

Key Clinical Message
Coughing could induce symptomatic, frequent atrial premature contractions (APCs), and episodes of atrial tachycardia (AT) in a rare case. If multiple arrhythmic drugs therapy failed to control the symptoms, catheter ablation was an effective therapeutic option for abolishing such atrial tachyarrhythmias guided by the electroanatomic mapping systems.
Keywords: atrial premature contractions, Coughing‐induced atrial tachyarrhythmias, electroanatomic mapping, short atrial runs
Introduction
Physiological activity‐induced tachyarrhythmias are seldom seen in clinical practice, of which the common type is swallowing‐induced atrial premature contractions (APCs) or atrial tachycardia (AT), with the prevalence of 0.6% according to a previous report 1. Here, we report a rarer case of coughing‐induced atrial tachyarrhythmias, which was medication‐resistant and was successfully treated by catheter ablation.
Case report
A 58‐year‐old man experienced coughing‐induced palpitation for 2 years. The symptom was induced by spontaneous or intentional coughing rather than by swallowing or other physiological activities. His 24‐h Holter monitoring detected frequent APCs and short AT when he coughed. His past history was unremarkable. After failure of antiarrhythmic drug (AAD) treatment with metoprolol, propafenone, and amiodarone, the patient was referred for radiofrequency (RF) catheter ablation.
Ventricular‐atrial (V‐A) dissociation was noted by pacing from right ventricular apex (RVa) at baseline cycle length (CL) of 500 ms, and no A‐H jump was present by programmed S1S2 stimulation (500 ms/350 ms) from high right atrium (HRA). Intravenous isoproterenol infusion (2–5ug/min) could not induce the clinical arrhythmias. However, repetitive APCs and short AT with a variable CL (271 ms–320 ms) were recorded when the patient coughed spontaneously or intentionally (Figure 1).
Figure 1.

Panel A: Tracings were surface ECG lead II, V1, CS1, 2‐CS9, 10, and RVa. Short atrial tachycardia was induced by coughing (Red arrow), with constant proximal to distal CS sequence and varying cycle length 271 ms‐320 ms. CS, coronary sinus. RVa, right ventricular apex.
Electroanatomic mapping was commenced in the right atrium. The earliest activation at the right‐sided postero‐inferior interatrial septum was targeted for ablation. Saline‐irrigated RF energy delivery (35W, 43°C for 150 sec) at this site successfully eliminated both APCs and short AT (Figure 2A–D). After ablation no atrial tachyarrhythmias could be induced by coughing. The procedure was completed uneventfully. The patient was discharged 2 days postablation without taking AADs.
Figure 2.
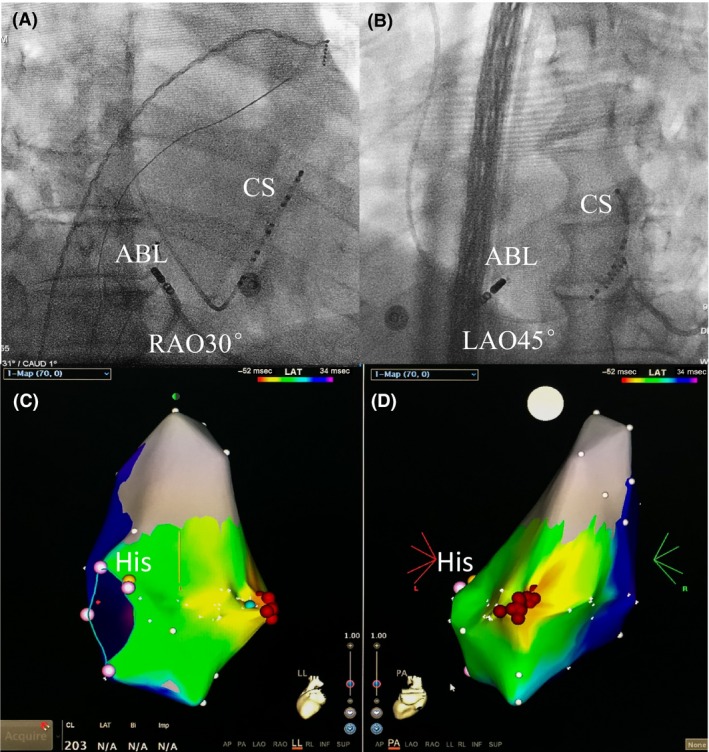
Panel A and Panel B right anterior oblique (RAO) 30° and left anterior oblique (LAO) 45° view of the position of ablation catheter tip (ABL), where the ectopic focus was successfully ablated. CS, coronary sinus. Panels C and D left lateral (LL) and postero‐anterior (PA) view of left atrial activation mapping for short atrial runs. The earliest activation was coded with red and the latest with blue and purple. His, His potential. White dots represented tricuspid annulus. Red dots indicated ablation lesions.
The patient was symptoms free, and no arrhythmia recurrence was detected by ECG and Holter recording (off AADs) at the end of 9‐month follow‐up.
Discussion
Compared to swallowing‐induced tachycardia, coughing‐induced tachyarrhythmia was even more rarely reported 1, 2. The postulated mechanisms included the neural reflex (vasovagal or adrenergic) or direct compression of the left atrium by the solid content within the esophagus 1, 2. The latter might not be the causative factor for coughing‐induced tachyarrhythmias. Unlike mechanical stimulation of the posterior wall of left atrium during swallowing solid food, it seemed no direct compression of the left atrium occurred at the time of coughing. The vasovagal reflex, rather than adrenergic ones, might be responsible for the occurrence of such arrhythmias in this patient, because not APCs or AT could be induced by intravenous isoproterenol infusion. While coughing could elevate pressure in the right atrium, trigger vasovagal reflex, and the increased vagal tone might lead to dispersion of atrial repolarization and favor the occurrence of microreentry in some specific parts of the atrium.
Conclusion
Similar to swallowing, coughing might induce atrial tachyarrhythmias in a rare case. Catheter ablation might be an effective therapeutic option for a patient with symptomatic and drug‐refractory coughing‐induced atrial tachyarrhythmias.
Conflict of interest
None declared.
Authorship
XW, ZL, and JW: contributed to the preparation and submission of the manuscript. BH: contributed to the review of the manuscript.
Clinical Case Reports 2017; 5(12): 2133–2135
References
- 1. Tada, H. , Kaseno K., Kubota S., Naito S., Yokokawa M., Hiramatsu S., et al. 2007. Swallowing‐induced atrial tachyarrhythmias: prevalence, characteristics, and the results of the radiofrequency catheter ablation. Pacing Clin. Electrophysiol. 30:1224–1232. [DOI] [PubMed] [Google Scholar]
- 2. Omori, I. , Yamada C., Inoue D., Katsume H., and Ijichi H.. 1984. Tachyarrhythmia provoked by coughing and other stimuli. Chest 86:797–799. [DOI] [PubMed] [Google Scholar]