pediatric and adolescent years.6,14 The forces acting on the proximal humerus during the throwing motion cause a slowing of the developmental humeral derotation process, leading to a position of increased HRT within the dominant side of baseball athletes.30 The degree of nondominant HRT likely represents an individual’s unaltered, genetically predetermined degree of HRT, as the humerus on this side is not exposed to the stresses of throwing.12,30,36 Although no consensus exists, current literature supports the hypothesis that there may exist a “sweet spot” of necessary increased dominant-arm HRT that is protective against injury for throwing athletes,27 but that excessive or inadequate levels of HRT may increase the risk of shoulder or elbow injuries.10,24,27 Interestingly, we found no difference in dominant-arm HRT between groups. We did, however, find that the pain group demonstrated a larger degree of side-to-side HRT asymmetry, as a result of less HRT on the nondominant side (Figures 3 and 4). Our findings illustrating a relationship between nondominant HRT and throwing-related pain are similar to those of Whiteley et al,36 who found the degree of nondominant HRT to be predictive of injury within a sample of 35 adolescent (mean age, 16.6 years) baseball players. It has been hypothesized that players who have less genetic HRT (ie, lower degrees of nondominant HRT) will have a greater need for adaptation of HRT within the dominant arm to obtain the protective benefits.36 In turn, these players may impose greater throwing-induced remodeling stressors to the proximal humerus, resulting in greater potential for injuries such as proximal humeral epiphysiolysis (Little League shoulder), ulnar collateral ligament injuries, or shoulder labral injuries. Our results imply that assessment of a player’s genetic (nondominant) HRT may be of value as a screening tool that can identify at-risk players who may need to be monitored more closely for the development of upper extremity injury. Additional longitudinal research studies, with serial tracking of HRT and injuries within preadolescent or adolescent baseball players, are necessary to more fully understand this relationship.
Figure 3.

Humeral retrotorsion (HRT) values on the dominant and nondominant sides for each group. A significant difference (P = .03) was found in the nondominant shoulder, with the pain group demonstrating less HRT.
Figure 4.

Asymmetry in humeral retrotorsion (HRT). Lower values of HRT within the nondominant shoulder of the pain group resulted in a statistically significant (¥ P = .03) side-to-side asymmetry in HRT.
This study has several limitations that we must acknowledge. We classified participants into their respective groups using self-reported recall of throwing-related pain within the past 30 days. We did not require any time missed from playing or specific medical diagnosis to classify players into the pain group. This low threshold for classification may have allowed players to be placed into the pain group without having a specific diagnosed injury. However, using this subclinical classification scheme allowed us to identify risk factors that may lead to more serious shoulder or elbow pathological conditions. In addition, athletes undertook no standardized warm-up prior to ROM assessment. This may have affected our shoulder rotation measurements; however, all data were obtained during active practice times, and all players had undergone a team-specific warm-up at the time of measurement. Therefore, we believe that there was likely proportionate tissue preconditioning across all measurements, limiting the impact of this factor. Our study was cross-sectional in nature, which limits our ability to interpret how these variables change over time. Longitudinal data are necessary to more fully understand this issue. Our pain group was somewhat small, which may have caused our study to become underpowered and thus limited our ability to detect statistical significance among other variables. Additionally, the smaller number of individuals in the pain group did not allow us to analyze factors for elbow or shoulder pain independently, nor could we differentiate risk factors based on pitcher or positional player. However, within this age group and competition level, most pitchers also play field positions and have not specialized in pitching alone. In addition, most of the throwing exposure at this level comes as a result of practice and free-play rather than specific throwing from a particular position during games. Thus, we believe that comparing pitchers versus field players, a comparison typically seen in adult literature, may not be appropriate within our sample. Finally, as part of our larger study, we recruited only players who played baseball 6 months per year or more, so our data related to baseball exposure may have lacked adequate variability and influenced the findings.
Conclusion
Our results indicate that monitoring player height may assist in identifying youth baseball players at the highest risk of developing throwing-related shoulder or elbow pain. In addition, injury prevention efforts may be strengthened through regular assessment of shoulder ROM, specifically GIRD, as well as HRT. However, further research is necessary to improve our understanding of these risk factors, specifically within the youth athlete.
Acknowledgment
We thank Divya Talwar, PhD, for assistance with the statistical analysis.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A portion of this study was funded by the Legacy Fund Grant awarded by the Sports Section of the American Physical Therapy Association.
Ethical approval for this study was obtained from Arcadia University Committee for Protection of Research Subjects (protocol No. 14-03-16).
References
- 1. Bailey LB, Beattie PF, Shanley E, Seitz AL, Thigpen CA. Current rehabilitation applications for shoulder ultrasound imaging. J Orthop Sports Phys Ther. 2015;45(5):394–405. [DOI] [PubMed] [Google Scholar]
- 2. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology, part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19:404–420. [DOI] [PubMed] [Google Scholar]
- 3. Chalmers PN, Sgroi T, Riff AJ, et al. Correlates with history of injury in youth and adolescent pitchers. Arthroscopy. 2015;31:1349–1357. [DOI] [PubMed] [Google Scholar]
- 4. Dines JS, Frank JB, Akerman M, Yocum LA. Glenohumeral internal rotation deficits in baseball players with ulnar collateral ligament insufficiency. Am J Sports Med. 2009;37:566–570. [DOI] [PubMed] [Google Scholar]
- 5. Donatelli R, Ellenbecker TS, Ekedahl SR, Wilkes JS, Kocher K, Adam J. Assessment of shoulder strength in professional baseball pitchers. J Orthop Sports Phys Ther. 2000;30:544–551. [DOI] [PubMed] [Google Scholar]
- 6. Edelson G. The development of humeral head retroversion. J Shoulder Elbow Surg. 2000;9:316–318. [DOI] [PubMed] [Google Scholar]
- 7. Fleisig GS, Andrews JR. Prevention of elbow injuries in youth baseball pitchers. Sports Health. 2012;4:419–424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers: a 10-year prospective study. Am J Sports Med. 2011;39:253–257. [DOI] [PubMed] [Google Scholar]
- 9. Fleisig GS, Weber A, Hassell N, Andrews JR. Prevention of elbow injuries in youth baseball pitchers. Curr Sports Med Rep. 2009;8:250–254. [DOI] [PubMed] [Google Scholar]
- 10. Greenberg EM, Fernandez-Fernandez A, Lawrence JT, McClure P. The development of humeral retrotorsion and its relationship to throwing sports. Sports Health. 2015;7:489–496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Greenberg EM, Lawrence JT, Fernandez-Fernandez A, McClure P. Humeral retrotorsion and glenohumeral motion in youth baseball players compared with age-matched nonthrowing athletes. Am J Sports Med. 2017;45:454–461. [DOI] [PubMed] [Google Scholar]
- 12. Hibberd EE, Oyama S, Myers JB. Increase in humeral retrotorsion accounts for age-related increase in glenohumeral internal rotation deficit in youth and adolescent baseball players. Am J Sports Med. 2014;42(4):851–858. [DOI] [PubMed] [Google Scholar]
- 13. Kibler WB, Kuhn JE, Wilk K, et al. The disabled throwing shoulder: spectrum of pathology—10-year update. Arthroscopy. 2013;29:141–161.e126. [DOI] [PubMed] [Google Scholar]
- 14. Krahl VE. The torsion of the humerus; its localization, cause and duration in man. Am J Anat. 1947;80:275–319. [DOI] [PubMed] [Google Scholar]
- 15. Leggin BG, Neuman RM, Iannotti JP, Williams GR, Thompson EC. Intrarater and interrater reliability of three isometric dynamometers in assessing shoulder strength. J Shoulder Elbow Surg. 1996;5:18–24. [DOI] [PubMed] [Google Scholar]
- 16. Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463–468. [DOI] [PubMed] [Google Scholar]
- 17. Lyman S, Fleisig GS, Waterbor JW, et al. Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Med Sci Sports Exerc. 2001;33:1803–1810. [DOI] [PubMed] [Google Scholar]
- 18. Makhni EC, Morrow ZS, Luchetti TJ, et al. Arm pain in youth baseball players: a survey of healthy players. Am J Sports Med. 2015;43:41–46. [DOI] [PubMed] [Google Scholar]
- 19. Mullaney MJ, McHugh MP, Johnson CP, Tyler TF. Reliability of shoulder range of motion comparing a goniometer to a digital level. Physiother Theory Pract. 2010;26:327–333. [DOI] [PubMed] [Google Scholar]
- 20. Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006;34:385–391. [DOI] [PubMed] [Google Scholar]
- 21. Myers JB, Oyama S, Clarke JP. Ultrasonographic assessment of humeral retrotorsion in baseball players: a validation study. Am J Sports Med. 2012;40:1155–1160. [DOI] [PubMed] [Google Scholar]
- 22. Myers JB, Oyama S, Goerger BM, Rucinski TJ, Blackburn JT, Creighton RA. Influence of humeral torsion on interpretation of posterior shoulder tightness measures in overhead athletes. Clin J Sport Med. 2009;19:366–371. [DOI] [PubMed] [Google Scholar]
- 23. Myers JB, Oyama S, Rucinski TJ, Creighton RA. Humeral retrotorsion in collegiate baseball pitchers with throwing-related upper extremity injury history. Sports Health. 2011;3:383–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Noonan TJ, Thigpen CA, Bailey LB, et al. Humeral torsion as a risk factor for shoulder and elbow injury in professional baseball pitchers. Am J Sports Med. 2016;44(9):2214–2219. [DOI] [PubMed] [Google Scholar]
- 25. Olsen SJ II, Fleisig GS, Dun S, Loftice J, Andrews JR. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905–912. [DOI] [PubMed] [Google Scholar]
- 26. Petty DH, Andrews JR, Fleisig GS, Cain EL. Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med. 2004;32:1158–1164. [DOI] [PubMed] [Google Scholar]
- 27. Polster JM, Bullen J, Obuchowski NA, Bryan JA, Soloff L, Schickendantz MS. Relationship between humeral torsion and injury in professional baseball pitchers. Am J Sports Med. 2013;41(9):2015–2021. [DOI] [PubMed] [Google Scholar]
- 28. Ray TR. Youth baseball injuries: recognition, treatment, and prevention. Curr Sports Med Rep. 2010;9:294–298. [DOI] [PubMed] [Google Scholar]
- 29. Reinold MM, Gill TJ, Wilk KE, Andrews JR. Current concepts in the evaluation and treatment of the shoulder in overhead throwing athletes, part 2: injury prevention and treatment. Sports Health. 2010;2:101–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Sabick MB, Kim YK, Torry MR, Keirns MA, Hawkins RJ. Biomechanics of the shoulder in youth baseball pitchers: implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med. 2005;33:1716–1722. [DOI] [PubMed] [Google Scholar]
- 31. Sgroi T, Chalmers PN, Riff AJ, et al. Predictors of throwing velocity in youth and adolescent pitchers. J Shoulder Elbow Surg. 2015;24:1339–1345. [DOI] [PubMed] [Google Scholar]
- 32. Shanley E, Kissenberth MJ, Thigpen CA, et al. Preseason shoulder range of motion screening as a predictor of injury among youth and adolescent baseball pitchers. J Shoulder Elbow Surg. 2015;24:1005–1013. [DOI] [PubMed] [Google Scholar]
- 33. Shanley E, Rauh MJ, Michener LA, Ellenbecker TS, Garrison JC, Thigpen CA. Shoulder range of motion measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am J Sports Med. 2011;39:1997–2006. [DOI] [PubMed] [Google Scholar]
- 34. Sullivan SJ, Chesley A, Hebert G, McFaull S, Scullion D. The validity and reliability of hand-held dynamometry in assessing isometric external rotator performance. J Orthop Sports Phys Ther. 1988;10:213–217. [DOI] [PubMed] [Google Scholar]
- 35. Trakis JE, McHugh MP, Caracciolo PA, Busciacco L, Mullaney M, Nicholas SJ. Muscle strength and range of motion in adolescent pitchers with throwing-related pain: implications for injury prevention. Am J Sports Med. 2008;36:2173–2178. [DOI] [PubMed] [Google Scholar]
- 36. Whiteley RJ, Adams RD, Nicholson LL, Ginn KA. Reduced humeral torsion predicts throwing-related injury in adolescent baseballers. J Sci Med Sport. 2010;13:392–396. [DOI] [PubMed] [Google Scholar]
- 37. Wilk KE, Macrina LC, Fleisig GS, et al. Deficits in glenohumeral passive range of motion increase risk of elbow injury in professional baseball pitchers: a prospective study. Am J Sports Med. 2014;42:2075–2081. [DOI] [PubMed] [Google Scholar]
- 38. Wilk KE, Macrina LC, Fleisig GS, et al. Correlation of glenohumeral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers. Am J Sports Med. 2011;39:329–335. [DOI] [PubMed] [Google Scholar]
- 39. Wilk KE, Reinold MM, Macrina LC, et al. Glenohumeral internal rotation measurements differ depending on stabilization techniques. Sports Health. 2009;1:131–136. [DOI] [PMC free article] [PubMed] [Google Scholar]