

Abstract
Purpose/objectives
Despite mounting evidence for the use of re-irradiation (re-RT) in recurrent high grade glioma, optimal patient selection criteria for re-RT remain unknown. We present a novel scoring system based on radiobiology principles including target independent factors, the likelihood of target control, and the anticipated organ at risk (OAR) toxicity to allow for proper patient selection in the setting of recurrent glioma.
Materials/methods
Thirty one patients with recurrent glioma who received re-RT (2008–2016) at NCI – NIH were included in the analysis. A novel scoring system for overall survival (OS) and progression free survival (PFS) was designed to include:1) target independent factors (age, KPS (Karnofsky Performance Status), histology, presence of symptoms), 2) target control, and 3) OAR toxicity risk. Normal tissue complication probability (NTCP) calculations were performed using the Lyman model. Kaplan-Meier analysis was performed for overall survival (OS) and progression free survival (PFS) for comparison amongst variables.
Results
No patient, including those who received dose to OAR above the published tolerance dose, experienced any treatment related grade 3–5 toxicity with a median PFS and OS from re-RT of 4 months (0.5–103) and 6 months (0.7–103) respectively. Based on cumulative maximum doses the average NTCP was 25% (0–99%) for the chiasm, 21% (0–99%) for the right optic nerve, 6% (0–92%) for the left optic nerve, and 59% (0–100%) for the brainstem. The independent factor and target control scores were each statistically significant for OS and the combination of independent factors plus target control was also significant for both OS (p = 0.02) and PFS (p = 0.006). The anticipated toxicity risk score was not statistically significant.
Conclusion
Our scoring system may represent a novel approach to patient selection for re-RT in recurrent high grade glioma. Further validation in larger patient cohorts including compilation of doses to tumor and OAR may help refine this further for inclusion into clinical trials and general practice.
Electronic supplementary material
The online version of this article (10.1186/s13014-017-0930-9) contains supplementary material, which is available to authorized users.
Background
Survival following concurrent radiation (RT) and temozolomide (TMZ) as per the EORTC 26981/22981-NCIC CE3 trial remains poor with median survival ranging from 39 months in RPA (Recursive Partitioning Analysis) class I patients to 5.2 months in RPA class VI patients [1]. Despite improvements in the detection of distinct molecular signatures [2], increased precision in the administration of radiation therapy and the increasing availability of targeted and non-targeted systemic agents, additional improvements are still needed.
Brain tumor recurrences can be identified by the development of new neurological symptoms, radiographic changes or both [3]. Upon recurrence, the treatment recommendations can vary widely and are partially based on the patient’s performance status, tumor location, and time interval since last treatment. Depending on these factors, options may include re-resection, chemotherapy, re-irradiation (re-RT) or enrollment on a clinical trial [4]. However, tumor re-resection is possible in less than 50% of patients [5] and the response to systemic treatment, if it occurs, is short lived with overall survival (OS) from 7.1 to 9.6 months [4]. For a significant proportion of patients with recurrent glioma in whom re-resection is not possible and for whom systemic options have been exhausted, re-RT has emerged as a possible treatment option.
In multiple retrospective trials, re-RT for brain tumors has been shown to be feasible, with a median OS benefit of 8 months, a progression free survival (PFS) of 5 months and minimal reported significant toxicities [6–15]. Acute toxicities including alopecia, headaches and nausea/vomiting, were mild and well managed with medical therapy, while late CNS toxicity was reported in most retrospective studies at a rate of less than 5%.
Existing scoring systems that may help guide patient selection for re-RT have been validated in some cohorts [10] but not in others [11]. Whilst they all include some common features rated as important by glioma re-RT experts (personal communication), they also differ with respect to inclusion of resection status, recurrent tumor size, patient symptoms and steroid use.
Toxicity attribution in patients with CNS tumors is challenging as both tumor progression and symptomatic radiation necrosis can cause significant clinical decline in the setting of short survival which limits long term evaluation. The current toxicity reporting structure is the Common Terminology Criteria for Adverse Events (CTCAEv4) [16]. For the three organs at risk (OAR) involved when contemplating CNS re-RT, the optic nerves, chiasm and brainstem, the toxicity scales remain imprecise or absent all together. In addition, most re-RT for recurrent glioma is by necessity administered in hypofractionated schedules where toxicity data and the ability to estimate normal tissue complication probabilities is limited. Since 50% of superiorly selected patients can live up to 2 years following re-RT as the systemic therapies become more effective, toxicity estimation in the setting of re-RT will become increasingly important.
In this study, we examined patient outcome using patient and recurrent tumor related factors as well as OAR dose and clinical toxicity information with NTCP calculations in patients who underwent re-RT with commonly used dose fractionation schemes. Despite the lack of a clear definition of toxicity [17–19], While NTCP calculations suggest the possibility of significant toxicity in some patients, clinical data suggests minimal toxicity following re-RT. Our novel scoring system based on the ability to control recurrent tumor, risk of toxicity as well a more traditional scoring parameters (age, histology, symptomatic, disease free interval) with re-RT, may represent a step forward in the selection of patients for re-RT.
Methods and materials
Patients
Thirty one patients with recurrent glioma or gliosarcoma underwent re-RT, at the National Cancer Institute between 2008 and 2016. Chart review and treatment planning information including dose distributions and treatment volumes were collected from both the original and subsequent treatment plans whenever possible. CTCAE v4.0 was employed to define toxicity. The patients were originally treated for glioma or gliosarcoma using IMRT or 3D conformal technique. Dosimetric analysis for NTCP was performed if the original treatment plan could be obtained and if they received their treatment at a fraction size ≤300 cGy [20]. This was possible in 25 patients.
NTCP model and calculation
Maximum and equivalent uniform dose (EUD) for optic chiasm, optic nerves and brain stem were extracted from ECLIPSE™ or the patient’s original treatment plan documents. NTCP calculations were performed using tolerance dose values for the uniform irradiation of critical structures based on literature data and fit by Burman [21] to the NTCP model proposed by Lyman [22]. Original and retreat gross tumor volume (GTV) and planning target volume (PTV) volumes were recorded when available. The original GTV volume was obtained from the original treatment plan and in all cases was based on the T1 gadolinium enhancing component as contoured by the treating radiation oncologist. The original PTV represents the volume treated to the highest dose and is based on the original GTV. For the NTCP calculation involving the maximum dose, the maximum dose to the OAR in the first and re-treatment were obtained, converted to account for dose per fraction, and subsequently added. For the NTCP calculation involving EUD, the mean dose to the organ between the first and re-treatment were added, after adequate contouring of the OAR in both the first and re-treatment plans.
Scoring system
A scoring system was designed to capture the parameters that underlie the administration of re-RT (Table 1). A set of imaging independent factors (target independent score) was made up by: patient age, KPS (Karnofsky Performance Status), histology and the presence of the symptoms. The ability to control the target was based on tumor size (GTV in cm3), tumor recurrence location with respect to original location and the presence of diffuse disease on MRI brain. The anticipated toxicity risk with re-RT administration was evaluated as a function of the location of OAR with respect to previously treated area, the dose contribution to each OAR and disease free interval from the original RT. A score of 1–3 per variable was assigned in each category for a cumulative score ranging from 10 (worst prognosis) to 30 (best prognosis).
Table 1.
Krauze Scoring System
| Prognostics Factor | Subgroups | Value for prognostic score |
|---|---|---|
| Independent Factors | ||
| Patient Age | >60 years | 1 |
| 50–60 years | 2 | |
| <50 years | 3 | |
| KPS | <50% | 1 |
| 50–70% | 2 | |
| >70% | 3 | |
| Histology | WHO Grade IV | 1 |
| WHO Grade III | 2 | |
| WHO Grade II | 3 | |
| Presence of symptoms | Documented neurological symptoms related to recurrence requiring steroid management | 1 |
| Documented neurologicalsymptoms relatedto recurrence or impending neuro symptoms | 2 | |
| No neurological symptoms related to recurrence | 3 | |
| Target Control | ||
| Tumor size (GTV) | >500 cm3 or diffuse disease/ gliomatosis | 1 |
| 20–500 cm3 | 2 | |
| <20 cm3 | 3 | |
| Tumor recurrencelocation withrespect to originaltreatment field (60Gy isodose line) | <1 cm away or completelywithin the original treatment field | 1 |
| 1–3 cm away | 2 | |
| >3 cm away | 3 | |
| Diffuse disease present | Multiple T1 gadolinium- enhancing lesions | 1 |
| T2 FLAIR diffuse involvement | 2 | |
| None (localized recurrence only) | 3 | |
| Anticipated Toxicity Risk | ||
| OAR location with respect to recurrence area | >1 cm away from or in the recurrence area | 1 |
| 1–3 cm away from recurrence area | 2 | |
| >3 cm away from the recurrence area | 3 | |
| OAR dose contribution from original treatmenta | <90% dose allowed as per Quantec dose constraints | 1 |
| Within +/− 10% of dose allowed as per Quantec constraints | 2 | |
| Exceeds >10% over the Quantec constraints | 3 | |
| Disease free interval from initial treatment with radiation | <1 year | 1 |
| 1–3 years | 2 | |
| >3 years | 3 | |
aOAR QUANTEC dose constraints: Chiasm: 55Gy, Optic Nerves: 55Gy, Brain Stem: 54 Gy. WHO World Health Organisation
Results
Patient characteristics
Thirty one patients were included in the analysis. The median age was 47y/o (18-73y), 58% were male, and 81% had a pre re-RT KPS ≥70 (Table 2). 58% of patients were initially diagnosed with a GBM with the majority located in the fronto-parietal lobes. The median disease free interval was 33.7 months (11.4–174). The location of the recurrent tumor was within the previous field in all but 6 patients. During re-RT 13 patients received concurrent systemic therapy in the form of TMZ [4], bevacizumab [5], or both [1].
Table 2.
Patient, Tumor and Treatment Characteristics
| Parameter | N = 31 |
|---|---|
| Age (yrs), median (range) | 47 (18–73) |
| Sex | |
| Male | 18 |
| Female | 13 |
| KPS at time of reRT | |
| ≤ 50 | 1 |
| 50–70 | 5 |
| > 70 | 25 |
| Original histology | |
| WHO grade IV | 18 |
| WHO grade III | 5 |
| WHO grade II | 7 |
| Gliosarcoma | 1 |
| Original tumor location | |
| Frontal | 13 |
| Parietal | 5 |
| Temporal | 3 |
| Occipitoparietal | 1 |
| Temporoparietal | 3 |
| Frontotemporal | 2 |
| Brainstem/Cerebellum | 3 |
| Other | 1 |
| Recurrence location wrt to the 80% isodose line | |
| Within | 25 |
| Outside | 6 |
| Other hemisphere | 1 |
| Brainstem | 2 |
| 4th ventricle/post fossa | 2 |
| Adjacent Lobe | 1 |
| DFS median (range)(months) | 33.7 (11.4–174) |
| Tissue diagnosis prior to re-RT | 22 |
| Concurrent agent administration | 13 |
| Temozolomide alone | 4 |
| Bevacizumab alone | 5 |
| Temozolomide and Bevacizumab | 1 |
| Other | 3 |
| Management upon progression after re-RT | |
| Bevacizumab | 8 |
| BSC | 20 |
| Other (BCNU, study) | 3 |
DFS Disease Free Survival, BSC Best Supportive Care, WHO World Health Organisation
Treatment and volume characteristics
Twenty-five patients for whom the complete original treatment plan was available were included in the dosimetric analysis (Table 3). The original treatment dose was 60Gy (median), with one patient (brainstem tumor) treated to 55.8Gy with 66% of patients treated with IMRT. The median original GTV was 28cm3 (5.8-72 cm3), and the original PTV was 307cm3 (107-601 cm3) (N = 18). Re-RT dose was 30Gy (15-54Gy) with a median retreat GTV of 29cm3 (0.3-313 cm3) and PTV of 124cm3 (0.5–511 cm3) with 77% treated using IMRT. The cumulative BED between the two radiation treatments had a median of 96Gy (72–112Gy). Patients treated with hypofractionated regimens (dose/fraction >300 cGy), were not included in the NTCP analysis due to concerns over the use of the linear quadratic equation as means of dose conversion and the differences in the radiobiological effects at a higher dose per fraction [20]. They represent a patient with cerebellar sarcoma treated upfront with 35Gy in 5 fractions using Cyberknife technique, and 3 additional patients re-irradiated using SRS [1] or SRT [2] technique.
Table 3.
Radiation Treatment Characteristics
| Parameter | N = 31 |
|---|---|
| Dose of original RT (Gy) | |
| Median | 60 |
| Range | 18–60 |
| Original RT technique | |
| 3D conformal | 10 |
| IMRT | 20 |
| Unknown (Plan not available) | 1 |
| Original GTV volume (cm3) | |
| Median | 27.9 |
| Range | 5.8–72 |
| Original PTV volume (cm3) | |
| Mean | 307 |
| Range | 107–601 |
| Interval between original RT and Re-RT (yrs) | |
| Median | 4.28 |
| Range | 0.95–14.5 |
| Re-RT dose (Gy) | |
| Median | 30 |
| Range | 15–54 |
| Re-RT dose per fraction (Gy) | |
| Median | 2.5 |
| Range | 1.8–15 |
| Re-RT technique | |
| 3D conformal | 5 |
| IMRT | 23 |
| 3D conformal with IMRT boost | 2 |
| SRS | 1 |
| Retreat GTV volume (cm3) | |
| Median | 29 |
| Range | 0.3–313 |
| Retreat PTV volume (cm3) | |
| Median | 124 |
| Range | 0.5–511 |
| Cumulative BED (α/β = 2), (Gy) | N = 25 |
| Median | 96 |
| Range | 72–112 |
NTCP calculation
Performing NTCP calculations was possible for 25 of the re-RT patients. During the process of obtaining the volume and dose values from original and subsequent treatment plans, we noted that a significant variation can occur in how the OAR are contoured between different providers. Using CNS contouring atlases [23, 24] (IMAIOS SAS Anatomy, IMAIOS SAS, www.imaios.com, www.qarc.org/cog/ACNS0331Atlas.pdf) we re-contoured OAR structures to enable a more adequate calculation of mean dose to the organ (Fig. 1). In addition, when adding plans using the “plan sum” function in Eclipse™ inconsistent values often resulted due to changes in volume contouring, location of OAR maximal point dose and treatment technique. In order to avoid these inconsistent results we collected the max and mean values from the respective plans, converted them to account for BED, and then manually added the values (Fig. 1 and Additional file 1: Table S1A and B) as previously described in dose tolerance literature [25, 26].
Fig. 1.
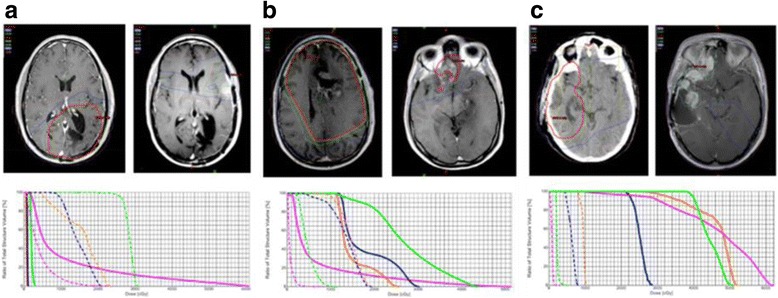
Initial treatment and reRT dose distribution with corresponding dose volume histogram (DVH) for the first (solid lines) and second (dashed lines) radiation plans. Possible scenarios are displayed: (a) dose to OAR lower than accepted dose constraints, (b) OAR barely meeting dose constraints, and (c) OAR above accepted constraints. Green = optic chiasm, Pink = brain stem, Blue = left optic nerve, Orange = right optic nerve
Toxicity and NTCP
Based on the cumulative maximum doses received from the first and the second courses of radiation, the average NTCP was 25% (0–99%) for the chiasm, 21% (0–99%) for the right optic nerve, 6% (0–92%) for the left optic nerve, and 59% (0–100%) for the brainstem (Additional file 2: Figure S1A and Additional file 1: Table S1A). Based on the mean (EUD) doses the average NTCP was 11% (0–91%) for the chiasm, 5% (0–50%) for the right optic nerve, 0% (0–4%) for the left optic nerve, 5% (0–92%) for the brainstem (Additional file 2: Figure S1B and Additional file 1: Table S1B). As per chart documentation and ongoing follow-up, no patient including those who received dose to OAR above the published tolerance dose, experienced any treatment related grade 3–5 toxicity. At the time of re-RT initiation, 39% of the patients were on steroids for symptom management, and an additional patient was started on steroids during re-RT. Pretreatment KPS was maintained for 45% of the patients at 1 month. The decline in KPS correlated with documentation of tumor progression outside the re-RT field in all patients. The two patients who had the highest NTCP to chiasm, optic nerves and brainstem survived 8 and 15 months from retreatment, respectively. Aside from fatigue and alopecia, no significant side effects that could be attributed to re-RT were observed.
Scoring system
Using the new scoring system (Table 1), we analyzed the impact of target control and the anticipated toxicity risk on OS and PFS for all re-RT patients using Kaplan-Meier analysis (Fig. 2). The independent factor subgroup was statistically significant for both OS and PFS but the target control subgroup was only significant for OS and not PFS. The anticipated toxicity risk subgroup was not statistically significant for either OS or PFS. Furthermore, the combination of the independent factor subgroup and target control subgroup was statistically significant for both OS and PFS (Fig. 3). Moreover, the presence of symptoms prior to re-RT and KPS were statistically significant for OS. Thus, using clinical parameters (age, KPS, histology and symptoms) in combination with tumor radiobiological parameters (volume, total dose, unifocal) a modified scoring system has been derived that may stratify patients better than the currently available scoring systems.
Fig. 2.
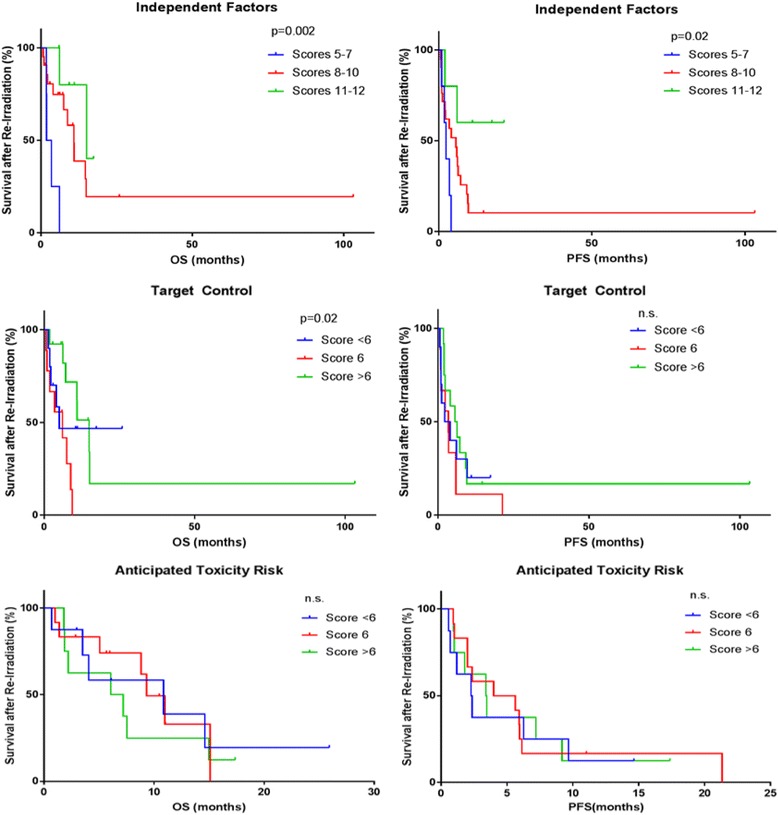
Kaplan-Meier analysis pf progression-free survival (PFS) and overall survival (OS) in re-RT patients by independent factors, anticipated target control and anticipated toxicity risk control
Fig. 3.
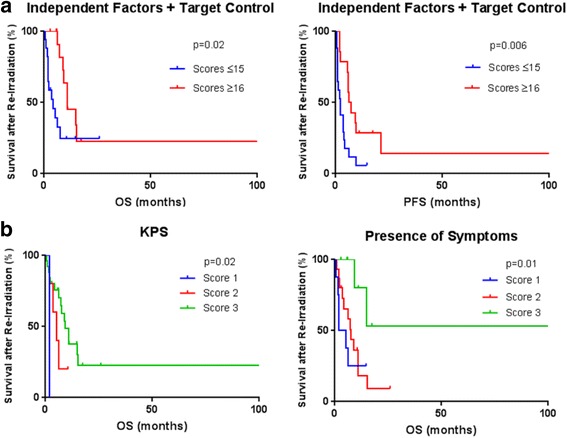
a. Kaplan-Meier analysis of overall survival (OS) and progression-free survival (PFS) and in re-RT patients by independent factors + target control. b. Kaplan-Meier analysis of overall survival (OS) by presence of symptoms and Karnofsky Performance Status (KPS)
Discussion
With the use of advanced therapy techniques and careful treatment planning, for the most part, physicians are able to minimize dose to previously radiated OAR allowing safe re-RT of brain tumor recurrences with an improvement in OS and PFS (6–15). According to the nomogram developed by Combs et al., 50% of patients with a score of 2 (i.e. GBM patients <50 year old) survive at least another 12 months from the time of re-RT [1]. Thus, a more thorough understanding of the potential toxicities that may occur after tumor re-RT are needed. Although acute toxicities in the form of alopecia, headaches and nausea/vomiting have been reported, they are self-limited and controlled with medical management. Likewise, late CNS toxicity remains underreported but in most retrospective studies is less than 5%. In our cohort of 31 patients we had no grade 3, 4 or 5 acute or late toxicities with a median PFS of 4 months (range 0.5–103 months) and OS of 6 months (range 0.7–103 months), a range in keeping with both existing validated prognostic scores [1, 11] and retrospective data.
When working on a re-RT plan for a CNS patient, the physician can use two normal tissue dose reports Emami, 1991 [27] and Quantec 2010 [17–19] to help them decide the safety of the proposed treatment as well as the side effect profile to report to the prospective patient. Additionally, mathematical models using the Lyman–Kutcher–Burman NTCP [21] based on dose have been implemented in an attempt to calculate NTCP [28]. However, several problems arise with toxicity attribution. These include the lack of reliable toxicity estimation, the relatively short PFS and OS times, the overlapping symptoms of re-RT toxicity and tumor recurrence and the concurrent or adjuvant administration of systemic agents that can alter radioresponse and toxicity measurements. Our analysis suggests that the Emami and Quantec papers and the NCTP calculations appear to overestimate the rates of clinical toxicity.
To our knowledge ours is the only paper examining NTCP and cumulative dose in the setting of re-RT for gliomas. Calculation of the cumulative dose to OAR by creating a “plan sum” for the two treatment plans was found to often result in erroneous cumulative dose to OAR hence manual summation of dose delivered was employed to calculate NTCP in this study. Nonetheless, the calculated NTCP using maximum doses to OAR between the two different treatment plans was as high as 100% in the case of all four major OAR. An expected difference in NTCP was observed when mean dose (EUD) [29] versus max dose were employed for its calculation. Considering the lack of toxicity observed, we propose that NTCP calculations based on EUD may represent a more accurate estimation of risk. Mean dose may be both more accurate and more realistic [30, 31] due to its decreased dependency on biologic parameters, including alpha/beta ratio. This raises the question as to whether the OAR in question behaves as serial, parallel or serial-parallel in terms of toxicity and this is yet unclear [32, 33].
Additionally, neither dose per fraction nor time between the two radiation treatments, or the use of concurrent agents all of which may play a significant role in the development of treatment related toxicity, are currently accounted for when calculating NTCP. The impact of concurrent chemotherapy is unclear in the re-RT setting and may further defined by results of ongoing trialssuch as RTOG1205) which explores concurrent bevacizumab, NCT02709226 (Krauze et al.) allowing both concurrent temozolomide and bevacizumab and upcoming trials that explore concurrent temozolomide. Furthermore, most patients who receive re-RT tend to be younger with superior performance status and patient age has been shown to have some correlation with the development of toxicity or lack thereof [17]. This is an important factor when considering the lack of toxicity noted in this study. Limitations to our data include long recruiting times for the patient cohort and inability to carry out NTCP calculations in all patients Long recruiting times for the patient cohort add to the heterogeneity of the data, they are however unavoidable as patients who are referred for re-RT are often referred by virtue of the fact that they have a long disease free interval and a change in the treatment technique is therefore also more likely as technology evolves. However, our data does not suggest that technique played a role. We did note that patients who received 3D conformal RT the first time were more likely to receive IMRT on re-RT in order to decrease dose to OAR. NCTP calculations were only possible for 25 of 31 patients due to the following limitations: 1) inability to obtain the first radiation treatment plan often due to a longer time period since previous treatment (>5 years) or loss of the previous planning data and 2) use of a non conventional fractionation scheme, ie a hypofractionated scheme wherein usage of the linear quadratic equation for BED calculation is not generally accepted [20]. This does limit the results of the study in that it reduced the overall data available, however overall the results obtained do reflect a more homogenous set of dose fractionation schemes, which are employed in ongoing and upcoming prospective trials. It is likely that the inclusion of patients who were treated with hypofractionated schemes would potentially alter the conclusions since a higher level of late toxicity may be postulated. Of note, previous treatment plans are often labor intensive to difficult to obtain and integrate with the re-irradiation plan and thus re-irradiation may be practiced in the community without evaluation of the previous plan raising the issue of cumulative dose to OAR and hence the lack of retrospective data to produce superior models for NTCP in the re-RT setting.
The identification of true toxicity and its relationship to dose, will require 1) greater reporting of dose to OAR after re-RT and 2) robust testing for potential OAR toxicity, including visual field testing, audiology, neurocognitive function and quality of life assessment. Baseline visual field testing although inconsistently obtained is more commonly carried out and thus may more readily provide information on OAR toxicity in the short term. However, visual evoked potentials may represent a more accurate modality of assessing toxicity to the visual apparatus and bears consideration for inclusion in prospective clinical trials [32]. The lack of such data in the literature delegates estimation of risk to retrospective studies and models that are inadequate thus, making already challenging patient discussions and decision making, even more so.
When applying either the Carson 2007 [34] or the Combs 2013 [1] scoring system to our data, we did not achieve a statistically significant separation of the curves (Additional file 3: Figure S2) as has been noted in other published dataset comparisons [9], this however may reasonably be related to the small sample size in our study as compared to that of other authors Unlike the Carson 2007 scoring system, the Combs 2013 scoring system does not include KPS or steroid use but does include time since previous RT in addition to age and histology. Our scoring system considers the likelihood of controlling the recurrent tumor (target control) based on tumor size, tumor location and presence of diffuse disease parameters derived from our own practice and review of the practice and that of other radiation prominent oncologists (personal communication). In our analysis, the tumor control subgroup was highly significant for OS. In addition, we have shown that while KPS matters in terms of OS with re-RT, it is the patient’s symptomatic or asymptomatic status, which may be a more important surrogate of both PFS and OS. This indicates that parameters, currently not included in existing scoring systems may represent reasonable additions to a universally validated scoring system. The use of steroids is a challenging parameter for OS or PFS or for that matter as a study endpoint, as a significant proportion of patients is on steroids prior to re-RT, some for symptoms, others prophylactically. We did not find steroid use to be a useful parameter in our study. Steroid use may be helpful although the heterogeneity of its use in terms of doses, dose increases and the inconsistent capture of steroid usage details may make its consistent comparison and inclusion in scoring systems challenging.
This scoring system was developed out of the need to find a better way to select optimal patients for re-RT who stand to gain palliative benefit and for whom the risk of re-RT is considered acceptable. Further validation in larger cohorts will be required to validate and refine target based scoring systems such as this one.
Conclusion
No treatment related complications were observed in re-RT patients included in our study. Existing NTCP calculations based on maximal point dose and mean dose (EUD) to OAR may overestimate NTCP in the re-RT of high grade glioma. Ongoing heterogeneity in the approach to patient selection for re-RT underscores the need for a universally validated tumor and patient characteristics based scoring system.
Additional files
A. maximum Dose and NTCP to OAR based on Maximum Dose values. B. Mean Dose (EUD) and NTCP to OAR based on Mean Dose values. (DOCX 200 kb)
Normal Tissue complication probability (NTCP) (%) vs. A. maximum dose administered to the organ. B. Mean Dose administered to the organ. TheTD65/5 (Maximum Tolerated Dose 50% rate at 5 years at a dose of 65 Gy) curve based on Emami et al. was used to model NTCP using our retrospective data. (DOCX 58 kb)
Comparison with existing scoring systems A. Carson 2007. B. Combs 2013. (DOCX 28 kb)
Acknowledgements
Not applicable.
Funding
This work was supported in part by the Centers for Cancer Research, NCI. #ZIASC 010372.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional files.
Abbreviations
- BED
Biologically Equivalent Dose
- CNS
Central Nervous System
- CTCAE
Common Terminology Criteria for Adverse Events
- EORTC
European Organisation for Research and Treatment of Cancer
- EUD
Equivalent Uniform Dose
- GBM
Glioblastoma
- GTV
Gross Tumour Volume
- IMRT
Intensity Modulated Radiation Therapy
- KPS
Karnofsky Performance Status
- MRI
Magnetic Resonance Imaging
- NCI
National Cancer Institute
- NTCP
Normal Tissue Complication Probability
- OAR
Organs at Risk in the Field
- OS
Overall Survival
- PFS
Progression Free Survival
- PTV
Planning Treatment Volume
- Re-RT
Re-irradiation
- RPA
Recursive Partitioning Analysis
- RT
Radiation Therapy
- SRS
Stereotactic Radiosurgery
- SRT
Stereotactic Radiotherapy
- TMZ
Temozolomide
Authors’ contributions
AVK conceived the study, participated in its design and coordination, collected patient data, performed statistical data analysis and drafted the manuscript. CP collected and organized patient data, performed statistical data analysis. JC conceived and performed NTCP calculations and addressed dosimetry considerations. HN conceived approach to NTCP calculations and addressed dosimetry considerations. MM collected patient data. LR treated patients included in the analysis. TCZ provided research nursing support and enabled data collection and analysis. DS treated patients included in the analysis. KC conceived the study with AVK and participated in draft of the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
This study reports on data collected from humans. This research was exempt from NCI IRB approval as one of the six exemptions to the regulatory requirements are described in section 46.101(b) of 45 CFR 46, subsection [4]: Research involving the collection or study of existing data, documents, records, pathological specimens, or diagnostic specimens, if these sources are publicly available or if the information is recorded by the investigator in such a manner that subjects cannot be identified, directly or through identifiers linked to the subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (10.1186/s13014-017-0930-9) contains supplementary material, which is available to authorized users.
Contributor Information
Andra Valentina Krauze, Phone: (301) 496-5457, Email: andra.oprea@gmail.com.
Cord Peters, Email: cordjpeters@gmail.com.
Jason Cheng, Email: jason.cheng@nih.gov.
Holly Ning, Email: hning@mail.nih.gov.
Megan Mackey, Email: mmackey@mail.nih.gov.
Lindsay Rowe, Email: lindsay.rowe@nih.gov.
Theresa Cooley-Zgela, Email: Theresa.CooleyZgela@nih.gov.
Dee Dee Smart, Email: smartd@mail.nih.gov.
Kevin Camphausen, Email: camphauk@mail.nih.gov.
References
- 1.Combs SE, Edler L, Rausch R, Welzel T, et al. Generation and validation of a prognostic score to predict outcome after re-irradiation of recurrent glioma. Acta Oncol. 2013;52(1):147–152. doi: 10.3109/0284186X.2012.692882. [DOI] [PubMed] [Google Scholar]
- 2.Verhaak RG, Hoadley KA, Purdom E, et al. Cancer genome atlas research network. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell. 2010;17(1):98–110. doi: 10.1016/j.ccr.2009.12.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wen PY, Macdonald DR, Reardon DA, et al. Updated response assessment criteria for highgrade gliomas: response assessment in neurooncology working group. J Clin Oncol. 2010;28:1963–1972. doi: 10.1200/JCO.2009.26.3541. [DOI] [PubMed] [Google Scholar]
- 4.Rhun EL, Taillibert S, Chamberlain MC. The future of high-grade glioma: where we are and where are we going. Surg Neurol Int. 2015;6(Suppl 1):S9–S44. doi: 10.4103/2152-7806.151331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Park JK, Hodges T, Arko L, et al. Scale to predict survival after surgery for recurrent glioblastoma multiforme. J Clin Oncol Off J Am Soc Clin Oncol. 2010;28:3838–3843. doi: 10.1200/JCO.2010.30.0582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Minniti G, Armosini V, Salvati M, et al. Fractionated stereotactic reirradiation and concurrent temozolomide in patients with recurrent glioblastoma. J Neuro-Oncol. 2011;103(3):683–691. doi: 10.1007/s11060-010-0446-8. [DOI] [PubMed] [Google Scholar]
- 7.Scholtyssek F, Zwiener I, Schlamann A, et al. Reirradiation in progressive high-grade gliomas: outcome, role of concurrent chemotherapy, prognostic factors and validation of a new prognostic score with an independent patient cohort. Radiat Oncol. 2013;8:161. doi: 10.1186/1748-717X-8-161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shapiro LQ, Beal K, Goenka A, et al. Patterns of failure after concurrent bevacizumab and hypofractionated stereotactic radiation therapy for recurrent high-grade glioma. Int J Radiat Oncol Biol Phys. 2013;85(3):636–642. doi: 10.1016/j.ijrobp.2012.05.031. [DOI] [PubMed] [Google Scholar]
- 9.Cuneo KC, Vredenburgh JJ, Sampson JH, et al. Safety and efficacy of stereotactic radiosurgery and adjuvant bevacizumab in patients with recurrent malignant gliomas. Int J Radiat Oncol Biol Phys. 2012;82(5):2018–2024. doi: 10.1016/j.ijrobp.2010.12.074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kessel KA, Hesse J, Straube C, Zimmer C, Schmidt-Graf F, Schlegel J, Meyer B, Combs SE. Validation of an established prognostic score after re-irradiation of recurrent glioma. Acta Oncol. 2017;56(3):422–426. doi: 10.1080/0284186X.2016.1276621. [DOI] [PubMed] [Google Scholar]
- 11.Niyazi M, Flieger M, Ganswindt U, et al. Validation of the prognostic Heidelberg re-irradiation score in an independent mono-institutional patient cohort. Radiat Oncol. 2014;9:128. doi: 10.1186/1748-717X-9-128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fogh SE, Andrews DW, Glass J, et al. Hypofractionated stereotactic radiation therapy: an effective therapy for recurrent high-grade gliomas. J Clin Oncol. 2010;28(18):3048–3053. doi: 10.1200/JCO.2009.25.6941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gutin PH, Iwamoto FM, Beal K, et al. Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int J Radiat Oncol Biol Phys. 2009;75(1):156–163. doi: 10.1016/j.ijrobp.2008.10.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Combs SE, Thilmann C, Edler L, et al. Efficacy of fractionated stereotactic reirradiation in recurrent gliomas: long-term results in 172 patients treated in a single institution. J Clin Oncol. 2005;23(34):8863–8869. doi: 10.1200/JCO.2005.03.4157. [DOI] [PubMed] [Google Scholar]
- 15.Grosu AL, Weber WA, Franz M, et al. Reirradiation of recurrent high-grade gliomas using amino acid PET (SPECT)/CT/MRI image fusion to determine gross tumor volume for stereotactic fractionated radiotherapy. Int J Radiat Oncol Biol Phys. 2005;63(2):511–9. 15. http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_40. Last accessed March 10, 2017 [DOI] [PubMed]
- 16.Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys. 1991;21:109–122. doi: 10.1016/0360-3016(91)90171-Y. [DOI] [PubMed] [Google Scholar]
- 17.Mayo C, Martel MK, Marks LB, et al. Radiation dose-volume effects of optic nerves and chiasm. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S28–S35. doi: 10.1016/j.ijrobp.2009.07.1753. [DOI] [PubMed] [Google Scholar]
- 18.Lawrence YR, Li XA, el Naqa I, et al. Radiation dose-volume effects in the brain. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S20–S27. doi: 10.1016/j.ijrobp.2009.02.091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sheu T, Molkentine J, Transtrum MK, et al. Use of the LQ model with large fraction sizes results in underestimation of isoeffect doses. Radiother Oncol. 2013;109(1):21–25. doi: 10.1016/j.radonc.2013.08.027. [DOI] [PubMed] [Google Scholar]
- 20.Burman C, Kutcher GJ, Emami B, et al. Fitting of normal tissue tolerance data to an analytic function. Int J Radiat Oncol Biol Phys. 1991;21:123–135. doi: 10.1016/0360-3016(91)90172-Z. [DOI] [PubMed] [Google Scholar]
- 21.Lyman JT. Complication probability as assessed from dose-volume histograms. Radiat Res. 1985;8(Suppl):S13–S19. [PubMed] [Google Scholar]
- 22.IMAIOS SAS Anatomy, IMAIOS SAS. www.imaios.com. Accessed 10 Mar 2017.
- 23.2017. www.qarc.org/cog/ACNS0331Atlas.pdf. Accessed Mar 10.
- 24.Pyakuryal A, Myint WK, Gopalakrishnan M, et al. A new formula for normal tissue complication probability (NTCP) as a function of equivalent uniform dose (EUD) Phys Med Biol. 2008;53:23–36. doi: 10.1088/0031-9155/53/1/002. [DOI] [PubMed] [Google Scholar]
- 25.Marks LB, Yorke ED, Jackson A, et al. Use of normal tissue complication probability models in the clinic. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S10–S19. doi: 10.1016/j.ijrobp.2009.07.1754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mayer R, Sminia P. Reirradiation tolerance of the human brain. Int J Radiat Oncol Biol Phys. 2008;70(5):1350–1360. doi: 10.1016/j.ijrobp.2007.08.015. [DOI] [PubMed] [Google Scholar]
- 27.Mayo C, Yorke E, Merchant TE. Radiation associated brainstem injury. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S36–S41. doi: 10.1016/j.ijrobp.2009.08.078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kukolowicz P. Clinical aspects of normal tissue complication probability. Rep Pract Oncol Radiother. 2004;9:261–267. doi: 10.1016/S1507-1367(04)71038-X. [DOI] [Google Scholar]
- 29.Niemierko A. Reporting and analyzing dose distributions: a concept of equivalent uniform dose. Med Phys. 1997;24:103–110. doi: 10.1118/1.598063. [DOI] [PubMed] [Google Scholar]
- 30.Qi XS, Schultz CJ, Li XA. An estimation of radiobiologic parameters from clinical outcomes for radiation treatment planning of brain tumor. Int J Radiat Oncol Biol Phys. 2006;64(5):1570–1580. doi: 10.1016/j.ijrobp.2005.12.022. [DOI] [PubMed] [Google Scholar]
- 31.Webb S, Nahum AE. A model for calculating tumor control probability in radiotherapy including the effects of inhomogeneous distributions of dose and clonogenic cell density. Phys Med Biol. 1993;38:653–666. doi: 10.1088/0031-9155/38/6/001. [DOI] [PubMed] [Google Scholar]
- 32.Stavrev PV, Stavreva NA, Round WH. A study of objective functions for organs with parallel and serial architecture. Australas Phys Eng Sci Med. 1997;20(1):4–10. [PubMed] [Google Scholar]
- 33.Carson KA, Grossman SA, Fisher JD, Shaw EG. Prognostic factors for survival in adult patients with recurrent glioma enrolled onto the new approaches to brain tumor therapy CNS consortium phase I and II clinical trials. J Clin Oncol. 2007;25(18):2601–2606. doi: 10.1200/JCO.2006.08.1661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pietilä S, Lenko HL, Oja S, Koivisto AM, Pietilä T, Mäkipernaa A. Electroretinography and visual evoked potentials in childhood brain tumor survivors. J Child Neurol. 2016;31(8):998–1004. doi: 10.1177/0883073816634863. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
A. maximum Dose and NTCP to OAR based on Maximum Dose values. B. Mean Dose (EUD) and NTCP to OAR based on Mean Dose values. (DOCX 200 kb)
Normal Tissue complication probability (NTCP) (%) vs. A. maximum dose administered to the organ. B. Mean Dose administered to the organ. TheTD65/5 (Maximum Tolerated Dose 50% rate at 5 years at a dose of 65 Gy) curve based on Emami et al. was used to model NTCP using our retrospective data. (DOCX 58 kb)
Comparison with existing scoring systems A. Carson 2007. B. Combs 2013. (DOCX 28 kb)
Data Availability Statement
The datasets supporting the conclusions of this article are included within the article and its additional files.