

Abstract
Foreign body in the urethra is a relatively rare occurrence. A variety of foreign bodies, majority of which were mostly self-inflicted for psychiatric disorder, senility, intoxication, and autoerotic stimulation, have been reported in the literature. We report a case of self-inserted foreign body (olive seed) in the urethra.
Keywords: Foreign body, Bladder, Urethra: self-infliction, Obstruction
1. Introduction
Foreign body (FB) insertion in the lower urinary tract is uncommon, but some cases had been reported.1, 2, 3 Objects have included fishhooks, metal rods, bones, screws, pellets, safety pins, a plastic cup, straws, a marble, cottontipped swab, needles, pencils, ball point pens, pen lids, garden wire, copper wire, speaker wire, Allen keys, wire such as objects (telephone cables, rubber tubes, feeding tubes, straws, string), toothbrushes, household batteries, light bulbs, marbles, cotton tip swabs, plastic cups, thermometers, plants and vegetables (carrot, cucumber, beans, hay, bamboo sticks, grass leaves), parts of animals (leeches, squirrel tail, snakes, bones), toys, pieces of latex gloves, blue tack, intrauterine contraceptive devices, tampons, pessaries, powders (cocaine), and fluids (glue, hot wax).1, 2, 3
Most cases are associated with psychiatric disorders, senility, intoxication or autoerotic stimulation. Patients often present with dysuria, frequency, haematuria, urinary retention, penile pain and/or swelling. The most common symptom is frequency with dysuria, but sometimes gross haematuria and urinary retention can also be seen.1, 2 Diagnosis is done by history and clinical examination in generally. However, few radiological examinations and cystoscopy are required for diagnosis, especially for treatment planning.4
Here, we present a case of 37-years old men, he had a psychiatric disorder and self-inserted a foreign body (olive seed) into the urethra.
2. Case presentation
A 37-year-old unmarried male patient with urethral catheter was referred to our hospital to undergo the removal of a foreign body from his bladder. The patient underwent urethrocystoscopy and urethral catheterization in another hospital one week ago, because he had inserted a self-made foreign body into the urethra, which caused complete urethral retention. In the urethrocystoscopy note, it was reported that there was a foreign body (bead?) in the bulbar urethra, which was pushed into the bladder by the cystoscope, followed by catheterization with 18 F urethral catheter. On questioning, no clear information was obtained from the patient because he had a psychiatric disorder (schizophreni). He said that 'I do not remember how I did it but it was a bead.' But there was no radiopaque object on abdominal/pelvic X-ray. On ultrasonography, there was a foreign body in the bladder lumen and it was 15 × 5 mm of size. Endoscopic treatment planned for the patient. The urethral catheter was removed and cystoscope inserted from the urethral meatus under the optical vision guide. There were mucosal injuries/tears in the urethra. Foreign body was seen in the bulbar urethra (probably it has migrated to the urethra from the bladder when the urethral catheter was removed) (Fig. 1). Foreign body was caught with flexible forceps and removed successfully (Fig. 2). The removed foreign body was an olive seed size of 15 × 5 mm (Fig. 3). The patient was discharged the same day by oral antibiotic therapy for 1 week. After 1 week, the patient had no any urinary complaints and his urination was normal. Psychiatric evaluation was recommended.
Fig. 1.
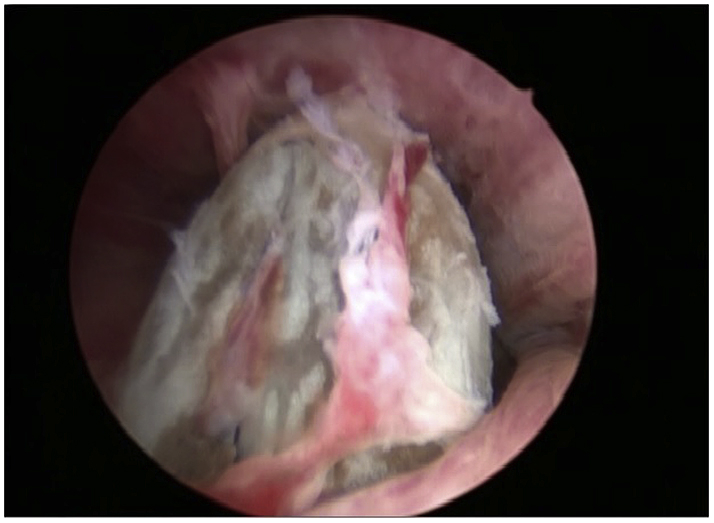
Foreign body in the urethra.
Fig. 2.
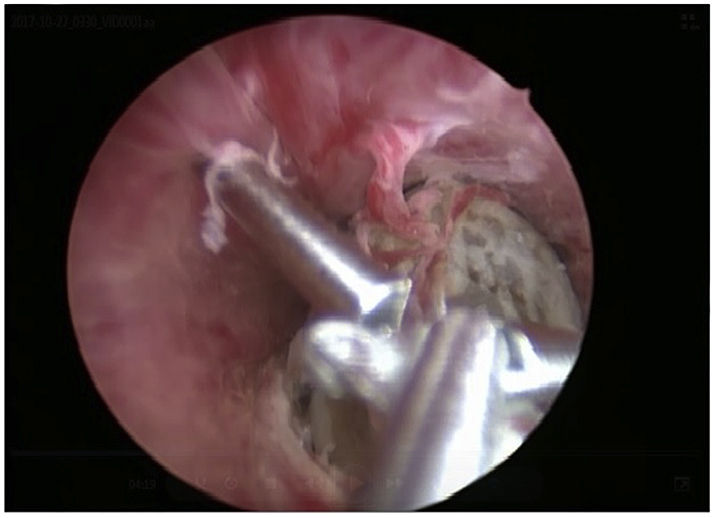
Catching of the foreign body with flexibles forceps.
Fig. 3.
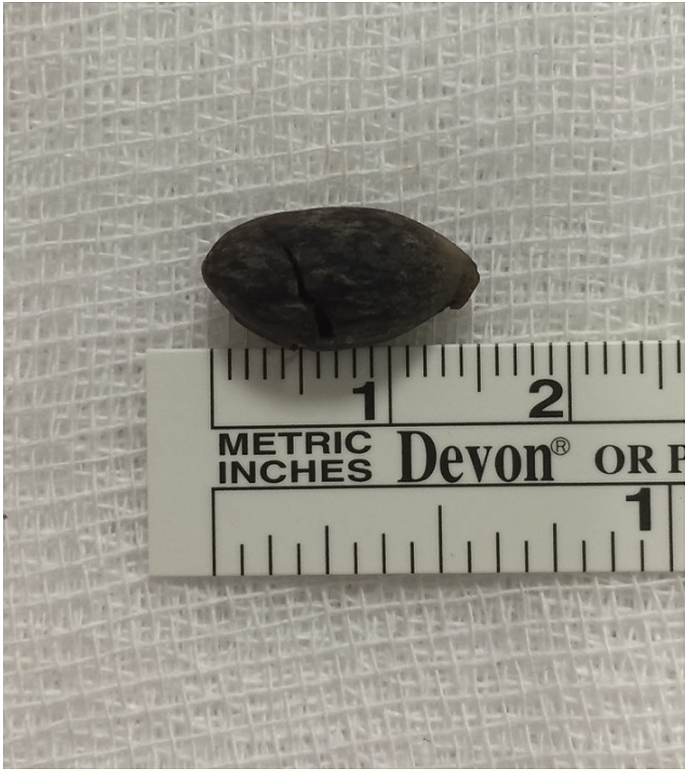
Shape and size of the foreign body removed from the urethra.
3. Discussion
FB in the lower urinary tract can cause some complications when the misplaced object migrates into the proximal urethra or bladder and is not retrievable.1, 2 FB usually be successfully treated endoscopically. But sometimes open surgical treatment may be needed if endoscopic treatment is not possible.1, 3
FB located distal to the urogenital diaphragm can often be successfully extracted by endoscopic methods with the aid of forceps, snares, and baskets, and as such have become the standard of care. But rarely, more invasive FB extraction procedures are required – external urethrotomy (for pendulous urethral foreign bodies), suprapubic cystotomy (for posterior urethral foreign bodies), or meatotomy. Complications following these procedures are rare but can include infection, fistula, urethral stricture, diverticulum, and incontinence.1, 2
Aliabadi et al.3 reported their experience with self-inflicted FB involving the lower urinary tract in 15 patients over a 42-year period. Endoscopic retrieval was successful in six patients with foreign bodies in the anterior urethra; five of the remaining nine patients, with foreign bodies in the posterior urethra and bladder, required open surgery. In the present series, perineal urethrotomy was necessary in only one patient because of difficulties with safe removal of several open safety pins. According to them, these differences in treatment approach can be explained by the variation in the type and location of the objects.
Rahman el al.1 reported that 17 men (aged 17–48 years) were treated for self-inflicted FB insertion. Endoscopic retrieval was successful in 16 of the 17 patients, although ingenuity was required with grasping instruments, which included forceps, snares, stone retrieval baskets, and modified versions of these devices. In one case this was unsuccessful and a perineal urethrotomy was required for several open safety pins in the distal bulb.
Some reports support the notion that the motive of self-insertion of a FB into the urethra is usually autoerotic stimulation.2 Co-morbidities reported in patients presenting with foreign body insertion include exotic impulses, most commonly sexual in nature, a disturbed schizoid personality and borderline personality disorder.5
In a series of 10 self-inflicted urethral FB cases reported by Mahadeyappa et al.,2 one patient had maniac depressive psychiatric disorder, one patient had mental retardation, one patient had impulsive behavior and autoerotic stimulation was the cause recorded in two patients. Lack of partner or spouse and misconception about masturbation was noted as a cause in three patients. Because of these findings, they proposed psychiatric evaluation for all patients, although the controversial. This may be beneficial not only for the diagnosis and treatment of any underlying mental disorders, but also for the prevention of other episodes.
Psychiatric evaluation for all patients is controversial,5 as some will be psychologically normal. However, an initial evaluation in these cases is necessary to identify and treat those with an underlying mental disorder. Furthermore, because this population is often transient, inpatient psychiatric consultation may keep the patient from being lost to follow-up.1
Conclusily, self-inflicted FB in the urethra can be often successfully treated endoscopically. But sometimes open surgical treatment may also be necessary. In addition, psychiatric evaluation should be recommended in these patients and appropriate medical therapy should be performed when indicated.
Conflicts of interest
There is no conflict of interest.
Footnotes
Supplementary data related to this article can be found at https://doi.org/10.1016/j.eucr.2017.11.023.
Contributor Information
Zeki Bayraktar, Email: zbayraktar@medipol.edu.tr.
Selami Albayrak, Email: salbayrak@medipol.edu.tr.
Appendix A. Supplementary data
The following is the supplementary data related to this article:
References
- 1.Rahman N.U., Elliott S.P., McAninch J.W. Self-inflicted male urethral foreign body insertion: endoscopic management and complications. BJU Int. 2004 Nov;94(7):1051–1053. doi: 10.1111/j.1464-410X.2004.05103.x. [DOI] [PubMed] [Google Scholar]
- 2.Mahadevappa N., Kochhar G., Vilvapathy K.S., Dharwadkar S., Kumar S. Self-inflicted foreign bodies in lower genitourinary tract in males: our experience and review of literature. Urol Ann. 2016 Jul-Sep;8(3):338–342. doi: 10.4103/0974-7796.184904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Aliabadi H., Cass A.S., Gleich P., Johnson C.F. Self-inflicted foreign bodies involving the lower urinary tract and male genitalia. Urology. 1985 Jul;26(1):12–16. doi: 10.1016/0090-4295(85)90245-6. [DOI] [PubMed] [Google Scholar]
- 4.Barzilai M., Cohen I., Stein A. Sonographic detection of a foreign body in the urethra and urinary bladder. Urol Int. 2000;64:178–180. doi: 10.1159/000030524. [DOI] [PubMed] [Google Scholar]
- 5.Kenney R.D. Adolescent males who insert genitourinary foreign bodies: is psychiatric referral required. Urology. 1988;32:127–129. doi: 10.1016/0090-4295(88)90313-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.