

Abstract
Larsen, MN, Nielsen, CM, Ørntoft, CØ, Randers, M, Manniche, V, Hansen, L, Hansen, PR, Bangsbo, J, and Krustrup, P. Physical fitness and body composition in 8–10-year-old Danish children are associated with sports club participation. J Strength Cond Res 31(12): 3425–3434, 2017—We investigated whether physical fitness and body composition in 8–10-year-old Danish children are associated with sports club participation. The study included 423 schoolchildren, comprising 209 girls and 214 boys, of whom 67 and 74%, respectively, were active in sports clubs. Yo-Yo intermittent recovery level 1 for children (YYIR1C), balance, jump and coordination tests, together with dual-energy X-ray absorptiometry, were used to determine exercise capacity and body composition. Children active in sports clubs had better (p < 0.05) YYIR1C (33%, 767 ± 26 vs. 575 ± 29 m), 20-m sprint (3%, 4.33 ± 0.03 vs. 4.48 ± 0.04 seconds), coordination (6%, 68 ± 1 vs. 72 ± 1 second), and balance test performances (9%, 19.3 ± 0.5 vs. 21.2 ± 0.7 falls·min−1) and lower fat mass index (16%, 3.8 ± 0.1 vs. 4.5 ± 0.2 kg[fat]·m−2) than children not active in sports clubs. Ball game players had better (p < 0.05) YYIR1C (38%, 925 ± 39 vs. 671 ± 28 m), 20-m sprint (4%, 4.25 ± 0.03 vs. 4.42 ± 0.04 seconds), and coordination test performances (5%, 65 ± 1 vs. 69 ± 1 second), along with higher (p < 0.05) lean body mass (5%, 24.00 ± 0.22 vs. 22.83 ± 0.25 kg) and whole-body BMD (2%, 0.90 ± < 0.01 vs. 0.88 ± <0.01 g·cm−2) compared with children active in other sports. The study showed that 8‒10-year-old Danish children engaged in sports-club activity, especially ball game players, have better exercise capacity and superior body composition compared with children not active in sports clubs.
Key Words: DXA, body fat, lean body mass, bone mineralization
Introduction
It is well known that regular physical activity is associated with significant positive physical and mental health benefits (30) and plays an important role in the prevention of various chronic diseases (7,13). Physical activity habits and attitudes are formed during childhood and carried into adulthood (23). Thus, body mass index (BMI) during childhood is correlated with the risk of coronary artery disease in adulthood (6). Several studies have emphasized that there is an association between clustering of cardiovascular disease risk factors and physical inactivity (23) as well as poor fitness in 9–16-year-old schoolchildren (5). Moreover, several training studies have shown that short-term (6–26 weeks) team sport training improves intermittent exercise performance and aerobic fitness, and elicits significant adaptations of myocardial structure and function, respectively, in 8–12-year-old schoolchildren (9,15–17,22).
Several strategies are being used to increase the physical activity and fitness of children, including physical education at school, school playground activities, organized leisure-time sports-club activity, and nonorganized activities during leisure time. Recent studies have shown that sports-club participation contributes significantly to the amount of time that younger Danish children spend engaged in physical activity, including moderate-to-vigorous physical activity, and therefore plays an important role in targeting the World Health Organization global recommendation of 60 minutes of moderate-to-vigorous intensity daily physical activity (20,27,40). In fact, as many as 98% of 9–11-year-old Danish boys and girls who participate in 1–4 weekly training sessions at local football clubs meet the recommendation on daily physical activity, with corresponding figures of 83% for those participating in other sports-club activities and 76% for children not involved in sports-club activity (20).
Less data are available on the physical fitness and body composition of younger ball game players and children active in other sports clubs compared with age-matched children not participating in organized sports-club activities, although there are some indications that physical fitness and body composition are influenced positively by sports-club participation, at least for certain sports. Indeed, 2 studies from Southern Europe have shown that 10–15-year-old children involved in team sport have stronger bones than children involved in organized swimming and cycling as well as children not participating in sports club activities (33,37–39). Likewise, 2 recent investigations conducted in Portugal have shown that aerobic fitness evaluated by Yo-Yo intermitting running test performance, which is correlated to maximal oxygen uptake, is much higher in 9–16-year-old girls and boys participating in football club training than in age-matched children not active in sports clubs (31,32). Specifically, it was observed that performance in the Yo-Yo intermittent recovery level 1 children's (YYIR1C) test was 43 and 57% higher, respectively, in 8–10-year-old girls and boys active in football clubs (31,32). These 2 studies also showed markedly lower-body fat in the girls and boys active in football clubs in the age groups 12–13 and 14–16, whereas there were no significant differences in body fat in 9–11-year olds (31,32). This may be related to fewer years of sports club participation. These findings require confirmation in children from other countries and it would be of interest to study whether the body composition and musculoskeletal fitness components, such as muscle strength, balance and coordination, are associated with children's sports club participation.
Thus, the aims of this study were to investigate whether physical fitness and body composition in 8–10-year-old Danish schoolchildren are related to participation in sports club training, type of sports club training, and sex.
Methods
Experimental Approach to the Problem
The study has a cross-sectional design, including physical testing and basal information to test whether physical fitness and body composition are associated with sports club participation. All study-dependent variables and methods were selected based on established practice and documented use for providing valid measurements on schoolchildren's physiological development and health in the investigated domains, i.e., cardiorespiratory fitness, motor fitness and skills, and anthropometrics, respectively.
Subjects
We invited 447 third-grade pupils from 20 classes at 8 Danish municipal schools, of whom 423 (209 girls and 214 boys) aged 9.3 ± 0.3 years (97% in Tanner stage 1, 70% active in sports clubs) took part in the study. An overview of the study population can be found in Tables 1 and 2. The study was approved by the Committees on Biomedical Research Ethics for the Capital Region of Denmark (J.no. H-3-2013-038) and registered at ClinicalTrials.gov (NCT02000492). Informed child assent and written informed parental consent were obtained for all participants. All tests were performed during school time at the beginning of the school year by members of the study group, supported by the schools' teachers. All the children were interviewed and physically examined by a medical doctor (CMN) with pediatric expertise. The doctor also evaluated their physical development according to Tanner stages by inspecting genitals, breasts, and pubic hair. Three children were excluded because of physical disabilities or handicaps. Questionnaires were used to determine whether the children participated in sports club activities at least once a week. Initially, the children were divided into 2 groups (active or not active in sports clubs). For detailed analysis, the children active in sports clubs were then categorized by ball games activities (e.g., football, team handball, basketball, floorball, and volleyball) or other sports (e.g., dance, gymnastics, badminton, and swimming). Previous investigations have shown that the intensity and organization are similar for football, team handball, basketball, and floorball (9,20), and it should be noted that the majority of Danish 8–10-year-old children involved in ball game activities attend football or team handball clubs.
Table 1.
Descriptive characteristics and anthropometrics of the study population, stratified by sex and sports club involvement.*†
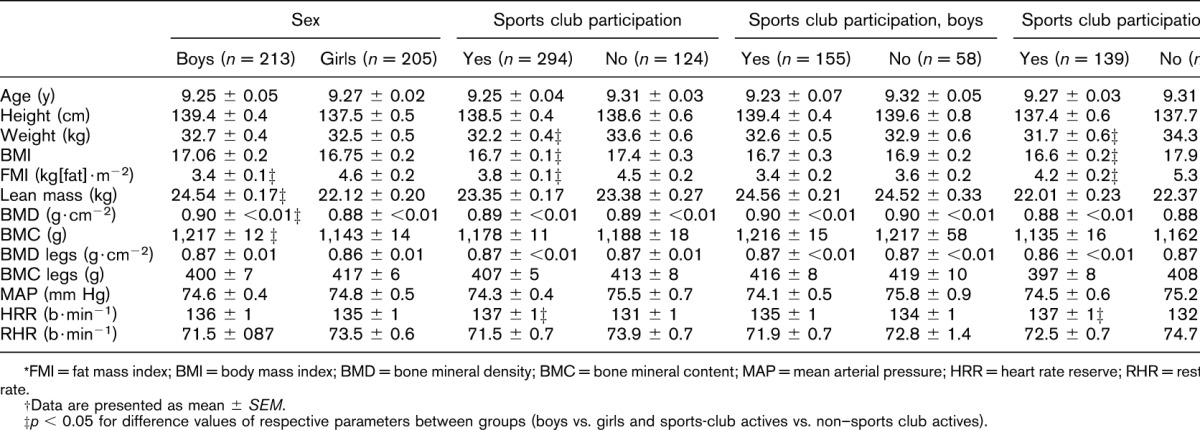
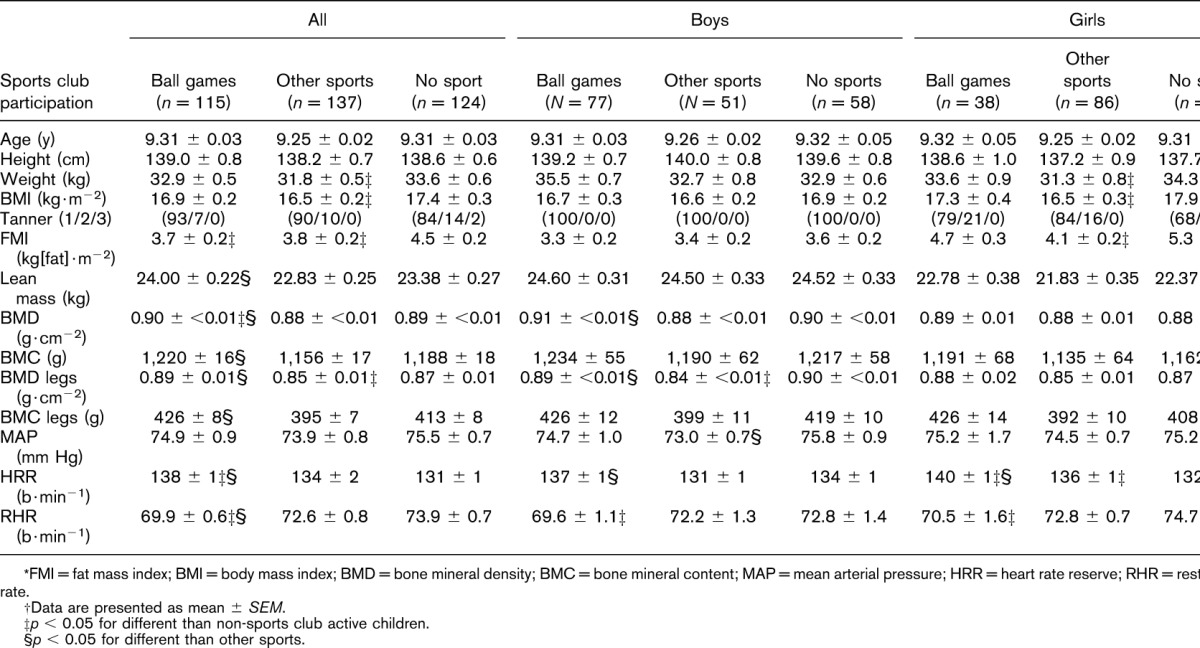
Table 2.
Descriptive characteristics and anthropometrics of the study population, stratified by sex and sports club involvement.*†
Procedures
Yo-Yo Intermittent Recovery Level 1 Children's Test
YYIR1C, a modified version of the Yo-Yo intermittent recovery level 1 test (2), was used to measure fitness level. The test was conducted at the schools in indoor sports halls or gyms with wooden floors. After a standardized warm-up procedure, including the first 3 running bouts, the subjects had to run 16 m back and forth in a straight lane marked by cones, followed by a 10-second recovery period in which they walked around a cone 4 m behind the running lane. The running pace, determined by beep-signals from loudspeakers in the gym, was increased gradually during the test according to the test protocol. The first time the subject failed to reach the finishing line in time, a warning was issued. The second time this happened, the test was terminated and the result noted by the research team. The researchers also participated in the test to ensure that the children knew the right pace and to motivate the last children running. Heart rate (HR) was recorded at 1-second intervals during the tests using a Polar Team System 2 (Polar Electro Oy, Kempele, Finland) to determine maximal HR (HRmax), i.e., the highest value registered during each test. Submaximal HR (HRsubmax) was calculated 2 minutes into the test as mean HR from 1:45 to 2:15 minutes. Submaximal aerobic loading 2 minutes into the test and YYIR1C performance have been shown to be valid measures of aerobic fitness in children younger than 10 years (8).
Postural Balance
Postural balance was evaluated using the single-leg flamingo balance test (1) performed on a 3-cm-wide and 5-cm-high bar. The subject was instructed to take off his or her shoes and stand on one leg on the bar, with eyes open, holding the contralateral leg at the ankle joint. The number of times the subject fell off the bar (defined as touching the ground or unable to hold the contralateral leg at the ankle joint) within 1 minute was counted and used as an indicator of postural balance (1). The subjects were given one try with each leg before choosing their preferred leg for the test. If the children fell more than 20 times before 1 minute had elapsed, the time at 20 falls was recorded. The time recorded at 20 falls was used to calculate the number of falls for a 1-minute period.
Maximal Horizontal Jump Length
After a standardized warm-up procedure, including squat jumps with arms behind the back as instructed, the children were asked to stand upright behind a line with their feet parallel and shoulder-width apart. After flexing the knees to the squat position, the children counted to 2 and jumped as far as they could. If the jump was accepted by the scientific staff, the distance to where the heel landed was measured. If the jump was not accepted, the children got another chance after a rest period. This is a reliable method (41), and maximal horizontal jump performance is well correlated with leg muscle strength in children (10,29).
Twenty-meter Sprint Test
After the warm-up and squat jump, the children performed 2 × 20-m maximal sprints with at least 2 minutes of recovery between sprints. All sprints started from a standing position and were timed using 2 gates of light sensors (Witty Microgate, Bolzano, Italy) placed at 0 m (positioned 30 cm in front of the standing-start position) and at 20 m. The best time recorded was noted as the test result.
Gross Motor Skills
Time (in seconds) to complete a coordination wall with 3 stages of increased difficulty was used to evaluate gross motor skill (14). Each stage consisted of a table (9 × 8 A5 size squares) with numbered marks from 1 to 10. Half the numbers were blue, half red. The 2 lowest ranks were separated from the higher ranks by a thick line. The subjects had a red mark on the right hand and a blue mark on the left hand, and were instructed to touch the numbers from 1 to 10 in the correct order and as fast as possible with the hand (above the thick line) or foot (below) matching the color of the number. If they made a mistake, they were told to correct the mistake and proceed, while the clock was still ticking. Stage 1 was unilateral, with no crossing over the vertical midline, stage 2 with crossing over the vertical midline, and stage 3 bilateral. Each child was given 3 attempts at each stage, and the best (shortest) times from each stage were summed to get a combined score.
Resting Blood Pressure and Resting Heart Rate
Systolic and diastolic blood pressure (BP) were measured with the participants in a supine position after 10–20 minutes of supine rest in a quiet, dimly lit room. Blood pressure was recorded 3 times on the right upper arm using an automatic BP monitor (M6 HEM-7223-E; Omron, Lake Forest, IL, USA) with a cuff adjusted to the arm size as appropriate (18). Mean arterial BP was calculated as diastolic BP + 1/3 × (systolic BP − diastolic BP). Resting HR was measured simultaneously using a chest belt monitor (Polar Team 2 system; Polar, Kempele, Finland). Heart rate was recorded at 5-second intervals throughout the measurement period, with the lowest average value over a 30-second period used to denote resting HR. Heart rate reserve (HRR) was determined by subtracting the resting HR from HRmax.
Anthropometric Measures
Height was measured to the nearest millimeter (235 Heightronic Digital Stadiometer; QuickMedical, Issaquah, WA, USA), and the children were then weighed to the nearest 0.1 kg (Tanita WB-110 MA; Tanita, Amsterdam, The Netherlands) while barefoot and wearing light clothing. Whole-body and leg-bone mineral density (BMD) and bone mineral content (BMC), as well as lean body mass and fat mass index (FMI), were estimated with a whole-body dual-energy X-ray absorptiometry (Lunar Prodigy; GE Medical Systems, Madison, WI, USA) using Encore software version 13.5 (Encore, Madison, WI, USA), with a coefficient of variation for whole-body variables of <1%. The children were instructed to fast for at least 2 hours and to visit the toilet before the scan. The children were scanned in a supine position wearing light clothing (24).
Statistical Analyses
Data are presented as mean ± SEM. All data were tested for normality using the Shapiro-Wilk's test. Baseline values for the groups (children active in sports clubs vs. children not active in sports clubs and ball games vs. other sports vs. no sports) were compared using 1-way analyses of variance. The significance level was set at 0.05.
Results
Physical Fitness
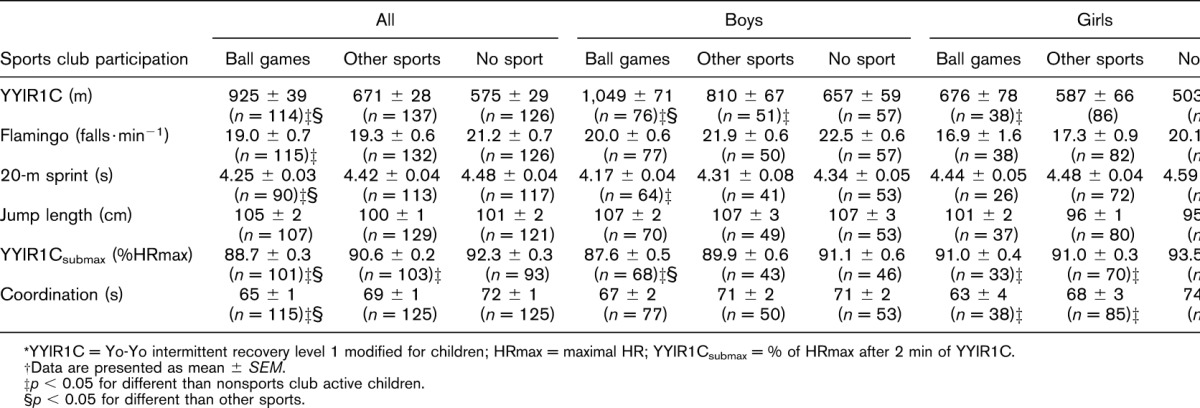
Children active in sports clubs had better YYIR1C performance (33%, 767 ± 26 vs. 575 ± 29 m; p < 0.01) and lower HRsubmax (2%, 90.3 ± 0.4 vs. 92.3 ± 0.3% HRmax; p < 0.05) after 2 minutes of YYIR1C, and these scores were better in ball game players than in those active in other sports (38%, 925 ± 39 vs. 671 ± 28 m and 2%, 88.7 ± 0.3 vs. 90.6 ± 0.2% HRmax; p < 0.05). The ball game players also had better 20-m sprint (4%, 4.25 ± 0.03 vs. 4.48 ± 0.04 seconds; p < 0.05), balance test (10%, 19.0 ± 0.5 vs. 21.2 ± 0.7 falls·min−1; p < 0.05), and coordination test (10%, 65 ± 1 vs. 72 ± 1 second; p < 0.05) performances than the children not active in sports clubs (Tables 3 and 4). Moreover, the ball game players performed better in the 20-m sprint (4%, 4.25 ± 0.03 vs. 4.42 ± 0.04 seconds; p < 0.05) and coordination (5%, 65 ± 1 vs. 69 ± 1 second; p < 0.05) tests than the children active in other sports. No significant difference was observed between the groups in respect of jump performance (103 ± 1 vs. 101 ± 2 cm; p = 0.35).
Table 3.
Physical performance of the study population, stratified by sex and sports club involvement.*†
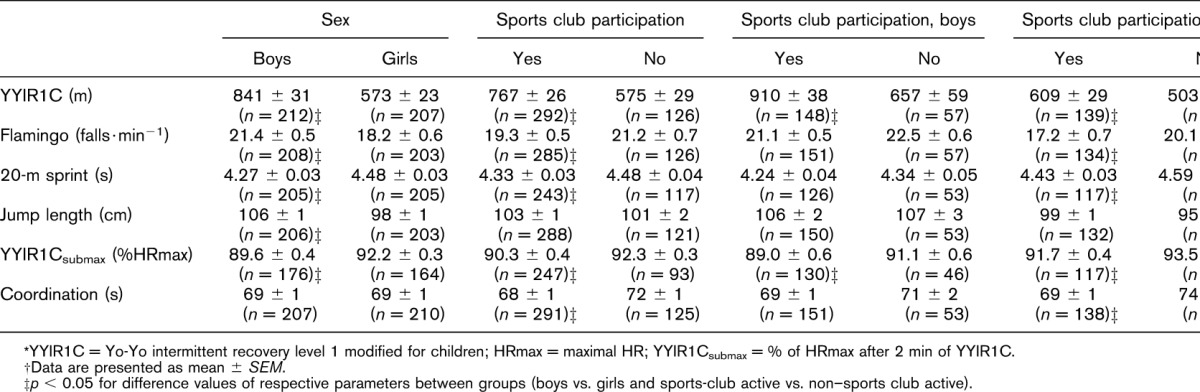
Table 4.
Physical performance of the study population, stratified by sex and sports club involvement.*†
The girls had 15% better balance test performance than the boys (18.2 ± 0.6 vs. 21.4 ± 0.5 falls·min−1, p < 0.05), whereas the boys performed 47% better (p < 0.05) than the girls in YYIR1C (840 ± 31 vs. 573 ± 23 m; p < 0.05). The boys also performed better in the 20-m sprint test (5%, 4.23 ± 0.03 vs. 4.45 ± 0.03 seconds, p < 0.05), had lower HRsubmax in the YYIR1C test (2%, 89.6 ± 0.4 vs. 92.2 ± 0.3%; p < 0.05), and had better jump test performance (8%, 106 ± 1 vs. 98 ± 1 cm; p < 0.05) than the girls (Table 3). There were no differences in coordination abilities between sexes (Tables 3 and 4).
Heart Rate and Blood Pressure
The children active in sports clubs had higher HRR than those not active in sports clubs (5%, 137 ± 1 vs. 131 ± 1 b·min−1; p < 0.05). The ball game players had higher HRR (p < 0.05) than subjects active in other sports and those not active in sport (Table 2). Resting HR was lower (p < 0.05) in ball game players (69.9 ± 0.6 b·min−1) than in subjects active in other sports (72.6 ± 0.8 b·min−1) and those not active in sport (73.9 ± 0.7 b·min−1). Mean arterial BP tended to be lower for the children active in sports clubs (74.3 ± 0.4 vs. 75.5 ± 0.7 mm Hg; p = 0.09). No differences were observed in HRR or BP between boys and girls.
Body Composition
Body composition variables are presented in Tables 1 and 2. The children active in sports clubs had lower FMI than those not active in sports clubs (16%, 3.8 ± 0.1 vs. 4.5 ± 0.2 kg·m−2; p < 0.001). The children active in other sports had lower-body weight (5%, 31.8 ± 0.5 vs. 33.6 ± 0.6 kg; p < 0.001) and BMI (16.5 ± 0.2 vs. 17.4 ± 0.3 kg·m−2; p < 0.001) than those not active in sport. Ball game players had higher lean body mass (5%, 24.00 ± 0.22 vs. 22.83 ± 0.25 kg; p < 0.001) than subjects active in other sports. Whole-body and leg BMD (2%, 0.90 ± <0.01 vs. 0.88 ± <0.01 g·cm−2 and 4%, 0.89 ± 0.01 vs. 0.85 ± 0.01 g·cm−2; p < 0.001), as well as BMC (6%, 1,220 ± 16 vs. 1,156 ± 17 g and 8%, 426 ± 8 vs. 395 ± 7; p < 0.001), were also higher in ball game players than in subjects active in other sports. Whole-body BMD was also higher in ball game players than in subjects not active in sports clubs (1%, 0.90 ± <0.01 vs. 0.89 ± <0.01 g·cm−2; p < 0.001), whereas leg BMD was lower in subjects active in other sports (2%, 0.85 ± 0.01 vs. 0.87 ± 0.01; p < 0.001) (Tables 1 and 2).
Boys had a 25% lower FMI (3.4 ± 0.1 vs. 4.6 ± 0.2 kg·m−2; p < 0.001) and an 11% higher lean body mass than girls (24.5 ± 0.2 vs. 22.1 ± 0.2 kg; p < 0.05). Whole-body BMD and BMC were higher in boys than in girls (3%, 0.90 ± 0.01 vs. 0.88 ± 0.01 g·cm−2; p < 0.05 and 6%, 1,217 ± 12 vs. 1,143 ± 14 g; p < 0.05), whereas no differences were observed in leg BMD and BMC between sexes (Table 1).
Discussion
The main findings of this large-scale study were that 8–10-year-old children involved in sports clubs with ball game activities have higher aerobic and musculoskeletal fitness, sprint performance, postural balance and coordination abilities, and lower FMI than children not active in sports clubs, whereas children involved in other types of sports clubs had less superior scores within these variables and poorer BMD scores. This aligns with studies showing that children active in sports clubs with ball game activities are more likely to meet the recommendations for daily physical activity (20), probably due to the high intensity of those activities compared with other types of physical activity (9).
It was found that YYIR1C performance was 61% (350 m) better in 8–10-year-old Danish children active in ball games than in children not active in sports clubs, which is slightly more than the performance differences observed in 9–11-year-old Portuguese girls (43%) and boys (57%) active in football clubs compared with children not active in football clubs (31,32), whereas a significant difference between those active in other sports and not active in sport was only found among boys (23%). In this study, children active in sports clubs also had lower HRsubmax after 2 minutes of YYIR1C (HRsubmax, 90 vs. 92% HRmax) and higher HRR (137 vs. 131 bpm), whereas children participating in ball games had lower HRsubmax than children participating in other sports (89 vs. 91% HRmax), indicating superior cardiovascular fitness in children active in sports clubs (2,8). This difference in cardiovascular fitness may well be related to the high amount of vigorous exercise conducted during training at many Danish team sport clubs, such as those where football and handball are played (20,27). Indeed, we recently observed that 9–11-year-old children had high HRs during school-based football, basketball, and unihockey training, along with a marked improvement in aerobic fitness, after only 6 weeks of twice-weekly 30-minute training sessions (9), and that 8–10-year-old schoolchildren had structural and functional myocardial adaptations after 10 weeks of 3 × 40 minutes of small-sided football games (22). Another important finding was that children active in sports clubs had a 16% lower FMI than those not active in sports clubs. This difference was significant for the girls (21%), but not for the boys (6%), and for girls participating in ball games compared with other sports. Interestingly, it has recently been observed that body fat is lower in male and female football club members than in non-members, but only in children older than 11 years, not in 9–10-year olds (31,32). Altogether, our observations show that 8–10-year-old Danish children active in sports clubs have a better cardiovascular health profile than those not active in sports clubs, and the results have important consequences in view of the well-known clustering of low physical activity with other cardiovascular risk factors (3,4,26,34).
In this study, sprint performance was 5.1% better in the children active in sports club with ball game activities than in those not active in sports clubs, which may be due in part to a nonsignificantly lower-body weight and a significantly higher lean body mass (2.7%). The difference in sprint performance may also be related to better motor function in the children active in sports clubs with ball game activities, as evidenced by 10% better postural balance and coordination skills. Previous cross-sectional studies have shown that the bone effects of sports participation are related to the type of sport, with team sports having marked positive associations with bone mineralization, but non–weight-bearing endurance sports like swimming and cycling having no or even negative associations (38,39). Moreover, the bone effects may be related to training frequency and number of years of training. Thus, in agreement with our findings, a Portuguese study has shown higher BMC and lower-limb BMD in children aged 9–10 years who play football 3 or more times a week, whereas other Portuguese studies have shown higher BMC and BMD in football players aged 11–15 years than in children not active in sports clubs (33) and markedly higher overall BMC and femur and hip BMD at the end of a 3-year follow-up study, despite no initial differences in bone mineralization, between children who played football and those who were not active in sports clubs at the age of 9–10 years.
This study showed that, irrespective of participation in organized leisure-time sports, boys had higher BMD and BMC than girls, which is in line with previous findings showing that boys play more outside during school breaks (19), probably exposing them to higher mechanical loads, which leads to stronger bones (19,21,36). In accordance with previous findings demonstrating higher maximal aerobic power, anaerobic performance and muscle strength in boys than in girls (12), the boys in our study sprinted faster and jumped further than the girls. However, the girls had better balance than the boys, which is in agreement with a number of other studies (11,16,25,28). It has been suggested that one reason for boys having inferior balance skills to girls may be a lower attention span in boys, which may interfere with the visual, vestibular, and proprioceptive system functions that are important for postural stability (25,35).
The lack of information on everyday life activities (e.g., active transport and leisure-time activities) is a limitation of the study. The children had all been exposed to 90 minutes of compulsory physical education during their school time, but apart from that their levels of physical activity were not evaluated. Another limitation of the study is the medium sample size, which only allowed for division of the children into 3 groups (ball games, other sports, and no sport), although it should be emphasized that the majority of 8–10-year-old Danish children who play ball games attend football or team handball activities that are known to be similar in intensity and organization (20).
In conclusion, this study showed that 8–10-year-old children engaged in sports club activity, especially ball games, have better physical fitness and a healthier body composition than those not active in sports clubs, as evidenced by superior aerobic and musculoskeletal fitness, sprint performance, postural balance, and coordination abilities, as well as markedly lower FMI. Moreover, the study demonstrated that 8–10-year-old girls have better postural balance but poorer aerobic fitness and sprint performance than boys of the same age as well as lower bone mineralization, suggesting that intervention studies including ball games aiming at enhancing physical performance levels, especially within the girls should be investigated.
Practical Applications
This article suggests that team sports played in sports clubs constitute intense and versatile training activities with a broad-spectrum positive impact on schoolchildren's health and highlights the importance of high-intensity physical activities in schools, such as team sports, where the least active children can be reached.
These results should be taken into consideration by parents, sports organizations, and politicians responsible for increasing children's participation in sports clubs. Moreover, the findings call for medium- and long-term exercise intervention studies in prepubertal children to evaluate effects on aerobic fitness, fat mass, muscle strength, and bone mineralization. It would be valuable if such studies focused on the quality of the training to investigate whether ball games are superior to other types of physical activity for improving fitness and health profiles in children.
Acknowledgments
The authors thank the participating pupils, teachers, and schools in Frederikssund and Copenhagen for their contribution, as well as Frederikssund Municipality for its collaboration and support. Special thanks to Henrik Pedersen and Therese Hornstrup for their excellent technical assistance. Also, special thanks to Ida Elkjær, Jan R. Jacobsen, and Henrik Oksholm for their assistance during testing sessions. In addition, this study was supported by the FIFA Medical Assessment and Research Center (F-MARC), the Danish Football Association (DBU), KFU, Aase and Ejnar Danielsen's Foundation, and the Augustinus Foundation. The Copenhagen Center for Team Sport and Health is supported by a grant from the Nordea Foundation (Nordea-fonden). The foundations did not participate in the analysis, interpretation, or writing of the paper.
References
- 1.Adam C, Klissouras V, Ravazzolo M, Renson R, Tuxworth W. EUROFIT: European test of physical fitness. Rome, Italy: Council of Europe, Committee for the Development of Sport, 1988: 10–70. [Google Scholar]
- 2.Ahler T, Bendiksen M, Krustrup P, Wedderkopp N. Aerobic fitness testing in 6- to 9-year-old children: Reliability and validity of a modified Yo-Yo IR1 test and the Andersen test. Eur J Appl Physiol 112: 871–876, 2012. [DOI] [PubMed] [Google Scholar]
- 3.Andersen LB, Bugge A, Dencker M, Eiberg S, El-Naaman B. The association between physical activity, physical fitness and development of metabolic disorders. Int J Pediatr Obes 6(Suppl 1): 29–34, 2011. [DOI] [PubMed] [Google Scholar]
- 4.Andersen LB, Harro M, Sardinha LB, Froberg K, Ekelund U, Brage S, Anderssen SA. Physical activity and clustered cardiovascular risk in children: A cross-sectional study (the European youth heart study). Lancet 368: 299–304, 2006. [DOI] [PubMed] [Google Scholar]
- 5.Andersen LB, Sardinha LB, Froberg K, Riddoch CJ, Page AS, Anderssen SA. Fitness, fatness and clustering of cardiovascular risk factors in children from Denmark, Estonia and Portugal: The European youth heart study. Int J Pediatr Obes 3(Suppl 1): 58–66, 2008. [DOI] [PubMed] [Google Scholar]
- 6.Baker JL, Olsen LW, Sørensen TI. Childhood body-mass index and the risk of coronary heart disease in adulthood. N Engl J Med 357: 2329–2337, 2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bencke J, Damsgaard R, Saekmose A, Jørgensen P, Jørgensen K, Klausen K. Anaerobic power and muscle strength characteristics of 11 years old elite and non-elite boys and girls from gymnastics, team handball, tennis and swimming. Scand J Med Sci Sports 12: 171–178, 2002. [DOI] [PubMed] [Google Scholar]
- 8.Bendiksen M, Ahler T, Clausen H, Wedderkopp N, Krustrup P. The use of Yo-Yo intermittent recovery level 1 and Andersen testing for fitness and maximal heart rate assessments of 6- to 10-year-old school children. J Strength Cond Res 27: 1583–1590, 2013. [DOI] [PubMed] [Google Scholar]
- 9.Bendiksen M, Williams CA, Hornstrup T, Clausen H, Kloppenborg J, Shumikhin D, Brito J, Horton J, Barene S, Jackman SR, Krustrup P. Heart rate response and fitness effects of various types of physical education for 8- to 9-year-old schoolchildren. Eur J Sport Sci 14: 861–869, 2014. [DOI] [PubMed] [Google Scholar]
- 10.Castro-Piñero J, Ortega FB, Artero EG, Girela-Rejón MJ, Mora J, Sjöström M, Ruiz JR. Assessing muscular strength in youth: Usefulness of standing long jump as a general index of muscular fitness. J Strength Cond Res 24: 1810–1817, 2010. [DOI] [PubMed] [Google Scholar]
- 11.Condon C, Cremin K. Static balance norms in children. Physiother Res Int 19: 1–7, 2014. [DOI] [PubMed] [Google Scholar]
- 12.Docherty D, Gaul C. Relationship of body size, physique, and composition to physical performance in young boys and girls. Int J Sports Med 12: 525–532, 1991. [DOI] [PubMed] [Google Scholar]
- 13.Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: Public-health crisis, common sense cure. Lancet 360: 473–482, 2002. [DOI] [PubMed] [Google Scholar]
- 14.Essendrop M, Hansen L, Klausen KJ. Balance and Co-ordination Abilities Related to Training in Youth Athletes. Children and Exercise XIX. Exeter, UK: Washington Singer Press, 1997: 161–166. [Google Scholar]
- 15.Faude O, Kerper O, Multhaupt M, Winter C, Beziel K, Junge A, et al. Football to tackle overweight in children. Scand J Med Sci Sports 20(Suppl 1): 103–110, 2010. [DOI] [PubMed] [Google Scholar]
- 16.Geldhof E, Cardon G, De Bourdeaudhuij I, Danneels L, Coorevits P, Vanderstraeten G, De Clercq D. Static and dynamic standing balance: Test-retest reliability and reference values in 9 to 10 year old children. Eur J Pediatrics 165: 779–786, 2006. [DOI] [PubMed] [Google Scholar]
- 17.Hansen PR, Andersen LJ, Rebelo AN, Brito J, Hornstrup T, Schmidt JF, Jackman SR, Mota J, Rêgo C, Oliveira J, Seabra A, Krustrup P. Cardiovascular effects of 3 months of football training in overweight children examined by comprehensive echocardiography: A pilot study. J Sports Sci 31: 1432–1440, 2013. [DOI] [PubMed] [Google Scholar]
- 18.Hansen HS, Froberg K, Hyldebrandt N, Nielsen JR. A controlled study of eight months of physical training and reduction of blood pressure in children: The Odense schoolchild study. BMJ 303: 682–685, 1991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hasselstrøm H, Karlsson KM, Hansen SE, Grønfeldt V, Froberg K, Andersen LB. Sex differences in bone size and bone mineral density exist before puberty. The Copenhagen School Child Intervention Study (CoSCIS). Calci Tissue Int 79: 7–14, 2006. [DOI] [PubMed] [Google Scholar]
- 20.Hebert JJ, Moller NC, Andersen LB, Wedderkopp N. Organized sport participation is associated with higher levels of overall health-related physical activity in children (CHAMPS study-DK). PLoS One 10: e0134621, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Khan K. Physical Activity and Bone Health. Human Kinetics, 2001. [Google Scholar]
- 22.Krustrup P, Hansen PR, Nielsen CM, Larsen MN, Randers MB, Manniche V, Hansen L, Dvorak J, Bangsbo J. Structural and functional cardiac adaptations to a 10-week school-based football intervention for 9-10-year-old children. Scand J Med Sci Sports 24(Suppl 1): 4–9, 2014. [DOI] [PubMed] [Google Scholar]
- 23.Malina RM. Tracking of physical activity and physical fitness across the lifespan. Res Q Exerc Sport 67(Suppl 3):S48–S57, 1996. [DOI] [PubMed] [Google Scholar]
- 24.Margulies L, Horlick M, Thornton JC, Wang J, Ioannidou E, Heymsfield SB. Reproducibility of pediatric whole body bone and body composition measures by dual-energy X-ray absorptiometry using the GE Lunar Prodigy. J Clin Densitom 8: 298–304, 2005. [DOI] [PubMed] [Google Scholar]
- 25.Mickle KJ, Munro BJ, Steele JR. Gender and age affect balance performance in primary school-aged children. J Sci Med Sport 14: 243–248, 2011. [DOI] [PubMed] [Google Scholar]
- 26.Nadeau KJ, Maahs DM, Daniels SR, Eckel RH. Childhood obesity and cardiovascular disease: Links and prevention strategies. Nat Rev Cardiol 8: 513–525, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nielsen G, Bugge A, Andersen LB. The influence of club football on children's daily physical activity. Soccer Soc 1–13, 2015. [Google Scholar]
- 28.Nolan L, Grigorenko A, Thorstensson A. Balance control: Sex and age differences in 9- to 16-year-olds. Dev Med Child Neurol 47: 449–454, 2005. [DOI] [PubMed] [Google Scholar]
- 29.Ortega FB, Artero EG, Ruiz JR, Vicente-Rodriguez G, Bergman P, Hagströmer M, Ottevaere C, Nagy E, Konsta O, Rey-López JP, Polito A, Dietrich S, Plada M, Béghin L, Manios Y, Sjöström M, Castillo MJ; HELENA Study Group. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study. Int J Obesity 32: S49–S57, 2008. [DOI] [PubMed] [Google Scholar]
- 30.Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 16: 3–63, 2006. [DOI] [PubMed] [Google Scholar]
- 31.Povoas SC, Castagna C, da Costa Soares JM, Silva P, Coelho-e-Silva M, Matos F, Krustrup P. Reliability and construct validity of Yo-Yo tests in untrained and soccer-trained schoolgirls aged 9–16. Pediatr Exerc Sci 28: 321–330, 2016. [DOI] [PubMed] [Google Scholar]
- 32.Póvoas SC, Castagna C, Soares JM, Silva PM, Lopes MV, Krustrup P. Reliability and validity of Yo-Yo tests in 9-to 16-year-old football players and matched non-sports active schoolboys. Eur J Sport Sci 16: 755–763, 2016. [DOI] [PubMed] [Google Scholar]
- 33.Seabra A, Marques E, Brito J, Krustrup P, Abreu S, Oliveira J, et al. Muscle strength and soccer practice as major determinants of bone mineral density in adolescents. Joint Bone Spine 79: 403–408, 2012. [DOI] [PubMed] [Google Scholar]
- 34.Søltoft F, Hammer M, Kragh N. The association of body mass index and health-related quality of life in the general population: Data from the 2003 health survey of England. Qual Life Res 18: 1293–1299, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Steindl R, Kunz K, Schrott-Fischer A, Scholtz A. Effect of age and sex on maturation of sensory systems and balance control. Dev Med Child Neurol 48: 477–482, 2006. [DOI] [PubMed] [Google Scholar]
- 36.Sundberg M, Gärdsell P, Johnell O, Karlsson M, Ornstein E, Sandstedt B, Sernbo I. Physical activity increases bone size in prepubertal boys and bone mass in prepubertal girls: A combined cross-sectional and 3-year longitudinal study. Calci Tissue Int 71: 406–415, 2002. [DOI] [PubMed] [Google Scholar]
- 37.Vicente-Rodriguez G. Enhanced bone mass and physical fitness in prepubescent footballers. Bone 33: 853–859, 2003. [DOI] [PubMed] [Google Scholar]
- 38.Vicente-Rodriguez G, Ara I, Perez-Gomez J, Dorado C, Calbet JA. Muscular development and physical activity as major determinants of femoral bone mass acquisition during growth. Br J Sports Med 39: 611–616, 2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Vicente-Rodriguez G, Ara I, Perez-Gomez J, Serrano-Sanchez JA, Dorado C, Calbet JA. High femoral bone mineral density accretion in prepubertal soccer players. Med Sci Sports Exerc 36: 1789–1795, 2004. [DOI] [PubMed] [Google Scholar]
- 40.World Health Organization. World Health Organization Global recommendations on physical activity for health. Geneva, Switzerland: WHO, 2010. Available at: http://apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf. [PubMed] [Google Scholar]
- 41.Zahner L, Puder JJ, Roth R, Schmid M, Guldimann R, Pühse U, Knöpfli M, Braun-Fahrländer C, Marti B, Kriemler S. A school-based physical activity program to improve health and fitness in children aged 6–13 years (“Kinder-Sportstudie KISS”): Study design of a randomized controlled trial [ISRCTN15360785]. BMC Public Health 6: 1, 2006. [DOI] [PMC free article] [PubMed] [Google Scholar]