

Abstract
PET/CT imaging is frequently utilized for cancer diagnosis and re-staging as metabolically active cells, including cancer, utilize glucose for proliferation. 18F-FDG is the most commonly utilized radiopharmaceutical in PET/CT imaging. Limitations of 18F-FDG imaging include intense physiologic uptake in benign tissues such as the brain and myocardium. We present a case of non-small cell lung cancer with myocardial and pericardial metastases obscured by physiologic 18F-FDG cardiac uptake but detected with the investigational PET radiotracer (4S)-4-(3-(18)F-fluoropropyl)-l-glutamate (18F-FSPG), which targets glutaminolysis, an alternative energy pathway for proliferation. This case demonstrates the added value of 18F-FSPG PET/CT imaging.
Keywords: lung cancer, glutaminolysis, PET/CT, lung nodule
Figure 1.
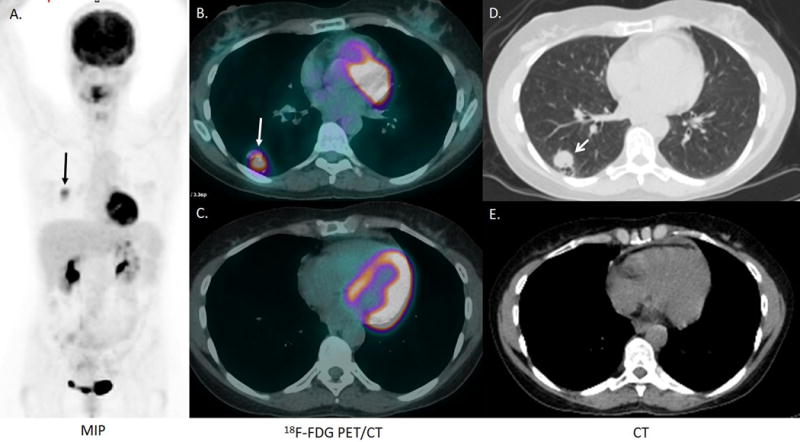
A 54-year-old woman with a history of stage IV non-small cell lung adenocarcinoma, metastatic to the mediastinum and brain, was previously treated with chemoradiation with 4 cycles of carboplatin, paclitaxel, and bevacizumab, radiation and stereotactic radiosurgery to all metastatic brain sites was in remission for 5 years. A surveillance chest CT revealed a 2.0 × 1.6 cm right lower lobe indeterminate pulmonary nodule (not shown). 18F-FDG PET/CT was performed 73 minutes after the intravenous injection of 395.9, MBq (10.7 mCi) of 18F-FDG. The MIP image (A) and the fusion and CT images (B, C) demonstrate intense FDG uptake in the 2.0 × 1.6 cm right lower lobe nodule, and physiologic intense FDG uptake in the brain and myocardium (A, B, C). Intense FDG uptake was also detected in a 1.4 × 1.5 cm left adrenal nodule and 1.7 × 2.5 cm proximal right thigh soft tissue nodule (not shown). A brain MRI demonstrated no significant changes in the appearance of the treated brain metastases, and no new brain metastases (not shown). Pathology from an excisional biopsy of the right thigh nodule revealed metastatic sarcomatoid carcinoma most compatible with a lung primary. Immunohistochemical stains demonstrated that the tumor cells were diffusely and strongly positive for cytokeratins (AE1/AE3 and CAM 5.2), while negative for S100, muscle-specific actin, smooth muscle actin, h-caldesmon, and myogenin. Genetic analysis of the tumor revealed a KRAS mutation and a BRAF V600L mutation.
Figure 2.
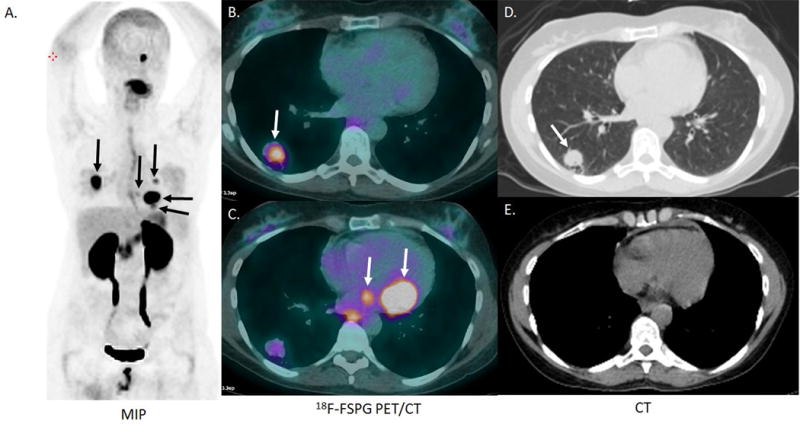
18F-FSPG imaging was subsequently performed as part of a clinical trial (NCT02448225), with local IRB approval and after informed consent. 18F-FSPG PET/CT was performed 62 minutes after the intravenous administration of 300.8 MBq (8.13 mCi) 18F-FSPG. Other than surgical excision of the right thigh metastasis, there was no intervening treatment in the 34 days between the 18F-FDG and 18F-FSPG PET/CT scans. The MIP image shows low physiologic uptake of 18F-FSPG within the brain and heart (A). The 18F-FSPG PET/CT images demonstrate intense uptake in the right lower lobe lung nodule (A, B, C, D) and left adrenal metastases seen with 18F-FDG (not shown). This examination also revealed multiple intensely FDG avid cardiac metastatic lesions (A, C) and one metabolically active brain metastasis (A), which were not detected with 18F-FDG PET/CT imaging. The patient had no symptoms related to these unsuspected cardiac and pericardial lesions.
Figure 3.
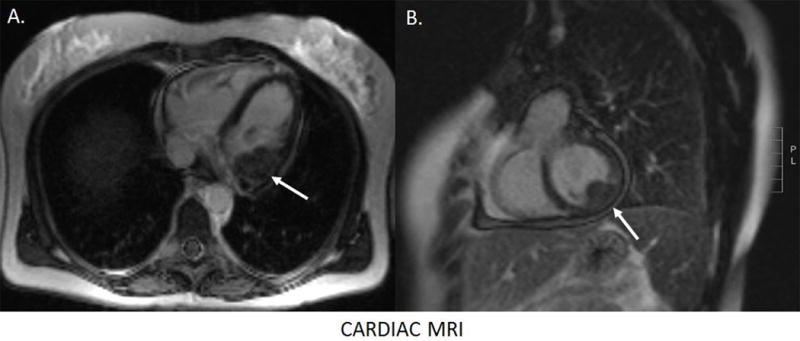
Subsequently, a cardiac MRI with contrast was performed. Multiple cardiac metastatic lesions were identified, the largest in the basal inferolateral left ventricular wall (A, B). The patient’s tumor progressed through treatment with Docetaxel and Gemcitabine with enlargement of the myocardial metastasis and development of a pericardial effusion. The patient developed complete heart block and decided to forego pacemaker implantation, passing away from metastatic lung cancer 6 months after the diagnosis of the cardiac metastases by 18F-FSPG PET/CT. This case highlights the unique advantage of 18F-FSPG PET/CT in tumor imaging. 18F-FSPG is taken up by metabolically active cells via the xC− cystine/glutamate antiporter.1–4 18F-FSPG has a more favorable biodistribution profile than 18F-FDG for detecting malignancy in the liver, bowel, myocardium and brain.5–8 Further investigations in the use of 18F-FSPG in lung cancer and other malignancies are needed to further establish the sensitivity and specificity as well as the role of 18F-FSPG PET/CT in clinical imaging.8–9
Acknowledgments
Funding Information: Institutional support from the Department of Radiology and Radiological Sciences, Vanderbilt University Medical Center, Nashville, TN, and from Piramal Life Sciences, Mumbai, India
Footnotes
Conflicts of Interest: All authors report no personal conflicts of interest
Prior publications or abstract presentations: None
All figures are original and not previously published.
References
- 1.Koglin N, Mueller A, Berndt M, et al. Specific PET imaging of xC-transporter activity using a (1)(8)F-labeled glutamate derivative reveals a dominant pathway in tumor metabolism. Clin Cancer Res. 2011;17:6000–6011. doi: 10.1158/1078-0432.CCR-11-0687. [DOI] [PubMed] [Google Scholar]
- 2.Baek S, Choi CM, Ahn SH, et al. Exploratory clinical trial of (4S)-4-(3-[18F]fluoropropyl)-L-glutamate for imaging xC-transporter using positron emission tomography in patients with non-small cell lung or breast cancer. Clin Cancer Res. 2012;18:5427–5437. doi: 10.1158/1078-0432.CCR-12-0214. [DOI] [PubMed] [Google Scholar]
- 3.Mosci C, Kumar M, Smolarz K, et al. Characterization of Physiologic (18)F FSPG Uptake in Healthy Volunteers. Radiology. 2016;279:898–905. doi: 10.1148/radiol.2015142000. [DOI] [PubMed] [Google Scholar]
- 4.Krasikova RN, Kuznetsova OF, Fedorova OS, et al. 4-[(18)F]Fluoroglutamic acid (BAY 85-8050), a new amino acid radiotracer for PET imaging of tumors: synthesis and in vitro characterization. J Med Chem. 2011;54:406–10. doi: 10.1021/jm101068q. [DOI] [PubMed] [Google Scholar]
- 5.Kavanaugh G, Williams J, Morris AS, et al. Utility of [18F]FSPG PET to Image Hepatocellular Carcinoma: First Clinical Evaluation in a US Population. Mol Imaging Biol. 2016;18:924–934. doi: 10.1007/s11307-016-1007-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Smolarz K, Krause BJ, Graner FP, et al. (S)-4-(3-18F-fluoropropyl)-L-glutamic acid: an 18F-labeled tumor-specific probe for PET/CT imaging–dosimetry. J Nucl Med. 2013;54:861–866. doi: 10.2967/jnumed.112.112581. [DOI] [PubMed] [Google Scholar]
- 7.Shreve PD, Anzai Y, Wahl RL. Pitfalls in oncologic diagnosis with FDG PET imaging: physiologic and benign variants. RadioGraphics. 1999;19:61–77. doi: 10.1148/radiographics.19.1.g99ja0761. [DOI] [PubMed] [Google Scholar]
- 8.Krause BJ, Smolarz K, Graner FP, et al. [18F]BAY 85-8050 (TIM-1): a novel tumor specific probe for PET/CT imaging - First clinical results. J Nucl Med. 2010;51(Suppl 2):118. [Google Scholar]
- 9.Chae SY, Choi C, Shim T. Exploratory Clinical Investigation of (4S)-4-(3-18F-Fluoropropyl)-L-Glutamate PET of Inflammatory and Infectious Lesions. J Nuc Med. 2016;57:67–69. doi: 10.2967/jnumed.115.164020. [DOI] [PubMed] [Google Scholar]