

Abstract
Background:
Acupuncture may improve the menstrual frequency of women with polycystic ovary syndrome (PCOS). However, more sufficient data are needed to improve the efficacy of acupuncture.
Methods:
A total of 172 participants diagnosed with PCOS would be randomly assigned to either the acupuncture group or sham-acupuncture group, at a ratio of 1:1. Participants in both groups will receive treatment for 12 weeks, 3 times a week. The primary outcome will be the proportion of participants with at least a 50% increase from baseline in the monthly menstrual frequency from baseline after 12 weeks intervention, while secondary outcomes will be the difference in anthropometrics, serum hormone level, ovarian morphology, anxiety and depression, and quality of life from baseline to after 12 weeks intervention and to 12 weeks postintervention follow-up between groups.
Discussion:
The aim of this study is to evaluate the efficacy and safety of acupuncture for improving menstrual frequency and other symptoms of patients with PCOS. The limitation of this trial is that it would be difficult to blind the acupuncturists. In addition, these findings may not be suitable for women with PCOS who are seeking pregnancy.
Keywords: acupuncture, polycystic ovary syndrome, protocol, randomized controlled trial, sham-acupuncture
1. Introduction
Polycystic ovary syndrome (PCOS) is a dysfunction of endocrine system in women of reproductive age.[1] Irregular menstruation (oligomenorrhea or amenorrhea), hyperandrogenism, and infertility are the common clinical manifestation of PCOS.[2] The prevalence of PCOS is 6% to 21%, depending on the diagnostic criteria applied and population studied.[3] Approximately 5.6% women in China have this syndrome, according to an epidemiological investigation.[4] The daily life of patients with PCOS would be affected severely due to intensive mental pressure.[5] Moreover, there is also a huge economic burden brought by this disease. A study is reported that 4.36 billion dollars have been spent for evaluating and providing care to reproductive-aged women with PCOS in the United States.[6]
As for the diagnosis of PCOS, 3 consensuses have been successively proposed by the National Institutes of Health, by both the European Society for Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM), and by the Androgen Excess Society, respectively.[7] The Rotterdam criteria proposed by ESHRE and ASRM have been recommended to be used in China.[8]
Menstrual-related disorders, androgen-related symptoms, and infertility are the common reasons for women with PCOS who visit their doctors. There is no uniform therapeutic regimen of PCOS due to the different goals of treatment. Lifestyle intervention and weight loss should be applied as the first choice for overweight patients.[9] For inducing ovulation, the first-line pharmacological treatment is clomiphene citrate, the second-line pharmacological treatment is the administration of exogenous gonadotropins or laparoscopic ovarian surgery, and the third-line treatment is high-complexity reproduction treatment such as in vitro fertilization or intracytoplasmic sperm injection.[10]
Hormonal contraceptives have been recommended to be used as first-line management for the menstrual abnormalities and hirsutism/acne of PCOS. Combined oral contraceptives (COCs) are a combination of low doses of synthetic estrogens and progestogens, which have been used for patients not seeking pregnancy.[11] Major morbidities, including cardiovascular events related to these combined COCs, have been reported among women of reproductive age, although data remain limited for these results.[12]
Recently, it has been reported that acupuncture may be useful for improving ovulation rate[13–15] and treating oligo/amenorrhea.[16] A systematic review revealed that there was an improvement in the menstrual frequency of PCOS patients after acupuncture treatment.[17] However, menstrual frequency was not used as the primary outcome, and more sufficient data would be needed to prove the efficacy of acupuncture.[18,19] A sham-controlled randomized trial will be performed in this trial to evaluate the efficacy of acupuncture in improving the menstrual frequency of PCOS patients who do not have fertility requirements.
2. Methods
2.1. Study aims
In this study, the efficacy of acupuncture on improving the menstrual frequency in women with PCOS will be evaluated.
2.2. Study design
This study is a prospective, randomized and sham-controlled trial. The flow chart is shown in Fig. 1 and the time point of assessment is shown in Fig. 2. The Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)[20] and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA)[21] guidelines were followed during the development of the protocol of this study.
Figure 1.
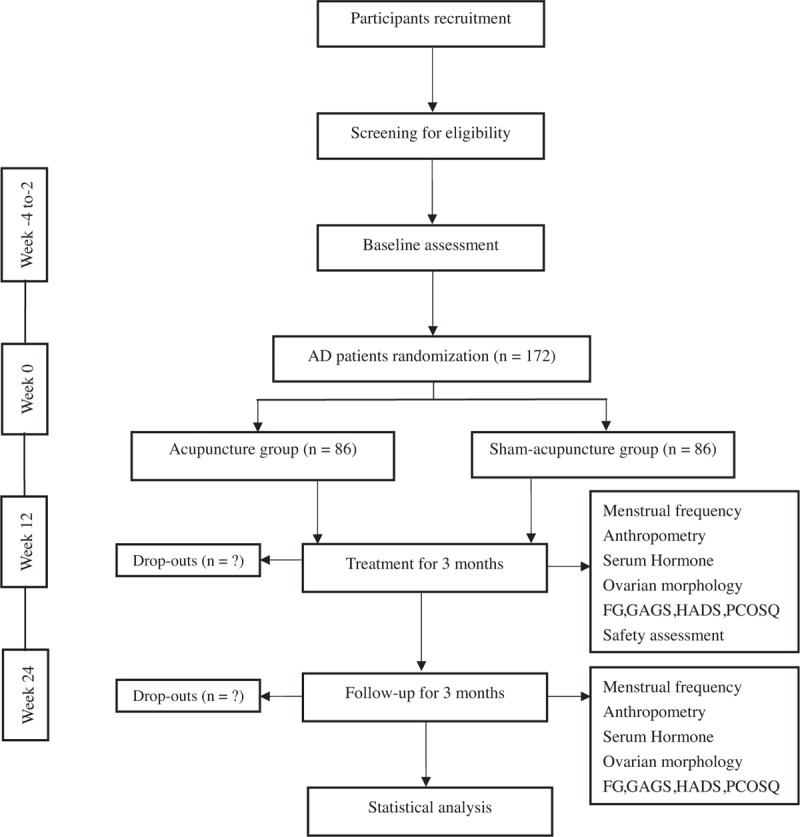
The flow chart of the trial.
Figure 2.
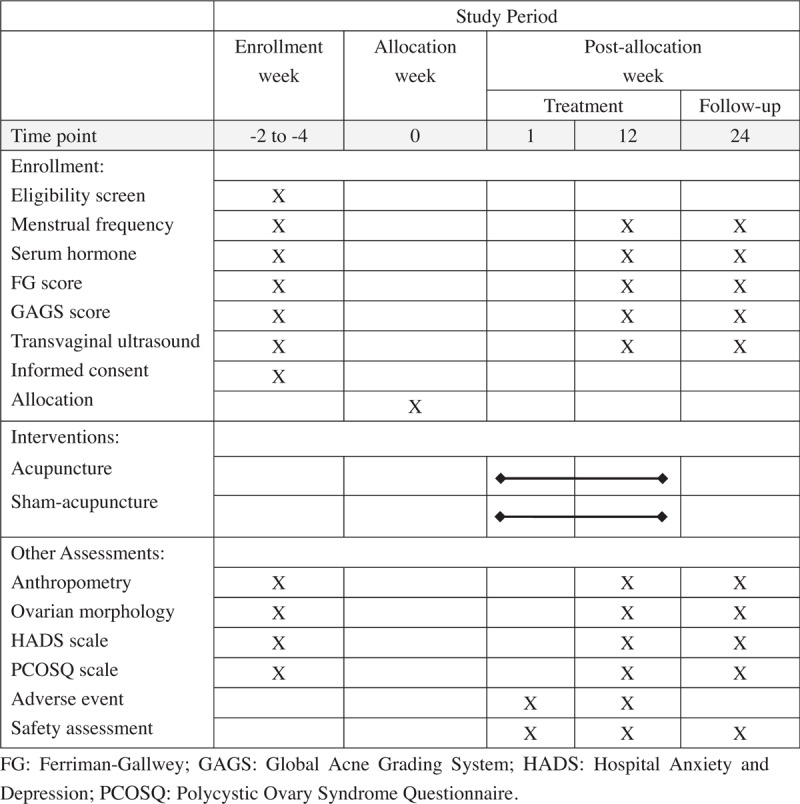
The time point of assessment.
2.3. Study setting and recruitment
This study will be conducted between July 2018 and December 2019. A total of 172 participants will be recruited in Guang’anmen Hospital, China Academy of Chinese Medical Sciences, through posters, hospital webs, and networks. The research assistants will be in charge of recruitment, and a gynecologist will be in charge of the diagnosis of the participants.
2.4. Inclusion criteria
Participants who fulfill the following criteria will be included.
-
1.
Participants meet the Rotterdam diagnostic criteria[2] with oligomenorrhea or amenorrhea. (Oligomenorrhoea is defined as an intermenstrual interval of >35 days or <8 menstrual bleedings in the past year. Amenorrhea is defined as absent menstrual bleeding or no menstrual bleeding in the previous 90 days.)
-
2.Participants who have at least 2 of the following features that meet the Rotterdam diagnostic criteria:
-
a.Clinical or biochemical hyperandrogenism: Biochemical hyperandrogenemia is defined as a total serum testosterone concentration above normal threshold, and/or clinical hyperandrogenism is defined as a Ferriman–Gallwey (FG) score[22] of ≥5[23] or acne defined by the Global Acne Grading System (GAGS)[24] as “mild”/ “moderate”/ “severe”/ “very severe.”
-
b.Polycystic ovary morphology is defined as the presence of ≥12 follicles in each ovary measuring 2 to 9 mm in diameter and/or an ovarian volume >10 mL on transvaginal ultrasound.
-
a.
-
3.
Participants who are between 18 and 40 years old.
-
4.
Participants who joined the research and provided a signed informed consent voluntarily.
2.5. Exclusion criteria
Participants who fulfill any of the following criteria will be excluded.
-
1.
Participants with fertility requirements.
-
2.
Participants with oligomenorrhea or amenorrhea caused by hyperandrogenemia, premature ovarian failure, or hypothalamus or pituitary disorders.
-
3.
Participants with hyperandrogenism caused by congenital adrenal hyperplasia, Cushing syndrome, and androgen-secreting tumors.
-
4.
Participants with endocrine disorders such as thyroid dysfunction, adrenal disorders, hyperprolactinemia, and diabetes mellitus.
-
5.
Participants with severe heart disease, hepatic disease, renal system and hematopoietic system disease, or malnutrition of the whole body.
-
6.
Participants who use hormones or other medications that would affect reproductive function, or received the same protocol of this study in the past 3 months.
2.6. Randomization and blinding
2.6.1. Randomization
A 2-week to 4-week baseline assessment will be needed before randomization. The randomization process will be performed by the Clinical Pharmacological Assessment Center at Guang’anmen Hospital using the Statistics Analysis System (SAS) software. The participants will be divided into 2 groups: acupuncture group and sham-acupuncture group; at a ratio of 1:1. Opaque envelopes with sequence numbers marked outside will be used for sealing the paper-written random numbers and grouping information inside. The acupuncturists will obtain the information of the random numbers and group assignment by opening these envelopes.
2.7. Blinding
Researchers responsible for the recruitment or data collection, participants, statisticians, and other researchers who are not participants in the treatment process will be blinded.
2.8. Intervention
2.8.1. Acupuncture group
Acupuncturists who have an official license and at least 2-year of clinical experience of acupuncture will perform the treatment. Bilateral ST25, EX-CA1, CV4, and SP6 will be selected for treatment. The location of the acupoints will be based on the “Nomenclature and location of acupuncture points”[25] drafted in 2006 by the National Standard of the People's Republic of China (GB/T 12346–2006) and the consensus of experts. After routine sterilization of the local skin, bilateral ST25, EX-CA1, CV4, and SP 6 will be inserted by the needles (0.30 mm in diameter, 40 mm in length) (Hwato Brand, Suzhou Medical Appliance Factory, China) to a depth of 25 to 30 mm to the abdominal muscle layer with the manipulation of lifting, thrusting, and rotating until “de qi” [26] (the sensation of sourness, numbness, and heaviness). Each session will last for 30 minutes, and the manipulation of lifting, thrusting, and rotating evenly 3 times will be used for CV 4 and SP 6 every 10 minutes. If the date of treatment is during the menstrual circle, the treatment will be continued as usual. Participants will be treated 3 times a week for 12 weeks with 36 sessions.
2.9. Sham-acupuncture group
The sham ST25, EX-CA1, CV4, and SP 6, which are 1 cun (25 mm) outward to ST25, EX-CA1, CV4, and SP 6, will be inserted to 2 to 3 mm with needles with a diameter of 0.30 mm and a length of 13 mm. The needles will be inserted without de qi or any manipulation. The treatment sessions will be the same as those in the acupuncture group.
The treatment will be discontinued for pregnant patients. After the treatment, if patients have no menstrual bleeding for 3 months, progesterone (Zhejiang Aisheng Pharmaceutical Co., Ltd., Hangzhou, Zhejiang, China ) will be taken for hormonal withdrawal bleeding. Two 200-mg tablets will be continuously taken every night for 10 days. Patients will stop taking the medicine when menstrual bleeding occurs during these 10 days.
2.10. Outcome measure
2.10.1. Primary outcome measure
The proportion of participants who have at least a 50% increase from baseline in monthly menstrual frequency after 3 months of intervention.
Baseline monthly menstrual frequency was calculated through the number of menstrual bleeds in 3 months before intervention divided by 3. Monthly menstrual frequency from baseline to 3 months was calculated through the number of menstrual bleeds during the 3-month intervention divided by 3.
2.11. Secondary outcome measure
2.11.1. Change in menstrual frequency
The proportion of participants who have at least a 50% increase from baseline in monthly menstrual frequency to 3 months postintervention follow-up, and the change in monthly menstrual frequency from baseline, to after 3 months of intervention, and 3 months postintervention follow-up.
2.11.2. Change in anthropometry
The change in measurements for height, weight, waist and hip circumference, body mass index (BMI), and waist-hip ratio (WHR) at month 3 and 6. BMI is calculated by dividing the weight by the square of the height. WHR is calculated by dividing the circumference of the narrowest point of the waist by the circumference of the widest point of the hip.
2.11.3. Change in serum hormone level
The change in serum luteinizing hormone (LH), serum follicle-stimulating hormone (FSH), LH/FSH ratio, testosterone (T), estrogen (E), prolactin (PRL), progesterone (Prog), dehydroepiandrosterone (DHEA), sex-hormone binding globulin (SHBG), and androstenedione (AND) from baseline at month 3 and 6. Blood samples will be taken at menstrual cycle days 2 to 4 when ovulation or bleeding occurs. Otherwise, this will be performed on the arbitrary day of the cycle.
2.11.4. Change in ovarian morphology
Calculation changes in bilateral ovaries, mean difference in ovary volume, thickness of the endometrium, and the number of follicles <9 mm by ultrasonography from baseline at month 3 and 6.
2.11.5. Change in hirsutism and acne
Change in FG [22] and GAGS[23] scores from baseline measured at month 3 and 6. The FG score assesses the hair growth of nine anatomic sites, and has a maximum score of 36 with a scale of 0 to 4 for each site. GAGS evaluate 6 locations, including the forehead, right cheek, left cheek, nose, chin, and chest or upper back. A local score is rated with a factor (1–3 scale) specific to the acne location, multiplying the grade on the acne of this location (0–4 scale). The global score is the summation of all local scores.
2.11.6. Change in anxiety and depression
The score of the Hospital Anxiety and Depression Scale (HADS)[27] changed from baseline at month 3 and 6. HADS is validated and standardized for measuring the state of anxiety and depression.[28] HADS has 2 subscales with 14 items (7 items each), and a total score of 0 to 21 with 0 to 3 for each item. A score of ≥8 shows the presence of anxiety and/or depression.
2.11.7. Change in quality of life (QOL)
The change in Polycystic Ovary Syndrome Questionnaire (PCOSQ)[5] scores from baseline at month 3 and 6. PCOSQ has 26 questions and includes 5 domains, which are emotions, body hair, weight, infertility, and menstrual problems. A lower score indicates a more impaired QOL.[29]
2.11.8. Blinding assessment
Participants will answer the following questions after 12 weeks of intervention, in order to assess the blinding: “Do you think you have received traditional acupuncture in the past weeks?” The participants can answer “Yes,” “No,” or “Unclear.”
2.11.9. Expectation value of the acupuncture effect assessment
Participants will answer the following questions before the intervention: “Do you think acupuncture will be effective for treating the disease?” “Do you think acupuncture will be effective for improving the related symptoms of PCOS?” The participants can answer “Yes,” “No,” or “Unclear.”
2.11.10. Safety assessment
All adverse reactions will be presented in tables with a description on the categories, severity, rate of incidence, and correlation with the treatment. Adverse reactions related to acupuncture (severe pain, local hematoma, infection and abscess, and retained needle and broken needle during the treatment), including some discomforts after treatment, will be recorded in time in detail. Adverse events irrelevant with the treatment will also be recorded in detail.
2.12. Statistics
2.12.1. Sample size
The calculation of the sample size was based on the primary outcome, which is the proportion of participants with at least a 50% increase from baseline in monthly menstrual frequency during the 12-week intervention.
According to 1 previous study,[16] 38% of participants had increased menstrual frequency after 14 sessions of electro-acupuncture, and the proportion of participants with at least a 50% increase from baseline to 12 weeks was assumed to be 35% in the acupuncture group and 15% in the sham-acupuncture group. Each group sample size of 71 achieves 80% power to detect a difference between group proportions of 20%. A total of 172 participants (86 participants in each group) will be required for the study, with an alpha risk of 5% and a beta risk of 20%, assuming 20% loss to follow-up.
2.12.2. Statistical analysis
Data will be analyzed using SPSS software V.20.0 (IBM SPSS Statistics; IBM Corp, Somers, NY), based on the intention-to-treat (ITT) principle. Missing data will be calculated using the actual observational value instead of the method last observation carried forward. For continuous data, the data will be presented as mean ± standard deviation when normally distributed, or be presented as median (interquartile range) when not normally distributed. Statistical comparisons will be performed by Student t test and Wilcoxon rank sum test for continuous data and by X2-test for categorical data. The difference between groups will be analyzed by X2-test or Wilcoxon rank sum test. A P value <.05 will be considered statistically significant. The phenotypic distribution will be analyzed according to the included participants, and a subgroup analysis will be conducted according to these phenotypes. Moreover, the phenotypes of these participants will be divided into polycystic ovaries combined with oligo/amenorrhea and hyperandrogenism, oligo/amenorrhea and hyperandrogenism combined with polycystic, and oligo/amenorrhea combined with polycystic ovaries.
2.12.3. Data collection, management, and monitoring
The research assistants will be in charge of the randomization process and data collection. All data will be well-preserved safely, and the double input method will be used for data entry. The data of these participants will be reviewed by the quality monitoring board or revealed with the permission of the principal investigator for emergency circumstances. A quality monitor board consists of a gynecologist, a clinician, an acupuncturist, a medical statistician, and an epidemiologist independent from the researchers and the sponsor. The principal investigator will be in charge of the whole monitoring process. Every detail of adverse events during this study should be recorded in the case report forms. The whole process of this study will be under strict supervision.
2.12.4. Ethics approval and consent to participate
This study will be conducted in accordance with the principles of the Declaration of Helsinki, and has been approved by the Ethics Committee of Guang’anmen Hospital (2015EC15). This trial has been registered at clinical trials.gov (NCT02653911). All eligible participants will be required to provide a sign informed consent before being randomly allocated. These participants will be informed about the aim of the study, the eligible criteria of participants, the course of treatment, the potential benefits, and the risks of the study. All participants will have the right to withdraw from the study at any time. The personal data of these participants will only be used for this study.
2.12.5. Protocol amendment and data dissemination
All modifications of this protocol will be submitted to the Ethics Committee of Guang’anmen Hospital. The data results obtained from this study will be coordinated for dissemination in conferences or peer-reviewed publications.
2.12.6. Study organization and funding
This study will be conducted in and funded by Guang’anmen Hospital, China Academy of Chinese Medical Sciences.
3. Discussion
The aim of this study is to evaluate the efficacy and safety of acupuncture for improving menstrual frequency and other symptoms of patients with PCOS. Previous studies have shown that acupuncture can modulate endogenous regulatory systems, including the sympathetic nervous system, endocrine system, and neuroendocrine system.[30] Some studies have also found that acupuncture might be effective for menstrual frequency, improving ovulation rate and serum hormone level.[31–33] Moreover, menstrual irregularity or amenorrhea may increase endometrial proliferation, which is related to potentially premalignant disorders.[34] Therefore, the choice of acupuncture may provide an alternative means for women with PCOS who are not willing to be pregnant, and only want to improve their symptoms. According to a systematic review, no studies have reported the comparison of acupuncture to sham-acupuncture in terms of menstruation frequency at present.[35] In order to reduce the placebo effect of sham-acupuncture, the expectation value of the acupuncture effect will be evaluated before treatment.
Furthermore, assessing the psychological index would be meaningful for the effectiveness evaluation. According to 1 study, women with PCOS had increased anxiety and depression, compared with women without PCOS.[28] A systematic review also reported that PCOS diagnosis is associated with an increased risk of moderate and severe depressive and anxious symptoms.[36] However, very few studies have currently examined the impact of the use of oral contraceptive pills on depressive and anxiety symptoms in women with PCOS.[37] Thus, psychological function should be considered when assessing the effect of treatment.
In addition, PCOS affects the health-related QOL of patients.[38] According to a systematic review, due to the small number of studies, restricted sample size, and the methodological diversity of the questionnaires used, there is a lack of detailed understanding of QOL that patients are facing.[39] Assessing the effectiveness of treatment in terms of QOL should not be ignored. It is reliable and valid to use the Chinese version of PCOSQ for women with PCOS.[5]
The limitation of this trial is that it is difficult to blind the acupuncturists. In order to minimize the potential bias, a strict process of randomization and concealment will be performed. Meanwhile, the participants, outcome assessors, and statisticians will be blinded. In addition, our findings may not be suitable for women with PCOS who are seeking pregnancy.
Acknowledgment
All authors of this manuscript would like to give our sincere thanks to the editors of Medjaden Bioscience Limited who have helped us to proofread the manuscript.
Footnotes
Abbreviations: AND = androstenedione, ASRM = American Society for Reproductive Medicine, BMI = body mass index, COCs = combined oral contraceptives, DHEA = dehydroepiandrosterone, E = estrogen, ESHRE = European Society for Human Reproduction and Embryology, FG = Ferriman–Gallwey, FSH = follicle-stimulating hormone, GAGS = Global Acne Grading System, HADS = Hospital Anxiety and Depression Scale, ITT = intention-to-treat, LH = luteinizing hormone, PCOS = polycystic ovary syndrome, PCOSQ = Polycystic Ovary Syndrome Questionnaire, PRL = prolactin, Prog = progesterone, QOL = quality of life, SAS = Statistics Analysis System, SHBG = sex-hormone binding globulin, SPIRIT = Standard Protocol Items: Recommendations for Interventional Trials, STRICTA = Standards for Reporting Interventions in Clinical Trials of Acupuncture, T = testosterone, WHR = waist-hip ratio.
Authorship: ZJ and LZS conceived the concept and design of the study. ZJ drafted and edited the final paper for submission. LZS reviewed and amended the final paper. YLK, YJN, and WY prepared the related information sheets, consent forms, and case report forms. All authors approved the final manuscript.
Funding/support: This study is funded by Guang’anmen Hospital, China Academy of Chinese Medical Sciences.
This study was approved by Ethics Committee of Guang’anmen Hospital (Reference number: 2015EC15), and all participants will be required to provide a written informed consent. No personal information will be included in the published analysis results.
This study will be conducted in accordance with the principles of the Declaration of Helsinki, and was approved by the Ethics Committee of Guang’anmen Hospital. The data of the results from this study will be planned to disseminate in conferences or peer-reviewed publications.
The authors declare that they have no competing interests for this work.
Trial registration: Clinical Trials.gov (https://clinicaltrials.gov/), Registration number: NCT02653911.
References
- [1].Norman RJ, Dewailly D, Legro RS, et al. Polycystic ovary syndrome. Lancet 2007;370:685–97. [DOI] [PubMed] [Google Scholar]
- [2].The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod 2004;19:41–7. [DOI] [PubMed] [Google Scholar]
- [3].Joham AE, Teede HJ, Ranasinha S, et al. Prevalence of infertility and use of fertility treatment in women with polycystic ovary syndrome: data from a large community-based cohort study. J Womens Health 2015;24:299–307. [DOI] [PubMed] [Google Scholar]
- [4].Li R, Zhang QF, Yang DZ, et al. Prevalence of polycystic ovary syndrome in women in China: a large community based study. Hum Reprod 2013;9:2562–9. [DOI] [PubMed] [Google Scholar]
- [5].Cronin L, Guyatt G, Wong E, et al. Development of a health-related quality-of-life questionnaire for women with polycystic ovary syndrome. J Clin Endocrinol Metab 1998;6:1876–86. [DOI] [PubMed] [Google Scholar]
- [6].Azziz R, Marin C, Hoq L, et al. Health care-related economic burden of the polycystic ovary syndrome during the reproductive life span. J Clin Endocrinol Metab 2005;90:4650–8. [DOI] [PubMed] [Google Scholar]
- [7].Cui LL, Chen ZJ. Diagnosis criteria and guidelines for the diagnosis and treatment of polycystic ovary syndrome (article in Chinese). J Int Reprod Health/Fam Plan 2011;30:405–8. [Google Scholar]
- [8].Yu Q. Consensus on diagnosis and treatment of polycystic ovary syndrome (article in Chinese). Chin J Prac Gynecol Obstetr 2007;23:474. [Google Scholar]
- [9].Rocca ML, Venturella R, Mocciaro R, et al. Polycystic ovary syndrome: chemical pharmacotherapy. Expert Opin Pharmacother 2015;16:1369–93. [DOI] [PubMed] [Google Scholar]
- [10].Melo AS, Ferriani RA, Navarro PA. Treatment of infertility in women with polycystic ovary syndrome: approach to clinical practice. Clinics 2015;70:765–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Yildiz BO. Oral contraceptives in polycystic ovary syndrome: risk-benefit assessment. Semin Reprod Med 2008;26:111–20. [DOI] [PubMed] [Google Scholar]
- [12].World Health Organization. Medical Eligibility Criteria for Contraceptive Use. Third edition. 2005. [2017-11-11]. Available at: http://www.who.int/reproductivehealth/publications/family_planning/MEC-5/en/. [Google Scholar]
- [13].Pastore LM, Williams CD, Jenkins J, et al. True and sham acupuncture produced similar frequency of ovulation and improved LH to FSH ratios in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2011;96:3143–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Johansson J, Redman L, Veldhuis PP, et al. Acupuncture for ovulation induction in polycystic ovary syndrome: a randomized controlled trial. Am J Physiol Endocrinaol Metab 2014;304:934–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Chen D, Chen SR, Shi XL, et al. Clinical study on needle-pricking therapy for treatment of polycystic ovary syndrome (Article in Chinese). Chin Acup Moxib 2007;27:99–102. [PubMed] [Google Scholar]
- [16].Jedel E, Labrie F, Odèn A, et al. Impact of electro-acupuncture and physical exercise on hyperandrogenism and oligo/amenorrhea in women with polycystic ovary syndrome: a randomized controlled trial. Am J Physiol Endocrinol Metab 2011;300:37–45. [DOI] [PubMed] [Google Scholar]
- [17].Wu Y, Robinson N, Hardiman PJ, et al. Acupuncture for treating polycystic ovary syndrome: guidance for future randomized controlled trials. J Zhejiang Univ Sci B 2016;17:169–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Johansson J, Stener-Victorin E. Polycystic ovary syndrome: effect and mechanisms of acupuncture for ovulation induction. Evid Based Complement Alternat Med 2013;2013:762615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Ren LN, Guo LH, Ma WZ, et al. A meta-analysis on acupuncture treatment for polycystic ovary syndrome (Article in Chinese). Zhen Ci Yan Jiu 2014;39:238–46. [PubMed] [Google Scholar]
- [20].Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ 2013;346:e7586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].MacPherson H, Altman DG, Hammerschlag R, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med 2010;3:140–55. [DOI] [PubMed] [Google Scholar]
- [22].Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women. J Clin Endocrinol Metab 1961;21:1440–7. [DOI] [PubMed] [Google Scholar]
- [23].Zhao XM, Ni RM, Li L, et al. Defining hirsutism in Chinese women: a cross-sectional study. Fertil Steril 2011;96:792–6. [DOI] [PubMed] [Google Scholar]
- [24].Doshi A, Zaheer A, Stiller JM. A comparison of current acne grading systems and proposal of a novel system. Int J Dermatol 1997;36:416–8. [DOI] [PubMed] [Google Scholar]
- [25].Standardization Administration of the People's Republic of China. GB/T12346-2006, Nomenclature and Location of Acupuncture Points [S]. 2006. [Google Scholar]
- [26].Zhou K, Fang J, Wang X, et al. Characterization of de qi with electroacupuncture at acupoints with different properties. J Altern Complement Med 2011;17:1007–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;6:361–70. [DOI] [PubMed] [Google Scholar]
- [28].Moran LJ, Deeks AA, Gibson-Helm ME, et al. Psychological parameters in the reproductive phenotypes of polycystic ovary syndrome. Hum Reprod 2012;27:2082–8. [DOI] [PubMed] [Google Scholar]
- [29].Chung JPW, Kwan AHW, Kwok JWK, et al. Health-related quality-of-life questionnaire for women with polycystic ovary syndrome: a Chinese translation and validation study. BJOG 2016;123:1638–45. [DOI] [PubMed] [Google Scholar]
- [30].Stener-Victorin E, Wu XK. Effects and mechanisms of acupuncture in the reproductive system. Auton Neurosci 2010;157:46–51. [DOI] [PubMed] [Google Scholar]
- [31].Lim Chi ED, Wong Wu SF. Current evidence of acupuncture on polycystic ovarian syndrome. Gynecol Endocrinol 2010;26:473–8. [DOI] [PubMed] [Google Scholar]
- [32].Zheng HY, Wang XH, Lai MH, et al. Effectiveness of abdominal acupuncture for patients with obesity-type polycystic ovary syndrome: a randomized controlled trial. J Altern Complement Med 2013;19:740–5. [DOI] [PubMed] [Google Scholar]
- [33].Stener-Victorin E, Jedel E, Janson PO, et al. Low-frequency electroacupuncture and physical exercise decrease high muscle sympathetic nerve activity in polycystic ovary syndrome. Am J Physiol Integr Comp Physiol 2009;297:387–95. [DOI] [PubMed] [Google Scholar]
- [34].Hardiman P, Pillay OS, Atiomo W. Polycystic ovary syndrome and endometrial carcinoma. Lancet 2003;361:1810–2. [DOI] [PubMed] [Google Scholar]
- [35].Jo JY, Lee YJ, Lee H. Acupuncture for polycystic ovarian syndrome: a systematic review and meta-analysis. Medicine 2017;96:e7066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Cooney LG, Lee I, Sammel MD, et al. High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod 2017;32:1075–91. [DOI] [PubMed] [Google Scholar]
- [37].Dokras A. Noncontraceptive use of oral combined hormonal contraceptives in polycystic ovary syndrome—risks versus benefits. Fertil Steril 2016;106:1572–9. [DOI] [PubMed] [Google Scholar]
- [38].Stener-Victorin E, Holm G, Janson PO, et al. Acupuncture and physical exercise for affective symptoms and health-related quality of life in polycystic ovary syndrome: secondary analysis from a randomized controlled trial. BMC Complement Altern Med 2013;13:131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Kaczmarek C, Haller DM, Yaron M. Health-Related quality of life in adolescents and young adults with polycystic ovary syndrome: a systematic review. J Pediatr Adolesc Gynecol 2016;29:551–7. [DOI] [PubMed] [Google Scholar]