

Abstract
Aims:
The aim of this study is to compare clinical features of sphenofrontal craniosynostosis (SFC) and unilateral coronary craniosynostosis.
Settings and Design:
This was a retrospective study with two groups of patients with sphenofrontal and coronary craniosynostosis.
Materials and Methods:
This was a retrospective study of the 1999–2016 archive data in Russian Children's Clinical Hospital. Ninety-five patients were diagnosed with frontal plagiocephaly. Eighty-three had deformations of unilateral craniosynostosis of coronary suture, 12 had premature closures of sphenofrontal suture. The age at the time of diagnosis varied from 5 months to 2, 5 years.
Results:
SFC is featured by ipsilateral flattening of forehead and supraorbital margin, and ipsilateral dystopia of supraorbital margin downward. X-ray signs are the closure of sphenofrontal suture on the lesion side with open and symmetrically located remaining skull sutures and contralateral deviation of the midline of the ethmoid.
Conclusions:
SFC distinguishes from other plagiocephalias by following signs: supraorbital margin on the affected side is shifted downward; tip of the nose is displaced toward the affected side, root of the nose toward the healthy side. These signs facilitate correct diagnosis and treatment tactics.
Keywords: Craniosynostosis, frontal plagiocephaly, sphenofrontal craniosynostosis, unicoronary craniosynostosis
INTRODUCTION
Sphenofrontal craniosynostosis (SFC) is a new form of premature closure of the skull suture. The first description of the clinical picture of SFC was published in 1995 by Francel et al.[1] Over the past 20 years, a little over 20 cases were described in the literature. It indicates to an extreme rarity of the isolated closure of the sphenofrontal suture and probably explains frequent errors of diagnosis that occur during the initial examination of such patients.[2,3,4] This work aimed to identify the most vivid and persistent clinical and radiologic signs of SFC that differentiate it from other cases of asymmetric sinostosis deformities of the skull. We analyzed all cases described in English publications and compared the findings with SFC symptoms in 12 patients that we observed personally. The results of the research are presented in this paper.
MATERIALS AND METHODS
Study group
We conducted a retrospective study of the 1999–2016 archive data of the department of craniomaxillofacial surgery in Russian Children's Clinical Hospital (RCCH). Over the indicated period, we observed 520 patients with various forms of craniosynostosis. Ninety-five patients were diagnosed with frontal plagiocephaly. Eighty-three patients had deformations of unilateral craniosynostosis of the coronary suture, and 12 were diagnosed with premature closures of the sphenofrontal suture. The latter cases were observed in eight boys and four girls. Left and right lesions had the same frequency 6:6. The age of children at the time of diagnosis varied from 5 months to 2, 5 years.
Inspection report
According to RCCH craniosynostosis treatment protocol, in addition to clinical examination and evaluation of general medical indicators, neurologist, and ophthalmologist examined all patients. They looked for signs of intracranial hypertension and visual impairments associated with deformation of the orbit. All patients were mandatory photographed before and after the operation, as well as during all follow-up visits. The photos were taken in standard positions: front, left and right side, submental (from the bottom of the chin upward), and axially (from the arch of the skull downward). All patients underwent computed tomography with an interval of not >0, 6 mm, and mandatory capture of the entire skull and facial bones for subsequent three-dimensional (3D) reconstruction.
Selection of data for analysis
During our study, we analyzed all available data from patient examination including obstetric history, pediatric, neurological, and ophthalmological status. Particular attention was paid to the analysis of clinical and radiographic signs of deformation.
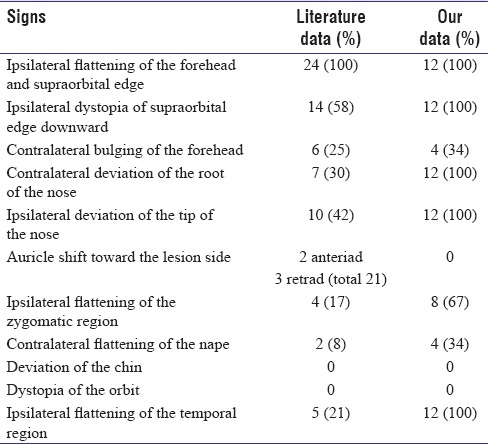
Analysis of publication revealed most frequently mentioned clinical signs of SFC such as, ipsilateral flattening of the forehead and the supraorbital margin; ipsilateral dystopia of the supraorbital margin downward (among the sign of this symptom were eyebrow drooping, ptosis, displacement of the inner canthal ligament downward, and displacement of the lateral canthal ligament upward); contralateral forehead bulging; contralateral deviation of the root of the nose; ipsilateral deviation of the tip of the nose; ipsilateral displacement of the ear posteriorly or anteriorly; flattening of the occiput; orbit dystopia; deviation of the chin; ipsilateral flattening of the zygomatic area; and ipsilateral flattening of the temporal area.
The same analysis was carried out for X-ray signs based on computed tomography data. We outlined following symptoms from publications: isolated synostosis of the sphenofrontal suture on the flattening side, open coronary, lambdoid and sagittal suture of the skull, deformation of the harlequin, and contralateral deviation of the midline of the anterior cranial fossa. All available data from publications and our own observations are presented in Table 1 for comparison.
Table 1.
Clinical (external, obtained by examination) signs of sphenofrontal craniosynostosis
Incidence
Based on the cases of craniosynostosis and frontal plagiocephaly, observed in RCCH since 1999, we estimated the incidence of isolated SFC as 1:43 among all cases of synostosis, and 1:8 among cases of frontal plagiocephaly. Approximate birth rate of patients with SFC amounts to 1:107500 provided that average birth rate of patients with craniosynostosis is 1:2500.[5] A slightly higher frequency of SFC can be obtained by analyzing the data on the incidence of hemicoronary synostosis. Given that the birth rate of children with hemicoronary synostosis is 1:10000,[6] birth rate for children with SFC equals to 1:80000. The average arithmetic of the ratios above makes it possible to estimate the birth rate of children with sphenofrontal synostosis at approximately 1 case/94000 newborns.
Gender and side
The predominance of males in SFC cases corresponds to data presented in publications. 18 cases out of 24 described had indication of gender: 5 patients were girl and 13 were boy. Based on all the cases described in publications up to the present date and our observations, we can assume that the ratio of boys to girls is approximately 1:2.
We did reveal any difference in the side of the lesion, but among the previously described 24 cases, 10 patients had left-sided synostosis and 14 had a right-sided one. Aggregation of data in publications and our experience allows us to state predominance of right-handed forms over left-handed ones with a frequency of 1:1, 25.
Symptoms and features
Uncomplicated obstetrical history was noted in all 12 cases. Analysis of general, neurological, and ophthalmological examinations did not reveal any signs of intracranial hypertension, as well as visual organs and its adnexa dysfunction.
Analysis of the clinical signs of deformity of our patients and those described in publications showed that the ipsilateral flattening of the forehead and the supraorbital margin and the ipsilateral dystopia of the supraorbital margin downward are distinctive and thus absolute signs of isolated SFC. Signs such as contralateral root deviation and ipsilateral deviation of the tip of the nose were noted by several but not all authors. Thorough study of our own group revealed these signs, as well as flattening of the temporal region on the side of the lesion in all our patients. Furthermore, more than half of our patients had flattening of the zygomatic area on the affected side (67%). The contralateral frontal region bulging and flattening of the occiput was noted only in 34% of our patients, and we did not find such deformations as orbital dystopia, chin deviation, and anterior or posterior auricle displacement [Table 1].
The most distinctive X-ray signs of SFC described in publications and observed in our patients were (a) the closure of the sphenofrontal suture on the side of the lesion with open and symmetrically located other sutures of the skull; (b) contralateral deviation of the midline of the ethmoid. In none of the observations, “deformation of the Harlequin” was noted [Table 2].
Table 2.
Radiological signs of sphenofrontal craniosynostosis

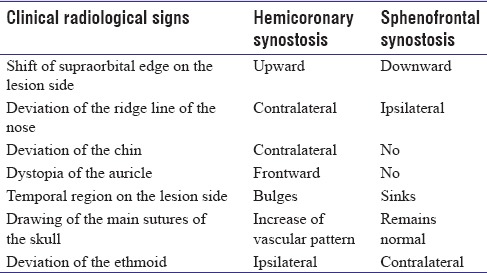
There is no doubt that these features make it easy to differentiate SFC from hemicoronary craniosynostosis based only on close examination. Computed tomography data easily confirm the initial diagnosis [Figure 1 and Table 3].
Figure 1.

Differential diagnosis of hemicoronary synostosis and sphenofrontal synostosis. Left column (a,c,e and g): frontal and downward view, 3-D reconstruction of skull of the patient with isolated right-sided sphenofrontal craniosynostosis. Right column (b,d,f and h): frontal and downward view, 3-D reconstruction of skull of the patient with right-sided coronary synostosis
Table 3.
Differential diagnosis of hemicoronary and sphenofrontal craniosynostosis
DISCUSSION
Accumulated clinical experience and advance in X-ray diagnostics showed that craniosynostosis of the coronary or labdoid suture are not the only reasons for asymmetric skull deformations. Descriptions of plagiocephaly associated with the closure of other cranial sutures have appeared.[7,8,9,10] One of these cases is recently discovered SFC,– the result of premature closure of the frontowedge-shaped suture. The first case of frontal plagiocephaly conditioned by SFC was described in 1995 by Francel et al.[1] Following them, similar condition of craniosynostosis was described successively in 23 patients.[2,3,4,11,12,13,14,15,16]
At present, SFC is described in detail, and the clinical picture is determined to such extent that diagnosis can be made on the basis of a single examination of the patient. A logical question arises, why craniosynostosis presenting such an obvious deformation was not described until 1995. One of the possible explanations is the rarity of this condition of craniosynostosis, which did not allow accumulating sufficient experience necessary to distinguish SFC from the group of frontal plagiocephalias. The second, more obvious reason, lies in the imperfection of X-ray diagnostics. It was almost impossible to determine the true cause of deformation before the development of the CT method. The work of Currarino[17] can serve proof. The author described two cases of plagiocephaly, which he explained by the closure of the zygomatic frontal suture. Curriano based his work on the study of radiographs of the skull in standard projections. For one patient, an intraoperative description of the clotting area was available. The author noted the narrowing of the sphenofrontal suture on the side of the lesion. However, the detailed study of the X-ray diffraction patterns presented by the author, and the analysis of the clinical signs of deformity (in the presented photos), points to SFC. Even in the fundamental work of Tessier, devoted to craniosynostosis,[18] there is an illustration of a patient number 5 with the indicative for SFC flattening of the fronto-orbital region and the dystopia of the supraorbital margin downward. In this case, the deformation is mistakenly explained by unilateral closure of the coronary suture. Ehret[19] has an illustrative confirmation (photo number 6) that this type of asymmetry could be misinterpreted as deformational (nonsynostotic) frontal plagiocephaly.
Thus, the main signs of SFC that distinguish it from other plagiocephalies are as follows: supraorbital margin on the affected side is shifted downward, the nose deviation is insignificant, and always manifests itself in the form of displacement of the tip of the nose toward the affected side, and the root of the nose toward the healthy side. Patients do not have compensatory bulging of the temporal region on the side of the lesion, as they do in cases of hemicoronal synostosis. On the contrary, flattening of the forehead seems to smoothly turn into a flattening of the temporal region, thus increasing the visual distance between the auricle and the outer edge of the orbit on the affected side. It is probably this effect that allowed some authors to believe that the auricle is displaced posteriorly.[2,15] We cannot explain why other researchers noted the displacement of the auricle anteriorly,[4] as well as we cannot confirm it based on the photographs presented by authors. A slight flattening of the occiput on the healthy side, discovered in some patients, is most likely a consequence of compensatory changes.
Different authors provide various explanation of deformation in patients with SFC. Based on the law of Virchow, Francel et al. concluded that sphenofrontal synostosis, as well as hemicoronary synostosis, damages the ventral enlargement of the anterior cranial fossa. This leads to its compression (shortening) and as a consequence, to the recession of the supraorbital margin with flattening of the forehead. In such conditions, the growth vector of the frontal lobe is redirected upward and contralateral. The upward pressure of the growing brain leads to an increase in the height of the forehead, whereas downward pressure causes deformation of the adjacent middle cranial fossa, manifesting itself in the ventral expansion of the large wing of the sphenoid bone.[1] However, we did not observe neither an increase in the height of the forehead on the affected side nor the ventral expansion of the large wing of the sphenoid bone in patients with SFC. All described changes fully correspond only to hemicoronary synostosis. Furthermore, the authors do not explain the reason for the dystopia of the supraorbital margin downward, and the contralateral deviation of the midline of the ethmoid, which clearly distinguish SFC from hemicoronary craniosynostosis.
Rogers et al. believe that the simple application of the Virchow law to this case of synostosis is challenging. The authors explain deformations with theory of the “coronary ring,” which considers the parietal-frontal (coronary) suture, the sphenofrontal suture and the sphenoethmoidal suture on each side as a single semicircle, and consequently consider both semicircles as a coronary ring, which is a single functional system for the skull bones growth. Based on this theory, the authors state that the synostosis that arises at any point of the coronary ring disrupts growth in all the sutures along its axis within the ipsilateral hemisphere. Thus, the closure of the sphenofrontal suture leads to deceleration of growth in the entire ipsilateral half of the coronary ring. Accordingly, even remaining open, the parietal frontal suture functions poorly, which results in flattening of the forehead, whereas restriction of growth in the open frontoethmoidal and sphenoethmoidal sutures leads to compensatory unilateral anteroposterior shortening of the frontal bone and “coronary” expansion of the ethmoid bone. Thus, the ethmoid bone unfolds contralaterally, from behind frontward, as a result of the difference in the size of the joints located on both sides of the ethmoid. A slight anteroposterior shortening of the temporal portion of the sphenoid bone was attributed to a possible growth disturbance in the region of the zygomaticosphenoidal suture, which, in fact, is a continuation of the coronary ring.[2] Certainly, this theory does not explain the displacement of the upper edge of the orbit downward.
Mathijssen et al. explained deformation by the features of the embryonic development of the cranial sutures. The authors drew attention to the fact that the synostosis of the sphenofrontal suture begins in the uppermost angle of the eye, in the same place, where the primary closure of the frontal and sphenoid bones normally occurs. The synostosis continues in accordance with the normal seam formation vector. Early closure leads to limiting the growth of the roof of the orbit anteriorly and upward and is expressed in limiting the distances of the supraorbital margin and shifting it downward. The authors attributed relatively mild manifestations of deformation in SFC (compared to hemicoronary synostosis) to different time of physiological closure and accordingly, the time of possible synostosis of sphenofrontal (21 weeks of gestation) and coronary (16 weeks of gestation) cranial sutures.[14]
We believe that all the signs of the SFC can be explained by the Virchow law, applied to the 3D space. For a better understanding of the occurring changes, it is worth refreshing memory on some features of the development and structure of the sphenofrontal suture (ideally with anatomical atlas and a native skull preparation – dry skull). The sphenofrontal suture consists of two parts: the medial and the lateral. The medial part is straight, almost horizontal and connects the small wing of sphenoid bone with the frontal bone. Anatomically, it is part of the anterior cranial fossa. The suture axis extends in the mediolateral direction and is parallel to the line drawn from the outer edge of the orbit to the hypophyseal fossa of sphenoid. The surface of the joint (or suture plane) is represented by a thin band corresponding to the frontal plane, which provides growth of the roof of the orbit frontward.
The lateral part of the sphenofrontal suture is in the middle cranial fossa. This part is more massive than the medial one and has more complex shape. The surface of the closing of the large wing of the sphenoid and frontal bones is represented by a platform consisting of two unequal fragments connected together in L-shape. The vertical axis of this shape is located in the front, and its horizontal axis corresponds to the line drawn from the outer edge of the orbit to the hypophyseal fossa of sphenoid. The plane of connection of this area is mainly front-oriented. However, compared to the medial part of the sphenofrontal suture, the plane is located with a slight slanting backward, that is, facing frontward, outward, and upward. Thus, a small fragment of the lateral part of the seam provides an increase in the uppermost angle of the orbit, mainly frontward and slightly outward and upward.
The medial and lateral parts of the suture differ not only anatomically but also by embryonic development. The medial part connects the bones of the endochondral and membranous types of ossification, which makes it chondral-branched joint. The lateral part is a genuine membranous joint between the bones with the membrane type of development.[12] This anatomical and embryonic heterogeneity of the two parts of the sphenofrontal suture makes them two different sutures: medial and lateral sphenofrontal sutures.
Certainly, there is no mention of the extent of premature synostosis of the sphenofrontal suture in publication. Based on our data, we could not clearly determine whether both sutures are closed or only the lateral part. However, there are signs that in cases of bilateral closure of the coronary ring sutures, with the primary lesion of its basilar part, upper micrognathia develops (like in syndromes of Aper, Cruson, and Pfeiffer).[20] On the contrary, cases of nonsyndrome unilateral coronary craniosynostosis with simultaneous closure of the sphenofrontal suture show no signs of middle-face area underdevelopment.[21] This may indicate that in isolated hemicoronary synostosis, the normal structure of the medial part of the sphenofrontal suture and sphenoethmoid synhondrosis[2] remains. Based on the presented observations, we assume that the medial and lateral parts of the sphenofrontal suture can be included in the pathological process independently, which also confirms their heterogeneity.
Now let us discuss the deformation caused by isolated SFC. Undoubtedly, the main part in its formation belongs to the lateral area of the sphenofrontal suture. Its synostosis limits the growth of the upper-lateral edge of the orbit to the top, outward, and frontward, causing the main signs of synostosis, such as the descent of the roof of the orbit, the flattening of the supraorbital region, frontal and temporal areas (which are adjacent to each other at this point). In accordance with Virchow's law, compensation of growth should occur in area parallel to the line of closed suture. In our case, the suture is curvilinear, thus the compensatory changes are more complicated than the standard linear closure. The disruption of the growth of the supraorbital margin outward can be compensated by the open medial part of the sphenofrontal suture and the frontoetmoidal suture on the side of the lesion. The compensatory growth along the line of these sutures explains the contralateral deviation of the ethmoid bone and the deviation of its midline to a healthy side. Growth disorder of the upper margin of the orbit frontward is compensated by growth along the open parietal-temporal and sphenoidal-temporal sutures. This compensatory mechanism makes it possible to maintain the anterior-posterior size of the middle cranial fossa within normal limits and even with a slight elongation backward. Growth along the lines of these seams explains why distance from the outer edge of the orbit to the auditory aperture remains normal and does not decrease in proportion to the shortening of the greater part of the lateral fragment of the sphenofrontal suture. The growth disorder of the orbit roof upward is easily compensated by the growth of the frontal bone along the open coronary suture, which explains remaining symmetry of the large fontanel. Thus, as a result of the described changes, the anteroposterior flattening, mediolateral expansion, and deepening of the anterior cranial fossa on the side of the lesion develops. Compensatory changes of the middle cranial fossa on the side of the lesion are insignificant and are represented by anteroposterior elongation. That is, the compensation of growth occurs mainly due to changes in the anterior and middle cranial fossa on the side of the lesion. This radically distinguishes SFC from a coronary synostosis, in which compensation occurs mainly by deepening the middle cranial fossa on the side of the lesion and widening the anterior cranial fovea on the opposite side.
CONCLUSIONS
SFC has highly typical clinical picture, which allows distinguishing it from the group of synostotic plagiocephaly with high accuracy. Knowledge of key external signs of SFC, such as the dystopia of the supraorbital margin downward and deviation of the tip of the nose toward the affected side, and the root of the nose to the healthy side will help to avoid diagnostic errors leading to incorrect treatment tactics.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Francel PC, Park TS, Marsh JL, Kaufman BA. Frontal plagiocephaly secondary to synostosis of the frontosphenoidal suture. Case report. J Neurosurg. 1995;83:733–6. doi: 10.3171/jns.1995.83.4.0733. [DOI] [PubMed] [Google Scholar]
- 2.Rogers GF, Proctor MR, Mulliken JB. Unilateral fusion of the frontosphenoidal suture: A rare cause of synostotic frontal plagiocephaly. Plast Reconstr Surg. 2002;110:1011–21. doi: 10.1097/01.PRS.0000021308.37931.18. [DOI] [PubMed] [Google Scholar]
- 3.Plooij JM, Verhamme Y, Bergé SJ, van Lindert EJ, Borstlap-Engels VM, Borstlap WA, et al. Unilateral craniosynostosis of the frontosphenoidal suture: A case report and a review of literature. J Craniomaxillofac Surg. 2009;37:162–6. doi: 10.1016/j.jcms.2008.10.005. [DOI] [PubMed] [Google Scholar]
- 4.Sauerhammer TM, Oh AK, Boyajian M, Magge SN, Myseros JS, Keating RF, et al. Isolated frontosphenoidal synostosis: A rare cause of synostotic frontal plagiocephaly. J Neurosurg Pediatr. 2014;13:553–8. doi: 10.3171/2014.1.PEDS1378. [DOI] [PubMed] [Google Scholar]
- 5.Persing JA. MOC-PS(SM) CME article: Management considerations in the treatment of craniosynostosis. Plast Reconstr Surg. 2008;121:1–1. doi: 10.1097/01.prs.0000305929.40363.bf. [DOI] [PubMed] [Google Scholar]
- 6.Bruneteau RJ, Mulliken JB. Frontal plagiocephaly: Synostotic, compensational, or deformational. Plast Reconstr Surg. 1992;89:21–31. [PubMed] [Google Scholar]
- 7.Sze RW, Hopper RA, Ghioni V, Gruss JS, Ellenbogen RG, King D, et al. MDCT diagnosis of the child with posterior plagiocephaly. AJR Am J Roentgenol. 2005;185:1342–6. doi: 10.2214/AJR.04.1388. [DOI] [PubMed] [Google Scholar]
- 8.Schmelzer RE, Fearon JA. ‘Z-pattern’ craniosynostosis: A novel presentation of trisutural fusion. J Craniofac Surg. 2007;18:568–74. doi: 10.1097/scs.0b013e318052feee. [DOI] [PubMed] [Google Scholar]
- 9.Sauerhammer TM, Patel K, Oh AK, Proctor MR, Mulliken JB, Rogers GF, et al. Combined metopic and unilateral coronal synostoses: A phenotypic conundrum. J Craniofac Surg. 2014;25:437–40. doi: 10.1097/01.scs.0000436674.59196.cd. [DOI] [PubMed] [Google Scholar]
- 10.Jimenez DF, Barone CM, Argamaso RV, Goodrich JT, Shprintzen RJ. Asterion region synostosis. Cleft Palate Craniofac J. 1994;31:136–41. doi: 10.1597/1545-1569_1994_031_0136_ars_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 11.Dundulis JA, Becker DB, Govier DP, Marsh JL, Kane AA. Coronal ring involvement in patients treated for unilateral coronal craniosynostosis. Plast Reconstr Surg. 2004;114:1695–703. doi: 10.1097/01.prs.0000142474.25114.cb. [DOI] [PubMed] [Google Scholar]
- 12.de Ribaupierre S, Czorny A, Pittet B, Jacques B, Rilliet B. Frontosphenoidal synostosis: A rare cause of unilateral anterior plagiocephaly. Childs Nerv Syst. 2007;23:1431–8. doi: 10.1007/s00381-007-0469-4. [DOI] [PubMed] [Google Scholar]
- 13.Marucci DD, Jones BM, Dunaway DJ, Hayward RD. Unilateral isolated frontosphenoidal craniosynostosis causing frontal plagiocephaly. J Plast Reconstr Aesthet Surg. 2009;62:e255–8. doi: 10.1016/j.bjps.2007.12.016. [DOI] [PubMed] [Google Scholar]
- 14.Mathijssen IM, van der Meulen JJ, van Adrichem LN, Vaandrager JM, van der Hulst RR, Lequin MH, et al. The frontosphenoidal suture: Fetal development and phenotype of its synostosis. Pediatr Radiol. 2008;38:431–7. doi: 10.1007/s00247-008-0750-z. [DOI] [PubMed] [Google Scholar]
- 15.Pickrell BB, Lam SK, Monson LA. Isolated unilateral frontosphenoidal craniosynostosis: A Rare cause of anterior plagiocephaly. J Craniofac Surg. 2015;26:1944–6. doi: 10.1097/SCS.0000000000001950. [DOI] [PubMed] [Google Scholar]
- 16.Bot G, Leshem D, Shiran SI, Ben-Shachar S, Constantini S, Roth J, et al. Frontosphenoid synostosis: An unusual cause of anterior plagiocephaly. J Craniofac Surg. 2015;26:174–5. doi: 10.1097/SCS.0000000000001183. [DOI] [PubMed] [Google Scholar]
- 17.Currarino G. Premature closure of the frontozygomatic suture: Unusual frontoorbital dysplasia mimicking unilateral coronal synostosis. AJNR Am J Neuroradiol. 1985;6:643–6. [PMC free article] [PubMed] [Google Scholar]
- 18.Tessier P. Relationship of craniostenoses to craniofacial dysostoses, and to faciostenoses: A study with therapeutic implications. Plast Reconstr Surg. 1971;48:224–37. doi: 10.1097/00006534-197109000-00005. [DOI] [PubMed] [Google Scholar]
- 19.Ehret FW, Whelan MF, Ellenbogen RG, Cunningham ML, Gruss JS. Differential diagnosis of the trapezoid-shaped head. Cleft Palate Craniofac J. 2004;41:13–9. doi: 10.1597/02-053. [DOI] [PubMed] [Google Scholar]
- 20.Kreiborg S. Postnatal growth and development of the craniofacial complex in premature craniosynostosis. In: Cohen MM Jr, MacLean RF, editors. Craniosynostosis: Diagnosis, Evaluation, and Management. 2nd ed. New York: Oxford University Press; 2000. pp. 158–74. [Google Scholar]
- 21.Seeger JF, Gabrielsen TO. Premature closure of the frontosphenoidal suture in synostosis of the coronal suture. Radiology. 1971;101:631–5. doi: 10.1148/101.3.631. [DOI] [PubMed] [Google Scholar]