

Abstract
The present study evaluates the effects of a behavioral skill training package on parent implementation of discrete trial teaching with their children with autism spectrum disorder. Three mothers of children with autism participated in the study. The training package improved implementation for all three of the mothers. Moreover, these improvements generalized to skills that were not taught during training, maintained during follow-up probes, and resulted in improvements in child behavior.
Keywords: Autism spectrum disorder, Generalization, Maintenance, Parent training, Social validity
Services for individuals with psychological disorders, such as autism spectrum disorder (ASD), are not well developed in Saudi Arabia and other developing countries (Alqahtani, 2012). While the exact number of children who have ASD in Saudi Arabia is unknown, as a country of 30.7 million people, it seems likely that a large need for services exists. One study estimated that 18 in 10,000 children in Saudi Arabia are diagnosed with ASD, and it is thought that there may be many more undiagnosed cases (Al-Salehi, Al-Hifthy, & Ghazziuddin, 2009). In addition, even less is known about the adequacy of the existing services in the region, including the extent to which existing support systems utilize evidence-based practices.
While a number of services may be recommended to help meet the needs of individuals with ASD in this region, one obvious step would be that of parent education. Even more beneficial would be training parents in various evidence-based practices, using evidence-based parent training packages. Discrete-trial teaching (DTT) is an instructional technique that involves the systematic presentation of instructions, prompts, and reinforcement and has been used widely in intervention programs for children with ASD (e.g., Smith, 2001). Behavior analysts have taught caregivers to implement DTT using behavioral skills training (BST). For example, Sarakoff and Sturmey (2004) used BST to teach three special education teachers how to implement DTT. The results showed that each of the teachers’ implementation improved after training involving instructions, review of baseline data, modeling, rehearsal, and feedback. Extending upon this study, Lafasakis and Sturmey (2007) evaluated the effects of a similar BST package on parent implementation of DTT with their children with developmental disabilities. The results showed that the BST package improved parent implementation of DTT and that the parents’ implementation skills generalized to instructional programs that were not targeted during training. Moreover, Lafasakis and Sturmey also measured child behavior during instruction and found that children engaged in more accurate responding as their parents improved implementation.
Given the need for services in the region and the growing support for BST packages in training caregivers, the goal of the present study is to further evaluate the effects of a BST package on parent implementation of DTT. Specifically, the current study aims to evaluate a) the effects of a BST training package on parent implementation of DTT, b) the generality of that training to instructional programs not specifically targeted during training, c) the maintenance of those skills during 2-week follow-up probes, d) the associated changes in child behavior pre- and post-parent training, and e) the social validity of the skills taught and the BST training package itself.
Method
Participants and Setting
Three parent-child dyads participated in the study. None of the parents or children in the study had previous experience with applied behavior analysis in general and DTT specifically. Each of the children attended a center for children where evidence-based practices are lacking. Arij was a 35-year-old woman with a 9th grade education, who participated in the study with her daughter, a 6-year-old child with ASD. Basma was a 28-year-old woman with a 12th grade education, who participated in the study with her son, a 6-year-old child with ASD. Lastly, Canda was a 40-year-old woman with a Bachelor’s degree, who participated in the study with her 4-year-old son with ASD. None of the children engaged in challenging behavior that interfered with their participation. Each of the participants was recruited through a research center in a large city in Saudi Arabia dedicated to education and research in the area of ASD. All sessions were conducted in a room that was 3 by 3 m. The room included a U-shaped table, three chairs, and leisure items. Specific preferred items were present during instructional sessions. A therapist was present during all sessions for all phases.
Response Measurement and Experimental Design
The effects of the training package on parent implementation and child responding were evaluated using a multiple-probe design (Horner & Baer, 1978). Phase change decisions were made with respect to parent implementation, as this was considered the main dependent variable.
The primary dependent variable was parent implementation of DTT. Specifically, parents were scored on the extent to which they 1) completed a brief mini-preference assessment (choice between two items), 2) required eye contact with the child for at least 1 s prior to the instruction, 3) waited until the child was ready (i.e., no problem behavior) before providing instructions, 4) gave a clear instruction relevant to the task, 5) implemented a least-to-most error correction procedure within 5 s of the instruction after the student failed to respond or responded incorrectly, 6) provided immediate reinforcement for correct responses (using item identified in #1), 7) used behavior-specific praise, and 8) recorded the data for each trial. Child behavior was also measured throughout and consisted of the child engaging in the correct response (specific to the instructional task, see below) within 5 s of the discriminative stimulus.
Specific instructional targets for each child were identified using the Assessment of Basic Language and Learning Skills-Revised (Partington, 2006). All three of the children had skill deficits in the area of motor imitation, following instructions, and listener responding. Specific instructional targets for each participant were chosen based upon this information. For Arij and Canda, the primary instructional target was following the instruction “touch head” and the correct child response was touching head. For Basma, the primary instructional target was following the instruction “touch tummy” and the correct child response was touching tummy. The generalization task was the same for all children and involved a listener response to the therapist discriminative stimulus (sd) “touch cup.” The corresponding correct child response was touching cup in an array of items.
Interobserver Agreement (IOA)
Interobserver agreement data was collected for a total of 50% of all sessions (47% for Arij, 58% for Basma, and 46% for Canda). Trial-by-trial (item) data were collected by calculating the total number of steps of the task analysis with agreement divided by the total number of steps with agreement plus those with disagreement for each session and multiplying this number by 100. Mean IOA was 90% (range, 76 to 100%).
Procedure
Baseline
During baseline, parents were given instructions (translated in Arabic) that involved a list of the steps for implementing DTT (similar to the previously outlined steps). Parents were told to try their best to teach their children using the steps outlined in the instructions. Parents had access to written instructions and datasheets throughout.
Training
During training, the therapist and parent reviewed the instructions and the parent had the opportunity to ask questions. The therapist then modeled correct implementation of DTT using the target skill with the parent’s child for 10 trials. The parents were again given an opportunity to ask questions after observing the model. Parents then practiced implementing DTT with their child with the therapist providing feedback throughout. Modeling, practice, and feedback were repeated until the parent completed two 10-trial blocks with 95% or greater fidelity. As with baseline, the parent had access to the instructions and datasheets throughout.
Post-Training
Post-training probes were conducted in the same manner as baseline sessions.
Generalization Probes
Generalization probes were conducted during both pre- (Arji and Basma) and post-training (all participants) and were the same as baseline probes with the exception that parents were asked to teach a different skill than they had been teaching in training.
Maintenance Probes
Maintenance probes were the same as baseline probes and conducted 2 weeks after the last post-training probe for each participant.
Generalization Overview and Social Validity
After the final maintenance probe, therapists reviewed strategies to promote generalization with parents and parents were also given a social validity survey. The social validity survey consisted of two questions: “Do you feel like you learned important skills by participating in this study?” and “Did you like participating in the training?”. Participants answered on a 5-point Likert-type scale with 1 being “no” and 5 being “definitely.”
Results
The results of the parent training evaluation are depicted in Fig. Fig. 1. Arij had low scores during baseline, with an average score of 10% (range, 7 to 12%). Arij’s baseline generalization probe was 34%. During training, Arij’s scores improved and she met criteria after seven sessions. Arij scored 98% during both post-test probes and 80% during the post-training generalization probe. Finally, Arij scored 95% during the maintenance probe. Figure Fig. 2 depicts the impact of the parent training on child behavior. Arij’s child scored an average of 3% correct during baseline (range, 0 to 10%), and her performance improved after parent training (M = 90%; range, 70 to 100%). Arij’s child scored 80% correct during generalization and 90% correct during the maintenance probe.
Fig. 1.
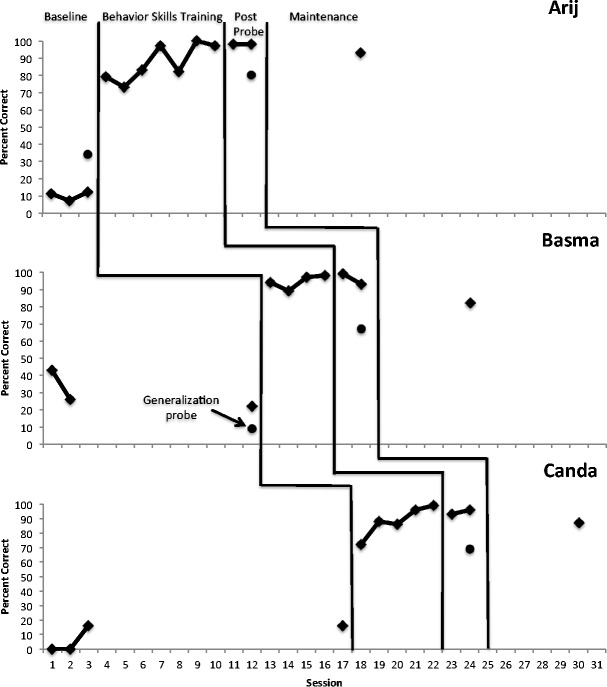
Percent correct of parent implementation during baseline, training, post-training, and follow-up phases
Fig. 2.
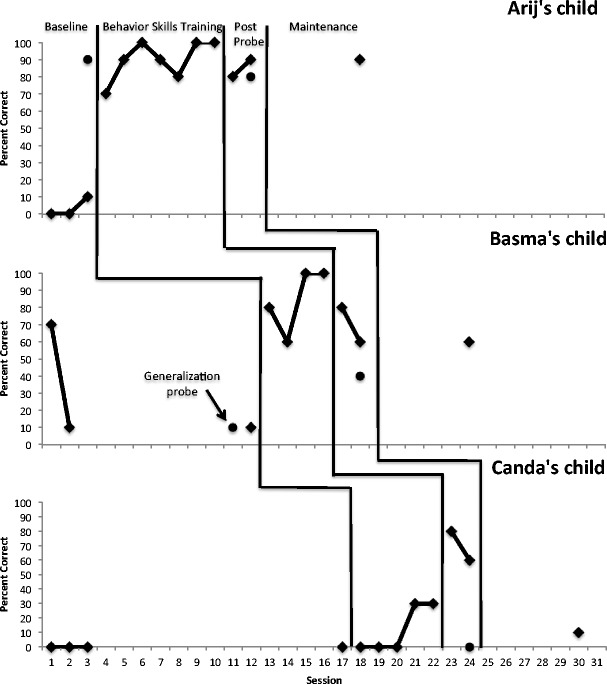
Percent correct of child behavior during baseline, training, post-training, and follow-up phases
Basma had low scores during baseline, with an average score of 30% (range, 22 to 43%). Basma’s baseline generalization probe was 9%. During training, Basma’s scores improved and she met the criteria after four sessions. During post-tests, Basma scored 99 and 93%. Basma’s post-training generalization probe was 67%, and her maintenance probe was 82%. Basma’s child scored low during baseline (M = 30%, range, 10 to 70%), and improved after his mother was trained (M = 80%, range, 60 to 100%). Basma’s son scored 40% during the generalization probe and 60% during the maintenance probe.
Canda also had low scores during baseline (M = 8%, range, 0 to 16%). During training, Canda’s scores improved and she met the criteria after five sessions. Canda scored 93 and 96% during post-tests, and 69 and 87% during the generalization and maintenance probes. Canda’s child scored 0% during all baseline sessions, and his performance improved after parent training (M = 70%; range, 60 to 80%). However, Canda’s child had low scores during generalization (0%) and maintenance (10%) probes.
Each of the parents rated both of the questions on the Social Validity Survey with a 5, the highest rating. This indicates that the parents believed the skills they learned were important and that they enjoyed participating in the training.
Discussion
The results of the present study show that a brief BST program can improve the implementation of DTT with parents of children with ASD in Saudi Arabia. Moreover, improvements in implementation skills were found to generalize untrained instructional programs and maintain at a 2-week follow-up. Importantly, improvement in parent implementation was also found to be associated with improvements in child behavior. Finally, each of the parents thought that the skills taught were important and enjoyed participating in the training. While information pertaining to social validity is always important, it may be particularly important when considering that the study was conducted in a country where little behavior analytic research has been conducted.
Future researchers may consider a number of issues pertaining to the present study, especially when considering the great need for qualified providers in Saudi Arabia. While the results of the present study are promising, it is possible that an even more efficient means to teach skills to parents and other caregivers would be via group parent training. Training one-on-one requires staff resources, and it is possible that group parent training programs may help to circumvent this issue. Of course, the extent to which various group parent trainings lead to behavior change requires further exploration. Similarly, it seems plausible that a pyramidal training arrangement may be helpful. In other words, an additional strategy to help with the lack of services in the region may be to train people (such as parents) to train others (such as other family members).
Future researchers may also want to look into the type of errors that were made by parents. It is possible that certain errors are more or less detrimental than others (see Fryling, Wallace, & Yassine, 2012), and researchers may want to examine whether or not these also tend to be the sort of errors that are made more often and alter training programs accordingly. In addition, future research may consider teaching task interspersal and related skills to parents. Finally, while the present study did assess maintenance at 2 weeks, the extent to which parental implementation maintains for longer periods of time is unknown. Along with this, more thorough assessments of generalization and child behavior acquisition may also be considered in future studies.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Footnotes
-Practitioners may teach parent skills quickly using behavioral skills training procedures.
-Skills learned generalized and maintained, though booster trainings may be needed.
-Social validity assessment is useful in understanding the acceptability of training targets and programs.
-Important to consider the type of errors made—some errors are more or less detrimental to learning.
References
- Alqahtani MMJ. Understanding autism in Saudi Arabia: a qualitative analysis of the community and cultural context. Journal of Pediatric Neurology. 2012;10:15–22. [Google Scholar]
- Al-Salehi SM, Al-Hifthy EH, Ghazziuddin M. Autism in Saudi Arabia: Presentation, clinical correlates, and comorbidity. Transcultural Psychiatry. 2009;46:340–347. doi: 10.1177/1363461509105823. [DOI] [PubMed] [Google Scholar]
- Fryling MJ, Wallace MD, Yassine J. Impact of treatment integrity on intervention effectiveness. Journal of Applied Behavior Analysis. 2012;45:449–453. doi: 10.1901/jaba.2012.45-449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horner RD, Baer DM. Multiple-probe technique: a variation on the multiple-baseline design. Journal of Applied Behavior Analysis. 1978;11:189–196. doi: 10.1901/jaba.1978.11-189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lafasakis M, Sturmey P. Training parent implementation of discrete-trial teaching: effects on generalization of parent teaching and correct child responding. Journal of Applied Behavior Analysis. 2007;40:685–689. doi: 10.1901/jaba.2007.685-689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Partington JW. Assessment of basic language and learning skills—revised. Pleasant Hill: Behavior Analysts, Inc.; 2006. [Google Scholar]
- Sarakoff RA, Sturmey P. The effects of behavioral skills training on staff implementation of discrete-trial teaching. Journal of Applied Behavior Analysis. 2004;37:535–538. doi: 10.1901/jaba.2004.37-535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith T. Discrete-trial training in the treatment of autism. Focus on Autism and Other Developmental Disabilities. 2001;16(2):86–92. doi: 10.1177/108835760101600204. [DOI] [Google Scholar]