

Abstract
Open reduction combined with ulnar osteotomy is the most common approach to treating missed Monteggia injuries. The osteotomy is usually performed at the proximal ulna to ensure better healing and fewer complications. The purpose of this study is to present a center of rotation angulation (CORA)-based osteotomy of the ulna for treating Bado type I Monteggia injuries.
We retrospectively reviewed the cases of patients who were treated with open reduction combined with a CORA-based ulnar osteotomy between February 2014 and December 2016. Each patient provided his or her internal control, and paired data of the involved and uninvolved sides were analyzed to evaluate forearm rotation function.
Five patients (3 male, 2 female) with median age 5.7 years (range, 3.4–6.8 years) were operated on by the senior author in our hospital. The median interval between the original injury and the corrective surgery was 3 months (range, 1–4 months). In a median follow-up of 10 months (range, 6–17 months), all patients obtained stable reduction of the radial head and uneventful healing of the ulnar osteotomy. All patients had pain-free elbows with no neurological or vascular complications and no implant breakage. Patients showed excellent outcomes evaluated using the Broberg and Morrey index.
Open reduction with a CORA-based osteotomy of the ulna for the treatment of missed Bado type I Monteggia injury with an obvious ulnar bowing deformity resulted in stable reduction of the radial head and excellent forearm function.
Keywords: monteggia injury, radial head dislocation, ulnar osteotomy
1. Introduction
A Monteggia injury is a fracture of the ulna coupled with radial head dislocation. Bado classified Monteggia injuries into 4 types according to the direction of the radial head dislocation. Type I, described as a fracture of the ulna with anterior dislocation of the radial head, is the most common pattern of injury (60%).[1] It is generally agreed that these injuries should be managed in the acute setting; however, in children, the dislocated radial head might be overlooked if the ulnar fracture is complete with obvious displacement.
More than 90% of missed Monteggia injuries are sequelae of Bado type I injuries.[2] Successfully treating these injuries with minimal complications or functional deficits is a challenge. Many procedures for this difficult problem have been described; however, the outcomes are unpredictable. In a recent review study, 5 different surgical procedures were mentioned, including open reduction of the radial head, reconstruction of the annular ligament, ulnar osteotomy, radial osteotomy and radial head replacement, and open reduction combined with ulnar osteotomy with or without reconstruction of the annular ligament, the latter being the most common[3]. Ulnar osteotomy was described by Hirayama et al[4] as the key procedure for obtaining and maintaining reduction of the radial head after open reduction. An ulnar osteotomy site located at the proximal metaphysis is expected to provide better bone healing and less loss of forearm rotation.[4–9] Only a few authors recommended performing the osteotomy at the deformity site of the ulna.[10–12] However, in some patients, the plastic deformation of the ulna may prevent the reduction, so correcting the ulna deformity may play an important role in radial head reduction. Here, we reviewed our outcomes of open reduction with CORA-based ulnar osteotomy for treating Bado type I Monteggia injuries.
2. Material and methods
The study was approved by the ethics committee of Shanghai Children's Medical Center. After obtaining written informed consent from the parents or guardians, we retrospectively reviewed our patients with missed Bado type I Monteggia injury treated between February 2014 and December 2016.
All patients were clinically and radiographically followed. Patients were included if a bowing ulna was visible on a plain lateral radiograph. Patients with isolated anterior radial head dislocation but without an ulnar plastic deformation were excluded. For all patients, open reduction combined with ulnar osteotomy at the apex of the deformity was performed by a senior author.
Data collected included patient demographics, original injury to surgery interval, and forearm range of motion. The postoperative posterior angulation of the ulna was measured on a lateral-view radiograph. The Broberg and Morrey rate index, which considers motion, strength, stability, and pain, was used to evaluate the postoperative subjective, objective, and elbow function, and the results are interpreted as excellent (≥95), good (80–94), fair (60–79), or poor (<59).[13]
As each patient provided his or her own internal control (i.e., unaffected side), potential confounders, such as age, sex, and health condition could be well controlled. To minimize bias, forearm range of motion was measured by one author using a goniometer, while we compared postoperative range of rotation of the operated forearm to that of the normal side to evaluate the postoperative rotation limitations. The statistical analysis was performed using Statistical Package for the Social Sciences version 17.0 (SPSS Inc., Chicago, IL). The significance of the findings was evaluated with a paired 2-tailed t test to compare all paired variables. Differences were considered significant at a P value < .05.
2.1. Surgical technique
The CORA was identified initially on the lateral-view radiograph and determined by the intersection of the proximal and distal axes of the ulna. The angulation correct axis is along the bisector and indicates that the deformity can be completely correct without translation.
Under general anesthesia, patients were placed in a supine position and 2 skin incisions were used. We used Boyd posterolateral elbow approach to expose the radiocapitellar joint, identified and removed the remnants of the annular ligament and fibrosis that might impede the radial head reduction. Reduction is sometimes possible in this situation; however, our cases were unstable. The ulnar shaft was approached directly after the CORA was defined under fluoroscopy. We performed a transverse dorsal open wedge osteotomy at the apex of the deformity of the ulna. We applied direct pressure to the proximal radius to reduce the radial head. A 5- or 6-hole reconstruction plate was bent to stabilize the osteotomy, and the amount of angulation was based on the reduction stability identified both directly and under fluoroscopy by rotating the forearm from pronation to supination and moving the elbow from full flexion to extension. The plate was initially screwed into only the most proximal and most distal holes. If the radial head was stable, the other 2 screws were affixed. Otherwise, the posterior angulation was adjusted to obtain a stable reduction. No further lengthening was performed at the osteotomy site. We felt an autologous bone graft was unnecessary, as the wedge gap was small. No extra procedures for repairing or reconstructing the annular ligament were performed before the incisions were closed. The arm was immobilized in an above-elbow cast for 6 weeks (Fig. 1).
Figure 1.

(A, B) Preoperative anteroposterior (AP) and lateral radiographs of a 5.8-year-old girl at 4 months after sustaining a Bado type I injury (Case 1) in which obvious ulnar bowing sign and the center of rotation of angulation is visible on the lateral radiograph. (C, D) An ulnar osteotomy was performed at the deformity area of the ulna with slight posterior angulation. (E, F) AP projection of the forearm at 17 months after the surgery showing that the radial head remained reduced and the ulnar remodeling was satisfactory.
3. Results
Five patients (3 male, 2 female), median age at surgery was 5.7 years (range, 3.4–6.8 years), with a median interval between the original injury and the corrective surgery of 3 months (range, 1–4 months) and median posterior angulation of the ulna of 15.8° on the postoperative radiograph were treated. In a median follow-up of 10 months (range, 6–17 months), all patients obtained stable reduction of the radial head with uneventful healing of ulnar osteotomies. All patients had pain-free elbows with no neurological or vascular complications and no broken implants. The median total flexion–extension arc of motion was 143°, almost the same as that of the uninvolved side (P = .374). The average arc of rotation of the forearm measured 157°, with median pronation of 62° and median supination of 95° (Table 1), and a slight but significant difference of pronation (P = .04) was observed. At the last follow-up, all patients showed an excellent outcome based on the Broberg and Morrey rate index. The ulnar osteotomy site was completely remodeled without an obvious posterior bowing at the last follow-up (Fig. 2).
Table 1.
Patients’ demographic and clinical data.
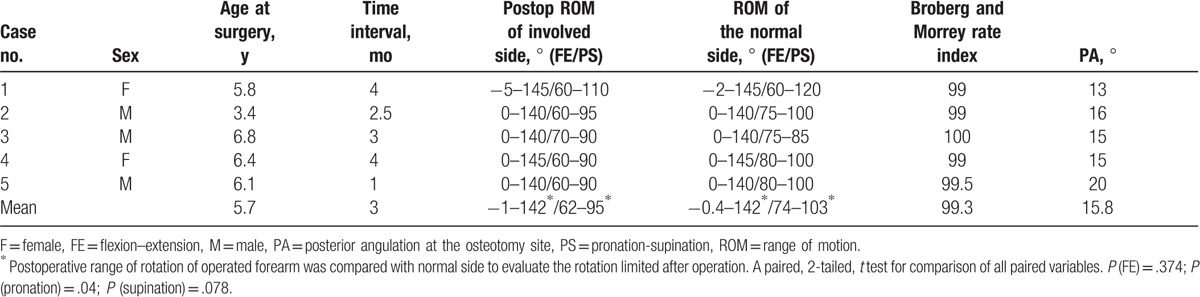
Figure 2.

The patient showed full range of motion at the last follow-up and no scars were obvious.
4. Discussion
Monteggia injury is an uncommon injury that comprises approximately 1% of all pediatric forearm injuries. Closed reduction of the radial head can be successfully performed in most acute cases; however, the dislocated radial head may not be identified at the time of the injury. When the diagnosis is delayed, some pathologic changes will prevent reduction of the radial head.[14] Therefore, the treatment of missed Monteggia injury is difficult and remains controversial, as many reposition procedures of the dislocated radial head show unsatisfactory results. In this study, we present our procedure for treating missed Bado type I Monteggia injury, which feature an anterior bowing deformation of the ulna, in 5 patients with a median follow-up of 10 months, all of whom healed with stable reduction of the radial head and minimal functional limitations.
Although many authors agree that ulnar osteotomy is the key to achieving and maintaining reduction[4,9,15] in treating this injury, the osteotomy site is most commonly performed at the proximal metaphysis of the ulna. Ladermann et al[7] described an ulnar osteotomy performed at the proximal metaphysis or the CORA; however, they advocated performing the osteotomy at the proximal metaphysis for 2 reasons: the CORA might be difficult to identify after remolding of the ulnar fracture; and better healing of the osteotomy occurs at the proximal metaphysis.
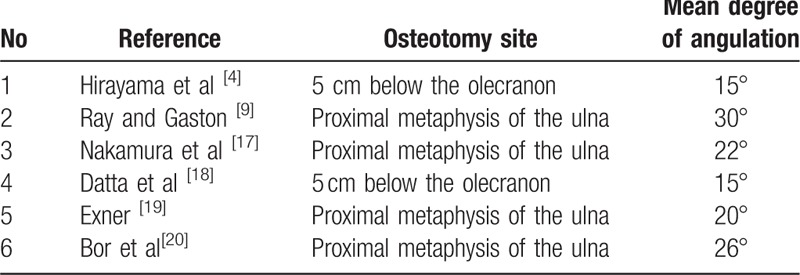
We performed the osteotomy at the CORA of the ulna, as we hypothesized that an anterior bowing ulna is one of the obstacles of radial head reduction. The radius and ulna are parallel when the forearm is in supination; however, in pronation, the radius crosses over the ulna and the apex of the anterior deformity is close to the radius and acts as a fulcrum forcing the radial head anteriorly. The CORA-based osteotomy could not only eliminate the fulcrum in supination but also restore the normal width of the interosseous membrane by creating a slight posterior angulation. This corresponds with the concepts of the osteotomy[16]: if it is not performed at the CORA level, it should be combined with translation. The median posterior angulation in our series was 15.8°, similar to those of studies reporting osteotomy at the proximal ulna.[4,7,9,17–20] (Table 2). As the osteotomy was done at the CORA, no further translation was required. However, there was a mild limitation in pronation compared with the opposite side (P = .04), and no patients had functional deficits. The patients’ Broberg and Morrey rate index of excellent outcome also indicated that the CORA-based osteotomy for Bado type I Monteggia fracture with deformity of the ulna was successful.
Table 2.
Studies reporting proximal ulnar osteotomy with posterior angulation.
Other procedures including annular ligament repair or reconstruction and temporary K-wire fixation of the radio-humeral joint were reported to achieve a stable reduction. However, stiffness of the elbow, intraarticular K-wire breakage, radioulnar synostosis, myositis ossificans ectopic ossification, or radial head osteonecrosis of annular ligament reconstruction have been described in these procedures.[14,21] Moreover, osteoarthritis, recurrence of dislocation or subluxation, and poor function after pin removal have been reported.[22] We did not perform these procedures in our series, as we believed that the posterior angulating ulna with the taut interosseous membrane was sufficient to maintain reduction stability. The interosseous membrane is normally taut in supination and lax in pronation, behaves as an articular unit (middle radioulnar joint), and fulfills the crucial biomechanical functions to restore the normal relationship between the radius and the ulna.[23–25] Posteriorly angulating the osteotomy allows the taut interosseous membrane to pull the radial head back.
Some authors have recommended closed reduction of the radial head after ulnar osteotomy.[17,19] They used the external fixator to reduce the radial head by acute or gradual ulnar lengthening. We did not attempt closed reduction in our patients, as when the diagnosis is delayed, “buttonholing” of the radial head through the capsular or other fibrous tissue, such as the remnant annular ligament, would impede the radial head reduction and make any effort futile.[26,27]
As the tension of the interosseous membrane will decrease even with slight displacement of the ulna and the radiocapitellar joint is very sensitive to ulnar alignment. Subtle changes of the angulation of the ulna can lead to subluxation of the radial head. A rigid fixation is important to achieve a successful outcome; thus, we agree with those authors who used a plate to fix the ulnar osteotomy.[10,15] Some authors have recommended a dual socket joint external fixator to fix the ulnar osteotomy,[8,28] as it can easily correct and adjust the osteotomy in 3 dimensions; however, the external fixator may not be tolerated in young children and socket joint loosening may result in loss of the correction angle. The external fixator is more suitable for ulnar elongation if overgrowth of the radius is present as in cases of long-standing dislocation.
Although open reduction and ulnar osteotomy are not novel procedures for treating missed Monteggia injury, few authors have reported CORA-based osteotomy of the ulna in detail, the radial head can be stably reduced. There are some drawbacks to the present study. First, the injury–surgery interval was short. It is known that a longer period of dislocation of the radial head makes reduction more difficult because of the more severe dysplastic changes around the capitellar–radioulnar joint,[14] and overgrowth of the radial head in particular. In such cases, additional ulnar lengthening is recommended. Second, our patients were <7 years of age, which means that potential bone remodeling and a lower risk of soft-tissue contracture were expected. Third, 2 surgical incisions may result in some cosmetic problems. Finally, the small sample size and short follow-up time may have created bias.
5. Conclusion
Our series of 5 patients showed that open reduction with CORA-based osteotomy of the ulna for the treatment of missed Bado type I Monteggia injury with an obvious ulnar bowing deformity results in stable reduction of the radial head and excellent function, especially for patients with a short injury–treatment interval. As our sample size was small and follow-up was short, further studies including long-term observations are required to validate our findings.
Acknowledgment
The authors thank Shijian Liu for assisting with the statistical analysis in this study.
Footnotes
Abbreviations: CORA = center of rotation angulation, F = female, FE = flexion-extension, M = male, PA = posterior angulation, PS = pronation-supination, ROM = range of motion.
Funding/support: This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
The authors report no proprietary or commercial interest in any product or concept discussed in this article.
The authors have no conflicts of interest to disclose.
References
- [1].Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50:71–86. [PubMed] [Google Scholar]
- [2].Bhaskar A. Current concepts in the management of missed Monteggia fracture-dislocation. Curr Orthop Pract 2013;24:49–52. [Google Scholar]
- [3].Goyal T, Arora SS, Banerjee S, et al. Neglected Monteggia fracture dislocations in children: a systematic review. J Pediatr Orthop Part B 2015;24:191–9. [DOI] [PubMed] [Google Scholar]
- [4].Hirayama T, Takemitsu Y, Yagihara K, et al. Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna. J Bone Joint Surg Br 1987;69:639–42. [DOI] [PubMed] [Google Scholar]
- [5].Rahbek O, Deutch SR, Kold S, et al. Long-term outcome after ulnar osteotomy for missed Monteggia fracture dislocation in children. J Child Orthop 2011;5:449–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Degreef I, De Smet L. Missed radial head dislocations in children associated with ulnar deformation: treatment by open reduction and ulnar osteotomy. J Orthop Trauma 2004;18:375–8. [DOI] [PubMed] [Google Scholar]
- [7].Ladermann A, Ceroni D, Lefevre Y, et al. Surgical treatment of missed Monteggia lesions in children. J Child Orthop 2007;1:237–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Lu X, Kun Wang Y, Zhang J, et al. Management of missed Monteggia fractures with ulnar osteotomy, open reduction, and dual-socket external fixation. J Pediatr Orthop 2013;33:398–402. [DOI] [PubMed] [Google Scholar]
- [9].Ray R, Gaston M. Treatment of late-presenting Monteggia variant with an isolated, simple flexion ulnar osteotomy. J Pediatr Orthop Part B 2014;23:472–6. [DOI] [PubMed] [Google Scholar]
- [10].Wang MN, Chang WN. Chronic posttraumatic anterior dislocation of the radial head in children: thirteen cases treated by open reduction, ulnar osteotomy, and annular ligament reconstruction through a Boyd incision. J Orthop Trauma 2006;20:1–5. [DOI] [PubMed] [Google Scholar]
- [11].Best TN. Management of old unreduced Monteggia fracture dislocations of the elbow in children. J Pediatr Orthop 1994;14:193–9. [DOI] [PubMed] [Google Scholar]
- [12].Devnani AS. Missed Monteggia fracture dislocation in children. Injury 1997;28:131–3. [DOI] [PubMed] [Google Scholar]
- [13].Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am 1986;68:669–74. [PubMed] [Google Scholar]
- [14].Kim HT, Conjares JN, Suh JT, et al. Chronic radial head dislocation in children, Part 1: pathologic changes preventing stable reduction and surgical correction. J Pediatr Orthop 2002;22:583–90. [PubMed] [Google Scholar]
- [15].Eygendaal D, Hillen RJ. Open reduction and corrective ulnar osteotomy for missed radial head dislocations in children. Strategies Trauma Limb Reconstr 2007;2:31–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Paley D. Kelly D. Osteotomy concepts and frontal plane realignment. Principle of Deformity Correction 1 ed.Berlin Heidelberg: Springer-Verlag; 2002. 99–106. [Google Scholar]
- [17].Nakamura K, Hirachi K, Uchiyama S, et al. Long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in children. J Bone Joint Surg Am 2009;91:1394–404. [DOI] [PubMed] [Google Scholar]
- [18].Datta T, Chatterjee N, Pal AK, et al. Evaluation of outcome of corrective ulnar osteotomy with bone grafting and annular ligament reconstruction in neglected monteggia fracture dislocation in children. J Clin Diagn Res 2014;8:LC01–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Exner GU. Missed chronic anterior Monteggia lesion. Closed reduction by gradual lengthening and angulation of the ulna. J Bone Joint Surg Br 2001;83:547–50. [DOI] [PubMed] [Google Scholar]
- [20].Bor N, Rubin G, Rozen N, et al. Chronic anterior monteggia lesions in children: report of 4 cases treated with closed reduction by ulnar osteotomy and external fixation. J Pediatr Orthop 2015;35:7–10. [DOI] [PubMed] [Google Scholar]
- [21].Hurst LC, Dubrow EN. Surgical treatment of symptomatic chronic radial head dislocation: a neglected Monteggia fracture. J Pediatr Orthop 1983;3:227–30. [DOI] [PubMed] [Google Scholar]
- [22].Delpont M, Jouve JL, Sales de Gauzy J, et al. Proximal ulnar osteotomy in the treatment of neglected childhood Monteggia lesion. Orthop Traumatol Surg Res 2014;100:803–7. [DOI] [PubMed] [Google Scholar]
- [23].Soubeyrand M, Wassermann V, Hirsch C, et al. The middle radioulnar joint and triarticular forearm complex. J Hand Surg Eur Vol 2011;36:447–54. [DOI] [PubMed] [Google Scholar]
- [24].Wallace AL, Walsh WR, van Rooijen M, et al. The interosseous membrane in radio-ulnar dissociation. J Bone Joint Surg Br 1997;79:422–7. [DOI] [PubMed] [Google Scholar]
- [25].Inoue G, Shionoya K. Corrective ulnar osteotomy for malunited anterior Monteggia lesions in children. 12 patients followed for 1-12 years. Acta Orthop Scand 1998;69:73–6. [DOI] [PubMed] [Google Scholar]
- [26].Aversano F, Kepler CK, Blanco JS, et al. Rare cause of block to reduction after radial head dislocation in children. J Orthop Trauma 2011;25:e38–41. [DOI] [PubMed] [Google Scholar]
- [27].Letts M, Locht R, Wiens J. Monteggia fracture-dislocations in children. J Bone Joint Surg Br 1985;67:724–7. [DOI] [PubMed] [Google Scholar]
- [28].Hasler CC, Von Laer L, Hell AK. Open reduction, ulnar osteotomy and external fixation for chronic anterior dislocation of the head of the radius. J Bone Joint Surg Br 2005;87:88–94. [PubMed] [Google Scholar]