

Abstract
The American Association of Physicists in Medicine (AAPM) is a nonprofit professional society whose primary purposes are to advance the science, education, and professional practice of medical physics. The AAPM has more than 8,000 members and is the principal organization of medical physicists in the United States.
The AAPM will periodically define new practice guidelines for medical physics practice to help advance the science of medical physics and to improve the quality of service to patients throughout the United States. Existing medical physics practice guidelines will be reviewed for the purpose of revision or renewal, as appropriate, on their fifth anniversary or sooner.
Each medical physics practice guideline represents a policy statement by the AAPM, has undergone a thorough consensus process in which it has been subjected to extensive review, and requires the approval of the Professional Council. The medical physics practice guidelines recognize that the safe and effective use of diagnostic and therapeutic radiology requires specific training, skills, and techniques, as described in each document. Reproduction or modification of the published practice guidelines and technical standards by those entities not providing these services is not authorized.
1. Introduction
The review and management of computed tomography (CT) protocols is a facility's ongoing mechanism of ensuring that exams being performed achieve the desired diagnostic image quality at the lowest radiation dose possible while properly exploiting the capabilities of the equipment being used. Therefore, protocol management and review are essential activities in ensuring patient safety and acceptable image quality. These activities have been explicitly identified as essential by several states 1 , 2 regulatory and accreditation groups such as the American College of Radiology (ACR) CT Accreditation program, (3) as well as the Joint Commission in its Sentinel Event Alert, (4) among others. The AAPM considers these activities to be essential to any quality assurance (QA) program for CT, and as an ongoing investment in improved quality of patient care.
CT exam protocols are used to obtain the diagnostic image quality required for the exam, while minimizing radiation dose to the patient and ensuring the proper utilization of the scanner features and capabilities. Protocol Review refers to the periodic evaluation of all aspects of CT exam protocols. These parameters include acquisition parameters, patient instructions (e.g., breathing instructions), the administration and amounts of contrast material (intravenous, oral, etc.), and postprocessing parameters. Protocol Management refers to the process of review, implementation, and verification of protocols within a facility's practice.
This is a complex undertaking in the present environment. The challenges in optimization of dose and image quality are compounded by a lack of an automated mechanism to collect and modify protocols system‐wide. The manual labor involved in identifying, recording, and compiling for review and subsequent implementation of all relevant parameters of active protocols is not inconsequential. (5) The clinical community needs effective protocol management tools and efficient methods to replicate protocols across different scanners in order to ensure consistent protocol parameters. The ability to quickly view and understand the myriad of CT protocol parameters contained within a single exam type is critical to the success of protocol review. The ability to quickly identify an outlier protocol parameter would also be hugely beneficial to the CT protocol review process.
This MPPG only applies to CT scanners used for diagnostic imaging. It is not applicable to scanners used exclusively for:
Therapeutic radiation treatment planning or delivery;
Only calculating attenuation coefficients for nuclear medicine studies; or
Image guidance for interventional radiologic procedures.
2. Definitions
CT Protocol ‐ the collection of settings and parameters that fully describe a CT examination (6) Protocols may be relatively simple for some body part specific systems or highly complex for full‐featured, general‐purpose CT systems. (7)
Qualified Medical Physicist ‐as defined by AAPM Professional Policy 1 (8)
3. Staffing Qualifications and Responsibilities
-
The Protocol Review and Management Team
Protocol Review and Management requires a team effort; this team must consist of at least a lead CT radiologist, the lead CT technologist, and qualified medical physicist (QMP). In addition, a senior member of the facility administration team should also be involved. This could be the Chief Medical or Administrative Officer for the facility, or a dedicated Radiology Department Administrator/Manager, as determined by hospital leadership. If a senior member of the facility administration team is not a member of the Protocol Review and Management Team, there should be a clear delineation of the reporting structure.
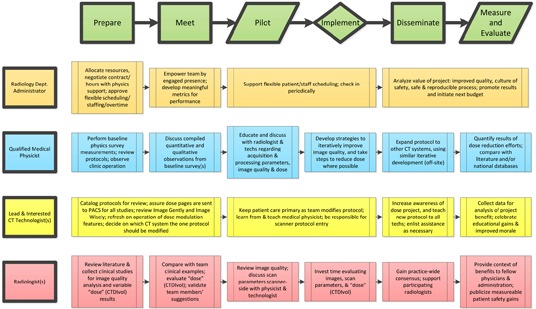
This team must be responsible for protocol design and review of all parameter settings. Each team member brings different expertise and may have different responsibilities in the Protocol Review and Management process. To be successful, it is very important that the expectations of roles and responsibilities of each member are clearly described. The ability to work together as a team will be an important attribute of each member of this group. The flow chart in Appendix A is an example of how team members should work together and in parallel during the process. (5) Additional examples of protocol management based on one facility's experience are discussed in References 9 and 10. The team members, their qualifications and expectations are described below.-
Qualified Medical Physicist (QMP)The first Professional Policy of the AAPM provides a comprehensive definition of a Qualified Medical Physicist (QMP). (8) The subfield of medical physics applicable for CT Protocol Management is Diagnostic Medical Physics. As stated by the Policy, “a [QMP] is an individual who is competent to independently provide clinical professional services in one or more of the subfields of medical physics” and meets each of the following credentials:
- “Has earned a master's or doctoral degree in physics, medical physics, biophysics, radiological physics, medical health physics, or equivalent disciplines from an accredited college or university; and
- Has been granted certification in the specific subfield(s) of medical physics with its associated medical health physics aspects by an appropriate national certifying body and abides by the certifying body's requirements for continuing education.”
- For Diagnostic Medical Physics, the acceptable certifying bodies as of 2012 are: the American Board of Radiology, the American Board of Medical Physics, and the Canadian College of Physicists in Medicine.
-
Responsibilities of the QMPIn the context of CT Protocol Management and Review, the QMP's responsibilities may vary, depending on the type of facility being supported; regardless, the QMP must be involved in the review of all protocols. These considerations should be balanced with adequate response times to facility inquiries.A QMP's time at a facility should include but not be limited to:
- meeting with the CT Protocol Management and Review team;
- clinical observation; phantom measurements;
- side‐by‐side image review with radiologist(s);
- artifact review with technologist(s) and/or radiologist(s); and
- discussion of equipment performance and operation, etc.
While regular dialogue is important, the QMP should also remember that facility personnel themselves, in particular the Lead CT Radiologist, should lead the CT Protocol Management and Review process; the QMP is an integral member of the team. The QMP may elect to perform baseline dose measurements and image quality tests at the outset of the project, particularly if the QMP does not have personal historical experience with the scanner(s) in the facility. -
In‐house QMPFor the in‐house QMP, this ongoing CT protocol review project may consume much of his/her time, so the QMP should be sure to adequately communicate with his/her supervisor(s), with other team members, and with department/hospital management in this regard. The facility should understand that the CT Protocol Management and Review process is an ongoing investment in improved quality of patient care.In‐house QMPs may be able to arrange more frequent meetings with CT Protocol Management and Review team members than their consulting colleagues; six to twelve meetings annually may be more appropriate for facilities with in‐house QMPs, with the meeting frequency likely decreasing as time goes on and the facility's protocols are sufficiently improved.
-
Consulting QMPIt is important to note that CT Protocol Management and Review services are above and beyond normal QMPs consulting services (e.g., the annual physics survey), which have traditionally been limited to image quality, dosimetry, and basic protocol review for a few selected examinations. Consultant QMPs should make this clear to their clients, and negotiate their services appropriately.QMPs providing consulting services should maintain regular dialogue with the facility via convenient means (e.g., email, phone, and perhaps text message, if appropriate). It may be beneficial to use a communication process that provides a log of these interactions. It is recommended that the consulting QMP discuss with each facility access to images, including, but not limited to, remote access to the facility's Picture Archiving and Communication System (PACS) for improved consultative capabilities.Consulting QMP's should work with the facility to arrange mutually agreeable times to visit the facility for CT protocol portfolio review activities. Three to four visits annually may be reasonable.
-
Qualifications and Expectation of the Lead CT TechnologistThe American Society of Radiologic Technologists (ASRT) has developed a practice standard entitled The Practice Standards for Medical Imaging and Radiation Therapy — Computed Tomography Practice Standards, effective June 19, 2011, which describes the education and certification requirements and scopes of practice for CT technologists. (11)The Lead CT Technologist is expected to provide the interface between the patient, staff, and the equipment. This includes workflow, the assembly and management of the CT portfolio, and education of the technologist pool.
-
Qualifications of the CT RadiologistFacilities should refer to the ACR for guidance on the requirements for physicians for accreditation or those in the Practice Guideline for Performing and Interpreting ) and CT Accreditation Program Requirements. (13)The CT radiologist leads the CT Protocol Management and Review and defines image quality requirements (14)
-
4. The Protocol Management Review Process
It is important that the CT Protocol Review and Management team designs and reviews all new or modified protocol settings for existing and new scanners to ensure that both image quality and radiation dose aspects are appropriate. Each member of CT Protocol Management team has a critical role related to his or her specific area of expertise for the evaluation, review, and implementation of protocols. The following elements should be considered for inclusion in a specific facilities' protocol review process:
While performing the review process, the CT Protocol Management team should pay particular attention to the oversight and review of existing protocols along with the evaluation and implementation of new and innovative technologies that can improve image quality and/or lower patient dose in comparison to the older protocol.
Particular attention should be paid to the specific capabilities of each individual scanner (e.g., minimum rotation time, automatic exposure controls including both tube current modulation, as well as kV selection technologies, iterative reconstruction, reconstruction algorithms, etc.) to ensure maximum performance of the system is achieved. In addition, consideration should be made to consolidate protocols or remove legacy protocols that may not be current or applicable any longer.
The review process should include a review of the most current literature such as ACR practice guidelines, (12) AAPM protocol list, (7) and peer‐reviewed journals, etc., to ensure state‐of‐the‐art protocols are being utilized.
The following considerations are important during review of a protocol:
-
Recommendations for State and National Guidance
Local, state, and federal law or regulation varies greatly depending on the state in which the facility is located. The QMP must be familiar with applicable federal law and the specific requirements for the state or local jurisdiction where the facility is located. Protocol review and management, while not always explicitly required by state law or regulation, may often facilitate compliance with many provisions within state laws and regulations relating to radiation dose from CT. Links to applicable state regulations can be found at: http://www.aapm.org/government_affairs/licensure/default.asp.
-
Frequency of Review
The review process must be consistent with federal, state, and local laws and regulations. If there is no specific regulatory requirement, the frequency of protocol review should be no less frequent than 24 months. This review should include all new protocols added since the last review. However, the best practice would be to review a facility's most frequently used protocols at least annually.
-
Clinically Significant Protocols that Require Annual Review
For every facility there are protocols that are used frequently or could result in significant doses. If a facility performs the following six clinical protocols, the CT Protocol Review and Management team must review these annually (or more frequently if required by state or local regulatory body). Facilities that do not perform all of the exams listed below must select additional protocols at their facility, either the most frequently performed or higher‐dose protocols, to a total of at least six for annual review. The six clinical protocols requiring annual review are:- Pediatric Head (1 year old) (if performed at the institution)
- Pediatric Abdomen (5 year old; 40–50 lb. or approx. 20 kg) (if performed at the institution)
- Adult Head
- Adult Abdomen (70 kg)
- High Resolution Chest
- Brain Perfusion (if performed at the institution)
-
Protocol Naming
A facility should consider naming CT protocols in a manner consistent with the RadLex Playbook ID. (15) This would provide a more consistent experience for patients and referring physicians, and allow more direct comparison among various facilities. This practice may also allow more direct utilization of the ACR Dose Index Registry (16) tools and provide more efficient automated processes with postprocessing workstations. Also, the standardization of protocol names between scanners, even when the scanners are of different makes and models, is strongly encouraged. Appropriate protocol naming will likely result in fewer technologist errors and allow more efficient comparison of protocol parameters between scanners. A facility should consider incorporating version dates in protocol names to easily confirm the latest approved version.
- Permissions
- It is important that each facility establish a process for determining who has permission to access the protocol management systems. Each facility should decide and document who has permission to change protocol parameters on the scanner(s). If the scanner allows password protection of protocols, then the facility is encouraged to use this important safety feature. Facilities should also decide how passwords are protected and archived.
- Each facility should decide on the process of making protocol adjustments and the frequency with which these adjustments should be made. This includes decisions as to what approvals need to be secured before a protocol adjustment may be made, and the documentation process (e.g., a change control log documenting the rationale for each change, as well as who authorized or motivated the change).
- Each facility should consider how to most effectively utilize the NEMA XR 26 standard (Access Controls for Computed Tomography) (17) when these tools become available on scanners at their facility.
- Acquisition parameters including kV, mA, rotation time, collimation or detector configuration, pitch, etc., should be reviewed to ensure they are appropriate for the diagnostic image quality (noise level, spatial resolution, etc.) necessary for the clinical indication(s) for the protocol, while minimizing radiation dose. For example, a slow rotation time and/or low pitch value would not be appropriate for a chest CT exam due to breath‐hold issues.
-
The facility should explicitly review the expected Volume Computed Tomography Dose Index () values. For the limited set of protocols where reference values are available, the values should be compared to the reference values of the ACR CT Accreditation Program, (3) Dose Reference Levels (DRLs), (18) AAPM CT Protocols, (7) or other available reference values for the appropriate protocols.Note: These reference values may be exceeded for individual patient scans (such as for a very large patient, or when the routine protocol is not used because of a different clinical indication, or when the reference value only refers to a single pass in a multipass study).
- For a facility's routine protocol for a standard sized patient, the expected values should be below these reference values.
-
Reconstruction parameters such as the width of the reconstructed image (image thickness), distance between two consecutive reconstructed images (reconstruction interval), reconstruction algorithm/kernel/filter, and the use of additional image planes (e.g., sagittal or coronal planes, etc.) should also be reviewed to ensure appropriate diagnostic image quality (noise level, spatial resolution, etc.) necessary for the clinical indication(s) for the protocol. For example, a high‐resolution chest exam typically generates thin (~ 1 mm) images using a sharp reconstruction filter.
- Advanced dose reduction techniques should be considered when the use of such techniques is consistent with the goals of the exam. Depending on the capabilities of each specific scanner, consider use of the following, if they are available:
- Automatic exposure control (e.g., tube current modulation or automatic kV selection) methods.
- Iterative reconstruction techniques.
Adjustments of acquisition parameters should be adjusted for patient size, either through a series of manual adjustments or through the use of automatic techniques (such as tube current modulation methods that adjust for patient size).
- Radiation dose management tools fall under two related but different categories, and may provide CT dose data that can be used to determine facility reference dose ranges.
- Radiation dose management tools that identify when potentially high‐radiation dose scans are being prescribed should be implemented when available. This includes dose reporting and tracking software, participation in dose registries, and methods as described in the MITA XR25 standard (“Dose Check”). (19)
- Radiation dose management tools may be used to monitor doses and collect data from routine exams. Statistical analysis of dose parameter values for a specific exam or clinical indication (e.g., average for a routine noncontrast head) can be provided. Participation in a national registry (such as the ACR Dose Index Registry) (16) and use of commercial dose tracking products are now available for this purpose.
-
Populating Protocols Across Scanners
Each facility should decide on the process by which protocol parameters are populated across additional scanners (whether this is done manually or by copy/paste, if the scanners allow). The facility should decide whether there are ‘master’ or ‘primary’ scanners in the facility where manual protocol adjustments are to be made and archived, and that set of protocols moved to the other similar scanners, or if another strategy will be employed.
-
Documentation
The CT Protocol Review and Management team should maintain documentation of all changes to protocols, and historical protocols should be available for review. Documentation should include the rationale for changes (e.g., improve temporal resolution, reduce breath‐hold time, reduce patient dose, etc.). The latest protocol should be readily and obviously available to users during clinical protocol selection. In some settings it may be helpful to maintain historical protocols on the scanner, in a less conspicuous location or clearly labeled as a legacy protocol.
The facility should decide and document who is responsible for maintaining the overall protocol description documentation. The facility should also describe whether the protocol description documentation is accessible to others for reference, how often it is updated, and how all protocols (on the scanners as well as the protocol description documentation) are archived.
-
Periodic Vendor‐specific Education/Refresher Sessions
The CT Protocol Management Process team is responsible for ensuring that each member is adequately trained for protocol review on each scanner used at his or her facility. Each member of the CT Protocol Management Process team should receive refresher training no less than annually or when new technology is introduced that substantially impacts image quality or dose to the patient.- Available educational resources should be considered in order to keep staff updated on current best practices.
- Periodic refresher training should be scheduled for all members of the CT Protocol Management Process team.
- Attendance should be taken at initial and all refresher‐training sessions, and consequences identified for failure to complete training.
-
Verification
Once a CT Protocol Management Process has been established, the CT Protocol Review and Management team must institute a regular review process of all protocols to be sure that no unintended changes have been applied that may degrade image quality or unreasonably increase dose.
As a best practice, the CT Protocol Review and Management team should conduct a random survey of specific exam types to verify that the protocols used are acceptable and consistent with protocols specified above. This should involve a limited review of recent patient cases to assess:- Acquisition and reconstruction parameters,
- Image quality, and
- Radiation dose.
5. Conclusion
CT protocol management and review is an important part of a CT facility's operation and is considered important by many state regulatory bodies, accrediting, and professional organizations. Protocol parameter control and periodic review will help maintain the facility's image quality to acceptable levels, and will serve to assure patient safety and continuous improvement in the imaging practice.
ACKNOWLEDGMENTS
This guideline was developed by the Medical Physics Practice Guideline Task Group‐225 of the Professional Council of the AAPM.
TG‐225 Members:
Dianna D. Cody, Chair, PhD, FAAPM
Tyler S. Fisher, MS
Dustin A. Gress, MS
Rick Robert Layman, Jr., MS
Michael F. McNitt‐Gray, PhD, FAAPM
Robert J. Pizzutiello, Jr., MS, FAAPM
Lynne A. Fairobent, AAPM Staff
AAPM Subcommittee on Practice Guidelines – AAPM Committee responsible for sponsoring the draft through the process.
Joann I. Prisciandaro, PhD, Chair
Maria F. Chan, PhD, Vice‐Chair Therapy
Jessica B. Clements, MS
Dianna D. Cody, PhD, FAAPM
Indra J. Das, PhD, FAAPM
Nicholas A. Detorie, PhD, FAAPM
Vladimir Feygelman, PhD
Jonas D. Fontenot, PhD
Luis E. Fong de los Santos, PhD
David P. Gierga, PhD
Kristina E. Huffman, MMSc
David W. Jordan, PhD
Ingrid R. Marshall, PhD
Yildirim D. Mutaf, PhD
Arthur J. Olch, PhD, FAAPM
Robert J. Pizzutiello Jr., MS, FAAPM, FACMP, FACR
Narayan Sahoo, PhD, FAAPM
J. Anthony Seibert, PhD, FAAPM, FACR
S. Jeff Shepard, MS, FAAPM, Vice‐Chair Imaging
Jennifer B. Smilowitz, PhD
James J. VanDamme, MS
Gerald A. White Jr., MS, FAAPM
Ning J. Yue, PhD, FAAPM
Lynne A. Fairobent, AAPM Staff
APPENDIX
Appendix A: Example of how team members may work together and in parallel during the process.
REFERENCES
- 1. AB 510, Radiation control: health facilities and clinics: records. 2011–2012 Reg. Sess. (CA 2012). An act to amend Sections 115111, 115112, and 115113 of the Health and Safety Code, relating to public health, and declaring the urgency thereof, to take effect immediately. Available from: http://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201120120AB510&search_keywords
- 2. Rules and Regulations ‐ Radiation Control Program [Internet]. Austin, TX: Texas Department of State Health Services (DSHS) Last updated 25 July 2013. Available from: http://www.dshs.state.tx.us/radiation/rules.shtm#227 [Google Scholar]
- 3. American College of Radiology. CT Accreditation Program. Available from: http://www.acr.org/Quality‐Safety/Accreditation/CT
- 4. The Joint Commission Sentinel Event Alert: Radiation risks of diagnostic imaging. Issue 47, August 24, 2011. Available from: http://www.jointcommission.org/assets/1/18/SEA 47.pdf [PubMed]
- 5. Siegelman JR, and Gress DA. Radiology stewardship and quality improvement: the process and costs of implementing a CT Radiation Dose Optimization Committee, in a medium sized community hospital system. J Am Coll Radiol. 2013;10(6):416–22. [DOI] [PubMed] [Google Scholar]
- 6. AAPM. CT Lexicon, ver. 1.3, 04/20/2012. Available from: http://www.aapm.org/pubs/CTProtocols/documents/CTTerminologyLexicon.pdf
- 7. AAPM. CT scan protocols. Available from: http://www.aapm.org/pubs/CTProtocols/
- 8. AAPM. Professional Policy Statement, PP 1‐H: Definition of A Qualified Medical Physicist. Available from: http://www.aapm.org/org/policies/details.asp?id=316&type=PP
- 9. Siegle C, Kofler JM, Torkelson JE, Leitzen SL, McCollough CH. CT scan protocol management. Presented at the Radiological Society of North America Scientific Assembly and Annual Meeting, Chicago, Illinois, November 2004. [Google Scholar]
- 10. Kofler JM, McCollough CH, Vrieze TJ, Bruesewitz MR, Yu L, Leng S. Team‐based methods for effectively creating, managing and distributing CT protocols. Presented at the Radiological Society of North America Scientific Assembly and Annual Meeting, Chicago, Illinois, November, 2010. [Google Scholar]
- 11. ASRT. The practice standards for medical imaging and radiation therapy ‐ computed tomography practice standards (effective June 19, 2011). Available from: http://www.asrt.org/main/standards‐regulations/practice‐standards/practice‐standards
- 12. ACR. ACR practice guideline for performing and interpreting diagnostic computer tomography (CT). Available from: http://acr.org/~/media/ACR/Documents/PGTS/guidelines/CT_Performing_Interpreting.pdf
- 13. ACR. CT accreditation program requirements. Available from: http://acr.org/~Ymedia/ACR/Documents/Accreditation/CT/Requirements.pdf
- 14. ACR. CT accreditation program clinical image quality guide. Available from: http://www.acr.org/~/media/ACR/Documents/Accreditation/CT/ImageGuide.pdf
- 15. RSNA. RadLex playbook. Available from: http://rsna.org/RadLex_Playbook.aspx
- 16. ACR. National radiology data registry: dose index registry [website]. Available from: www.acr.org/nrdr
- 17. NEMA. Access controls for computed tomography: identification, interlocks, and logs. NEMA XR 26–2012. Rosslyn, VA: National Electrical Manufacturers Association; 2012. [Google Scholar]
- 18. McCollough C, Branham T, Herlihy V, et al. Diagnostic reference levels from the ACR CT Accreditation Program. J Am Coll Radiol. 2011;8(11):795–803. [DOI] [PubMed] [Google Scholar]
- 19. NEMA. Computed tomography dose check. NEMA XR 25–2010. Rosslyn, VA: National Electrical Manufacturers Association; 2010. [Google Scholar]