

Abstract
Objectives
The risk of cognitive impairment is a concern for patients with major depressive disorder (MDD) receiving electroconvulsive therapy (ECT). Here, we evaluate the acute, short-term and long-term effects of ECT on tests of processing speed, executive function, memory, and attention.
Methods
Forty-four MDD patients receiving ECT (61% right unilateral (RUL), 39% mixed RUL-bitemporal, left UL and/or bitemporal lead placement underwent a cognitive battery prior to ECT (T1), after 2 sessions (T2), and at the end of the index (T3). Thirty-two patients returned for a 6-month follow-up (T4). Thirty-three controls were assessed at two times ~4 weeks apart (C1 and C2).
Results
At baseline, patients showed deficits in processing speed, executive function and memory compared to controls. Including depression severity and lead placement covariates, linear mixed model analysis showed significant improvement in only processing speed between T1 and T3 and between T1 and T4 in patients. An acute decline in attention and verbal memory was observed at T2, but performance returned to baseline levels at T3. Longitudinal cognitive outcomes did not differ in patients defined as ECT responders/non-responders.
Limitations
Episodic memory was not measured and medications were not controlled between T3 and T4. Controls also showed improvements in processing speed, suggesting practice effects for some measures.
Conclusions
In this naturalistic ECT treatment study, results show that the initiation of ECT may transiently affect memory and executive function, but cognition is largely unaffected during and post ECT. While some functions might improve, others will at least remain stable up to 6-months following the ECT index.
Keywords: Major depressive disorder, electroconvulsive therapy, cognition
Introduction
Electroconvulsive therapy (ECT) elicits a response in up to 70% of eligible patients, on average, and is currently the most effective treatment for severe depression (1, 2). Unlike antidepressant medications, the ECT procedure involves a direct effect on the central nervous system, is faster-acting, and avoids the systemic side-effects of psychotropic drugs. In 2002, ECT was estimated to be used annually for 100,000 US patients and 1 million patients globally (3). Despite its effectiveness, public stigma continues to surround ECT, which may stem, in part, from concerns over perceived lingering cognitive and memory impairments associated with older ECT methods. Even though contemporary ECT protocols are safe and well tolerated with only rare or serious side-effects, this stigma persists (4).
More recently, cognitive impairment has been recognized as a common problem in MDD (5, 6). Several studies have reported that patients with MDD consistently under perform on cognitive assessments compared to normal controls (6, 7). Specifically, areas of attention and executive function, including working memory, inhibitory control, cognitive flexibility and goal-oriented behavior, appear particularly vulnerable (8–11). Many reports suggest that impairments in these cognitive domains contribute to the profound and global disability linked with MDD (9, 12, 13). For patients already suffering from decreased cognitive function, the risk of further cognitive decline may be one of the main reasons for declining ECT (14).
While some recent studies have shown that ECT adversely effects cognitive and memory function (15–17) specifically within the first 7 to 8 days (18), others have reported that cognition returns to baseline (19) or even improves (20, 21) following treatment. Cognitive measurements included autobiographical (episodic) and working memory, information processing, and executive function. A meta-analysis of 84 studies reported that ECT is associated with acute deficits in cognitive domains (processing speed, executive function, attention/working/and verbal memory) following the ECT index series (0–3 days post final ECT), which then stabilize over a two-week period (22). For many cognitive domains (processing speed, attention/working memory, and executive function), performance improved thereafter (>15 days) (22). Thus, while cognitive effects have been investigated during and immediately after ECT index, results are somewhat variable and limited in the cognitive domains tested and ECT protocol used.
Few studies test the longer term effects of ECT on cognition and the relationship with depression status. Two reviews reported that initial cognitive deficits revert back to baseline at 6 months following ECT in all patients (23, 24). In a recent retrospective study, Fernie et al., reported poorer spatial recognition memory performance at each evaluation up to 3 months post-ECT compared to baseline, although performance improved at 6-month follow-up (25). In contrast, one of the largest studies investigating long-term memory outcomes following ECT (n=347) reported that cognitive effects persist at 6-month follow-up, though ECT parameters, and bilateral lead placement specifically, contributed to these findings (26). Few studies have examined executive function, attention, and processing speed to evaluate other aspects of cognition (24).
Lead placement is an important consideration for cognitive effects linked with ECT, as are the associated parameters of pulse width and dose relative to seizure threshold (ST). While bitemporal ECT may produce a more rapid clinical response with respect to right unilateral (RUL) ECT, this montage is generally associated with greater cognitive side effects (27). Some acute efficacy trials report RUL ECT is as effective as bitemporal ECT if delivered at sufficient multiples of ST (28–30) and, further, RUL at 5–6 × ST has been reported to induce less severe negative cognitive effects and less short- and long-term retrograde amnesia during and immediately after therapy (19, 28, 30, 31), compared with bilateral ECT at 1.5 to 2 × ST. However, other studies report similar adverse cognitive effects between high dose (5–8× ST) unilateral ECT and moderate dose (1–1.5× seizure threshold) bitemporal ECT (32, 33) and between ultra-brief unilateral and brief unilateral ECT (32, 34). Overall, studies have remained inconsistent on efficacy and cognitive effects.
While several studies have reported unchanged or improved cognitive performance post-ECT, others have reported persistent adverse cognitive effects. Most of these studies did not include controls to examine the presence of practice effects or to determine if cognitive effects differ in acute ECT responders and non-responders and in patients who respond to ECT but then subsequently relapse. We thus performed a longitudinal investigation of cognition (executive function, working, verbal and spatial long term memory and processing speed) in patients with MDD receiving predominantly RUL ultra-brief pulse ECT (61% RUL, and 39% mixed RUL-BL, left UL, and/or bitemporal placement). The cognitive battery was administered at four time points in patients and at two time points in controls. The four time points for MDD patients took place prior to ECT (T1), after 2 sessions (T2), at the end of the index (T3, short-term), and at 6-month follow-up (T4, long-term). Controls were assessed at two times ~4 weeks apart (C1 and C2). Based on the available literature, we hypothesized that the ECT index series would have no significant lasting adverse effect on cognition regardless of treatment response. We expected that acute cognitive impairments (between T1 and T2) due to ECT initiation would revert to baseline levels at T3 and T4.
Materials and Methods
Participants
Forty-four patients (Table 1) were recruited from individuals scheduled to begin ECT at the Resnick Neuropsychiatric Hospital, University of California, Los Angeles. Eligibility criteria included a diagnosis of recurrent major depression with a current episode lasting at least 6-months. Patient diagnoses were established by clinical consultation using Diagnostic and Statistical Manual of Mental Disorders IV-TR (DSM-IV-TR; (35)) criteria. Study exclusion criteria included comorbidity of dementia, first episode of depression, late onset of depression (>50 years of age), depression related to a medical condition, or ECT or other neuromodulation therapy in the previous 6 months. All patients were tapered off psychotropic medications including antidepressants and benzodiazepines, with complete cessation of these medications for at least 48–72 hours before ECT. The majority of patients returned to antidepressant medication therapy following the ECT index series. Medication treatment received between completion of ECT index and 6-month follow-up was naturalistic and not controlled for in this research study.
Table 1.
Demographics and clinical characteristics
| MDD (n= 44) | Normal Controls (n= 33) | |||||
|---|---|---|---|---|---|---|
| Gender (M/F, %F) | 18/26 (59.1%) | 14/19 (57.8%) | ||||
| Age (years) | 40.7±13.2 | 39.0±12.2 | ||||
| Education (years) | 15.7±2.5 | 17.0±2.4 | ||||
| Premorbid Function | 115.8±9.5 | 116.0±8.2 | ||||
| Dextral/non-dextrala | 40/4 | 29/4 | ||||
| Unipolar/bipolar | 37/7 | – | ||||
| Age of onset | 24.3±11.0 | – | ||||
| Current episode (years) | 2.3±3.1 | – | ||||
| Lifetime illness (years) | 16.4±11.1 | – | ||||
| Responders/non-respondersb | 21/23 | – | ||||
| Treatments in index | 11.68±3.4 | – | ||||
| RUL treatment | 9.07±3.2 | – | ||||
|
| ||||||
| Mood Scales | T1 | T2 | T3 | T4 (n= 32) | C1 | C2 |
|
| ||||||
| HAMD* | 23.6±6.1 | 18.1±6.9 | 13.4±7.6 | 11.7±7.7 | – | – |
| MADRS* | 37.1± 8.3 | 28.8±10.5 | 19.1±11.1 | 16.5±12.2 | – | – |
Abbreviations: T1: Patient baseline; T2: After the 2nd ECT; T3: After the ECT index series; T4: 6-month follow-up; C1: Control baseline; C2: Control follow-up; RUL: Right unilateral lead placement; HAMD: Hamilton Rating Scale for Depression- 17 Item; MADRS: Montgomery – Åsberg Depression Rating Scale.
Handedness was estimated using the modified Edinburgh Handedness Inventory (58) with a laterality quotient of <0.7 defined non-dextrals.
Response defined as >50% improvement in HAMD scores over the course of treatment
Significant effect of ECT (p<0.0001).
Demographically similar healthy controls (n =33) were recruited from the Los Angeles area using advertisements and screened with the Mini-International Neuropsychiatric Interview (M.I.N.I; (36)) to exclude for a history of depression, other psychiatric illness, as well as antidepressant use. Study inclusion for MDD and control groups required absence of neurological/physical/developmental disorders, substance abuse/dependence history and contraindication to MRI.
MDD participants completed up to 4 study time points while the control group completed 2 time points (Table 1). Thirty-two of the 44 patients who completed time point 3 returned for a 6-month follow-up visit. All participants provided written informed consent for participation as approved by the UCLA Institutional Review Board.
Data Acquisition
Patients received clinical and cognitive assessments at each time point: T1 or baseline- within 24 hours prior to the 1st ECT treatment; T2- within 48 hours after their 2nd ECT treatment to allow for seizure threshold titration occurring at the first ECT session; T3- within 1 week of completing the ECT treatment index series (short-term), and T4- approximately 6 months after completing the ECT index series (long-term). Controls completed cognitive assessments at two time points with intervals equivalent to patients’ T1 (C1) and T3 (C2) assessments to establish potential for practice effects for repeated assessments (Fig 1). The cognitive assessment battery comprised five established and well documented neuropsychological tasks: the Wechsler Adult Intelligence Scale 4th edition (WAIS) Digit Span and Coding, Hopkins Verbal Learning Test-Revised (HVLT-R), Brief Visuospatial Memory Test-Revised (BVMT-R), Trail Making Test including Parts A and B, and Stroop Color and Word Test (37–40). The Test of Premorbid Functioning (TOPF; Wechsler, 2001) from Advanced Clinical Solutions for the WAIS-IV and WMS-IV was also administered to all volunteers at baseline (41). Digit Span measures working memory, attention, concentration and mental control, and auditory processing. Coding measures processing speed, short-term visual memory, learning ability, psychomotor speed, visual perception, visual-motor coordination, and visual scanning ability. The HVLT-R measures verbal learning and memory, attention, and concentration. The BVMT-R measures visuospatial memory, attention, and concentration. The Trail Making Test Part A (Trail A) measures visual attention and processing speed, and the Trail B additionally measures cognitive flexibility (42). The Stroop measures selective attention, processing speed, cognitive flexibility, and executive function (43). To minimize practice effects for memory tests, different versions (forms 1–4) of the HVLT-R and BVMT-R were used at each of the four time points, with the order of versions randomized across patients for each time point. The same test versions were used for the other cognitive measures since alternate forms were not available. All scores except for the Stroop test were standardized for age prior to analysis.
Figure 1.
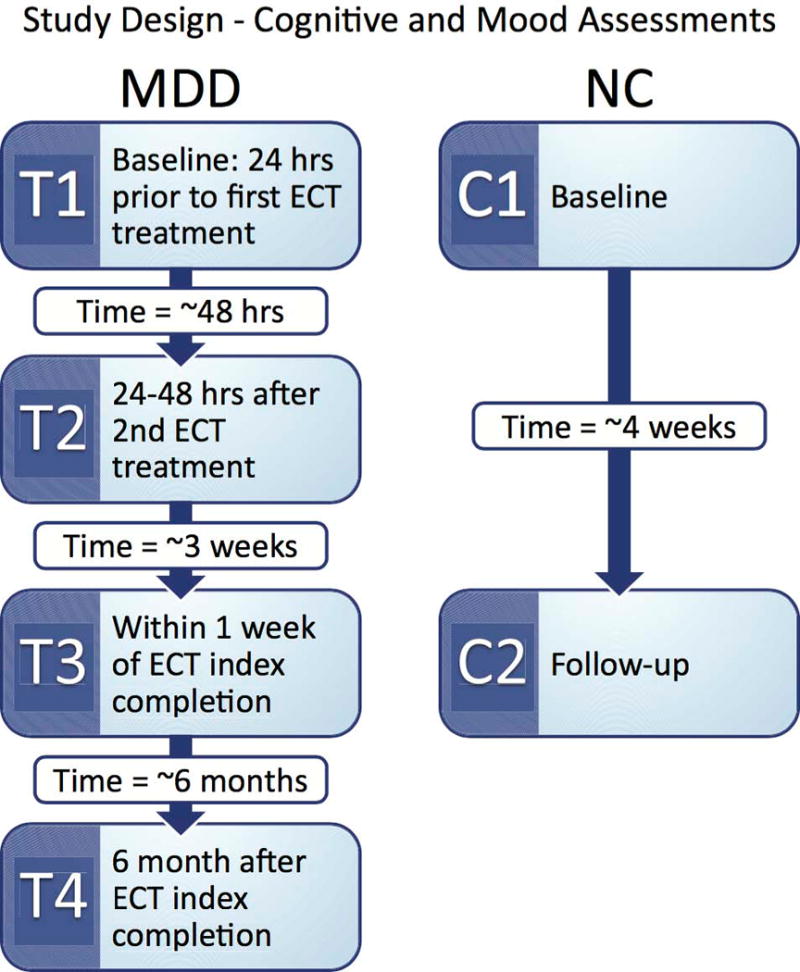
Study Design. Patients diagnosed with major depressive disorder (MDD) received cognitive and clinical assessments at 4 time points. Normal controls (NC) completed cognitive assessments at two time points with intervals equivalent to patients’ T1 and T3 assessments.
Clinical assessments
The Hamilton 17-item (HAMD; (44)) and Montgomery- Åsberg (MADRS; (45)) Depression Rating Scales were administered at each time point to assess symptoms and treatment response. These scales are highly correlated; therefore, the HAMD was chosen as the primary measure of clinical response and relapse. At T3, if HAMD scores had decreased by 50% from baseline the patient was identified as a responder. In responders, relapse was determined at T4 if HAMD scores increased by 50% from T3. For further descriptive purposes, other clinical measures were also recorded.
ECT Treatment
ECT (5000Q MECTA Corp.) was administered 3 times a week, using a standard protocol for anesthesia (methohexital at 1mg/kg dosage) and muscle relaxation (succinylcholine at 1mg/kg dosage). ECT followed the ST titration method where after establishing the ST at the first session, subsequent treatments were delivered at 5–6× ST for RUL d’Elia lead placement using an ultrabrief pulse-width (0.3 ms) and an amplitude of 800mA. This study was naturalistic and decisions about lead placement and amplitude were based on the clinical judgement of the ECT treatment provider. Patients routinely began with RUL ECT placement, unless there was compelling clinical need or other relevant history supporting starting with bitemporal ECT. Patients were treated with ECT until there was clinical evidence of sustained response or remission for at least 1 week as supported by mood scales. A standard index course of ECT is between 6 to 12 sessions for most patients on average. If the patient did not manifest a sufficient response to RUL ECT at any point in their series, after discussion with and at the discretion of the ECT provider, the patient could switch to bitemporal ECT if they so consented. The majority of patients (61%) received RUL exclusively. After retitration of ST for change in lead placement, bitemporal ECT was delivered at 1.5x ST using a brief pulse-width (0.5 ms) and an amplitude of 800mA. The length of the ECT treatment index was clinically and individually determined, where patients received a mean of 11.35 ECT treatments [Table 1].
Statistical Analysis
The results from the cognitive tests are presented as mean ± standard deviation in Table 2. To determine if normality assumptions held the Shapiro-Wilk test was used. Since the data did not follow a normal distribution, between group (patient/control at baseline) analyses were conducted using both log transformed and non-log-transformed data to determine if the degree of non-normality was sufficient to bias the results, as the GLMM is reasonably robust against some violations of the normality assumption. Results were similar, and for ease of interpretation the non-log transformed statistics are reported. Within subject analysis used non log-transformed data.
Table 2.
Means and standard deviations for cognitive scores at each time point in patients and controls.
| T1 | T2 | T3 | T4 | C1 | C2 | |
|---|---|---|---|---|---|---|
| Digit Span | 49.1±9.1 | 49.5±8.2 | 49.2±9.0 | 49.6±9.0 | 52.1±9.7 | 53.9±11.4 |
| Coding | 42.8±10.7 | 45.2±10.3 | 46.7±12.2* | 50.6±10.1*ˆ+ | 52.6±11.2 | 56.7±11.9* |
| HVLT total | 37.8±11.2 | 36.0±12.4 | 37.9±12.9 | 39.8±12.5 | 43.6±11.1 | 43.9±11.6 |
| HVLT delay | 40.4±11.9 | 33.6±14.7* | 37.5±14.7ˆ | 41.7±13.3ˆ | 46.0±11.0 | 46.2±11.2 |
| BVMT total | 49.3±15.7 | 48.3±13.7 | 48.1±13.4 | 51.1±13.1 | 54.4±11.2 | 53.8±12.4 |
| BVMT delay | 49.2±14.7 | 48.8±14.0 | 47.9±15.1 | 52.5±10.2 | 50.7±12.4 | 51.1±12.1 |
| Trail A | 48.8±12.6 | 52.1±10.6* | 51.8±9.6 | 53.0±11.2* | 55.1±7.8 | 58.8±6.7* |
| Trail B | 47.1±15.4 | 47.9±14.4 | 50.3±11.5 | 50.6±12.4 | 55.7±7.3 | 57.9±9.2 |
| Stroop | 51.1±6.6 | 54.1±8.1* | 53.6±8.0* | 52.5±6.6 | 53.0±7.3 | 53.9±7.0 |
Abbreviations: T1: Patient baseline; T2: After the 2nd ECT; T3: After the ECT index series; T4: 6-month follow-up; C1: Control baseline; C2: Control follow-up; HVLT-total: Hopkins Verbal Learning Test-Revised total score after 3 trials; HVLT-delay: score for words remembered after a 15 minute delay; BVMT-total: Brief Visuospatial Memory Test-Revised total score after 3 trials; BVMT-delay: score after a 15 minute delay.
Significant difference from baseline, p<0.05
Significant difference from T2, p<0.05
Significant difference from T3, p<0.05
For longitudinal analysis, a multivariate general linear mixed model (GLMM) that included all 9 cognitive variables, subject as a random factor, and time as a fixed factor, was performed. Results showed a significant interaction between cognitive test and time point (F=2.57 and p=0.001). To elaborate on this omnibus result, follow-up univariate analyses of each cognitive score over the course of ECT were conducted. Separate GLMMs, again including time as a fixed factor and subject as a random factor were thus then performed for each cognitive test separately. For measures showing significant overall effects of time, changes between individual time points were then examined. Baseline HAMD scores and percent RUL electrode placement were included as nuisance covariates for patient analyses to control for severity of disease and for lead placement. The same GLMMs were used to determine change in each cognitive measure over time in control subjects assessed twice. In post-hoc analyses, MDD patients were also separated into responders and non-responders (determined by at least 50% decrease in depressive symptoms according to the HAMD) to test for interactions based on response status as measured at T3.
For cross-sectional analysis of patient and control groups at baseline, a multivariate general linear model (GLM) was performed including all cognitive variables. Results showed a significant main effect of group (F=3.40 and p=0.002). Univariate analyses were subsequently performed to determine the extent of diagnostic group differences for each cognitive measure.
Finally, patients defined as ECT responders were also separated into two groups based on whether they had relapsed by 6-months (T4) to determine if change in cognitive measures between the end of index (T3) and T4 differed based on relapse.
Results
Demographic and Clinical Variables
Patients and controls showed similar distributions of age (F(1,75)=1.02, p=0.32) and sex (F(1,75)=0.06, p=0.80). While controls had significantly higher education scores than the MDD group (F(1,75)=0.07, p=0.03), estimates of premorbid function did not differ significantly between patients and control group (F(1,75)=0.16, p=0.69). Education scores were thus included as covariates in analyses comparing patients and controls at baseline.
HAMD and MADRS ratings improved significantly with ECT (57% and 51% decrease in depressive symptoms respectively; Fig. 2). Using a threshold of at least 50% symptom improvement as measured by the HAMD at T3, 21 patients were identified as responders (Table 1). Of the 44 MDD patients, 32 returned to complete a 6-month follow-up assessment. The 32 comprised of 17 responders and 15 non-responders. Of the 17 responders, 9 had sustained response while 8 had relapsed at T4.
Figure 2.
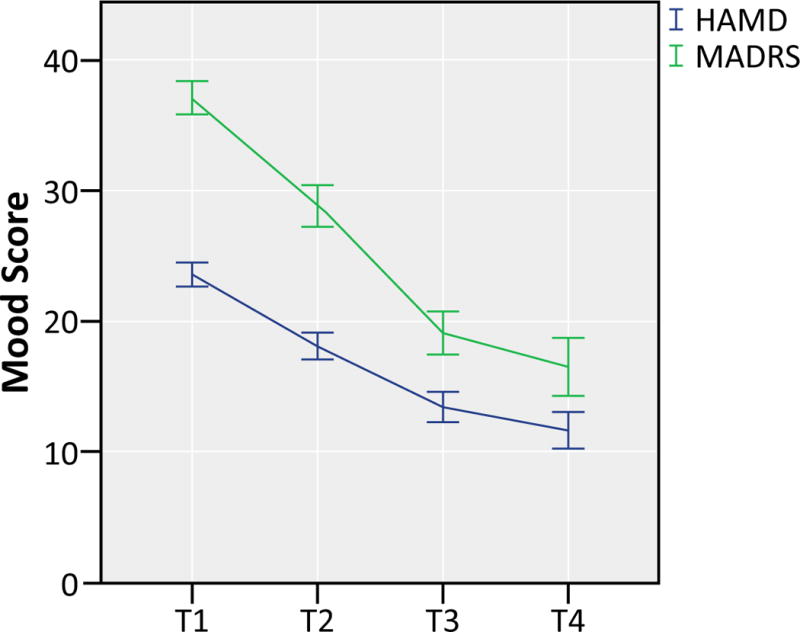
Scores for the Hamilton 17-item (HAMD) and Montgomery- Åsberg (MADRS) Depression Rating Scales are reported at each time point: T1- Patient baseline; T2- After the 2nd ECT; T3- After the ECT index series; T4- 6-month follow-up. HAMD and MADRS scores improved significantly (decrease in score =decrease in depressive symptoms) with ECT (57% and 51% respectively). Highest score possible on the HAMD and MADRS is 52 and 60 respectively and lowest is 0 for both. Error bars represent standard errors of the mean.
Longitudinal Change in Cognitive Performance
Standardized t-scores for the Digit Span, Coding, HVLT-R (total immediate and delayed recall), BVMT-R (total immediate and delayed recall), Trail A, Trail B, and Stroop (t-score of the difference between predicted and actual color-word score) are reported in Table 2. T-scores for Trails A and B were calculated using Table 12–14 of means and SDs for adults from Tombaugh, Rees, and McIntyre, 1998 (46). T-scores were computed from scaled scores for the Digit Span and Coding tests using the “Pocket Guide to Test Scores” (p4k.s3.amazonaws.com/day_2/Pocket_Guide.pdf). MDD patients showed significant changes in scores for Coding, and HVLT-R delayed recall and showed similar trends for Trail A and Stroop over the 4 time points (Fig. 3). While number of words recalled after a 15-minute delay on the HVLT-R (HVLT-R delay) significantly decreased at T2 compared to T1 (F(3, 40)=3.8, p=0.003), performance rebounded at T3, and no significant difference was found between T1 and T3. Similarly, while change in performance on the Stroop did not reach significance (F(3, 39.1)=2.6, p=0.066), a drop was observed at T2 which leveled back at T3. Coding (F(3,36.7)=5.9, p=0.002) showed an increasing trend: T3 (p=0.035) and T4 (p<0.001) showed significantly better scores compared to baseline. Trail A (F(3, 35.3)=2.4, p=0.088) also showed an increasing trend; however, significance was not reached. HVLT-R immediate recall, Digit Span, BVMT-R immediate recall and delay, and Trail B showed no significant change in performance over the four time points (all p>0.05).
Figure 3.
Cognitive measures showing significant effects of ECT across the 4 time points in patients with major depressive disorder (MDD) or significant effects of time in normal controls (NC) assessed at 2 time points. Hopkins Verbal Learning Test- Revised delayed portion (HVLT-R delay), Trail A, Stroop, and Coding showed changes with ECT. Significance between time points are indicated with an asterisk (see text for details). Error bars represent standard errors of the mean.
*p<0.05
**p<0.001
Across time, the control group showed a significant increase in performance at C2 for Trail A (F(1, 32)=8.7, p=0.006) and Coding (F(1, 32)=13.2, p=0.001) tests compared to baseline. Digit Span, HVLT-R, BVMT-R, Trail B and Stroop showed no significant change in performance over the two time points, noting that different versions of the HVLT-R and BVMT-R were used at each session.
Cross-sectional Differences in Cognitive Performance between Controls and MDD at Baseline
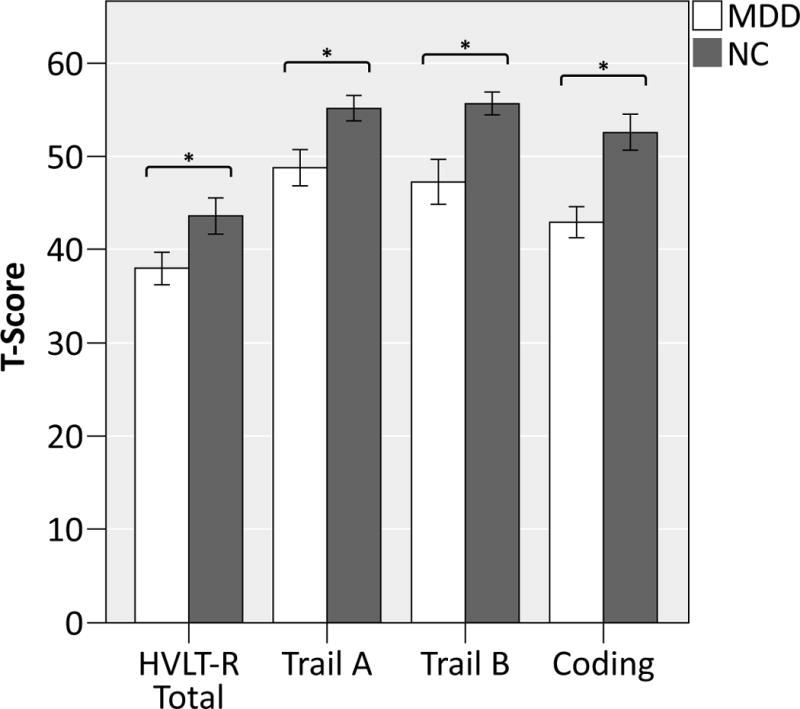
The MDD group showed poorer performance in several cognitive domains at baseline compared to normal controls as observed in the multivariate GLM reported above (Fig. 4). When examining each score separately, controls showed higher performance on Coding (F(1,71)=10.1, p=0.002), Trail A (F(1,71)=3.8, p=0.05), Trail B (F(1,71)=7.6, p=0.008), and HVLT-R total (F(1, 71)=4.0, p=0.049). No significant difference was found for the HVLT-R delay, Stroop, BVMT-R delay, BVMT-R total, or Digit Span tests (all p >0.05).
Figure 4.

Cognitive measures showing significant differences in patients with major depressive disorder (MDD) and normal controls at baseline. The Hopkins Verbal Learning Test- Revised total portion (HVLT-R total), Trail A and B, and Coding showed significant differences between the two groups at baseline. Significance is indicated with an asterisk. Error bars represent standard errors of the mean.
*p<0.05
Cognitive Performance in Responders vs Non-responders
There was no overall significant interaction for response status for any of the cognitive scores examined (all p>.0.05).
Cognitive Performance in Responders who subsequently relapsed
No significant changes in cognitive performance were observed in ECT responders who subsequently relapsed at T4. However, responders who sustained response showed an increase in performance on the Coding (F(1, 32)=7.9, p=0.013) test between T3 and T4. Non-responders at T3 also showed no significant changes between end of treatment and the 6-month follow-up.
Discussion
While several studies have investigated the impact of ECT on cognitive function, this investigation addresses some limitations in prior studies to provide several unique observations. Here, we included a cognitive battery of 5 established and well documented neuropsychological tasks with alternate forms when available (HVLT-R and BVMT-R) to control for practice effects, use of normative-adjusted data, a long-term follow-up, and inclusion of demographically matched controls in order to study practice effects of repeated administration of the cognitive battery. The cognitive battery comprised of a longitudinal analysis of executive function, attention, processing speed, verbal memory, and visual memory to investigate acute (between baseline and after the second ECT (T2)) short term (between baseline and end of the ECT index (T3)) and long term (between T3 and 6-month follow-up (T4)) effects of ECT on cognitive function in patients with MDD. After the first two ECT sessions of the series (T2), only verbal memory (HVLT-R delay) and executive function, specifically inhibition (Stroop), showed a decline in performance compared to baseline scores. However, at T3, the HVLT-R delay and Stroop test scores recovered to baseline values suggesting only a transient effect associated with the initiation of treatment. Therefore, similarly to Verwijk et al.’s review, an acute effect of ECT was observed after the first two treatments that stabilized after the full course of ECT (47). All other tests showed either no change or improvement from baseline to T2 or the end of the index series. In contrast to the results of Falconer et al. and Fernie et al., visual and visuospatial memory also remained stable from baseline to T3 (25, 48). Six-month follow-up assessments confirmed stability or further improvement in cognitive performance. Significant improvements in processing speed and a trend towards higher attention (Coding and Trail A) were observed for the MDD group at the short- (T3) and long-term (T4) follow-up visits compared to baseline (T1); however, the control group also showed significant improvement in these domains at C2 compared to C1 suggesting the presence of practice effects. ECT did not show different effects on cognition between responders and non-responders, suggesting changes in cognition relating to ECT are independent of clinical outcome. That is, even individuals who did not benefit from the anti-depressive effects of ECT showed no significant decline in cognitive function compared to baseline. Further, cognitive function remained stable at 6-month follow-up in patients who responded to ECT and then had a subsequent relapse.
Our results are in accordance with the majority of recent studies showing stability of cognitive performance as well as improvements in processing speed with ECT in the short-term (baseline to end of index) and long-term (after 6-months) (22, 25, 47, 49, 50). Semkovska, Bodnar, and Fernie reported significant improvement in cognition at varying time points after ECT completion (2 weeks (22), 3 months (50), and 6 months (25) respectively). These studies reporting improvements, however, did not assess control subjects. Here, we also show that improvements in processing speed and attention may be at least partly attributable to practice effects. Only acute adverse effects of ECT on verbal memory and executive function (specifically inhibition) after two sessions of ECT were observed; unlike some other studies these effects were not present after the index series was completed or at the 6-month follow-up (22, 50). In the current study, ECT did not have a long-term adverse effect on cognition and actually showed improvements in some aspects of cognitive function.
MDD patients show frequent difficulties concentrating, remembering, and making decisions, and cognitive impairments in related domains of function are commonly observed (5). The results in this study confirm that patients with severe MDD show significantly poorer performance for executive function and memory compared to age- and sex-matched normal controls pre-ECT. The risk of cognitive impairment frequently impacts an individual’s decision whether or not to receive ECT. The current results show that ECT is not associated with a significant decline in cognitive performance in the short-term (T3) or in the long-term (T4) even for patients who do not benefit from the antidepressant effects of ECT.
In this investigation, ECT was shown to have no overall negative cognitive side effects at the end of treatment (T3) and at 6 month follow up (T4) regardless of treatment response. While the results of this study do not show normalization towards normal controls for any of the measures, mild improvements were observed. Other studies have reported ECT-induced normalizing effects in the structure and function of the brain. For example, in an overlapping sample, we have reported ECT-induced neuroplasticity in the hippocampus and amygdala (51), and increased cortical thickness of the bilateral anterior cingulate cortex (ACC), inferior and superior temporal, parahippocampal, entorhinal and fusiform cortex and in distributed prefrontal areas over the course of ECT (52). We have also shown significant increases of fractional anisotropy (FA) indicating improved structural connectivity in dorsal fronto-limbic circuits (53). However, several of these neuroplastic changes do not significantly relate to changes of clinical response. Specifically, in our prior studies, changes in hippocampal and ACC morphometry and functional connectivity between the dorsal ACC, mediodorsal thalamus, hippocampus, right anterior temporal, medial parietal, and posterior cingulate cortex show moderate relationships with ECT symptom improvements (51, 52, 54). It is thus plausible that changes in particular structural and functional networks may relate to changes in cognitive function occurring with ECT that are at least partially independent of changes in network activity relating to clinical outcome. It is also possible that cognition improves in patients sustaining successful clinical response over a longer time frame (i.e. on a different temporal scale). Currently, very few investigations of structural and functional MRI correlates of cognitive changes in relation to ECT exist. Nordanskog et al., found no significant correlation between hippocampal volume and cognitive changes due to ECT (55) while Lekwauwa et al. reported that smaller hippocampal volumes associated with poorer cognitive outcomes (56). Another study reported a correlation between T2 increases in the thalamus and anterograde memory impairment following ECT (57). These few studies show inconsistent findings, perhaps attributable to small sample sizes. Therefore, it is an important avenue for future research.
Though the results of this study support that an index course of ECT does not impair overall cognitive function, it is possible that more subtle deficits or improvements in function remained undetected with the current sample size. Another limitation is that we did not specifically assess episodic autobiographical memory, which has been reported to be particularly susceptible to ECT (47, 58). Cognitive effects due to ECT can vary based on lead placement and pulse width. In this study, all patients with the exception of one, started on RUL ultra-brief pulse protocol. However, based on clinical decisions independent of the study protocol, some patients were switched to bitemporal placement during the course of the index series. We included lead placement as a covariate and observed no effects on cognitive outcome. Attrition with respect to 6-month follow-up assessments is another potential limitation. This was partially due to a 7-month disruption in study procedures due to a scanner hardware failure. Subjects were otherwise unreachable, not able or declined to return for the final follow-up. At the 6-month follow-up only half of the non-responders returned making our T4 data more representative of responders. However, in the non-responders who did return no significant cognitive changes were observed. Another potential limitation is that the control group had a higher level of education than the MDD group, which could influence the observed differences in cognitive scores at baseline. Education level was thus included as a covariate for diagnostic group contrasts. It is also worth noting, however, that premorbid functioning did not differ statistically between the 2 groups. Lastly, medication use between the end of ECT index and T4 was not controlled or evaluated.
Overall this investigation showed cognitive stability in the short (after completion of index, T3) and long-term (T4) regardless of treatment response when using predominantly RUL ECT protocols which are typically associated with fewer side-effects. Only mild transient negative effects on cognition were observed after 2 treatments (T2). While some functions improved with ECT, these functions also improved in controls suggesting practice effects. Further investigation of MRI correlates of cognitive changes caused by ECT and investigation of even longer term cognitive effects are needed as they may elucidate cognitive trajectories in patient receiving ECT.
Acknowledgments
Source of Funding
Funding for this study is provided by Award Numbers R01MH092301 from the National Institute of Mental Health
Footnotes
Conflicts of Interest
The authors declare no conflicts of interest.
References
- 1.Kho KH, van Vreeswijk MF, Simpson S, et al. A meta-analysis of electroconvulsive therapy efficacy in depression. J ECT. 2003;19:139–147. doi: 10.1097/00124509-200309000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Kellner CH, Greenberg RM, Murrough JW, et al. ECT in treatment-resistant depression. Am J Psychiatry. 2012;169:1238–1244. doi: 10.1176/appi.ajp.2012.12050648. [DOI] [PubMed] [Google Scholar]
- 3.Abrams R. Electroconvulsive therapy. 4th. Oxford; New York: Oxford Unversity Press; 2002. [Google Scholar]
- 4.Sackeim HA. Convulsant and anticonvulsant properties of electroconvulsive therapy: towards a focal form of brain stimulation. Clinical Neuroscience Research. 2004b;4:39–57. [Google Scholar]
- 5.Trivedi MH, Greer TL. Cognitive dysfunction in unipolar depression: implications for treatment. J Affect Disord. 2014;152–154:19–27. doi: 10.1016/j.jad.2013.09.012. [DOI] [PubMed] [Google Scholar]
- 6.Snyder HR. Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: a meta-analysis and review. Psychol Bull. 2013;139:81–132. doi: 10.1037/a0028727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cotrena C, Branco LD, Shansis FM, et al. Executive function impairments in depression and bipolar disorder: association with functional impairment and quality of life. J Affect Disord. 2016;190:744–753. doi: 10.1016/j.jad.2015.11.007. [DOI] [PubMed] [Google Scholar]
- 8.Cotrena C, Branco LD, Kochhann R, et al. Quality of life, functioning and cognition in bipolar disorder and major depression: A latent profile analysis. Psychiatry Res. 2016;241:289–96. doi: 10.1016/j.psychres.2016.04.102. [DOI] [PubMed] [Google Scholar]
- 9.Trivedi MH, Morris DW, Wisniewski SR, et al. Increase in work productivity of depressed individuals with improvement in depressive symptom severity. Am J Psychiatry. 2013;170:633–641. doi: 10.1176/appi.ajp.2012.12020250. [DOI] [PubMed] [Google Scholar]
- 10.Diamond A. Executive functions. Annu Rev Psychol. 2013;64:135–168. doi: 10.1146/annurev-psych-113011-143750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Miyake A, Emerson MJ, Friedman NP. Assessment of executive functions in clinical settings: problems and recommendations. Semin Speech Lang. 2000;21:169–183. doi: 10.1055/s-2000-7563. [DOI] [PubMed] [Google Scholar]
- 12.Selva G, Salazar J, Balanza-Martinez V, et al. Bipolar I patients with and without a history of psychotic symptoms: do they differ in their cognitive functioning? J Psychiatr Res. 2007;41:265–272. doi: 10.1016/j.jpsychires.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 13.Godard J, Baruch P, Grondin S, et al. Psychosocial and neurocognitive functioning in unipolar and bipolar depression: a 12-month prospective study. Psychiatry Res. 2012;196:145–153. doi: 10.1016/j.psychres.2011.09.013. [DOI] [PubMed] [Google Scholar]
- 14.Fraser LM, O’Carroll RE, Ebmeier KP. The effect of electroconvulsive therapy on autobiographical memory: a systematic review. J ECT. 2008;24:10–17. doi: 10.1097/YCT.0b013e3181616c26. [DOI] [PubMed] [Google Scholar]
- 15.Prudic J. Strategies to minimize cognitive side effects with ECT: aspects of ECT technique. J ECT. 2008;24:46–51. doi: 10.1097/YCT.0b013e31815ef238. [DOI] [PubMed] [Google Scholar]
- 16.Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry. 2000;57:581–590. doi: 10.1001/archpsyc.57.6.581. [DOI] [PubMed] [Google Scholar]
- 17.Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT. 2000;16:87–96. doi: 10.1097/00124509-200006000-00001. [DOI] [PubMed] [Google Scholar]
- 18.Schat A, van den Broek WW, Mulder PG, et al. Changes in everyday and semantic memory function after electroconvulsive therapy for unipolar depression. J ECT. 2007;23:153–157. doi: 10.1097/yct.0b013e318065aa0c. [DOI] [PubMed] [Google Scholar]
- 19.Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med. 1993;328:839–846. doi: 10.1056/NEJM199303253281204. [DOI] [PubMed] [Google Scholar]
- 20.Bosboom PR, Deijen JB. Age-related cognitive effects of ECT and ECT-induced mood improvement in depressive patients. Depress Anxiety. 2006;23:93–101. doi: 10.1002/da.20144. [DOI] [PubMed] [Google Scholar]
- 21.Fujita A, Nakaaki S, Segawa K, et al. Memory, attention, and executive functions before and after sine and pulse wave electroconvulsive therapies for treatment-resistant major depression. J ECT. 2006;22:107–112. doi: 10.1097/00124509-200606000-00006. [DOI] [PubMed] [Google Scholar]
- 22.Semkovska M, McLoughlin DM. Objective cognitive performance associated with electroconvulsive therapy for depression: a systematic review and meta-analysis. Biol Psychiatry. 2010;68:568–577. doi: 10.1016/j.biopsych.2010.06.009. [DOI] [PubMed] [Google Scholar]
- 23.Calev A. Neuropsychology and ECT: past and future research trends. Psychopharmacol Bull. 1994;30:461–469. [PubMed] [Google Scholar]
- 24.Ingram A, Saling MM, Schweitzer I. Cognitive side effects of brief pulse electroconvulsive therapy: a review. J ECT. 2008;24:3–9. doi: 10.1097/YCT.0b013e31815ef24a. [DOI] [PubMed] [Google Scholar]
- 25.Fernie G, Bennett DM, Currie J, et al. Detecting objective and subjective cognitive effects of electroconvulsive therapy: intensity, duration and test utility in a large clinical sample. Psychol Med. 2014;44:2985–2994. doi: 10.1017/S0033291714000658. [DOI] [PubMed] [Google Scholar]
- 26.Sackeim HA, Prudic J, Fuller R, et al. The cognitive effects of electroconvulsive therapy in community settings. Neuropsychopharmacol. 2007;32:244–254. doi: 10.1038/sj.npp.1301180. [DOI] [PubMed] [Google Scholar]
- 27.Semkovska M, Keane D, Babalola O, et al. Unilateral brief-pulse electroconvulsive therapy and cognition: effects of electrode placement, stimulus dosage and time. J Psychiatr Res. 2011;45:770–780. doi: 10.1016/j.jpsychires.2010.11.001. [DOI] [PubMed] [Google Scholar]
- 28.Sackeim HA, Prudic J, Devanand DP, et al. A prospective, randomized, double-blind comparison of bilateral and right unilateral electroconvulsive therapy at different stimulus intensities. Arch Gen Psychiatry. 2000;57:425–434. doi: 10.1001/archpsyc.57.5.425. [DOI] [PubMed] [Google Scholar]
- 29.Ranjkesh F, Barekatain M, Akuchakian S. Bifrontal versus right unilateral and bitemporal electroconvulsive therapy in major depressive disorder. J ECT. 2005;21:207–210. doi: 10.1097/01.yct.0000187041.79087.59. [DOI] [PubMed] [Google Scholar]
- 30.Sackeim HA, Prudic J, Nobler MS, et al. Effects of pulse width and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. Brain Stimul. 2008;1:71–83. doi: 10.1016/j.brs.2008.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Loo CK, Katalinic N, Martin D, et al. A review of ultrabrief pulse width electroconvulsive therapy. Ther Adv Chronic Dis. 2012;3:69–85. doi: 10.1177/2040622311432493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.McCall WV, Dunn A, Rosenquist PB, et al. Markedly suprathreshold right unilateral ECT versus minimally suprathreshold bilateral ECT: antidepressant and memory effects. J ECT. 2002;18:126–129. doi: 10.1097/00124509-200209000-00003. [DOI] [PubMed] [Google Scholar]
- 33.Kellner CH, Knapp R, Husain MM, et al. Bifrontal, bitemporal and right unilateral electrode placement in ECT: randomised trial. Br J Psychiatry. 2010;196:226–234. doi: 10.1192/bjp.bp.109.066183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Spaans HP, Verwijk E, Comijs HC, et al. Efficacy and cognitive side effects after brief pulse and ultrabrief pulse right unilateral electroconvulsive therapy for major depression: a randomized, double-blind, controlled study. J Clin Psychiatry. 2013;74:e1029–1036. doi: 10.4088/JCP.13m08538. [DOI] [PubMed] [Google Scholar]
- 35.APA. Diagnostic and statistical manual-text revision. American Psychiatric Association; 2000. (DSM-IV-TR, 2000) [Google Scholar]
- 36.Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33. [PubMed] [Google Scholar]
- 37.Shelton JT, Elliott EM, Matthews RA, et al. The relationships of working memory, secondary memory, and general fluid intelligence: working memory is special. J Exp Psychol Learn Mem Cogn. 2010;36:813–820. doi: 10.1037/a0019046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wechsler D. Wechsler Adult Intelligence Scale- Forth Edition (WAIS-IV) Pearson Education, Inc; San Antonio, TX: 2008. [Google Scholar]
- 39.Benedict RHB, Schretlen D, Groninger L, et al. Hopkins Verbal Learning Test Revised: Normative data and analysis of inter-form and test-retest reliability. Clin Neuropsychol. 1998;12:43–55. [Google Scholar]
- 40.Benedict RHB, Schretlen D, Groninger L, et al. Revision of the brief visuospatial memory test: Studies of normal performance, reliability, and validity. Psychol Assessment. 1996;8:145–153. [Google Scholar]
- 41.Wechsler D. Advanced Clinical Solutions for the WAIS-IV and WMS-IV (ACS) Pearson Education, Inc; San Antonio, TX: 2009. [Google Scholar]
- 42.Reitan RM, Wolfson D. Category test and trail making test as measures of frontal lobe functions. The Clinical Neuropsychologist. 1995;9:50–56. [Google Scholar]
- 43.Stroop JR. Studies of interference in serial verbal reactions [Ph D] Nashville, Tenn: George Peabody College for Teachers; 1935. [Google Scholar]
- 44.Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Williams JB, Kobak KA. Development and reliability of a structured interview guide for the Montgomery Asberg Depression Rating Scale (SIGMA) Br J Psychiatry. 2008;192:52–58. doi: 10.1192/bjp.bp.106.032532. [DOI] [PubMed] [Google Scholar]
- 46.Tombaugh TN, Rees L, McIntyre N. A compendium of neuropsychological tests: Administration, norms and commentary. 2. New York: Oxford University Press; 1998. Normative data for the Trail Making Test. Personal communication cited in Spreen and Strauss. [Google Scholar]
- 47.Verwijk E, Comijs HC, Kok RM, et al. Neurocognitive effects after brief pulse and ultrabrief pulse unilateral electroconvulsive therapy for major depression: a review. J Affect Disord. 2012;140:233–243. doi: 10.1016/j.jad.2012.02.024. [DOI] [PubMed] [Google Scholar]
- 48.Falconer DW, Cleland J, Fielding S, et al. Using the Cambridge Neuropsychological Test Automated Battery (CANTAB) to assess the cognitive impact of electroconvulsive therapy on visual and visuospatial memory. Psychol Med. 2010;40:1017–1025. doi: 10.1017/S0033291709991243. [DOI] [PubMed] [Google Scholar]
- 49.Maric NP, Stojanovic Z, Andric S, et al. The acute and medium-term effects of treatment with electroconvulsive therapy on memory in patients with major depressive disorder. Psychol Med. 2016;46:797–806. doi: 10.1017/S0033291715002287. [DOI] [PubMed] [Google Scholar]
- 50.Bodnar A, Krzywotulski M, Lewandowska A, et al. Electroconvulsive therapy and cognitive functions in treatment-resistant depression. World J Biol Psychiatry. 2016;17:159–164. doi: 10.3109/15622975.2015.1091501. [DOI] [PubMed] [Google Scholar]
- 51.Joshi SH, Espinoza RT, Pirnia T, et al. Structural Plasticity of the Hippocampus and Amygdala Induced by Electroconvulsive Therapy in Major Depression. Biol Psychiatry. 2016;79:282–292. doi: 10.1016/j.biopsych.2015.02.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Pirnia T, Joshi SH, Leaver AM, et al. Electroconvulsive therapy and structural neuroplasticity in neocortical, limbic and paralimbic cortex. Transl Psychiatry. 2016;6:e832. doi: 10.1038/tp.2016.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Lyden H, Espinoza RT, Pirnia T, et al. Electroconvulsive therapy mediates neuroplasticity of white matter microstructure in major depression. Transl Psychiatry. 2014;4:e380. doi: 10.1038/tp.2014.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Leaver AM, Espinoza R, Pirnia T, et al. Modulation of intrinsic brain activity by electroconvulsive therapy in major depression. Biol Psychiatry Cogn Neurosci Neuroimaging. 2016;1:77–86. doi: 10.1016/j.bpsc.2015.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Nordanskog P, Larsson MR, Larsson EM, et al. Hippocampal volume in relation to clinical and cognitive outcome after electroconvulsive therapy in depression. Acta Psychiatr Scand. 2014;129:303–311. doi: 10.1111/acps.12150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Lekwauwa R, McQuoid D, Steffens DC. Hippocampal volume is associated with physician-reported acute cognitive deficits after electroconvulsive therapy. J Geriatr Psychiatry Neurol. 2006;19:21–25. doi: 10.1177/0891988705284724. [DOI] [PubMed] [Google Scholar]
- 57.Diehl DJ, Keshavan MS, Kanal E, et al. Post-ECT increases in MRI regional T2 relaxation times and their relationship to cognitive side effects: a pilot study. Psychiatry Res. 1994;54:177–184. doi: 10.1016/0165-1781(94)90005-1. [DOI] [PubMed] [Google Scholar]
- 58.Sackeim HA. Autobiographical memory and electroconvulsive therapy: do not throw out the baby. J ECT. 2014;30:177–186. doi: 10.1097/YCT.0000000000000117. [DOI] [PMC free article] [PubMed] [Google Scholar]