

1. Introduction
Crohn's disease (CD) is a chronic inflammatory disorder of the gastrointestinal tract. Patients with this disease have an increased risk for both intestinal and various extra-intestinal malignancies. This risk is mainly attributed to chronic inflammation and drug-induced immunosuppression. Various extra-intestinal malignancies, such as lymphoproliferative disorders and non-melanoma skin cancers occur more frequently in IBD patients compared to the general population, mainly in those using immunosuppression. The association between IBD and renal cell carcinoma (RCC) was reported in a cohort study including 180 patients.1 However, the association with multilocular cystic renal neoplasm (MCRN) of low malignant potential has not been described previously.
We report the observation of a patient with a crohn disease and incidental MCRN of low malignant potential.
2. Case presentation
A 33 year old patient was presented with sub -occlusive syndrome lasting for one month associated to abdominal pain and fever during last 48 hours. Biological tests showed inflammatory syndrome. (Fig. 1). The ileocolonoscopy showed a normal colonic mucosa with congestive and ulcerated ileal mucosa. The biopsies revealed granuloma with acute and chronic inflammation. The diagnosis of penetrant Crohn's disease complicated with deep collection was made and the patient was treated with antibiotic associating cefotaxime and metronidazole. After 15 days of treatment, (Fig. 2). The patient underwent a renal lumpectomy. The gross examination of the specimen revealed a well encapsulated, multiseptate tumor mass of 2.5 cm. Cut section of the tumor showed multiple non-communicating cysts, ranging from 0.2 to 0.6 cm in diameter and filled with serous fluid. No solid nodules were seen. Microscopic sections revealed a multilocular, multicystic tumor mass with cysts separated by fibrocollagenous connective tissue lined by a mixture of cells including flattened to cuboidal and clear cells. The clear cells had small hyperchromatic nuclei with Fuhrman's nuclear grading 1. Adjacent renal parenchyma was normal (Fig. 3). Adjuvant therapy is not indicated for this type of renal tumor. For crohn's disease, since the ileal involvement is localized we opted for surgical treatment in order to avoid the use of immunomodulators. An ileocecal resection was planned.
Fig. 1.

Abdominal CT scan revealed an inflammatory thickening of the last ileal loop with, multiple fistulas and a collection of 3 cm. Moreover, at the mediorenal part of the right kidney, there was a well-defined and hypodense lesion measuring 2, 5* 3 cm.
Fig. 2.
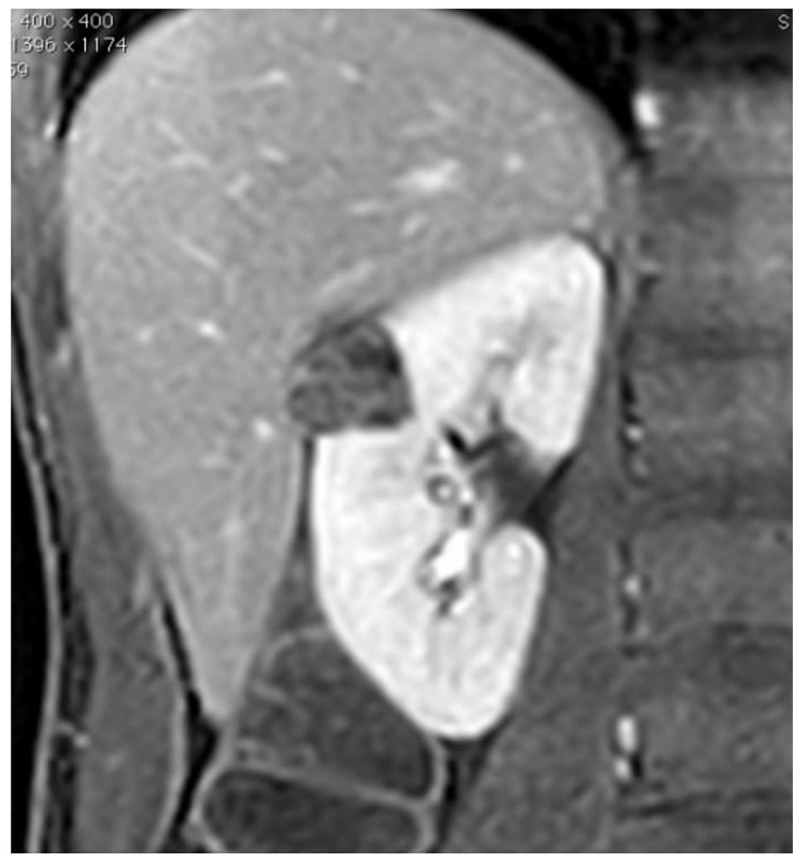
The entero-MRI revealed inflammatory ileal involvement of 8 cm with multiple fistula tracts without collection. There was also, a multicystic medio-renal mass with evident internal septations classified Bosniak 3.
Fig. 3.

Microscopic sections revealed a multilocular, multicystic tumor mass with cysts separated by fibrocollagenous connective tissue lined by a mixture of cells including flattened to cuboidal and clear cells. The clear cells had small hyperchromatic nuclei with Fuhrman's nuclear grading 1. Adjacent renal parenchyma was normal.
3. Discussion
Cystic RCCs account for 4%–15% of all RCC cases although the incidence of MCRN of low malignant potential, a distinct and rare subtype of cystic RCC, is as yet unknown. MCRN of low malignant potential has usually been reported in published studies as a series of several cases. The largest series including 76 cases was recently published.2
MCRN of low malignant potential is a distinct subtype of clear cell RCC and defined as a tumor composed of numerous cysts, the septa between cysts contain groups of clear cells indistinguishable from grade 1 clear cell carcinoma. Multiple reports of >200 patients with follow-up periods of >5 years concluded that no recurrence or metastasis developed in patients with this tumor. Based on this excellent outcome, this tumor has been designated by a new term of multilocular cystic clear cell renal cell neoplasm of low malignant potential, at the 2016 WHO classification of kidney tumors instead of multilocular cystic renal cell carcinoma.3
MCRN of low malignant potential mainly affects young adult and occurred slightly more often in men than in women. This type of tumor is often asymptomatic and is discovered incidentally on radiological examinations. Only a small portion of patients presented with flank pain, abdominal pain, hematuria, or hypertension, and none had the classic triad of RCC (palpable mass, flank pain, and hematuria). Enhanced CT and MRI are helpful in evaluating cystic renal masses using the Bosniak cyst classification system.4
To date, no reports have shown metastases, vascular invasion, or sarcomatoid changes with this disease. Patients with MCRN of low malignant potential have a better prognosis than those with other RCCs probably because of the fewer malignant cells in the tumor and the low nuclear grade of the tumor cells.2
Association with Crohn's disease has not been reported previously. However, the association of RCC and IBD has been described in a series including 180 IBD patients with incident RCC. In this study, patients with a more complex phenotype including Montreal E3 UC, penetrating CD and/or IBD related surgery were at increased risk for RCC development. Male gender and older age at IBD diagnosis were identified as independent risk factors. Use of 5-ASA protected against RCC development. Also, IBD patients had a statistically significant better overall survival compared to the general population independent of immunosuppressive or anti-TNFα therapy.1
IBD patients with a previous malignancy should be managed jointly with the oncologist, taking into account the natural history of the cancer, including location, histological type, prognosis, time from diagnosis and IBD severity. For these patients, available data are currently very limited and physicians are reluctant to give conventional IS to patients with past malignancies because, these agents could reactivate dormant micrometastasis. Also, national guidelines do not recommend anti-TNF use in these patients. In general, within 2 years after completing cancer treatment, 5-aminosalicylates, corticosteroids, antibiotics, nutritional therapy and surgery should form the foundation of IBD treatment. In patients with refractory IBD, administration of conventional IS or anti-TNF should be decided on a case-by-case.5
4. Conclusion
Multilocular cystic renal cell neoplasm of low malignant potential is a rare type of RCC with excellent prognosis. The association of this tumor and Crohn's disease has not been described previously. Although that the tumor was completely removed, the surgical treatment of crohn's disease, if possible, remains the preferred option to avoid the use of immunomodulators especially the first two years after the treatment of cancer.
References
- 1.Derikx Lauranne A.A.P., Nissen Loes H.C., Drenth Joost P.H., van Herpen Carla M., Kievit Wietske, Verhoeven Rob H.A. Better survival of renal cell carcinoma in patients with inflammatory bowel disease. Oncotarget. 2015 Nov 9;6(35) doi: 10.18632/oncotarget.5186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li T., Chen J., Jiang Y. Multilocular cystic renal cell neoplasm of low malignant potential: a series of 76 cases. Clin Genitourin Cancer. 2016 Dec;14(6):e553-e557 doi: 10.1016/j.clgc.2016.03.017. [DOI] [PubMed] [Google Scholar]
- 3.Moch H., Humphrey P.A., Ulbright T.M., Reuter V.E. IARC; Lyon: 2016. WHO Classification of Tumors of the Urinary System and Male Genitale Organs; pp. 11–76. [Google Scholar]
- 4.You D., Shim M., Jeong I.G. Multilocular cystic renal cell carcinoma:clinicopathological features and preoperative prediction using multiphase computed tomography: multilocular cystic renal cell carcinoma. BJU Int. 2011 Nov;108(9):1444–1449. doi: 10.1111/j.1464-410X.2011.10247.x. [DOI] [PubMed] [Google Scholar]
- 5.Laharie D. Previous cancer and/or lymphoma in patients with refractory IBD - pro: Anti-TNF or immunosuppressive treatment. Dig Dis. 2014;32(s1):116–121. doi: 10.1159/000367861. [DOI] [PubMed] [Google Scholar]