

Abstract
Purpose
Childhood cancer disrupts children’s daily life experiences. Eliciting children’s perspectives regarding their life experiences during cancer treatment can be challenging. The purpose of this study was to characterize elementary school-age children’s “good days” and “sick days” through their drawings.
Methods
This study used draw-and-tell interviews, a developmentally sensitive arts-based technique that supports children’s recall and communication of information, facilitating a deeper understanding of children’s personal interpretation and meaning of a given phenomenon of interest. Children were asked to draw pictures representing both a “good day” and a “sick day.” Following completion of each drawing, research team members used a semi-structured interview guide to elicit children’s explanations of their pictures. Content analysis techniques were used to descriptively characterize children’s drawings followed by thematic analysis to identify commonalities.
Results
Participants were 27 children 6.33 – 12.83 years of age (mean 9.16 years; SD=1.9) receiving treatment for cancer. “Good day” and “sick day” pictures were similar with regards to the presence of the child, the inclusion of other individuals, and the type of art medium used. Children’s pictures characterized “good days” as being happy, outside in sunny weather, and engaged in activities. In contrast, “sick days” were characterized as feeling sad, lying down or reclining, and experiencing illness-related symptoms.
Conclusions
Children’s drawings illustrate their capacity to provide rich personal data related to their “good days” and “sick days.” Incorporating arts-based strategies in the clinical setting may provide a child-centric strategy to understand the child’s perspective and direct interventions.
Keywords: childhood cancer, symptoms, arts-based techniques, development, quality of life, qualitative research
Background/Introduction
More than 10,000 children under the age of 14 will be diagnosed with cancer each year in the United States, and more than 80% of these children are anticipated to become long term survivors of their disease [1]. Advances in efforts to support and enhance children’s quality of life, regardless of the treatment outcome, however, have not kept pace with advances in curative therapy.
Childhood cancer disrupts the daily life experiences of the elementary school-age child (6–12 years of age), who is developing a growing sense of industry and achievement. Treatment occurs over months to years and requires frequent visits, often to a regional pediatric specialty center, for their treatment and related procedures. Children’s treatment plans often results in missed days of school [2] which reduces their opportunities to achieve key social and emotional milestones, including a growing emphasis on peer relationships. Frequent absences also limit children’s ability to maintain academic progress. Additionally, children experience multiple physical and psychosocial symptoms as a result of their disease and its treatment [3–7]. Collectively, these experiences can hinder both physiologic and psychologic aspects of children’s growth and development with potential adverse consequences on their quality of life.
Eliciting children’s perspectives regarding their life experiences during cancer treatment can be challenging. Because children’s verbal and cognitive abilities are developing, they may express their experiences in feeling states that are meaningful to them, but may not be understood by adults [8–9]. Although child-specific measures designed to address aspects of the child’s experience, including symptoms, have been developed, their scope is often limited to a single symptom or a short list of symptoms and may not fully capture aspects of children’s experiences that are of priority to them [2].
Qualitative interviews involving 39 children and adolescents with cancer, as well as their parents, related that “life is never the same” following a childhood cancer diagnosis. Losses, both shared and unique, a sense of moving forward, and the realization that the cancer experience is never over characterized the experience [10]. Thirteen children receiving treatment for acute lymphoblastic leukemia (ALL) described symptoms, limitations in usual activities, altered relationships, and treatment side effects as adversely affecting their quality of life [11].
Hinds and colleagues [12] identified six domains of quality of life among 46 children and adolescents receiving treatment for cancer: 1) symptoms, 2) usual activities, 3) social/family interactions, 4) health status, 5) mood, and 6) the meaning of being ill based on their responses to the questions, “What makes a good day for you?” and “How has being sick been for you?” In a follow up longitudinal study of 150 children and adolescents receiving treatment for ALL, “good days” were characterized by engaging in usual activities, being with friends or family, not being sick or at the hospital, able to eat, being in a good mood, and being at home. “Being sick” was characterized as both “not so bad” and the experience being “hard.” Children and adolescents also related symptoms of being sick, changes in their lives, missing friends and family, and not being able to do usual activities with the experience of “being sick.” Relative to adolescents, elementary school-age children more frequently reported “being able to do usual things,” and “being at home,” “receiving benefits” (includes not having to do homework or getting attention) and “not sure” as characterizing good days. Younger children also more frequently reported “receiving benefits” as part of the experience of being sick [13].
To date, the use of arts-based approaches to elicit perspectives of the illness experience from children with cancer is limited. The draw-and-tell interview is an arts-based technique that gives children the opportunity to draw first and then relate their narratives [14]. This developmentally sensitive technique supports children’s recall and communication of information using their internal, sensory cues, allowing for a deeper understanding of the child’s interpretation and meaning that can not be elicited from interviews and survey instruments alone [14–17]. Allowing children to draw first and then talk supports the child in relating a greater amount of information compared with techniques that rely on verbal responses alone [15]. Draw-and-tell interviews also emphasize what the child has to say about the drawing which allows the researcher to gain a more child-centric perspective [18]. In the healthcare setting, arts-based techniques have been used successfully to relate symptoms in children with chronic conditions, including sickle cell disease and asthma [17–22]. Children’s drawings have also demonstrated the capacity to communicate change in symptoms over time in children with headaches [20].
The purpose of this study was to characterize elementary school-age children’s “good days” and “sick days” using draw-and-tell interviews. This study extends previous research regarding children’s perceptions of their illness experience by using an approach that supports children in retrieving and relating information about their experiences, that can facilitate a more child-centric report [15]. Using draw-and-tell interviews provided an opportunity to gain insights into the experiences of a discrete developmental age group who are often included in study samples with adolescents. The study was part of a larger effort to understand children’s preferred ways to describe their symptom experiences for use in the development of a game-based symptom assessment application (app) for school-age children.
Methods
Design
This exploratory, descriptive study was guided by the contextual inquiry phase of the cooperative inquiry process. Cooperative inquiry engages end users in the co-design of technology. The contextual inquiry phase is based in field research and engages the researcher in observing and analyzing participants’ responses and patterns of activity [23].
Setting and Sample
The study setting was the Cancer Transplant Center (CTC) within a tertiary free-standing children’s hospital in the Intermountain West of the United States. The CTC includes a 32-bed inpatient unit and an ambulatory clinic that serves approximately 40 patients each day.
Inclusion criteria were children 6 to 12 years of age who were receiving treatment for cancer. Because of the exploratory emphasis of this study, participants were heterogeneous with regards to disease type. Children were required to speak English and be cognitively and physically able to complete study tasks. Parents and child participants also were required to be able and willing to provide permission and assent for the child’s participation.
Procedure
Recruitment and enrollment
Institutional review board (IRB) approval was granted for this study. Eligible participants were initially approached by an oncology team member to introduce the study and elicit interest in participation. Families expressing an interest were subsequently approached by the principal investigator to explain the study. Written parental permission was obtained for all participants. Participants 7 to 12 years of age provided written assent. Participants 6 years of age provided verbal assent.
Draw-and-tell interviews
Children participated in draw-and-tell interviews regarding their experiences of “good days” and “sick days.” Interviews occurred during the course of a scheduled ambulatory clinic visit or inpatient admission. Children received a packet of developmentally appropriate art supplies including a sketch tablet, crayons, colored pencils, markers, pencils, and stickers which they were allowed to keep at the conclusion of the interview.
Participants were initially asked to draw a picture of themselves to describe how their bodies felt when they were receiving their chemotherapy. Based on children’s responses and questions for clarification, the procedure was modified after the second participant to include two drawings. The second participant, a 7-year-old boy, indicated that he felt “normal” when getting his chemotherapy. He went on to relate that what really made him feel sick was taking his “sulfa/trim” (sulfamethoxazole/trimethoprim) and that he had a “sulfa/trim face.” He further detailed his personalized strategy for taking this medication and feeling “like I’m gonna puke” in a second drawing. Children were subsequently first asked to draw a picture of a “good day” and then a picture representing “sick day.” Following completion of each drawing, research team members used a semi-structured interview guide to elicit children’s explanations of their pictures. As part of the interview process, children were asked to elaborate on activities or objects depicted in their drawings. The semi-structured interview approach allowed children the freedom to express their individual experiences from their own perspectives with only occasional guidance and refocusing as needed. Research team members also recorded detailed field notes during the interviews. Drawings were retained by the research team at the conclusion of the interviews.
Data Management and Analysis
A modified content analysis approach was used to analyze the drawings. Content analysis procedures proceed from specific to general and provide a systematic approach for describing phenomena of interest including written, verbal, or visual responses [24–25].
Research team members developed a coding schema to characterize drawings with regards to the characteristics of the child and any other individual(s) present, emotions expressed, location, weather, depiction of activities, presence of personal objects, aspects of the illness experience, as well as the art medium and colors featured within pictures. All pictures, interview responses, and field notes were reviewed and coded independently by at least three research team members. The team then met together to review responses and to reach consensus. Coded responses were recorded in Excel spreadsheets and then transferred to SPSS to support quantitative descriptive analyses. Chi-square analyses explored differences in frequencies of descriptive characteristics based on “good days” and “sick days.”
A thematic analysis approach identified common themes and subthemes represented among children’s drawings and their accompanying narratives. Three team members met together to complete thematic analyses and reach consensus.
Results
Participants
Participants were 27 children 6.33 – 12.83 years of age (mean 9.16 years; SD=1.9) receiving treatment for cancer; 52% (n=14) were male. Participants were a median of 9 months since their initial cancer diagnosis with a range of 1 to 93 months; 55% were within 12 months of diagnosis. The majority (n=15) were being treated for acute lymphoblastic leukemia which is the most common type of cancer in this age group. Other demographic characteristics are summarized in Table 1.
Table 1.
Participant Characteristics
| Gender | N | % | |
|---|---|---|---|
| Males | 14 | 52% | |
| Females | 13 | 48% | |
|
| |||
| Age Group | |||
|
| |||
| Younger children (6–8 years) | 14 | 52% | |
| Older children (9–12 years) | 13 | 48% | |
|
| |||
| Race/Ethnicity | |||
|
| |||
| White/non-Hispanic | 25 | 93% | |
| American Indian/Alaska Native | 1 | 4% | |
| Black/African American | 1 | 4% | |
|
| |||
| Diagnosis | |||
|
| |||
| Acute lymphoblastic leukemia | 15 | 57% | |
| Other acute leukemia | 1 | 4% | |
| Hodgkin lymphoma | 1 | 4% | |
| Non-Hodgkin lymphoma | 1 | 4% | |
| Brain tumor | 2 | 7% | |
| Sarcoma | 5 | 19% | |
| Other solid tumor | 2 | 7% | |
|
| |||
| Disease stage | |||
|
| |||
| Primary disease | 26 | 96% | |
| Recurrent disease | 1 | 4% | |
|
| |||
| Median | Mean (SD) | Range | |
|
| |||
| Months since initial diagnosis | 9 | 15.5 (17.7) | 1–93 |
Thirty children and parents were approached for an accrual rate of 90%. Children’s reasons for non-participation included, “really don’t want to,” and “don’t feel like it.” All study-related procedures were completed during the course of a single ambulatory clinic or during an afternoon of an inpatient admission.
Descriptive Characteristics of Pictures
Twenty-six “good day” pictures, and 27 “sick day” pictures were included in the analyses. Descriptive characteristics are summarized in Table 2.
Table 2.
Good Day and Sick Day Picture Characteristics
| Picture Characteristic | Good Day n (%) |
Sick Day n (%) |
Chi-Square |
|---|---|---|---|
| Individuals in the picture | |||
|
| |||
| Child present | 2.163 | ||
| Yes | 19 | 24 | |
| No | 7 | 3 | |
| Other individuals present | 0.339 | ||
| Yes | 5 | 7 | |
| No | 21 | 22 | |
| Relationship of others present | 1.741 | ||
| Sibling(s) | 2 | 2^ | |
| Parent(s) | 2 | 5^ | |
| Hospital staff or volunteer | 1 | 1 | |
|
| |||
| Body proportion and position | |||
|
| |||
| Body proportion | .333 | ||
| Entire body | 17 | 20 | |
| Head/upper body | 2 | 4 | |
| Body position | 17.249** | ||
| Upright | 13*** | 6 | |
| Sitting | 4 | 1 | |
| Lying down or reclining | 0 | 12*** | |
| Bent over | 0 | 1 | |
|
| |||
| Emotions | 41.678** | ||
|
| |||
| Happy | 21*** | 1 | |
| Sad | 0 | 19*** | |
| Angry | 0 | 1 | |
| Other | 0 | 3 | |
| None | 5 | 3 | |
|
| |||
| Location | 10.265* | ||
|
| |||
| Inside | 6 | 17*** | |
| Outside | 10*** | 3 | |
| Both inside and outside | 1 | 0 | |
| Not indicated/specified | 9 | 7 | |
|
| |||
| Weather | 12.627** | ||
|
| |||
| Sunshine/blue sky | 8*** | 0 | |
| Rain/stormy | 0 | 4*** | |
| Other | 1 | 1 | |
| Not depicted | 17 | 22 | |
|
| |||
| Activities | |||
|
| |||
| Activities depicted in the picture | 14.605** | ||
| Yes | 13*** | 1 | |
| No | 13 | 26*** | |
| Location of activity | |||
| Inside activity | 7^ | 1 | |
| Outside physical activity | 7^ | 0 | |
|
| |||
| Personal coping and symptom management | |||
|
| |||
| Personal object present or named | .048 | ||
| Yes | 7 | 8 | |
| No | 19 | 19 | |
| Managing illness or treatment-related side effects depicted or described | 11.888** | ||
| Yes | 6 | 19*** | |
| No | 20*** | 8 | |
|
| |||
| Art medium and colors | |||
|
| |||
| Art medium | .008 | ||
| Pencil only | 8 | 8 | |
| Markers, colored pencils, crayons | 18 | 19 | |
| Number of colors present | .535 | ||
| One color | 9 | 12 | |
| More than one color | 17 | 15 | |
p <. 05
p<.01
Adjusted standardized residual ≥ 2
Note: picture included two or more of the characteristics of interest
Good days
“Good day” pictures were characterized by happy emotions, engaging in activities, and being free of illness or treatment-related side effects. Children also depicted themselves as being upright and being outside on “good days.” When weather was depicted, blue skies and sunshine predominated. Children’s narratives added additional detail to the experiences expressed in their pictures. As one 7-year-old girl related of her picture (Fig. 1) that included herself and her sister, “We’re playing together and having so much fun. We’re at the park going down the slide.”
Figure 1.
Good day: playing together with sibling
Sick days
In contrast, “sick day” pictures emphasized limitations children experienced as a consequence of their illness. Children most frequently depicted themselves as lying down or reclining and being inside. Only one child depicted himself as being engaged in an activity. This 10-year-old boy related, “…when I’m sick I like to read bigger books so that I can think about them more.” Although sadness predominated as an emotion, children also related experiences of anger and frustration in response to specific situations. When weather was depicted, rain and thunderstorms were most commonly represented. Children’s pictures and accompanying narratives also related the symptoms and side effects associated with their illness and its treatment as well as actions they took to manage their symptoms.
Similarities between good and sick day characteristics
Children’s “good day” and “sick day” pictures also featured several commonalities. The majority of children included themselves in their “good day” (73%) and “sick day” (89%) pictures. Although most children did not include other individuals in their drawings, parents and/or siblings were most commonly included. Parents’ roles within children’s drawings varied and included 1) caregiver, such as overseeing oral medication administration; 2) source of comfort, for example an 11-year-old girl related that when she feels sick, “I like to snuggle with my mom,” and 3) gatekeeper of information such as seeking out information to be able to tell the child what to expect. When siblings were present, they were most frequently depicted in the role of a similar-aged peer. One 8-year-old girl included hospital personnel in both pictures. Of note, no children included friends in their pictures. Two boys did, however, mention friends or neighborhood children when relating their descriptions of “good days.”
Personal objects were named with equal frequency on both “good” and “sick days.” These objects included blankets, stuffed animals, hats/scarves, pillows, chairs, books, and a bicycle. Personal objects were also depicted with similar frequency by younger (n=7) and older (n=8) children.
An inside location was more frequently depicted on “sick days.” The types of inside locations, however, were similar for both “good” and “sick days.” The hospital as well as the child’s home were depicted in both sets of pictures.
The type of drawing medium did not differ between “good day” and “sick day” pictures. Eight children drew exclusively in pencil whereas the others used a combination of pencil, colored pencil, crayons, and/or markers for each of their pictures. Although children’s use of colors did not differ between the two sets of pictures, some distinct individual preferences were noted. For example, one 6-year-old girl’s colorful “good day” picture featured herself “…playing soccer on the rainbow grass.” In contrast, her “sick day” picture was drawn exclusively in orange with a few added stickers. Her mother noted that orange was this child’s least favorite color.
Thematic Analyses
Themes represented within children’s “good day” and “sick day” pictures are summarized in Table 3.
Table 3.
Themes Represented within Children’s Good Day and Sick Day Pictures
| “Good Day” Themes | n (%) |
|---|---|
| Things I like to do | |
| Outside | 6 (23) |
| Inside | 4 (15) |
| Aspects of the illness and treatment experience | 6 (23) |
| Things I like | 6 (23) |
| Places I like to be | 4 (15) |
|
| |
| “Sick Day” Themes | |
|
| |
| Symptoms | 10 (37) |
| Managing my symptoms | 9 (33) |
| Emotions | 5 (19) |
| Stormy weather | 3 (11) |
Good days
Four themes emerged from children’s “good day” pictures. “Things I Like to Do” was the predominant theme, and ten children depicted themselves as being actively engaged in activities they enjoyed. This theme was further divided into two subthemes “Things I Like to Do Outside” (n=6) and “Things I Like to Do Inside” (n=4). Common outside activities included playing sports such as soccer, riding a bike, or playing on the playground. Inside activities included playing video games, doing crafts, playing games, and reading books.
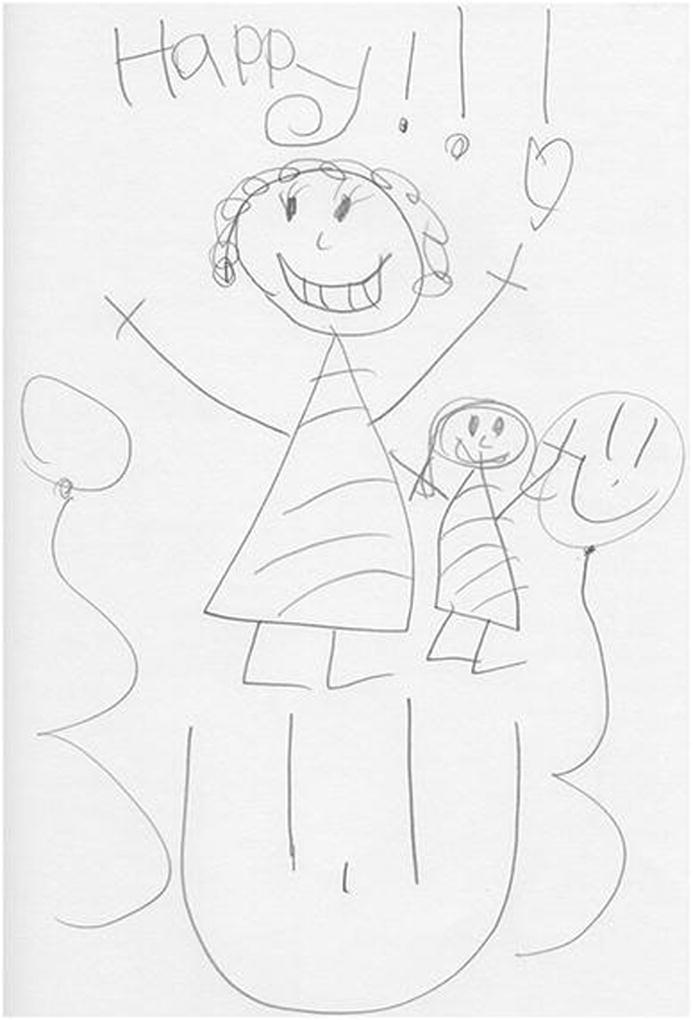
“Aspects of the Illness and Treatment Experience” (n=6) reflected that, even on “good days,” some children were acutely aware of their illness and its implications. Some children’s pictures reflected celebrating treatment-related milestones such as a final lumbar puncture (Fig. 2). Another child’s picture reflected her efforts to make the hospital room more like the home setting in the face of traveling considerable distances for repeated hospitalizations.
Figure 2.
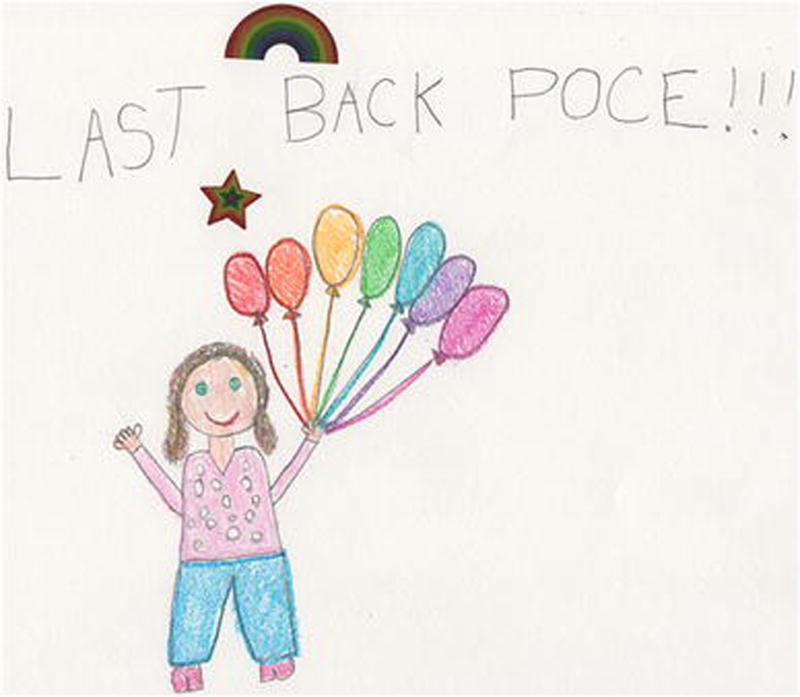
Good day: celebrating treatment milestones
Six children’s pictures emphasized “Things I Like.” This theme included both favorite characters as well an emphasis on a personal object. The emphasis within this theme was the child’s description of the character or item and why it was important to him or her.
“Places I Like to Be” (n=4) was the final theme and emphasized the place depicted in the picture. Places children depicted included memorable vacation locations, being outside in the sunshine, and home. Of note, a 10-year-old girl who had been not yet returned home following her diagnosis of Hodgkin lymphoma, personified her depiction of her house by giving it the appearance of a face with the windows featuring eyelashes and the door in the position of the mouth. A 10-year-old boy who had undergone rotationoplasty surgery and chemotherapy for osteosarcoma depicted a scene from a beach vacation that his family had taken shortly before his diagnosis (Fig. 3).
Figure 3.
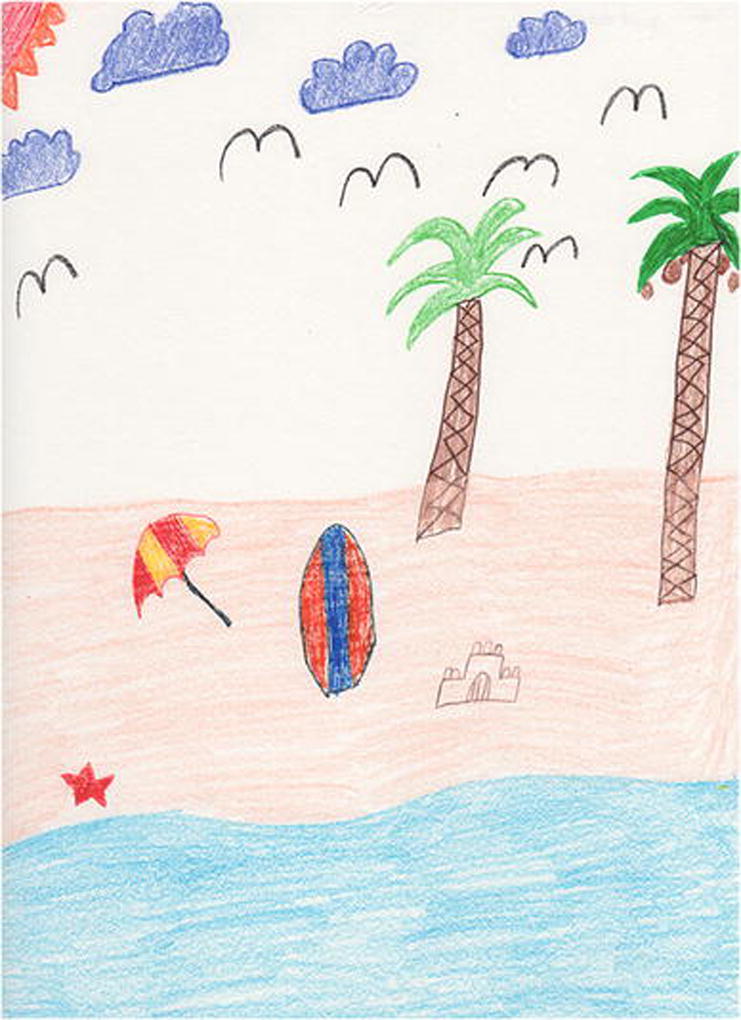
Good day: memorable vacation location
Sick days
Four themes also emerged from children’s sick day pictures. “Symptoms” was the most frequently occurring theme (n=10) and reflected children’s experience of both physical and psychosocial symptoms in response to their illness and its treatment. While children most frequently depicted nausea, fatigue, pain, and sadness as common symptoms on “sick days,” children’s pictures and accompanying narratives also identified symptoms such as difficulty with balance, itching, skin changes, and feeling embarrassed. Children’s accompanying narratives also related challenges in expressing their specific symptom experiences. For example, some children used expressions such as “droopy” or “crappy” to relate how they felt on “sick days.”
The theme, “Managing My Symptoms,” (n=9) was distinct from “Symptoms” in that it emphasized deliberate actions children took in an effort to manage their symptoms. These varied actions were personal to each child and included the use of pillows and/or blankets for comfort, maintaining close proximity to a bathroom, and the use of distractions (Fig 4).
Figure 4.
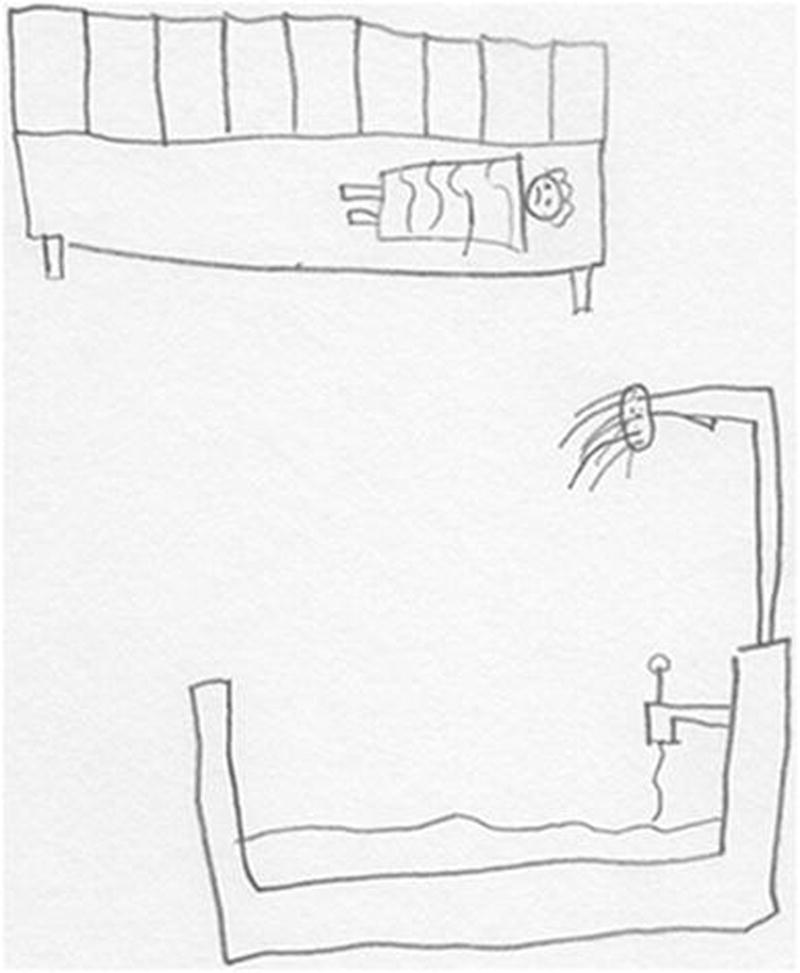
Sick day: managing symptoms
The theme, “Emotions,” (n=5) emphasized predominantly emotional responses as aspects of “sick days.” For example, a 7-year-old girl expressed sadness, uncertainty, and separation from other members of her family, even though they were depicted as being in the same home. An 8-year-old related a specific experience of anger and frustration during an earlier time in her treatment when she was receiving steroid therapy (Fig 5).
Figure 5.

Sick day: anger and frustration
The final theme for “sick days” was “Stormy Weather.” Three older children did not include individuals in their “sick day” pictures but drew pictures including storm clouds and rain (Fig 6). Two children, a 10-year-old boy and a 12-year-old girl related the limitations that the storm imposed, “… hate it because I can’t go outside,” and “…having to stay in bed.” A 10-year-old girl personified the storm cloud she drew with a sad face and tears.
Figure 6.
Sick day: stormy weather
Discussion
This study adds to the literature addressing the value of arts-based techniques to gain a greater understanding of children’s interpretation and meaning of a given phenomenon of interest. Participants’ drawings reflected shared, common experiences related to both “good days” and “sick days,” yet also reflected the distinct, individual experiences of each child. As children explained their pictures, they related additional detail and perspective that was not obvious from the drawing itself, demonstrating the capacity of the drawing process to foster recall. For example, an 8-year-old boy drew himself as bent over and “droopy.” He then went on to explain that he was “sad,” had “no energy,” was “tired,” his “head hurt,” and “[I] don’t like it.”
Similar to Woodgate’s prior work [10], children’s drawings illustrated changes associated with the cancer experience and that children’s lives are never the same following their diagnosis. The themes of “Symptoms” and “Managing My Symptoms” predominated “sick days” and prevented children from engaging in activities. In addition, nearly one fourth (n=6) of study participants included some aspect of their illness or the treatment experience in their “good day” pictures. Although none of these six children depicted themselves experiencing acute symptoms, their pictures reflected a change in life experiences as a consequence of their diagnosis.
Children’s drawings also demonstrated the capacity to distinguish between “good” and “sick” days. “Good” days were characterized by children being in an upright position, happy, engaged in some type of activity, and outside. In contrast, “sick” days were characterized by lying down or reclining, feeling sad, experiencing symptoms, and limited to being inside and not engaged in activities. These results parallel prior studies emphasizing the themes of mood, symptoms, and usual activities as developmentally meaningful aspects of quality of life for children receiving treatment for cancer [11–13]. Although weather was not depicted in most pictures, when present, it was an important feature distinguishing between good and sick days, with “good” days characterized by sunshine and “sick” days characterized by stormy weather.
On both “good” and “sick” days, parents and/or siblings were depicted as serving as children’s primary sources of social and emotional support. Children’s drawings highlighted the different ways in which their parents served as sources of support and emphasized the importance of supporting family relationships across the treatment continuum. Although social relationships were not the emphasis of this study, the absence of same-age peers from children’s pictures does illustrate potential feelings of isolation as a result of the child’s illness and treatment.
In addition to communicating the cancer experience, children’s drawings also reflected developmental characteristics typical of school-age children. While concrete, present-oriented thought predominates among children in this age group, abstract thought is emerging as children approach their teen years. Children’s drawings of both “good” and “sick” days were predominantly present-oriented. Some children, however, did elect to relate past experiences that had shaped their cancer treatment experience. Personal items were included in both “good” and “sick” day pictures and related aspects of the child’s identity, such as an emblem from a favorite sports team, as well as strategies for symptom management, such as the use of a favorite blanket. The depiction of stormy weather as a metaphor for “sick” days demonstrates emerging abstract thought among older children.
Clinical Implications
Through their drawings, children communicated an awareness of the impact of their illness and their insights into their experiences. Although children may be assumed not to understand the complexities of cancer and its treatment, children’s pictures illustrated an awareness of the consequences of cancer treatment and strategies that helped them cope with their treatment and its related symptoms. For some children, experiences that had occurred earlier in their treatment trajectory were particularly memorable and were depicted in their drawings. These findings highlight the importance of including even young children in developmentally meaningful dialogue about their diagnosis and care and involving them in choices when possible.
Although this study did not seek to evaluate changes in symptoms over time, key differences, specifically with regards to emotions, body position, and engagement in activities, distinguished “good days” from “sick days.” This ability to discriminate supports the potential for children’s drawings to be used as an adjunct to other clinical measures assessing symptoms and quality of life. Providing an opportunity for arts-based expression in the clinical setting may support children to relate their experiences more fully than through text-based or verbal responses.
Asking about the child’s activities may also provide a brief developmentally meaningful assessment of the child’s well-being and quality of life. Incorporating a deliberate question about engagement in activities could be easily integrated as part of the interval history with the child’s response prompting the need for additional follow up questions or interventions.
Limitations
Limitations of this study include a cross-sectional design and a relatively small sample size from a single clinical site that was heterogenous with regards to disease type and stage of treatment. The study sample was also predominantly White/non-Hispanic which limited the opportunity to explore racial/ethnic differences. The attention to a specific age group, school-age children, however, supported a more developmentally cohesive group. The small sample size did, however, limit greater exploration of differences and similarities between younger (6–8 years of age) and older (9–12 years of age) school-age children.
Because the emphasis of the study was on the children themselves and their depictions of “good” and “sick” days, the ability to draw conclusions about social relationships is limited. Research team members did not specifically ask about other individuals if they were not depicted in children’s pictures or addressed by children through the course of the interview. Because of the key importance of developing peer relationships among school-age children, attention to peer and other social relationships is warranted in future studies.
Directions for future research
Directions for future research include further exploration of the role of arts-based strategies to enhance chronically ill children’s communication of their illness-related experiences. As demonstrated in this study, the use of draw-and-tell interviews facilitated children’s abilities to relate their personal experiences in a developmentally meaningful manner. The inclusion of arts-based techniques as part of symptom assessment or quality of life measures may provide a more child-centric approach to addressing issues that are of priority to the child.
Additional exploration of children’s self-management strategies to address illness-related symptoms is also warranted. Children’s drawings and narratives indicated that many are actively engaging in self-management strategies to alleviate their symptoms. Further investigation of these strategies and their perceived effectiveness can add to the evidence base of child-centric symptom self-management strategies that can be implemented in the home and hospital settings.
Conclusion
Arts-based approaches, including draw-and-tell interviews provide a developmentally meaningful opportunity to gain insight into school-age children’s perceptions of aspects of their illness experience. Through their drawings, children in this study provided rich personal data related to their experiences and unique challenges that has the potential to direct interventions. Incorporating arts-based approaches may serve as additional resources to elicit the child’s voice in relating his or her quality of life.
Acknowledgments
Funding: This study was funded by the National Institute of Nursing Research: 1K23NR014874-01 The research reported in this publication was supported in part by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR000105. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Conflicts of Interest:
Lauri A. Linder, PhD, APRN, CPON declares that she has no conflict of interest.
Heather Bratton declares that she has no conflict of interest.
Anna Nguyen declares that she has no conflict of interest.
Kori Parker declares that she has no conflict of interest.
Susanna Phinney declares that she has no conflict of interest.
Compliance with Ethical Standards
Animal Research: N/A – no animals involved
Human Subjects Research: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent: Per institutional standard, written parental permission was obtained for all participants. Participants 7 to 12 years of age provided written assent. Participants 6 years of age provided verbal assent.
Contributor Information
Lauri A. Linder, University of Utah College of Nursing, Primary Children’s Hospital, Salt Lake City, UT.
Heather Bratton, University of Utah College of Nursing, Salt Lake City, UT.
Anna Nguyen, University of Utah, Salt Lake City, UT.
Kori Parker, University of Utah College of Nursing, Salt Lake City, UT.
Susanna Phinney, Primary Children’s Hospital, Salt Lake City, UT.
References
- 1.American Cancer Society. Cancer Facts & Figures 2017. Atlanta: American Cancer Society; 2017. [Accessed 29 March 2017]. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdf. [Google Scholar]
- 2.Vance YH, Eiser C. The school experience of the child with cancer. Child: Care, Health and Development. 2002;28(1):5–19. doi: 10.1046/j.1365-2214.2002.00227.x. [DOI] [PubMed] [Google Scholar]
- 3.Linder LA, Al-Qaaydeh S, Donaldson G. Symptom characteristics among hospitalized children and adolescents with cancer. Cancer Nursing. 2017 doi: 10.1097/NCC.0000000000000469. epub ahead of print January 20, 2017. [DOI] [PubMed] [Google Scholar]
- 4.Baggott C, Dodd M, Kennedy C, Matthay KK, Miaskowski C. Changes in children’s reports of symptom occurrence and severity during a course of myelosuppressive chemotherapy. Journal of Pediatric Oncology Nursing. 2010;27(6):307–315. doi: 10.1177/1043454210377619. http://dx.doi.org/10.1177/1043454210377619. [DOI] [PubMed] [Google Scholar]
- 5.Yeh CH, Wang CH, Chiang YC, Lin L, Chien LC. Assessment of symptoms reported by 10- to 18-year-old cancer patients in Taiwan. Journal of Pain and Symptom Management. 2009;38:738–746. doi: 10.1016/j.jpainsymman.2009.04.023. [DOI] [PubMed] [Google Scholar]
- 6.Walker AJ, Gedaly-Duff V, Miaskowski C, Nail L. Differences in symptom occurrence, frequency, intensity, and distress in adolescents prior to and one week after the administration of chemotherapy. Journal of Pediatric Oncology Nursing. 2010;27:259–256. doi: 10.1177/1043454210365150. doi: [DOI] [PubMed] [Google Scholar]
- 7.Miller E, Jacob E, Hockenberry MJ. Nausea, pain, fatigue, and multiple symptoms in hospitalized children with cancer. Oncology Nursing Forum. 2011;38:E382–E393. doi: 10.1188/11.ONF.E382-E393. doi: [DOI] [PubMed] [Google Scholar]
- 8.Woodgate RL. Feeling states: a new approach to understanding how children and adolescents with cancer experience symptoms. Cancer Nursing. 2008;31:229–238. doi: 10.1097/01.NCC.0000305731.95839.ca. [DOI] [PubMed] [Google Scholar]
- 9.Woodgate RL, Degner LF, Yanofsky R. A different perspective to approaching cancer symptoms in children. Journal of Pain and Symptom Management. 2003;26:800–817. doi: 10.1016/s0885-3924(03)00285-9. doi: S0885392403002859. [DOI] [PubMed] [Google Scholar]
- 10.Woodgate RL. Life is never the same: childhood cancer narratives. European Journal of Cancer Care. 2006;15:8–18. doi: 10.1111/j.1365-2354.2005.00614.x. [DOI] [PubMed] [Google Scholar]
- 11.Hicks J, Bartholomew J, Ward-Smith P, Hutto CJ. Quality of life among childhood leukemia patients. Journal of Pediatric Oncology Nursing. 2003;20:192–200. doi: 10.1177/1043454203253969. doi: [DOI] [PubMed] [Google Scholar]
- 12.Hinds PS, Gattuso JS, Fletcher A, Baker E, Coleman B, Jackson T, Pui CH. Quality of life as conveyed by pediatric patients with cancer. Quality of Life Research. 2004;13:761–762. doi: 10.1023/B:QURE.0000021697.43165.87. [DOI] [PubMed] [Google Scholar]
- 13.Momani TG, Mandrell BN, Gattuso JS, West NK, Taylor SL, Hinds PS. Children's perspective on health-related quality of life during active treatment for acute lymphoblastic leukemia: an advanced content analysis approach. Cancer Nursing. 2015;38:49–58. doi: 10.1097/NCC.0000000000000174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Driessnack M, Furukawa R. Arts-based data collection techniques used in child research. Journal for Specialists in Pediatric Nursing. 2012;17:3–9. doi: 10.1111/j.1744-6155.2011.00304.x. [DOI] [PubMed] [Google Scholar]
- 15.Driessnack M. Children's drawings as facilitators of communication: a meta-analysis. Journal of Pediatric Nursing. 2005;20:415–423. doi: 10.1016/j.pedn.2005.03.011. [DOI] [PubMed] [Google Scholar]
- 16.Gross J, Hayne H, Drury T. Drawing facilitates children’s reports of factual and narrative information: Implications for educational contexts. Applied Cognitive Psychology. 2008;23:953–971. doi: 10.1002/acp.1518. [DOI] [Google Scholar]
- 17.Butler S, Gross J, Hayne H. The effect of drawing on memory performance in young children. Developmental Psychology. 1995;31:597–608. [Google Scholar]
- 18.Driessnack M. Draw-and-tell conversations with children about fear. Qualitative Health Research. 2006;16:1414–1435. doi: 10.1177/1049732306294127. [DOI] [PubMed] [Google Scholar]
- 19.Stafstrom CE, Rostasy K, Minster A. The usefulness of children’s drawings in the diagnosis of headache. Pediatrics. 2002;109:460–472. doi: 10.1542/peds.109.3.460. [DOI] [PubMed] [Google Scholar]
- 20.Stafstrom CE, Goldenholz SR, Dulli DA. Serial Headache Drawings by Children With Migraine: Correlation with Clinical Headache Status. Journal of Child Neurology. 2005;20:809–813. doi: 10.1177/08830738050200100501. [DOI] [PubMed] [Google Scholar]
- 21.Stefanatou A, Bowler D. Depiction of pain in the self-drawings of children with sickle cell disease. Child: Care, Health, and Development. 1997;23:135–155. doi: 10.1111/j.1365-2214.1997.tb00889.x. [DOI] [PubMed] [Google Scholar]
- 22.Gabriels RL, Wamboldt MS, McCormick DR, Adams TL, McTaggart SR. Children’s illness drawings and asthma symptom awareness. Journal of Asthma. 2000;37:565–574. doi: 10.3109/02770900009090811. [DOI] [PubMed] [Google Scholar]
- 23.Druin A. Proceedings of the SIGCHI conference on Human factors in computing systems: the CHI is the limit. Association for Computing Machinery; 1999. Cooperative inquiry: Developing new technologies for children with children; pp. 592–599. Accessed at: http://hcil2.cs.umd.edu/trs/99-14/99-14.html. [Google Scholar]
- 24.Elo S, Kyngas H. The qualitative content analysis process. Journal of Advanced Nursing. 2008;62:107–115. doi: 10.1111/j.1365-2648.2007.04569.x. [DOI] [PubMed] [Google Scholar]
- 25.Krippendorff KH. Content analysis: An introduction to its methodology. 2. Thousand Oaks, CA: Sage Publications; 2004. [Google Scholar]