

Abstract
The most common discrepancy concerning tooth size is the presence of peg-shaped lateral incisors, which can cause teeth with reduced size, anterior diastema, and consequently an unpleasant smile. The development of the adhesive dentistry and ceramic veneers allowed all ceramic-bonded restorations to become an esthetic and functional approach to reestablish the smile harmony. The purpose of this clinical report is to describe a conservative treatment approach to recover an esthetic disharmony caused by bilateral peg-shaped lateral incisors. A 30-year-old female patient was seeking treatment to solve an esthetic disharmony of her smile. Lithium disilicate veneers were planned and build-up with the help of diagnostic models, wax-up, mock-up, and silicone guides, to restore the morphology, size, function, and esthetic of upper lateral incisors and smile. The lithium disilicate veneers were able to provide the harmonization of the patient's smile, recovering the teeth size, shape, and anatomic characteristics.
Keywords: Dental cement, dental esthetics, dental veneers, lithium disilicate
INTRODUCTION
The smile is one of the most important components of perception and self-perception of people.[1] It directly influences the facial expression and physical attractiveness of individuals.[1] People with beautiful and harmonic smiles are directly associated with positive characteristics such as intelligence, good health, friendliness, and extroversion.[1]
The major complaining about esthetic disharmony often involves anterior teeth alteration of color,[2] position,[3] shape, and size.[4] The conical crown-size reduction, also known as peg-shaped, of upper lateral incisors was reported to be higher than the prevalence of other morphological variations of permanent teeth.[5] The prevalence of peg-shaped maxillary permanent lateral incisors in the world population is one for every 55 (1.8%).[5] Yet, women have 1.35 more chance of having peg-shaped maxillary permanent lateral incisors when compared to men.[5] The spaces provoked by the teeth shape and size cause a disharmony in smile that retains the attention of the observer. According to literature, some DNA binding is responsible for genetic defects, resulting in peg-shaped upper lateral incisors that may be associated or not with other dental anomalies, such as tooth agenesis.[6]
Advances in esthetic restorative techniques and materials have helped dentists to offer better treatments to patients. Several techniques have been proposed to solve problems related to the morphology of the teeth, especially related to lateral incisors.[7,8] Treatment options may vary depending on different clinical aspects. In this way, laminated ceramic veneers appear to be a conservative treatment option for these situations, since in some cases, no tooth preparation is required.[7] Currently, dental adhesives and resin cement are able to produce a strong and stable bonding to dental structures, especially to enamel. On this way, the use of laminated veneers is strongly indicated to restore or even promote the harmony of the smile. Yet, laminated ceramic veneers have mechanical, optical, and physical properties that allow a perfect mimicry of the natural teeth esthetic and function.[9]
Thus, the aim of this case report is to describe a minimal intervention dentistry approach to recover disharmony caused by bilateral peg-shaped upper lateral incisors using indirect lithium disilicate ceramic-laminated veneers.
CASE REPORT
Diagnostic and treatment planning
A 30-year-old female patient attended the dental clinic with a chief complaint about the esthetic appearance of her smile due to the form and shape of their upper lateral incisors [Figure 1a–d]. The intraoral clinical examination revealed a disharmonious smile caused by bilateral peg-shaped incisors [Figure 1a–d]. The patient had good periodontal health and a stable intercuspal position, normal vertical and horizontal overlap, and canine-protected guidance. Clinical examination and radiography survey demonstrated adequate and healthy tooth structure, bone support, and the absence of periapical pathologies. One study cast was made as a supplementary tool to enhance the diagnostic stage [Figure 2a]. To simulate the teeth shape design and enhance the patient understanding of proposed treatment plan, a wax setup was made in the study cast [Figure 2b]. Then, an impression with addition silicone (Virtual, Ivoclar Vivadent, Brazil) was obtained to use the wax setup for the fabrication of a mock-up [Figure 2c]. Then, temporary mock-up veneers were created with a self-cure bisacrylic resin (Systemp, Ivoclar Vivadent, Brazil) [Figure 2d]. Once the patient has been satisfied with the result of the mock-up, a conservative treatment using indirect lithium disilicate veneers was performed.
Figure 1.

(a) The initial appearance of patient's smile, (b) intraoral view of the patient's dental status, (c and d) close-up of the peg-shaped upper lateral incisors
Figure 2.
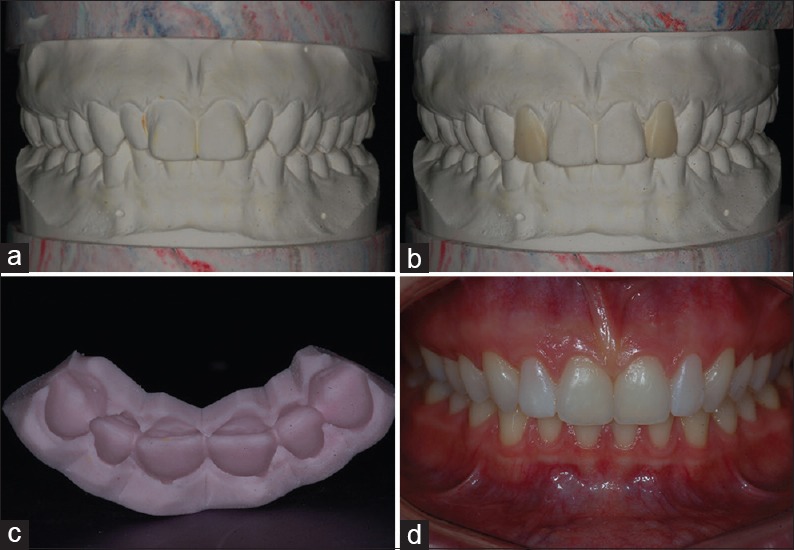
(a) Study model, (b) diagnostic wax-up, (c) waxing impression, and (d) analysis and adjustment of mock-up
Thus, teeth were cleaned with pumice and tooth shades were determined by comparison with a shade guide (Vitapan Classical, VITA Zahnfabrik, Germany). After that, retraction cords were placed in the gingival sulcus of the lateral incisors and a two-step impression was performed using heavy and light silicone. Later, the impression was sent to the prosthesis laboratory for the fabrication of two glass-ceramic lithium disilicate veneers (IPS e.max Press, Ivoclar Vivadent, Brazil).
Cementation procedures
After fabrication of ceramic veneers by the prosthetic [Figure 3a], the proof and cementation protocol were initiated. The ceramic veneers were etched with hydrofluoric acid at 10% for 20 s, and subsequently, rinsed with copious amounts of distilled water for 1 min. Then, the pieces were dried and were performed the active application of silane coupling agent for 1 min [Figure 3b], to promote the solvent evaporation. Then, a double layer of the adhesive system (ExciteF, Ivoclar Vivadent, Brazil) was applied on the surface. The teeth were isolated with cotton rolls, tiger tape, in conjunction with a saliva ejector. The enamel surface was etched for 30 s using a 37% phosphoric acid etchant [Figure 3c], rinsed abundantly with water, and subsequently dried with jets of air [Figure 3d]. Two consecutive coats of ExciteF adhesive system were applied to the enamel surface with a fully saturated brush tip, being gently air dried for 5 s [Figure 3e] and light-cured for 20 s, using a light-emitting diode (LED) curing unit (Radii-cal, SDI, Australia) at 1.200 mW/cm2. Finally, light-curing resinous cement was used to cement the ceramic laminates (Variolink Veneer, Ivoclar Vivadent, Brazil) on the surface of laminate porcelain veneers. The laminate veneers were placed in position, the gross excess was removed with a microbrush, and the photoactivation was performed for 60 s with a LED curing unit (Radii-cal, SDI, Australia) at 1.200 mW/cm2 [Figure 3f]. After that, a careful removal of small excess of resin cement was performed with a number 12 scalpel blade, followed by a three-step polishing system with a flame-shaped diamond finisher, a flame-shaped diamond polisher, and finally, a diamond paste and bristle brush (OptraFine, Ivoclar Vivadent, Brazil). The final aspect of the treatment can be observed in the Figure 4a–d.
Figure 3.

(a) Lithium disilicate veneers, (b) silane (left) and adhesive application (right), (c) phosphoric acid application at 37% on enamel for 30 s, (d) enamel appearance after acid etching, rinsing, and drying, (e) adhesive application, and (f) veneers in position and gross excess removal
Figure 4.

(a and b) Close-up of the veneers in position after gentle removal of the resin cement excess, (c and d) final appearance of patient's smile
DISCUSSION
The esthetic treatment in patients with peg-shaped lateral incisors frequently includes the anatomy correction of malformed teeth and the closure of diastema spaces.[7,8,9] However, in the clinical case presented here, the patient had no diastema between upper canines or upper central incisors. Therefore, the goal of the ceramic restoration was only correct the dental shape and volume. In clinical cases, where patients present small diastema, direct bonding restorations can be a treatment choice. It is a conservative, esthetic, and cost-effective option, especially in cases where occlusal problems are absent.[8] However, color stability and retention of polishing are some limitations of composite resin restorations in esthetic areas in the long-term.[10] Therefore, the indirect ceramic veneers were the material and treatment choice.
Another important factor to the simple resolution of this case is that the patient had a perfect health and gingival alignment. On the other hand, in many cases, gingival alignment corrections are necessary. However, the esthetic results are also very interesting.[9] Likewise, no tooth alignment correction was necessary. Since often, the association of restorative, orthodontic, and periodontal techniques is essential for a beautiful and functional outcome.[6,11,12]
The different treatment options must be carefully explained to the patient, including the advantages and limitations of each technique, which will help the patient in the treatment selection. In the case here presented, together with the professional, the patient chose indirect ceramic veneers, considering that this treatment would provide predictable esthetic results with minimal or none teeth preparation. For help in choosing the most appropriate treatment, study cast models and diagnostic wax-up were useful to enhance the evaluation of anatomical features, occlusion analysis, and restoration design, helping the patient visualization of the anticipated esthetic result.[8] Another advantage of the wax-up is the possibility to carry out a silicone index and mock-up.[8] The bisacrylic resin greatly facilitated the technique for mock-up obtainment.[8]
Under the perspective of adhesion, a total etch technique adhesive system was used. These adhesive systems have produced high bond strength values when bonded to enamel.[13] In addition, since that in the clinical case here reported, the entire adhesion area was located in enamel without dentin exposition; the long-term results may be more favorable, once the adhesion to enamel is stronger and more stable than adhesion to dentin.[13]
CONCLUSION
This clinical case report demonstrated the possibility of a simple treatment with high esthetic and functional performance, producing patient satisfaction.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Montero J, Gómez Polo C, Rosel E, Barrios R, Albaladejo A, López-Valverde A. The role of personality traits in self-rated oral health and preferences for different types of flawed smiles. J Oral Rehabil. 2016;43:39–50. doi: 10.1111/joor.12341. [DOI] [PubMed] [Google Scholar]
- 2.Joiner A. The bleaching of teeth: A review of the literature. J Dent. 2006;34:412–9. doi: 10.1016/j.jdent.2006.02.002. [DOI] [PubMed] [Google Scholar]
- 3.Miro AJ, Shalman A, Morales R, Giannuzzi NJ. Esthetic smile design: Limited orthodontic therapy to position teeth for minimally invasive veneer preparation. Dent Clin North Am. 2015;59:675–87. doi: 10.1016/j.cden.2015.04.001. [DOI] [PubMed] [Google Scholar]
- 4.Witt M, Flores-Mir C. Laypeople's preferences regarding frontal dentofacial esthetics: Tooth-related factors. J Am Dent Assoc. 2011;142:635–45. doi: 10.14219/jada.archive.2011.0245. [DOI] [PubMed] [Google Scholar]
- 5.Bäckman B, Wahlin YB. Variations in number and morphology of permanent teeth in 7-year-old Swedish children. Int J Paediatr Dent. 2001;11:11–7. doi: 10.1046/j.1365-263x.2001.00205.x. [DOI] [PubMed] [Google Scholar]
- 6.Steiner-Oliveira C, Gavião MB, dos Santos MN. Congenital agenesis of premolars associated with submerged primary molars and a peg-shaped lateral incisor: A case report. Quintessence Int. 2007;38:435–8. [PubMed] [Google Scholar]
- 7.Ittipuriphat I, Leevailoj C. Anterior space management: Interdisciplinary concepts. J Esthet Restor Dent. 2013;25:16–30. doi: 10.1111/j.1708-8240.2012.00515.x. [DOI] [PubMed] [Google Scholar]
- 8.Scarpelli AC, Reboucas AP, Compart T, Novaes-Júnior JB, Paiva SM, Pordeus IA. Seven-year follow-up of esthetic alternative for the restoration of peg-shaped incisors: A case study of identical twins. Gen Dent. 2008;56:74–7. [PubMed] [Google Scholar]
- 9.Soares PV, Spini PH, Carvalho VF, Souza PG, Gonzaga RC, Tolentino AB, et al. Esthetic rehabilitation with laminated ceramic veneers reinforced by lithium disilicate. Quintessence Int. 2014;45:129–33. doi: 10.3290/j.qi.a31009. [DOI] [PubMed] [Google Scholar]
- 10.Garber DA. Direct composite veneers versus etched porcelain laminate veneers. Dent Clin North Am. 1989;33:301–4. [PubMed] [Google Scholar]
- 11.Schmitz JH, Coffano R, Bruschi A. Restorative and orthodontic treatment of maxillary peg incisors: A clinical report. J Prosthet Dent. 2001;85:330–4. doi: 10.1067/mpr.2001.114684. [DOI] [PubMed] [Google Scholar]
- 12.Tausche E, Harzer W. Treatment of a patient with class II malocclusion, impacted maxillary canine with a dilacerated root, and peg-shaped lateral incisors. Am J Orthod Dentofacial Orthop. 2008;133:762–70. doi: 10.1016/j.ajodo.2006.09.052. [DOI] [PubMed] [Google Scholar]
- 13.De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et al. A critical review of the durability of adhesion to tooth tissue: Methods and results. J Dent Res. 2005;84:118–32. doi: 10.1177/154405910508400204. [DOI] [PubMed] [Google Scholar]