

Abstract
Background:
Whether early enteral nutrition (EEN) administration is more beneficial than delayed enteral nutrition (DEN) for patients with acute pancreatitis remains controversial.
Methods:
This meta-analysis aimed to pool all relevant articles to evaluate the effects of EEN within 48 hours versus DEN beyond 48 hours on the clinical outcomes of patients with acute pancreatitis. We searched PubMed, Scopus, Embase, and Web of Science for all relevant studies and extracted the data concerning basic characteristics, complications, and mortality. We calculated the pooled risk ratio (RR), weighted mean difference, and the corresponding 95% confidential interval (95% CI) using STATA 12.0.
Results:
For complications, the pooled analysis showed that EEN was related to a reduced risk of multiple organ failure (RR = 0.67, 95% CI 0.46–0.99, P = .04), but not for necrotizing pancreatitis (RR = 0.95, 95% CI 0.81–1.12, P = .57). There was a tendency for decreased systemic inflammatory response syndrome in the EEN group, but the trend was not significant (RR = 0.85, 95% CI 0.71–1.02, P = .09). For mortality, no significant difference was found between the EEN and DEN groups (RR = 0.78, 95% CI 0.27–2.24, P = .64).
Conclusion:
EEN within 48 hours is superior to DEN beyond 48 hours for patients with acute pancreatitis; however, more studies are required to verify this conclusion.
Keywords: acute pancreatitis, enteral nutrition, meta-analysis, multiple organ failure
1. Introduction
Acute pancreatitis is one of the most common diseases leading to hospital or intensive care unit (ICU) admission because of the risk of increased systemic inflammatory response syndrome (SIRS), multiple organ failure, septic organ dysfunction, local complications, and other ailments.[1–3]
Nutritional support is very important for patients with acute pancreatitis, especially for those with severe acute pancreatitis.[4] Infected pancreatic necrosis is associated with a mortality of 15%. Damage to the gut barrier in the early phase of acute pancreatitis accounts for the initiation of SIRS, sepsis, and infected pancreatic necrosis.[5,6] Thirty-three percent of pancreas infections take place in the first 24 hours and 75% between 48 and 96 hours.[7] Therefore, not only the gut barrier but also nutrition timing is crucial for patients with acute pancreatitis. Many trials have found that enteral nutrition was better at maintaining the gut barrier and decreasing bacterial translocation.[8] Recently, a series of clinical trials stressed the importance of early enteral nutrition (EEN) compared with delayed enteral nutrition (DEN).[9,10] In a meta-analysis including 11 studies, although EEN was associated with a lower rate of pancreatic infection, mortality, and organ failure than total parenteral nutrition (TPN) and DEN, there is still no sufficient and direct proof to support EEN being preferable to DEN for patients with acute pancreatitis.[11] That meta-analysis only performed comparative analyses between the EEN group and DEN plus PN groups; however, there was no separate comparison between the EEN group and DEN group.[11]
To explore whether EEN is more beneficial to patients with acute pancreatitis than DEN, we searched for eligible studies that reported the clinical outcomes of EEN and DEN groups and performed aggregating analyses.
2. Patients and methods
2.1. Search strategies
We searched for relevant studies concerning early EN in PubMed, Web of Science, Embase, and Scopus from inception to August 2016. The following terms and strategies were used to search in the databases: “Enteral nutrition OR tube feeding OR nasogastric OR nasojejunal” and “Randomized controlled trial OR RCT OR clinical trial OR trial” and “Pancreatitis.” During the search, no language limits were set. To avoid missing qualified trials, we also scrutinized the reference lists of relevant meta-analyses and reviews. All analyses were based on previous published studies and no ethical approval and patient consent were required
2.2. Selection criteria
Studies included in this meta-analysis had to fulfill the following criteria:
-
(1)
Randomized comparative trials (RCTs) or retrospective trails with available information;
-
(2)
Consecutive patients with acute pancreatitis;
-
(3)
EEN within 48 hours and DEN beyond 48 hours.
Studies were excluded if they were
-
(1)
Duplicate publications;
-
(2)
case reports, reviews, meta-analyses, or guidelines;
-
(3)
contained no available data for this meta-analysis.
2.3. Data extraction and management
The following information was extracted from the included trials: first author, year of publication, start time and route of EN administration, severity of acute pancreatitis, number of participants. Basic data about gender, age, APACHE II score, and C-reactive protein (CRP, mg/L) were extracted and analyzed. To compare the clinical outcomes of the EEN and DEN groups, data on SIRS, multiple organ failure, and mortality were extracted. We used a formula adopted by previous studies to acquire the mean and standard deviation.[12,13]
2.4. Quality assessment and bias assessment
The quality of the included RCTs was assessed according to the methodological criteria of the Cochrane Handbook for Systematic Reviews of Interventions, and the quality of retrospective researches was assessed by the Newcastle–Ottawa Scale (NOS). Begg test was used to assess the publication bias, which was based on the risk ratios (RRs) of mortality and necrotizing pancreatitis.
2.5. Statistical analysis
All analyses were performed using STATA 12.0 (Stata Corporation, College Station, Texas). Data of binary outcomes extracted from original studies were pooled to estimate the RRs and corresponding 95% confidence intervals (CIs), and continuous outcomes were pooled to estimate overall weighted mean difference and corresponding 95% CIs. The I2 test and Q test were used to measure statistical heterogeneity among the included studies and P < 0.1 or I2 > 50% indicated significant heterogeneity. A random-effect model was used for statistics with heterogeneity, otherwise a fixed-effect model was applied. A P < .05 in the Z test was considered as a significant difference for the pooled estimates. The potential publication bias was assessed by Begg test and a P <.05 was considered as a statistically significant publication bias.
3. Results
3.1. Included trials characteristics and quality assessment
A total of 1424 articles were obtained from PubMed, Scopus, Embase, and Web of Science. The flow diagram for searching and screening of eligible studies is shown in Fig. 1. Finally, 6 articles including enrolled 1007 patients were included in this meta-analysis, comprising 2 retrospective studies and 4 RCTs.[9,10,14–17] The characteristics of the included studies are illustrated in Table 1. The quality of the included RCTs, as assessed by the Cochrane Handbook for Systematic Reviews of Interventions, is displayed in Table 2, and quality assessment of the included retrospective trials, as assessed by the Newcastle–Ottawa Scale, is summarized in Table 3.
Figure 1.
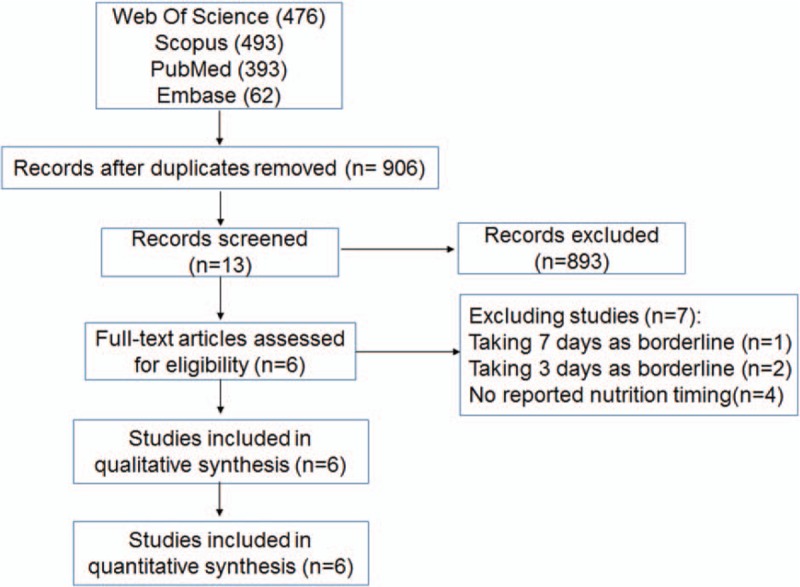
PRISMA flow diagram of the article screening process for the meta-analysis.
Table 1.
Included studies comparing EEN with DEN.

Table 2.
Quality assessment of included studies: quality of the included RCTs.

Table 3.
Quality assessment of included studies: quality of the included retrospective studies.

3.2. Basic characteristics comparison between EEN and DEN
To explore whether the baseline characteristics were similar, we aggregated the available data on age, gender, APACHE II score, and CRP (mg/L). Our results showed no differences between the EEN and DEN groups in terms of these characteristics (Figs. 2 and 3).
Figure 2.
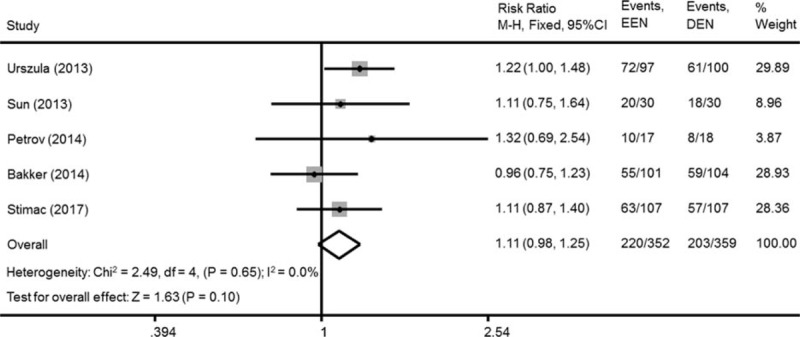
Gender of the patients at baseline (fixed-effect model).
Figure 3.
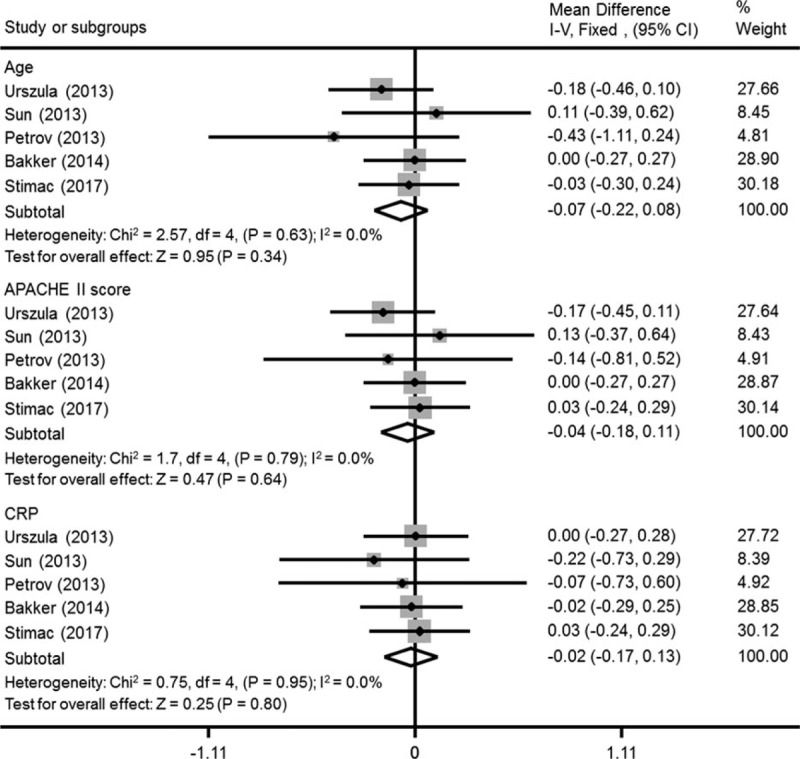
Age, APACHE II score, and CRP (mg/L) levels of the patients at baseline (fixed-effect model).
3.3. Effect of EEN on complications and mortality
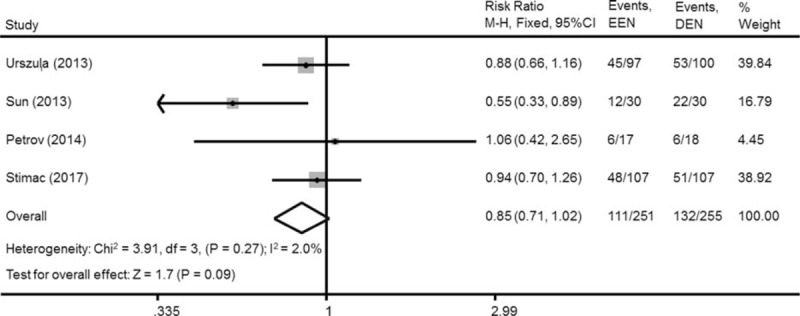
Acute pancreatitis can bring about many nonpancreatic complications, such as SIRS, multiple organ failure, and necrotizing pancreatitis. After aggregating the data, we found that EEN was associated with a significant reduction in the rate of multiple organ failure (RR = 0.67, 95% CI 0.46–0.99, P = .04, Fig. 4), but not for necrotizing pancreatitis (RR = 0.95, 95% CI 0.81–1.12, P = .57, Fig. 5). There was a tendency of decreased SIRS in EEN, but the difference was not significant (RR = 0.85, 95% CI 0.71–1.02, P = .09, Fig. 6).
Figure 4.
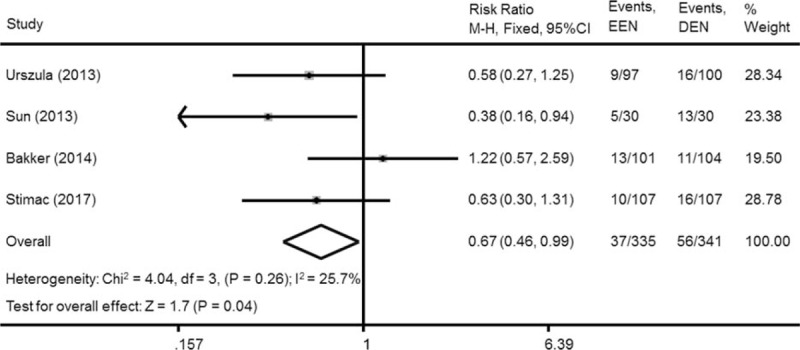
Effect of EEN on multiple organ failure in patients with acute pancreatitis (fixed-effect model).
Figure 5.
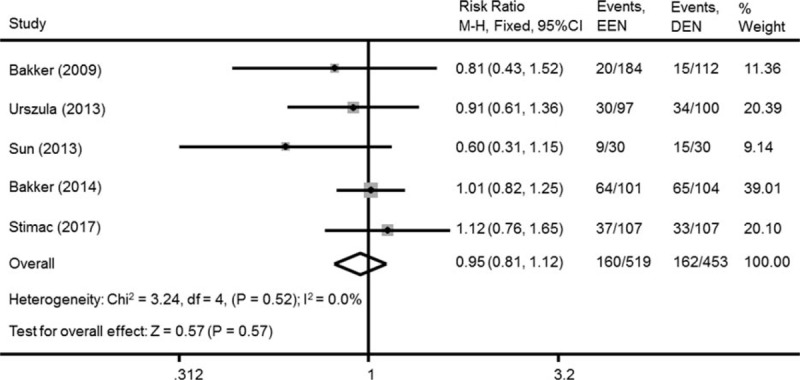
Effect of EEN on SIRS in patients with acute pancreatitis (fixed-effect model).
Figure 6.
Effect of EEN on mortality of acute pancreatitis (random-effect model).
3.4. Effect of EEN on mortality
Four studies presented data on the incidence of mortality of EEN and DEN. There was no significant reduction in mortality when comparing the EEN group with the DEN group (RR = 0.78, 95% CI 0.27–2.24, P = .64, Fig. 7).
Figure 7.
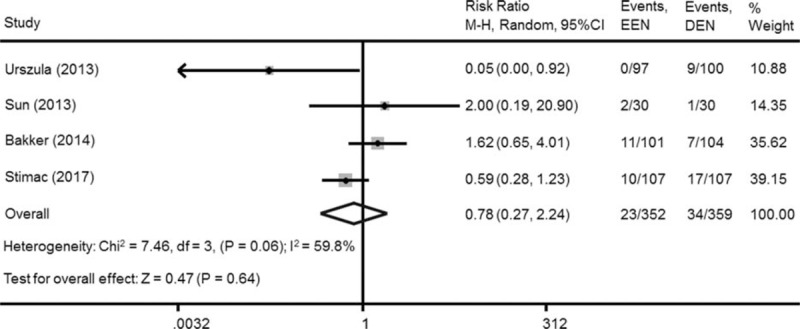
Effect of EEN on necrotizing pancreatitis in patients with acute pancreatitis (random-effect model).
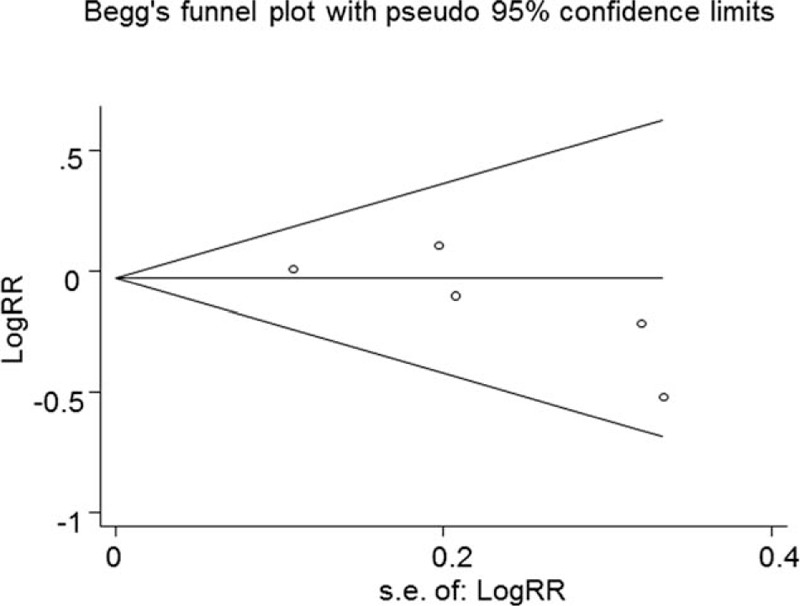
3.5. Publication bias
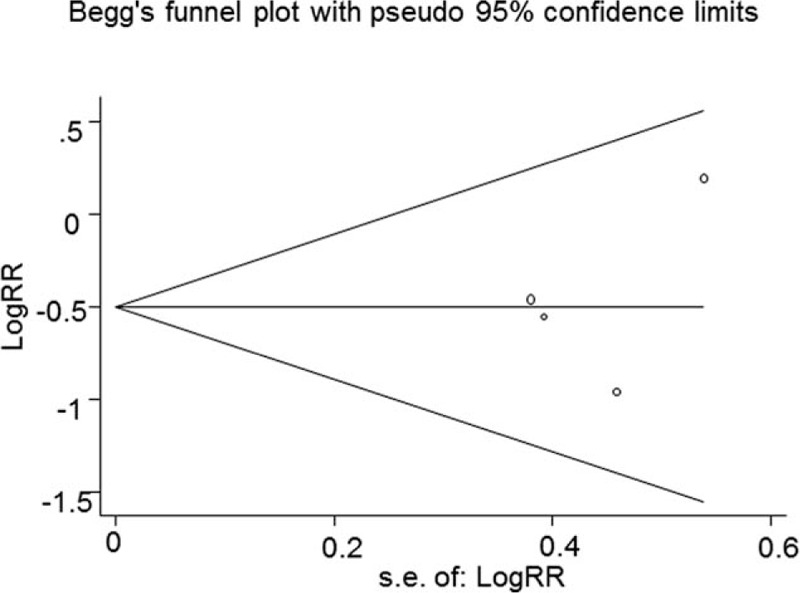
In this part of the study, 4 RCTs and 2 retrospective trials were included. The funnel plots of the RRs for mortality and necrotizing pancreatitis were used to assess publication bias. Begg test results showed Pr > |z| = 1.00 and Pr > |z| = 0.09, respectively (Figs. 8 and 9). Therefore, we believe that the risk of publication bias is low in this meta-analysis.
Figure 8.
Assessment of publication based on multiple organ failure data (Pr > |z| = 1.00).
Figure 9.
Assessment of publication based on necrotizing pancreatitis data (Pr > |z| = 0.09).
4. Discussion
Acute pancreatitis can lead to serious local and systemic complications, such as pancreatic necrosis, pancreatic infection, multiple organ failure, and SIRS. Many studies on nutrition have supported a shift from TPN to enteral nutrition for patients with pancreatitis because of fewer complications and lower mortality.[18] Moreover, some studies also indicated that the timing of EN should start as early as possible compared with conventional parenteral nutrition.[19,20] However, whether early EN is better than delayed EN in acute pancreatitis remains controversial. In this meta-analysis, we included 6 studies that satisfied our criteria and aggregated the data for clinical outcomes. We found that EEN was associated with a significant decrease in the incidence of multiple organ failure, but was not significant for other complications and mortality.
This meta-analysis was designed to compare the effect of early EN and delayed EN in acute pancreatitis. We set “beyond 48 hours” as the delayed EN, as in previous studies.[11] Our results showed that EEN could help to reduce the rate of multiple organ failure. Intestinal permeability caused by pancreatitis leads to increased serum endotoxin and cytokine levels, resulting in SIRS, which is involved in organ failure.[21] Gut function damage in the course of acute pancreatitis can occur as early as 48 to 72 hours after onset.[22,23] EEN may help to sustain gut permeability and result in less multiple organ failure. However, there was no significant difference in mortality, which was similar to the results of a previous meta-analysis that compared EEN with DEN in acutely ill patients, including postoperative, trauma, head-injured, burn, or medical ICU patients.[24] For other complications, although not significant, we identified a tendency for the EEN group to have a lower incidence of SIRS. These results could be explained in 2 ways: first, not only EEN but also DEN would partly help to sustain gut permeability and prevent bacterial translocation. Second, the starting time of EN in the included articles varied between 24 or 48 hours. Some studies set an optimal time of 24 hours, while others used 48 hours, or even 72 hours.[9,10,25] Therefore, early enteral feeding would help stabilize the integrity of the gut mucosa and enhance recovery from acute pancreatitis; however, the optimal time of administration remains controversial.
Some limitations of our study need to be discussed. First, not all included studies were RCTs; however, a sensitivity analysis was performed to assess the publication bias. Only 1 item among these studies showed significant heterogeneity. When the heterogeneity was over 50%, the random model was used. Second, because of the different feeding routes and timing, it was hard to avoid these slight differences. In this meta-analysis, we only focused the distinction between EEN and DEN and the time point of their administration was set as 48 hours after disease diagnosis, as described in a previous study.[11] Therefore, in this meta-analysis, we aimed to provide some general conclusions about the superiority of EEN over DEN for patients with acute pancreatitis. Finally, not every included study reported every item, such as mortality and multiple organ failure, even upon request.
Our results indicated that EEN should be recommended as the preferred nutrition routine in acute pancreatitis; however, more multicenter, randomized clinical trials are warranted to verify these findings.
Footnotes
Abbreviations: CI = confidential interval, CRP = C-reactive protein, DEN = delayed enteral nutrition, EEN = early enteral nutrition, RCT = randomized comparative trial, RR = risk ratio, SIRS = systemic inflammatory response syndrome.
The authors report no conflicts of interest.
References
- [1].Brisinda G, Vanella S, Crocco A, et al. Severe acute pancreatitis: advances and insights in assessment of severity and management. Eur J Gastroenterol Hepatol 2011;23:541–51. [DOI] [PubMed] [Google Scholar]
- [2].Frossard JL, Steer ML, Pastor CM. Acute pancreatitis. Lancet 2008;371:143–52. [DOI] [PubMed] [Google Scholar]
- [3].Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 2012;143:1179–87. e1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Gianotti L, Meier R, Lobo DN, et al. ESPEN guidelines on parenteral nutrition: pancreas. Clin Nutr 2009;28:428–35. [DOI] [PubMed] [Google Scholar]
- [5].Rodriguez JR, Razo AO, Targarona J, et al. Debridement and closed packing for sterile or infected necrotizing pancreatitis: insights into indications and outcomes in 167 patients. Ann Surg 2008;247:294–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].van Santvoort HC, Bakker OJ, Bollen TL, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011;141:1254–63. [DOI] [PubMed] [Google Scholar]
- [7].Foitzik T, Mithofer K, Ferraro MJ, et al. Time course of bacterial infection of the pancreas and its relation to disease severity in a rodent model of acute necrotizing pancreatitis. Ann Surg 1994;220:193–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Qin HL, Su ZD, Gao Q, et al. Early intrajejunal nutrition: bacterial translocation and gut barrier function of severe acute pancreatitis in dogs. Hepatobiliary Pancreat Dis Int 2002;1:150–4. [PubMed] [Google Scholar]
- [9].Bakker OJ, van Brunschot S, van Santvoort HC, et al. Early versus on-demand nasoenteric tube feeding in acute pancreatitis. N Engl J Med 2014;371:1983–93. [DOI] [PubMed] [Google Scholar]
- [10].Sun JK, Mu XW, Li WQ, et al. Effects of early enteral nutrition on immune function of severe acute pancreatitis patients. World J Gastroenterol 2013;19:917–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Li JY, Yu T, Chen GC, et al. Enteral nutrition within 48 hours of admission improves clinical outcomes of acute pancreatitis by reducing complications: a meta-analysis. PLoS One 2013;8:e64926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Yang L, Wang G, Du Y, et al. Remote ischemic preconditioning reduces cardiac troponin I release in cardiac surgery: a meta-analysis. J Cardiothorac Vasc Anesth 2014;28:682–9. [DOI] [PubMed] [Google Scholar]
- [13].Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 2005;5:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Bakker OJ, van Santvoort HC, Besselink MG, et al. Timing of enteral nutrition in patients with predicted severe acute pancreatitis: an early start is associated with a reduction in bacteremia. Gastroenterology 2009;141:1254–63. [Google Scholar]
- [15].Petrov MS, McIlroy K, Grayson L, et al. Early nasogastric tube feeding versus nil per os in mild to moderate acute pancreatitis: a randomized controlled trial. Clin Nutr 2013;32:697–703. [DOI] [PubMed] [Google Scholar]
- [16].Stimac D, Poropat G, Hauser G, et al. Early nasojejunal tube feeding versus nil-by-mouth in acute pancreatitis: a randomized clinical trial. Pancreatology 2016;16:523–8. [DOI] [PubMed] [Google Scholar]
- [17].Wereszczynska-Siemiatkowska U, Swidnicka-Siergiejko A, Siemiatkowski A, et al. Early enteral nutrition is superior to delayed enteral nutrition for the prevention of infected necrosis and mortality in acute pancreatitis. Pancreas 2013;42:640–6. [DOI] [PubMed] [Google Scholar]
- [18].Mirtallo JM, Forbes A, McClave SA, et al. International consensus guidelines for nutrition therapy in pancreatitis. JPEN J Parenter Enteral Nutr 2012;36:284–91. [DOI] [PubMed] [Google Scholar]
- [19].Li X, Ma F, Jia K. Early enteral nutrition within 24 hours or between 24 and 72 hours for acute pancreatitis: evidence based on 12 RCTs. Med Sci Monit 2014;20:2327–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Bakker OJ, van Brunschot S, Farre A, et al. Timing of enteral nutrition in acute pancreatitis: meta-analysis of individuals using a single-arm of randomised trials. Pancreatology 2014;14:340–6. [DOI] [PubMed] [Google Scholar]
- [21].Li Q, Wang C, Tang C, et al. Bacteremia in patients with acute pancreatitis as revealed by 16S ribosomal RNA gene-based techniques∗. Crit Care Med 2013;41:1938–50. [DOI] [PubMed] [Google Scholar]
- [22].Koh YY, Jeon WK, Cho YK, et al. The effect of intestinal permeability and endotoxemia on the prognosis of acute pancreatitis. Gut Liver 2012;6:505–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].McClave SA, Heyland DK. The physiologic response and associated clinical benefits from provision of early enteral nutrition. Nutr Clin Pract 2009;24:305–15. [DOI] [PubMed] [Google Scholar]
- [24].Marik PE, Zaloga GP. Early enteral nutrition in acutely ill patients: a systematic review. Crit Care Med 2001;29:2264–70. [DOI] [PubMed] [Google Scholar]
- [25].Zou L, Ke L, Li W, et al. Enteral nutrition within 72 h after onset of acute pancreatitis vs delayed initiation. Eur J Clin Nutr 2014;68:1288–93. [DOI] [PubMed] [Google Scholar]