

Key Clinical Message
Tumor lysis syndrome (TLS) occurs when tumor cells release their contents into the bloodstream, typically in response to chemotherapy, leading to the characteristic findings of hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia, and acute kidney injury. Twinkle artifacts on renal ultrasound may indicate calcium phosphate deposits in such patients.
Keywords: Hyperphosphatemia, hyperuricemia, renal ultrasound, tumor lysis syndrome
Case Description
A 51‐year‐old woman with history of chronic lymphocytic leukemia (CLL) and hypertension was admitted for acute kidney injury. She received the first cycle of chemotherapy a week ago, which consisted of Fludarabine and Cyclophosphamide. She was not taking her allopurinol and not able to stay hydrated because of vomiting. Her serum creatinine at presentation was 12.3 mg/dL and was hypervolemic. In response to chemotherapy, the WBC count has dropped from 165,000/mm3 a month ago to 3,500. Rest of the laboratory values were significant for a serum potassium of 7.8 mmol/L (3.4–5.1), bicarbonate 8 mmol/L (22–30), calcium 6.2 mg/dL (8–10.6), uric acid 34.6 mg/dL (2.6–6.8), phosphate 32 mg/dL (2.7–4.5), and serum lactate dehydrogenase of 804 U/L (135–225), suggestive of TLS 1. Such degree of hyperphosphatemia and hyperuricemia was never reported before to the best of author's knowledge.
Renal ultrasound images revealed twinkle artifacts on color Doppler without visible stones on gray scale images, which possibly represent calcium phosphate deposits (Fig. 1, arrows). Twinkle artifact occurs behind a strongly reflecting granular interface such as urinary tract stones or parenchymal calcification and appears as a rapidly fluctuating mixture of Doppler signals (red and blue pixels) that imitate turbulent flow 2. The patient improved with hemodialysis.
Figure 1.
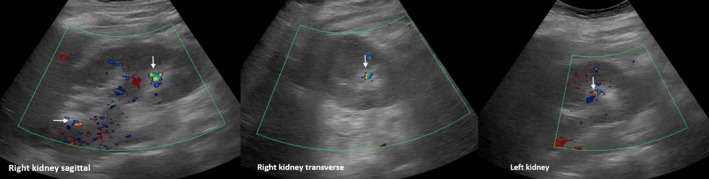
Renal ultrasound images with Doppler demonstrating twinkle artifacts (arrows).
Informed Consent
Informed consent has been obtained for the publication of this clinical image.
Authorship
The author has made substantial contribution to the preparation of this manuscript.
Conflict of Interest
The author has declared that no conflict of interest exists.
Clinical Case Reports 2017; 5(12): 2158–2159
References
- 1. Koratala, A. , Singhania G., Alquadan K. F., Shimada M., Johnson R. J., and Ejaz A. A.. 2016. Serum uric acid exhibits inverse relationship with estimated glomerular filtration rate. Nephron 134:231–237. [DOI] [PubMed] [Google Scholar]
- 2. Campbell, S. C. , Cullinan J. A., and Rubens D. J.. 2004. Slow flow or no flow? Color and power Doppler US pitfalls in the abdomen and pelvis. Radiographics 24:497–506. [DOI] [PubMed] [Google Scholar]