

Supplemental Digital Content is available in the text
Keywords: cohort studies, meta-analysis, night work, prostate cancer, shift work
Abstract
Background:
Epidemiology studies suggested that shift work or night work may be linked to prostate cancer (PCa); the relationship, however, remains controversy.
Methods:
PubMed, ScienceDirect, and Embase (Ovid) databases were searched before (started from the building of the databases) February 4, 2017 for eligible cohort studies. We pooled the evidence included by a random- or fixed-effect model, according to the heterogeneity. A predefined subgroup analysis was conducted to see the potential discrepancy between groups. Sensitivity analysis was used to test whether our results were stale.
Results:
Nine cohort studies were eligible for meta-analysis with 2,570,790 male subjects. Our meta-analysis showed that, under the fixed-effect model, the pooled relevant risk (RR) of PCa was 1.05 (95% confidence interval [CI]: 1.00, 1.11; P = .06; I2 = 24.00%) for men who had ever engaged in night shift work; and under the random-effect model, the pooled RR was 1.08 (0.99, 1.17; P = .08; I2 = 24.00%). Subgroup analysis showed the RR of PCa among males in western countries was 1.05 (95% CI: 0.99, 1.11; P = .09; I2 = 0.00%), while among Asian countries it was 2.45 (95% CI: 1.19, 5.04; P = .02; I2 = 0.00%); and the RR was 1.04 (95% CI: 0.95, 1.14; P = .40; I2 = 29.20%) for the high-quality group compared with 1.21 (95% CI: 1.03, 1.41; P = .02; I2 = 0.00%) for the moderate/low-quality group. Sensitivity analysis showed robust results.
Conclusions:
Based on the current evidence of cohort studies, we found no obvious association between night shift work and PCa. However, our subgroup analysis suggests that night shift work may increase the risk of PCa in Asian men. Some evidence of a small study effect was observed in this meta-analysis.
1. Introduction
Prostate cancer (PCa) is the most common form of cancer for men in developed countries and the 4th most common cancer in developing countries.[1] In 2017, the American Cancer Society estimated that 161,360 new cases of PCa will be diagnosed, of which 26,730 men will die from PCa in the United States.[2] Although the incidence of PCa dropped more than 10% from 2010 to 2013 each year, PCa remains the leader in both occurrence and death in the United States for cancer.[1]
Working status has been linked closely to health. Shift work is very common among office workers, and is considered the main cause of circadian rhythm disorder. According to American and European surveys,[3] approximately between 15% and 30% of adult workers are engaged in different degrees of shift work, with 32% to 36% of shift workers falling asleep at work more than once a week.[4]
Several epidemiology studies suggest that a disrupted circadian rhythm may increase the risk of PCa.[5,6] In a large Japanese cohort study, Kubo et al[7] revealed that rotating shift work is significantly associated with an increased risk of PCa. Several case–control studies also found that shift work or night work may be linked to an increased PCa risk,[8–10] while some other cohort studies showed no association.[11,12] An earlier meta-analysis by Rao et al[13] summarized 8 observational studies and found that night shift work was associated with a higher risk of PCa. However, the substantial heterogeneity and potential recall bias from case–control studies warrants caution about their conclusions.
In this study, the evidence was updated, based on cohort studies, to verify whether night shift work increases the risk of PCa. This meta-analysis was designed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement.[14]
2. Methods
2.1. Literature search
A comprehensive literature search was conducted based on PubMed, ScienceDirect, and Embase (Ovid). These databases were searched before (started from the building of the databases) February 4, 2017 by 2 independent reviewers, without language limitation. We also screened the reference lists of relevant studies manually. We used the following search terms to develop the strategy: sleep disorders, shift work, shift work, night work, rotate shift work, night shift work, prostate cancer, cancer, prostate tumor, and prostate neoplasm. The detailed search strategies for the 3 databases are presented in a supplementary file (Table S1).
2.2. Inclusion criteria
The inclusion criteria was developed ex ante, and eligible studies were included if they satisfied the following criteria: based on prospective or retrospective cohort design; the exposure was to shift work, night work, or occupation related with shift work (e.g., airline crew)[12]; the endpoint was any stage of PCa, and only primary cancer was considered; the potential population was male; and peer-reviewed publications and available data could be extracted. Two authors screened the literature and any disagreement was resolved by discussion. Conference abstracts, gray literature, and commentary were excluded from the search.
2.3. Data extraction and transformation
Data items were extracted by 2 authors with the following information: first author's name, publication year, region, population information (e.g., mean age at entry), follow-up years, exposure, endpoint, and effect sizes (relevant risk, RR) with 95% confidence interval (CI). We only extracted the multivariable controlled RR to minimize potential bias. The 2 authors checked each other's data after the extraction process.
Some prospective studies used the standard incidence ratio (SIR) as the measurement of risk for PCa. The relationship between SIR and RR can be expressed as follows[15]:
 |
where PE is the expected prevalence of PCa, we considered SIR as similarly equal to RR, since the expected prevalence of PCa is very low.[2]
2.4. Quality assessment
For included studies, we used the Newcastle–Ottawa Scale (NOS) to assess quality.[16] The NOS checklist contains 9 items for cohort studies, which evaluate the design quality and the implementation approach of original studies. We considered a study to be of high quality when it met 7 or more of the recommended items.
2.5. Statistical analysis
We used RR to reflect the risk of PCa when exposed to night shift work. The RRs were pooled across the studies by a random- or fixed-effect model, according to the heterogeneity tested by I2 statistics. Briefly, the I2 statistics range from 0% to 100% and the value of I2 ≥ 50 suggests substantial heterogeneity and that a random-effect model would be selected. Likewise, if I2 < 50, the fixed-effect model would be selected. The inverse variance method was used to combine the effect sizes.
We also conducted a predefined subgroup analysis by country, work type, study quality, mean age at entry, effect size, and follow-up years to determine the potential discrepancy between these subgroups. A one-by-one-omitted sensitivity analysis was conducted to confirm whether our results were stable. We used the Egger test to assess publication bias. All the statistical analyses were accomplished by Stata 12.0 software (Stata Corporation, College Station, TX). Ethical approval was not necessary due to the nature of meta-analysis.
3. Results
In total, 1573 primary records were retrieved from the databases, 308 of which were duplicates. The title and abstract were screened and 1185 publications were rejected as being not relevant. Therefore, 80 articles remained and required further screening by reading the texts in full. Of these, 71 studies did not meet the criteria and were subsequently excluded. Finally, 9 cohort studies were eligible for meta-analysis,[7,11,12,17–22] involving a total of 2,570,790 male subjects (Fig. 1).
Figure 1.
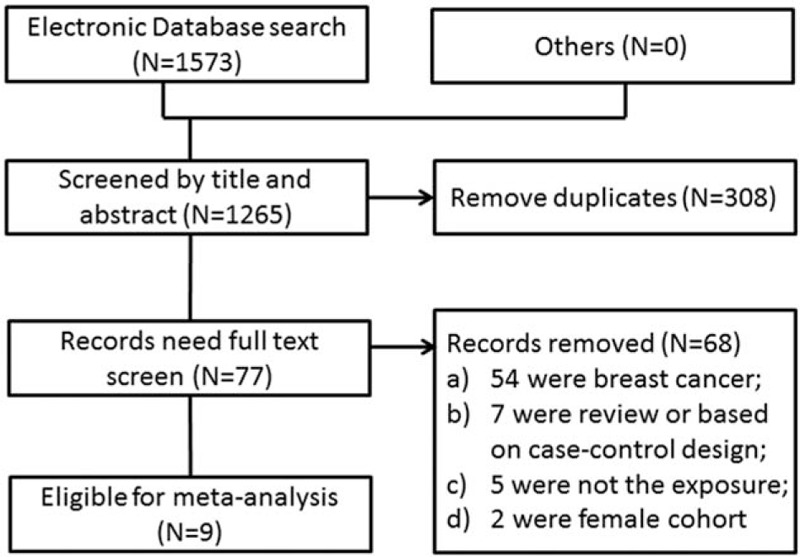
The flow diagram of the literature inclusion.
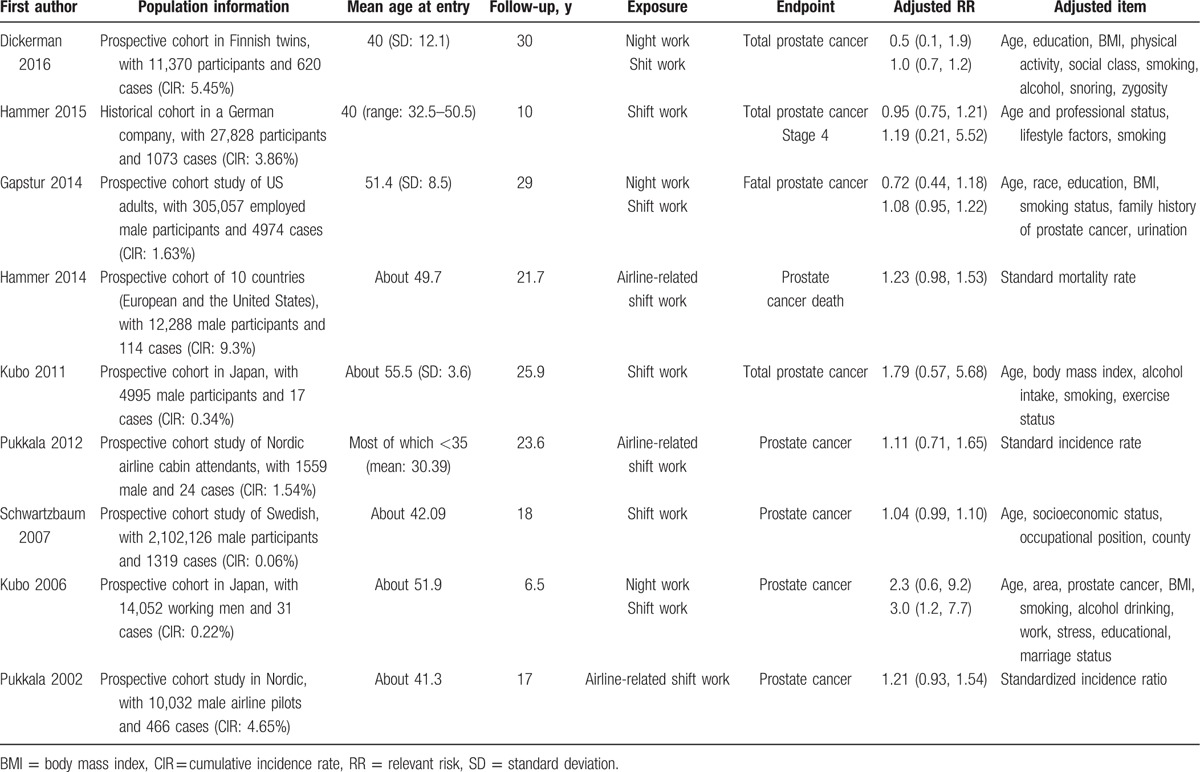
The mean age at entry of these subjects varied from 30.39 to 55.5 years, with an average value of 44.69 years. Among the 9 cohorts, 8 studies were based on a prospective design and 1 study was based on a historical design. Five studies were conducted in European counties, 2 studies were conducted in the United States, and 2 studies were conducted in Asian countries. The mean follow-up was 20.19 years, ranging from 6.5 to 30 years (Table 1).
Table 1.
Basic characters of included studies.
Regarding the quality of the included studies, we deemed 6 studies to be of high quality, while 3 studies[18,19,22] were deemed to be of moderate to low quality. The mean quality score was 7, and the range was from 5 to 9 (Table S2).
3.1. Night shift work and risk of PCa
Nine studies investigate the relationship between night shift work and the risk of PCa. Figure 2A and B presents the pooled results based on a fixed- and random-effect model. Our meta-analysis showed that, under the fixed-effect model, the pooled RR of PCa was 1.05 (95% CI: 1.00, 1.11; P = .06; I2 = 24.00%) for men who had ever engaged in night shift work; and under the random-effect model, the pooled RR was 1.08 (0.99, 1.17; P = .08; I2 = 24.00%).
Figure 2.
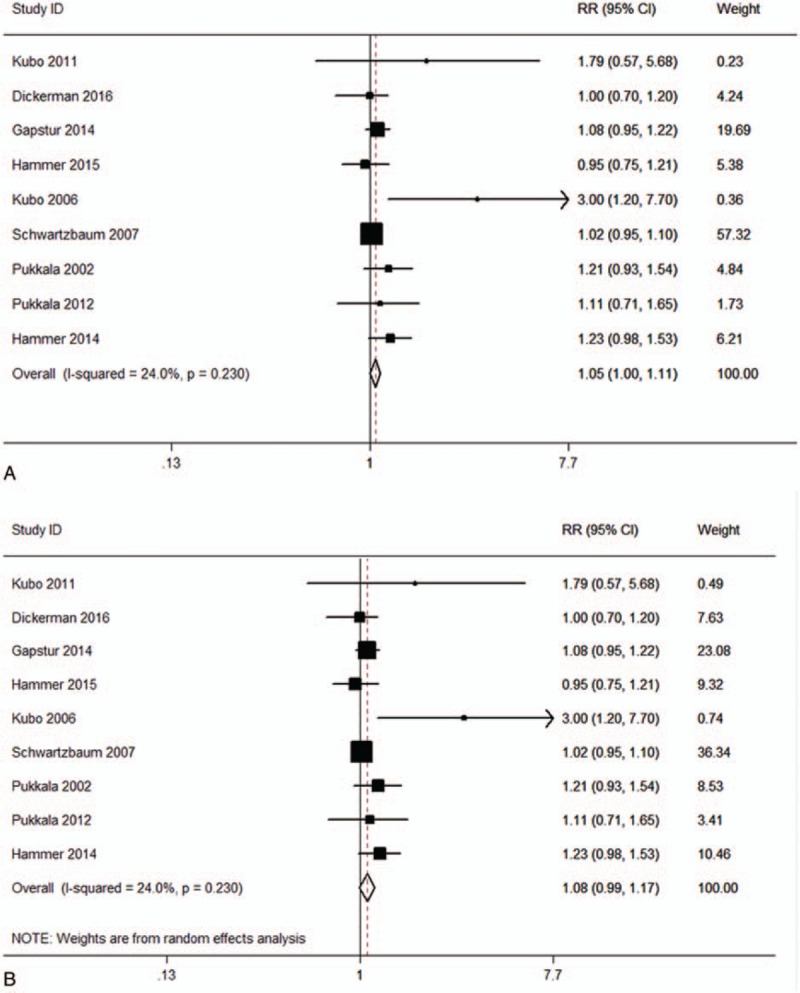
The relationship between night shift work and the risk of prostate cancer: (A) fixed-effect model and (B) random-effect model.
3.2. Subgroup analysis
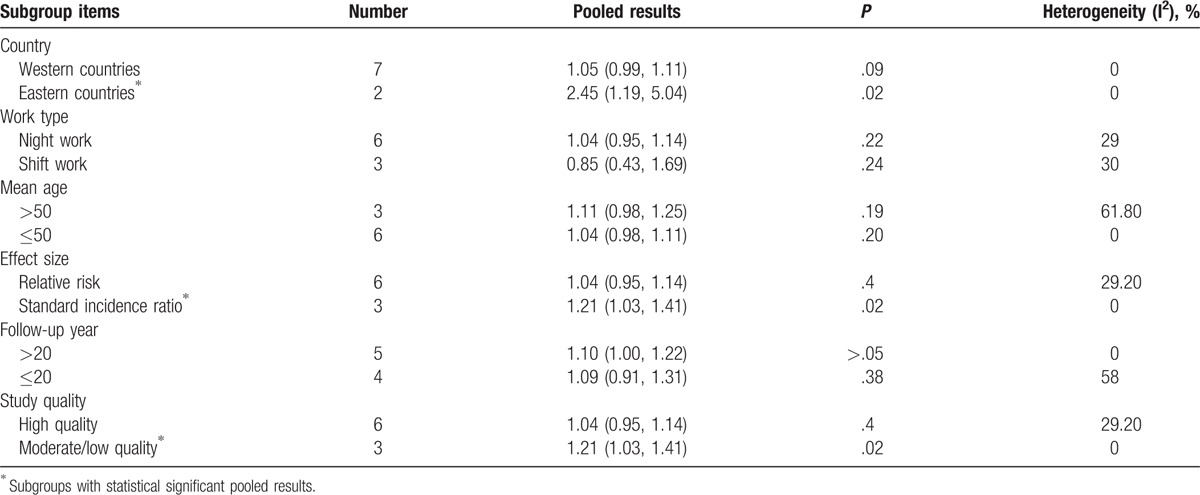
Our subgroup analysis was conducted by country (western countries and Asian countries), work type (shift work and night work), mean age at entry (>50 and ≤50 years), effect size (RR and SIR), follow-up years (>20 and ≤20 years), and study quality (high quality vs. moderate or low). Table 2 presents the results. Our subgroup analysis showed that, when grouped by country, the RR of PCa among males in western countries was 1.05 (95% CI: 0.99, 1.11; P = .09; I2 = 0.00%), while among Asian countries it was 2.45 (95% CI: 1.19, 5.04; P = .02; I2 = 0.00%). When grouped by effect size, the RR was 1.04 (95% CI: 0.95, 1.14; P = .40; I2 = 29.20%) for the RR group compared with 1.21 (95% CI: 1.03, 1.41; P = .02; I2 = 0.00%) for the SIR group. When grouped by study quality, the RR was 1.04 (95% CI: 0.95, 1.14; P = .40; I2 = 29.20%) for the high-quality group compared with 1.21 (95% CI: 1.03, 1.41; P = .02; I2 = 0.00%) for the moderate/low-quality group. Other means of subgroup analysis showed no obvious discrepancy between subgroups.
Table 2.
Subgroup analysis.
3.3. Sensitivity analysis and publication bias
Our one-by-one-omitted sensitivity analysis showed that the whole pooled result was stable (Fig. 3). The Egger test showed some evidence of publication bias: the P value of bias was .05 (Fig. 4). A trim and fill analysis by both the fixed-effect model (RR = 1.04; 95% CI: 0.98, 1.10) and the random-effect model (RR = 1.05; 95% CI: 0.95, 1.15) showed that our results were stable (Fig. 5).
Figure 3.
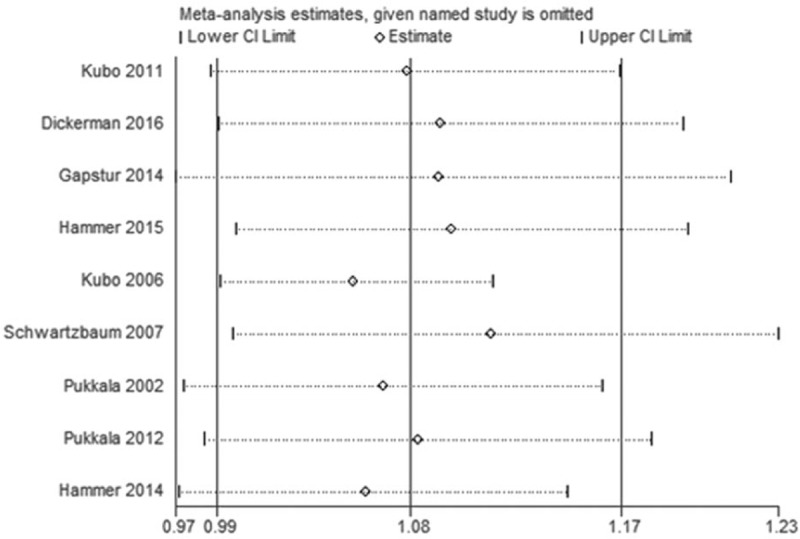
One-by-one-omitted sensitivity analyses.
Figure 4.
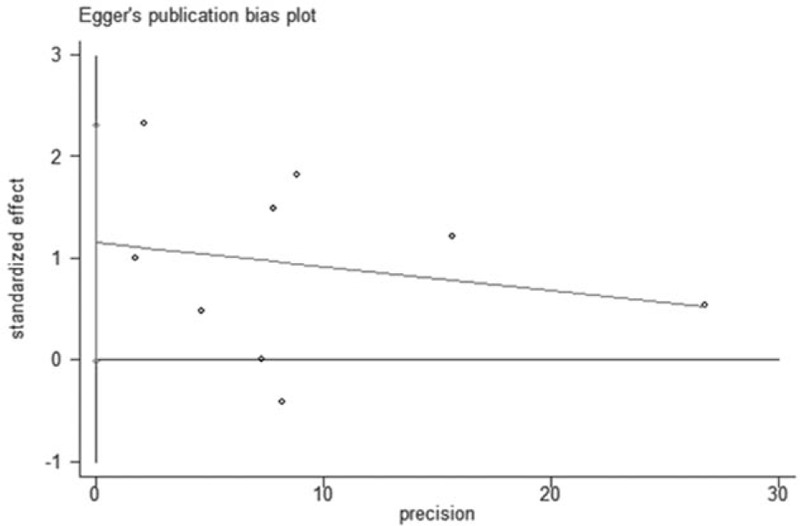
Publication bias by Egger test.
Figure 5.
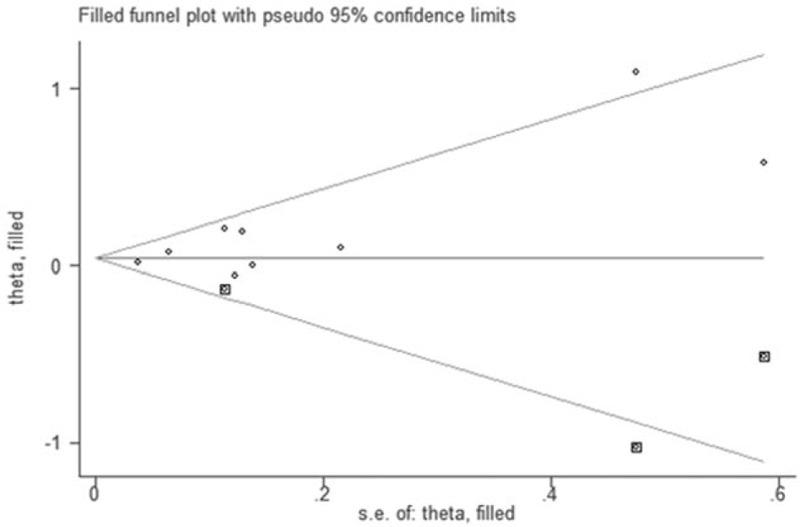
Filled funnel plot by trill and fill method.
4. Discussion
In our meta-analysis, we reviewed the evidence in respect of night shift work and the risk of PCa, based on cohort studies. We found that, based on our pooled results, night shift work is not associated with an increased risk of PCa for the total population, regardless of mean age, work type, or follow-up years. However, in our subgroup analysis, we found that, among males in Asian countries, night shift work may increase the risk of PCa, but this effect was not observed in western countries.
Interestingly, our subgroup analysis, based on study quality, reveals that for high-quality studies, the pooled results were not statistically significant; while for moderate- or low-quality studies, the pooled results showed a significant increase in PCa risk. This suggests that our meta-analysis may have been affected by the “small study effect.” The Egger test for publication bias also supports this hypothesis. By a series of additional analyses (e.g., subgroup analysis, sensitivity analysis, and trim and fill analysis) we provided evidence to suggest that night shift work is not linked to PCa risk in the total population.
Some evidence of publication bias was detected, and the small-study effect may have influenced our results. In our subgroup analysis, we found the pooled results of moderate- or low-quality studies tended to be positively associated with PCa risk. When pooled, the whole effect tended to trend positively. However, our overall pooled results were still negative, which indirectly demonstrates that night shift work may not increase the risk of PCa in the total population. The trim and fill analysis presenting stable results also supported our results.
A previous meta-analysis by Rao et al,[13] based on 5 cohorts and 3 case–controls, concluded that night shift work may increase the risk of PCa and there may be a dose–response effect. However, their pooled results showed substantial heterogeneity between studies. The 3 case–control studies they included may have also introduced potential bias since these are based on historical design. In this meta-analysis, we only pooled cohort studies, conducted a series of additional analyses, and found that night shift work may increase the risk of PCa among Asian males only.
It is not clear what may underlie these differences. One potential explanation is that the different effect of night shift work on Asian men compared with European and American men may be due to differing lifestyles and genotypes. Another possibility for the differences may be due to the varying types of jobs undertaken by the subjects. However, further research is required to investigate these differences.
There were several strengths in our meta-analysis. First, only cohort studies were included, with no case–control studies, which reduced bias.[23] Second, we conducted a predefined subgroup analysis to reveal any potential discrepancy among groups, avoiding selection bias.[24] Third, we conducted a series of additional analyses that all supported our main findings. However, there were still several limitations to our study. First, the number of included studies was relatively small. Although the sample size was sufficient, only part of the sample was researched, which may not be representative of the total population. Second, in several included studies, eligible subjects were all from a certain company, lowering the representativeness of the sample. Third, the small study effect may have positively influenced our results. The real effect may be more conservative than the current pooled effect.[25] Fourth, for subgroup analysis, only 2 studies involved Asian men. Although the pooled effect in this group was significant, the results may be at risk of a type II error due to the limited study numbers.[26]
5. Conclusion
Based on the current evidence of cohort studies, we found no obvious association between night shift work and PCa. However, our subgroup analysis suggests that night shift work may increase the risk of PCa in Asian men. Some evidence of a small study effect was observed in this meta-analysis.
Supplementary Material
Acknowledgment
The authors thank Dr. X.H. Wang for his previous assistant on this meta-analysis.
Footnotes
Abbreviations: CI = confidence interval, NOS = Newcastle–Ottawa Scale, PCa = prostate cancer, RR = relevant risk, SIR = standard incidence ratio.
Study design, literature search, data, and drafting the manuscript: H-BD; statistical analysis: H-BD and BK-Y; revise the manuscript and check the data and re-analysis the data: BK-Y, LW-H, YF-S.
The authors have no funding and conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Arnold M, Karim-Kos HE, Coebergh JW, et al. Recent trends in incidence of five common cancers in 26 European countries since 1988: analysis of the European Cancer Observatory. Eur J Cancer 2015;51:1164–87. [DOI] [PubMed] [Google Scholar]
- [2].Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin 2017;67:7–30. [DOI] [PubMed] [Google Scholar]
- [3].Boivin DB, Boudreau P. Impacts of shift work on sleep and circadian rhythms. Pathol Biol (Paris) 2014;62:292–301. [DOI] [PubMed] [Google Scholar]
- [4].Rajaratnam SM, Howard ME, Grunstein RR. Sleep loss and circadian disruption in shift work: health burden and management. Med J Aust 2013;199:S11–5. [DOI] [PubMed] [Google Scholar]
- [5].Sigurdardottir LG, Markt SC, Rider JR, et al. Urinary melatonin levels, sleep disruption, and risk of prostate cancer in elderly men. Eur Urol 2015;67:191–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Sigurdardottir LG, Valdimarsdottir UA, Mucci LA, et al. Sleep disruption among older men and risk of prostate cancer. Cancer Epidemiol Biomarkers Prev 2013;22:872–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Kubo T, Ozasa K, Mikami K, et al. Prospective cohort study of the risk of prostate cancer among rotating-shift workers: findings from the Japan collaborative cohort study. Am J Epidemiol 2006;164:549–55. [DOI] [PubMed] [Google Scholar]
- [8].Parent ME, El-Zein M, Rousseau MC, et al. Night work and the risk of cancer among men. Am J Epidemiol 2012;176:751–9. [DOI] [PubMed] [Google Scholar]
- [9].Papantoniou K, Castaño-Vinyals G, Espinosa A, et al. Night shift work, chronotype and prostate cancer risk in the MCC-Spain case-control study. Int J Cancer 2015;137:1147–57. [DOI] [PubMed] [Google Scholar]
- [10].Conlon M, Lightfoot N, Kreiger N. Rotating shift work and risk of prostate cancer. Epidemiology 2007;18:182–3. [DOI] [PubMed] [Google Scholar]
- [11].Dickerman BA, Markt SC, Koskenvuo M, et al. Sleep disruption, chronotype, shift work, and prostate cancer risk and mortality: a 30-year prospective cohort study of Finnish twins. Cancer Causes Control 2016;27:1361–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Hammer GP, Emrich K, Nasterlack M, et al. Shift work and prostate cancer incidence in industrial workers: a historical cohort study in a German Chemical Company. Dtsch Arztebl Int 2015;112:463–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Rao D, Yu H, Bai Y, et al. Does night-shift work increase the risk of prostate cancer? A systematic review and meta-analysis. Onco Targets Ther 2015;8:2817–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Chaturvedi AK, Mbulaiteye SM, Engels EA. Underestimation of relative risks by standardized incidence ratios for AIDS-related cancers. Ann Epidemiol 2008;18:230–4. [DOI] [PubMed] [Google Scholar]
- [16].Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses, 2011. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed November 2016. [Google Scholar]
- [17].Gapstur SM, Diver WR, Stevens VL, et al. Work schedule, sleep duration, insomnia, and risk of fatal prostate cancer. Am J Prev Med 2014;46(suppl 1):S26–33. [DOI] [PubMed] [Google Scholar]
- [18].Hammer GP, Auvinen A, De Stavola BL, et al. Mortality from cancer and other causes in commercial airline crews: a joint analysis of cohorts from 10 countries. Occup Environ Med 2014;71:313–22. [DOI] [PubMed] [Google Scholar]
- [19].Pukkala E, Helminen M, Haldorsen T, et al. Cancer incidence among Nordic airline cabin crew. Int J Cancer 2012;131:2886–97. [DOI] [PubMed] [Google Scholar]
- [20].Schwartzbaum J, Ahlbom A, Feychting M. Cohort study of cancer risk among male and female shift workers. Scand J Work Environ Health 2007;33:336–43. [DOI] [PubMed] [Google Scholar]
- [21].Kubo T, Oyama I, Nakamura T, et al. Industry-based retrospective cohort study of the risk of prostate cancer among rotating-shift workers. Int J Urol 2011;18:206–11. [DOI] [PubMed] [Google Scholar]
- [22].Pukkala E, Aspholm R, Auvinen A, et al. Incidence of cancer among Nordic airline pilots over five decades: occupational cohort study. BMJ 2002;325:567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Tam CC, Higgins CD, Rodrigues LC. Effect of reminders on mitigating participation bias in a case-control study. BMC Med Res Methodol 2011;11:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. http://www.cochrane-handbook.org. Accessed November 2016. [Google Scholar]
- [25].Sterne JAC, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol 2000;53:1119–29. [DOI] [PubMed] [Google Scholar]
- [26].Delorme P, de Micheaux PL, Liquet B, et al. Type-II generalized family-wise error rate formulas with application to sample size determination. Stat Med 2016;35:2687–714. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.