

Abstract
Purpose
This study investigated the expression of insulin-like growth factor binding protein-3 (IGFBP-3) in basal tears of patients with type 2 diabetes mellitus compared to nondiabetic controls; and correlated tear levels of IGFBP-3 with morphologic changes in the subbasal nerve plexus and density of basal corneal epithelial cells.
Methods
This was a single visit, cross-sectional study. Diabetic and control subjects were matched for age, sex, smoking status, and body mass index. Tear levels of IGFBP-3 were measured using ELISA. Corneal nerve and basal epithelial cell changes were measured using in vivo confocal microscopy.
Results
Tear levels of IGFBP-3 were 3.5-fold higher in those with diabetes. Patients with diabetes also showed a reduction in nerve fiber layer, nerve branch density, and corneal basal epithelial cell density. There was no significant difference in corneal sensitivity. IGFBP-3 levels were highly correlated with nerve fiber length and branch density; while hemoglobin (Hb)A1c was only moderately correlated. There were no significant differences in the clinical or subjective signs of dry eye between groups, indicating that tear levels of IGFBP-3 and corneal nerve changes were not due to the presence of mild dry eye.
Conclusions
These findings indicate that tear levels of IGFBP-3 are more tightly correlated to nerve fiber changes in diabetes than HbA1c. Future studies that stratify the severity of diabetic disease with tear levels of IGFBP-3 are needed to validate this finding.
Keywords: cornea, epithelium, IGFBP-3, subbasal nerve plexus, T2DM
The subbasal nerve plexus (SBNP) is located within the cornea between the basal epithelium and Bowman's layer.1 Early studies investigating the structure of the subbasal nerve plexus were all performed ex vivo using animal models or human cadaver tissue, introducing the possibility for fixation artifacts and postmortem degeneration of corneal nerve fibers.2–6 The introduction of in vivo corneal confocal microscopy (IVCM) introduced a novel, noninvasive way to study the normal subbasal nerve plexus and allowed, for the first time, the ability to monitor changes in the human cornea in disease states.7–11 As such, in vivo confocal microscopy is increasingly being used as a clinical tool to evaluate the corneal subbasal nerve plexus in patients with systemic disease, with a huge emphasis on corneal nerve loss in diabetes.12–16
A large number of studies have shown that corneal nerve fiber parameters such as nerve fiber length, nerve fiber density, nerve branch density, and tortuosity are altered in patients with type 2 diabetes mellitus (DM).14,17–24 More importantly, loss of the corneal subbasal nerve plexus has been shown to correlate with the severity of diabetic peripheral neuropathy and has been proposed as a surrogate marker for diabetic peripheral neuropathy, potentially eliminating the need for more invasive measurements such as skin punch biopsies and electrophysiologic testing.16,25,26 In support of this work, subsequent studies have shown that improvement in risk factors for diabetic complications, including diabetic peripheral neuropathy, corresponds to an improvement in the corneal subbasal nerve plexus through regeneration of corneal nerve fibers.27
In addition to changes in the subbasal nerve plexus, type 2 diabetes mellitus has also been found to be associated with dry eye and alterations in the tear film and the tear film proteome.28,29 Prior studies in our laboratory have shown that the insulin-like growth factor binding protein 3 (IGFBP-3), an N-linked glycosylated secretory protein, is elevated in the tear film in diabetes.30 IGFBP-3 is a pleiotropic protein that exerts antiproliferative effects through the binding of extracellular IGF-1, preventing IGF-1 binding to the IGF-1 receptor.31 IGFBP-3 has also been shown to have anti- and proapoptotic effects, which are tissue- and cell-type specific.32,33 In the tear film, the function of IGFBP-3 is unknown. Likewise, the source of IGFBP-3 has not yet been determined. Tears are a composite of lacrimal gland secretions, secreted proteins from corneal epithelial cells, and a derivative from blood via capillaries and small vessels across the ocular surface.34 Culture of corneal epithelial cells in high glucose media, however, suggests that corneal epithelial cells are responsible at least in part, for the high levels of IGFBP-3 present in diabetic tears.30
Based upon our prior data, we hypothesized that IGFBP-3 may correlate and represent a novel marker for severity of diabetic eye disease. In the present study, we examined the expression of IGFBP-3 in basal tears of patients with type 2 diabetes mellitus compared to nondiabetic controls. We then evaluated patients for clinical signs of dry eye and assessed corneal sensitivity and the morphology of the subbasal nerve plexus using remote controlled scanning in vivo confocal microscopy.
Materials and Methods
Study Design and Population
This was a single visit, cross-sectional, masked study designed to investigate tear levels of IGFBP-3 in relation to corneal nerve fiber morphology. This study adhered to the tenets of the Declaration of Helsinki. All study procedures were approved by the institutional review board at the University of Texas Southwestern Medical Center. All patients signed written informed consent before participating in this study. Patients were recruited through the Ophthalmology Clinic at the Aston Ambulatory Care Center at the University of Texas Southwestern Medical Center, Dallas, Texas, United States. Patients were placed into one of two groups according to their medical history: those with type 2 diabetes mellitus and nondiabetic controls. For inclusion in the diabetes group, a physician diagnosis was required. Normal controls consisted of healthy adults aged 18 years and older that were noncontact lens wearers or had no history of recent contact lens wear within the last year. For women who were not menopausal or had a negative medical history for tubal ligation or hysterectomy, a urine pregnancy test was performed to rule out possible pregnancy. Exclusion criteria for both diabetic and control groups included patients with a recent history of ocular surgery, trauma, use of topical glaucoma medications or other topical ophthalmic medications, contact lens wear, pregnancy or lactation, type 1 diabetes mellitus, respiratory disorders such as asthma or chronic obstructive pulmonary disease, end-stage renal disease, alcoholism, infectious disease, cancer, or any uncontrolled systemic disease that may adversely affect study results. For all outcome measures, the clinical investigator (DMR) was masked to the health status of the patient. Groups were matched for age, sex, obesity, and smoking status. Outcome measures included anthropometric measurements for the calculation of body mass index (BMI), and waist-to-height ratio. Each patient then underwent the following: serology testing, blood pressure measurement; a basic eye examination that included dry eye testing (described below); and a dilated fundus examination to check for the presence of diabetic retinopathy, tear collection, in vivo confocal microscopy assessment of corneal nerves, and measurement of corneal sensitivity. Patients were also asked to complete the Ocular Surface Disease Index (OSDI) questionnaire, a validated questionnaire to subjectively assess dry eye.
Assessment of the Cornea and Tear Film
The cornea and ocular surface were assessed by a single clinical examiner (DMR). A brief biomicroscopic examination of the lids, lashes, conjunctiva, and cornea was performed to rule out any existing corneal pathology. The cornea and ocular surface were evaluated for staining using fluorescein, and measures of tear film break-up time (TFBUT) and basal tear production were obtained. For the determination of TFBUT, 2 μL of 2.0% nonpreserved fluorescein (Greenpark Pharmacy, Houston, TX, USA) were instilled onto the superior bulbar conjunctiva. After three normal blinks, the time between the last blink and the first dark spot was timed using a stopwatch. Three readings were recorded with 30-second rest periods in between. For patients with a stable tear film that did not show signs of breakup, timing was truncated at 30 seconds. Immediately following the measurement of tear film break up time, the cornea was evaluated for fluorescein staining. Staining was graded according to the National Eye Institute scale for corneal staining in five regions using a scale of 0 to 3. For all fluorescein-based measurements, a Wratten #12 filter was used. As the last clinical test, basal tear production was assessed using a Schirmer's tear test without anesthesia. The Schirmer's strip was placed in the lower fornix near the lateral canthus and the subject was instructed to close their eyes. The length of the wetted area after 5 minutes was measured. All tests were performed for both eyes and the values for the right and left eyes were averaged to achieve a final measurement.
Tear Collection
Tear collection was performed as the first clinical test. Tears were collected from the temporal inferior tear meniscus on both eyes of each subject using 1 or 2 μL glass capillary tubes (Drummond, Fischer Scientific, Houston, TX, USA). The inferior tear meniscus was visualized using a slit lamp biomicroscope (Haag-Streit, Köniz, Switzerland) with low illumination. We collected 5 μL of minimally stimulated basal tear fluid from each eye. Care was taken to avoid touching the eye to minimize reflex tearing. Tears from each eye were pooled to reach a final volume of 10 μL. Samples were immediately placed on ice and then stored at –80°C until use. To control for diurnal fluctuations, all samples were collected between 8 AM and noon by a single trained investigator (DMR).
Corneal Sensitivity
After evaluation of the cornea and ocular surface, corneal sensitivity was measured in the right eye using an esthesiometer (Cochet-Bonnet esthesiometer; Luneau, Paris, France). The esthesiometer contained a 0.08-mm diameter nylon filament. The filament was used to applanate the inferior cornea approximately 2 mm above the inferior limbus. Initial measurements were performed with the filament fully extended to 6.0 mm. The filament length was systematically reduced in increments of 0.5 mm until the patient reported >2 of the 4 stimuli at one increment. False presentations were included to control for bias in patient response. All measurements were obtained by a trained investigator (DMR).
In Vivo Confocal Microscopy
In vivo confocal microscopy was performed using a modified HRT-RCM confocal microscope (Heidelberg Engineering, Heidelberg, Germany) to collect images of the corneal subbasal nerve plexus and the basal epithelium.35 The right eye of each patient was scanned. Prior to scanning, one drop of topical proparacaine (Alcon Laboratories, Ft. Worth, TX, USA) was instilled into both eyes. Eye gel (GenTeal; Alcon Laboratories) was applied to the confocal cap to optically couple the confocal tip to the cornea. Repeat scans were performed across the midperipheral and central cornea, moving from the superior temporal region toward the inferior nasal area. Scans were performed in real time while live streaming high-resolution images to an external hard drive. A remote control was used to adjust the focus of the objective and to continuously move the plane of focus back and forth through the cornea. Images of the subbasal nerve plexus were reconstructed in the laboratory to generate a minimum of eight nonoverlapping regions. Sequential image frames were stacked using microscopy automation and image analysis software (MetaMorph; Molecular Devices, Sunnyvale, CA, USA) and FIJI (provided in the public domain by the National Institutes of Health [NIH], Bethesda, MD, USA) to generate a maximum intensity projection to account for all nerves regardless of focal plane. This allowed for the generation of a single composite image (400 × 400 μm). Confocal images were then analyzed for determination of nerve fiber length, which is defined as the total length in μm of all the nerves in the 400 × 400 μm confocal microscopy image; and nerve branch density, defined as the total number of branch points per μm2 in the 400 × 400 μm confocal microscopy image. Corneal epithelial basal cell density, which is the total number of epithelial cells in the 400 × 400 μm confocal image, was also calculated. Quantification of nerve fiber length was measured by manually tracing the nerves within each image using image analysis software (Molecular Devices). Epithelial cell density was determined by manually counting the epithelial cells using the FIJI cell counter plugin.
Anthropometric Measurements
Neck, waist, and hip circumferences were measured using a standard seamstress tape measure. Waist circumference was measured at the midpoint between the lower palpable rib and the top of the iliac crest. Hip circumference was measured at the widest area of the buttocks. To rule-out effects of obesity between study groups, body mass index, was calculated based upon current height and weight, measured at the time of examination. Body mass index was classified as: underweight (≤18.5); normal (18.6–24.9); overweight (25.0–29.9); and obese (≥30.0).
Systemic Biomarkers
Phlebotomy was performed in nonfasted patients for assessment of systemic inflammatory and metabolic biomarkers. This included measurement of glycosylated hemoglobin (Hb)A1c, high-sensitivity C-reactive protein (hsCRP), and a lipid panel. Serology testing was performed at Quest Laboratories (Dallas, TX, USA). Systolic and diastolic blood pressure measurements were also obtained using an automated wrist sphygmomanometer.
ELISA
Human tear samples were assessed for the presence of insulin like growth factor binding protein 3 (IGFBP-3). A commercial kit (IGFBP-3 Quantikine ELISA kit; R&D Systems, Minneapolis, MN, USA) was used to determine tear concentration. We took 10 μL of pooled tear samples from both eyes of each patient and diluted 1:10 using calibrator diluent. The assay was performed according to manufacturer instructions. The samples were then read at an absorbance of 450 nm and compared against a standard curve of known concentrations. Concentrations of IGFBP-3 in tear samples were calculated and corrected by the dilution factor. Patients with IGFBP-3 levels outside the linear range of the standard were excluded.
Statistics
Statistical analysis was performed using commercial software (SigmaPlot 12.5; Systat Software, Inc., San Jose, CA, USA). A Shapiro-Wilk test was used to test whether the data was normally distributed. For data with a normal distribution, data are represented as mean ± standard deviation and the 95% confidence interval is presented. For analysis between two groups with a normal distribution, a Student's t-test was performed. For data with a nonnormal distribution, data are presented as the median with a range (min–max). Analysis between two groups with a nonnormal distribution used a Mann-Whitney rank sum test. For analysis between nominal variables, a χ2 was used. Linear regression analysis was performed to test for relationships between tear levels of IGFBP-3 and nerve fiber length, nerve branch density, and HbA1c. Statistical significance was set at P < 0.05.
Results
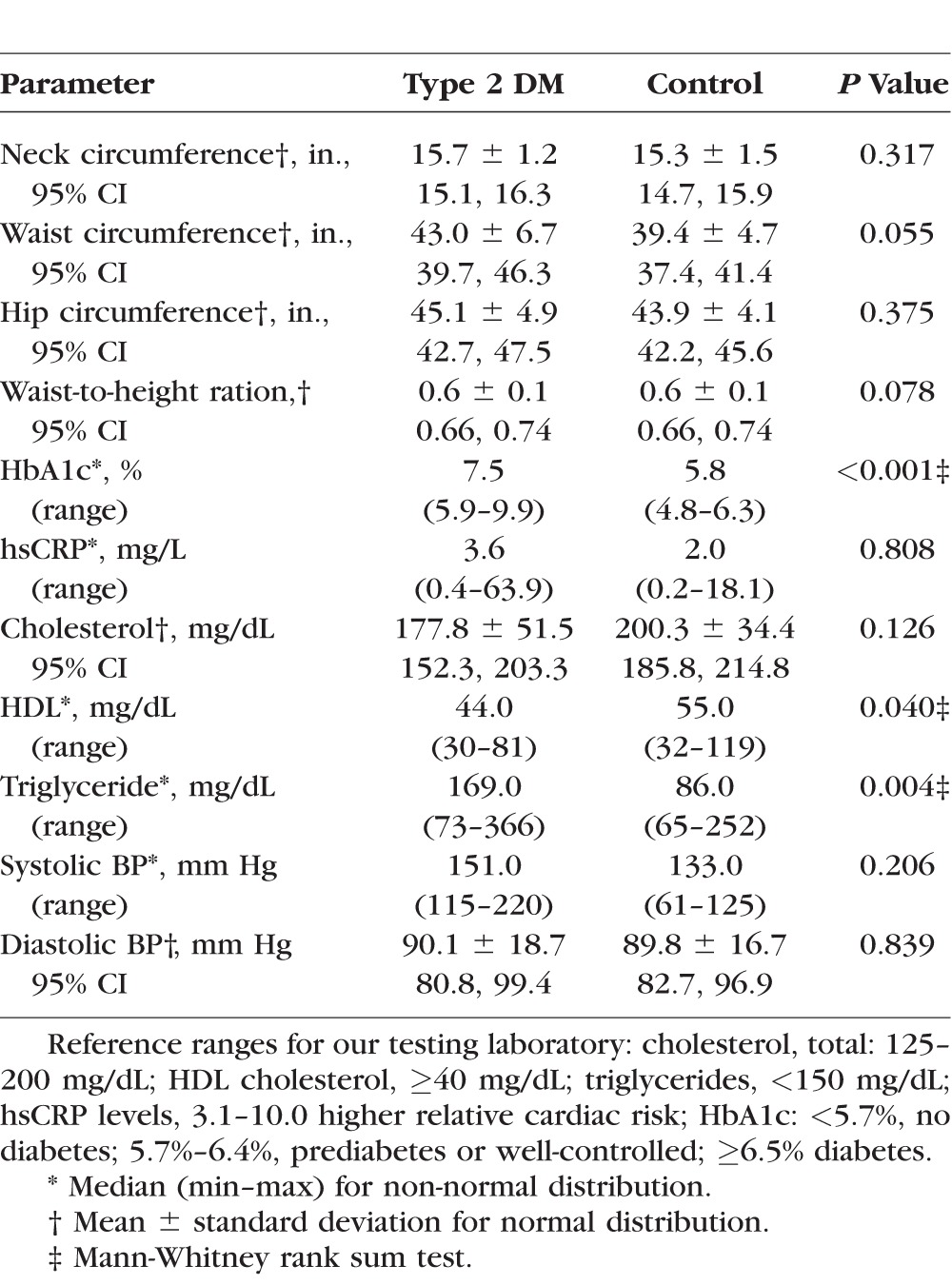
A total of 40 participants were recruited for this study. Participant demographics are displayed in Table 1. There were no differences in patient age between groups (58.8 ± 10.2 years of age versus 53.3 ± 9.7 years of age, P = 0.065, t-test). In the diabetic group, 33.3% of the participants were male and 66.7% were female. In the control group, 45.0% of participants were male and 55.0% were female. This was not significantly different (P = 0.111, χ2 test). Test and control groups were also matched for smoking status (11.2% compared to 14.0%, respectively, P = 0.669, χ2 test) and body mass index confirmed that all subjects were obese (33.5 ± 6.3 and 31.2 ± 4.3, respectively, P = 0.222, t-test). Serologic and anthropometric data are shown in Table 2. There were no significant differences in neck, waist, or hip circumferences between groups (P = 0.317, P = 0.055, and P = 0.375, respectively). Similar to body mass index, there was no significant difference in waist-to-height ratio between groups (P = 0.078, t-test). The median HbA1c for the diabetic group was 7.5% (range: 5.9%–9.9%) compared to 5.8% (range: 4.8%–6.3%) for the control group. This difference was significant (P < 0.001, Mann-Whitney rank sum test). Less than 5.7% is the normative value for our laboratory, indicating the presence of a few prediabetic individuals in the control group. There was no difference in hsCRP between groups (median value of 3.6 compared to 5.8 in diabetics and controls, respectively, P = 0.808, Mann-Whitney rank sum test). Similarly, there was no difference in total cholesterol (177.8 ± 51.5 mg/dL versus 200.3 ± 34.4 mg/dL, P = 0.126, t-test). However, high density lipoproteins were significantly higher in the control group (median value 44.0 mg/dL compared to 55.0 mg/dL, P = 0.040, Mann-Whitney rank sum test), while triglyceride levels were significantly higher in the diabetic group (169.0 mg/dL compared to 86.0 mg/dL, P = 0.004, Mann-Whitney rank sum test). Systolic and diastolic blood pressure ranges were not significantly different between diabetics and controls (median value 151.0 mm Hg versus 133.0 mm Hg for systolic and 90.1 ± 18.7 mm Hg versus 89.8 ± 17.4 mm Hg for diastolic, P = 0.206 and P = 0.839, respectively).
Table 1.
Patient Demographics
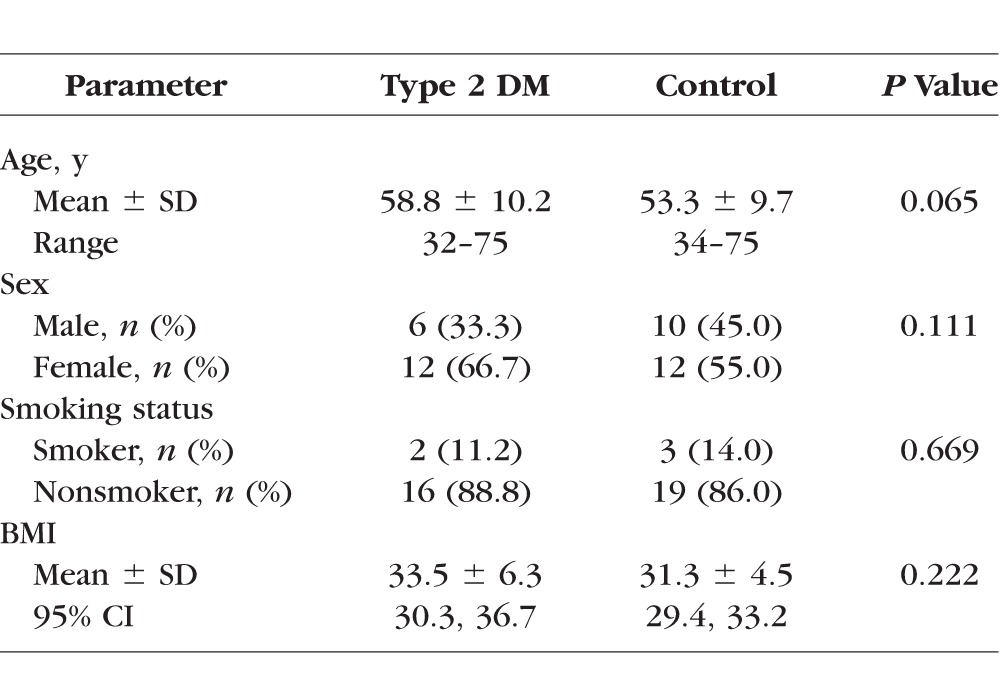
Table 2.
Serologic and Anthropometric Data
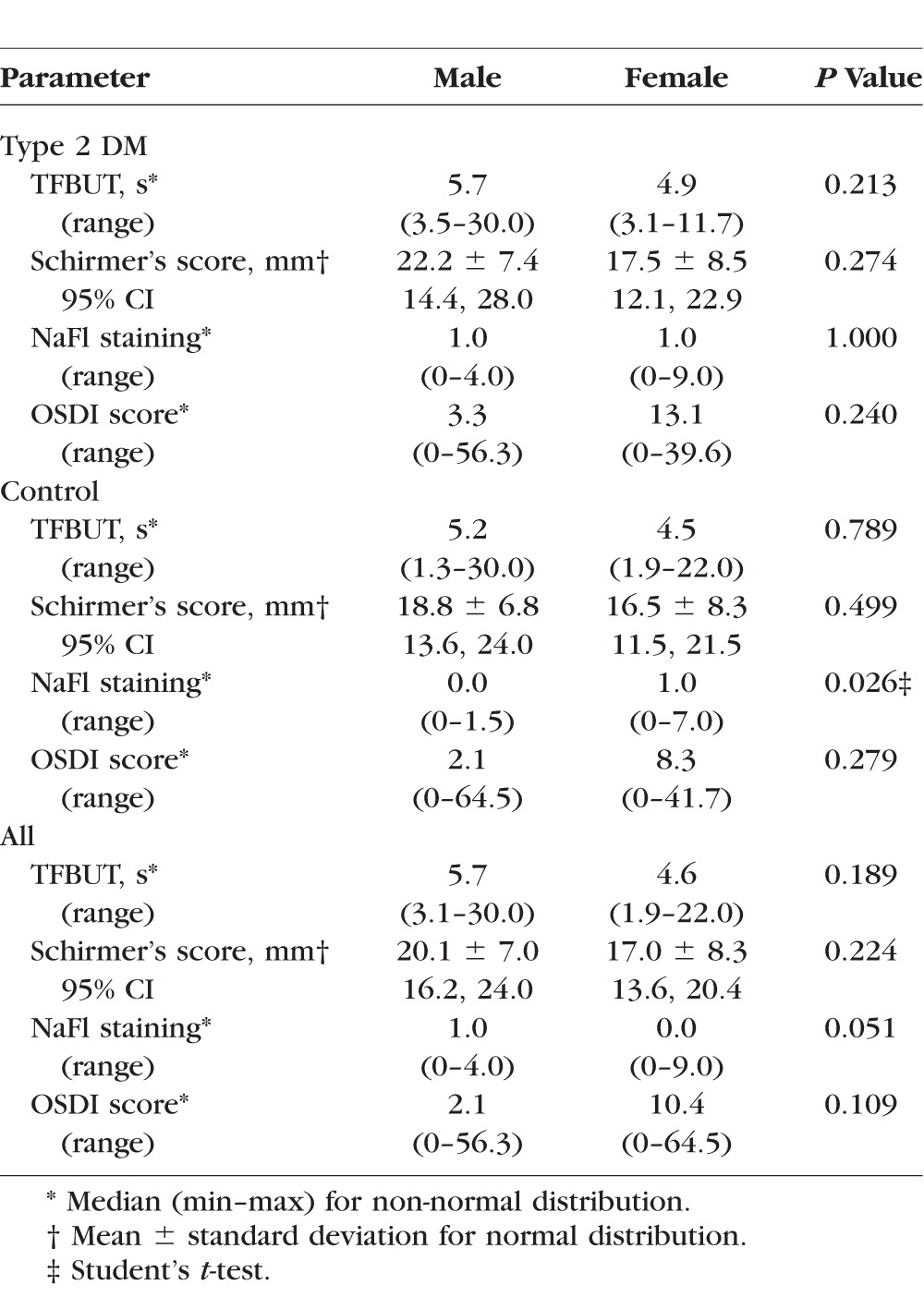
There were no significant differences in dry eye parameters between the diabetic group and controls (Table 3). With the exception of tear break-up time, all testing parameters were within normal values for a non–dry eye subject. Tear film break-up time was slightly lower in the control group, although not significant (median value of 5.5 seconds in diabetes compared to 4.8 seconds in the control, P = 0.765, Mann-Whitney rank sum test). Schirmer's scores averaged 19.1 ± 8.2 mm for the diabetic group and 17.8 ± 7.9 mm for controls (P = 0.510, t-test). Fluorescein staining scores were also similar, with median scores of 1.0 and 0.5 for diabetics and controls, respectively (P = 0.881, Mann-Whitney rank sum test). The Ocular Surface Disease Index questionnaire scores were marginally higher for the diabetic group, median value of 10.4 compared to 3.2 for the controls, although not statistically significant (P = 0.256, Mann-Whitney rank sum test). Since the proportion of women to men was slightly higher in the diabetic group, analysis of male versus female scores for the dry eye tests were further analyzed (Table 4). In general, measured values for tear film break-up time and Schirmer's testing were lower in females than males, while sodium fluorescein (NaFl) staining and the OSDI measures were higher. None of these changes were statistically significant, with the exception fluorescein staining in the control group. In addition, a comparison of nerve fiber length (1648.7 ± 607.6 mm2 compared to 1824.8 ± 499.7 mm2 for females and males, respectively) and nerve branch density (median value of 4.7 with a range of 0–14.6 for females, and 4.5 with a range of 0.4–14.8 for males) showed no differences (P = 0.375 and P =0.471 for nerve fiber length and nerve branch density, respectively).
Table 3.
Dry Eye Testing
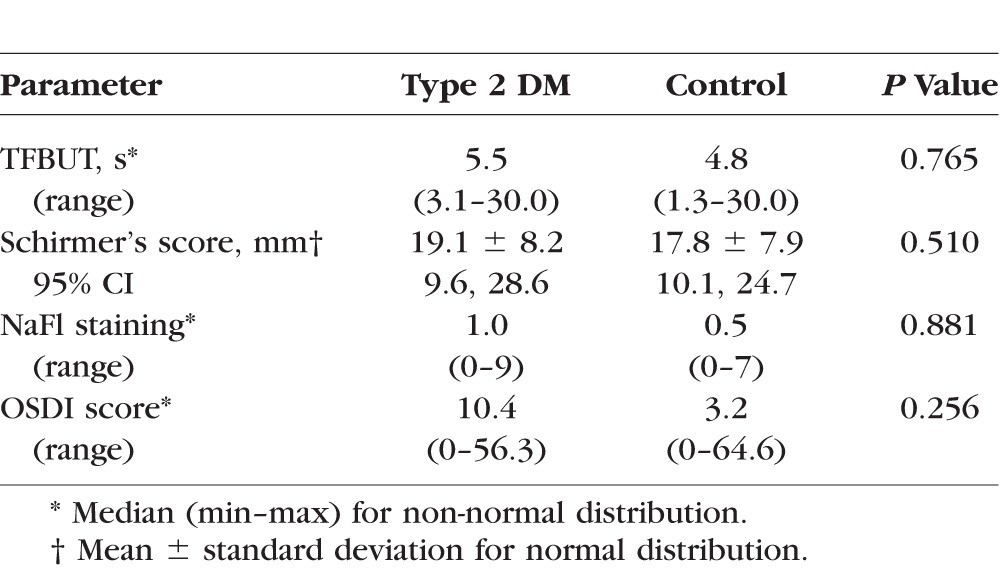
Table 4.
Sex Differences in Dry Eye Parameters
There was no difference in corneal sensitivity between test and control groups (P = 0.421, t-test, Fig. 2A). Representative in vivo confocal images of the subbasal nerve plexus in the normal and diabetic cornea are shown in Figure 1. There was a 22% reduction in nerve fiber length in participants with diabetes (1531.6 ± 144.4 μm) compared to control (1967.1 ± 92.9 μm; P = 0.012, t-test, Fig. 2B) and in nerve fiber branching (median value of 3.8, range 0–9 branches/μm2 for diabetics compared to 7.3, range: 2–14.8 branches/μm2 for controls, P = 0.024, Fig. 2C, Mann-Whitney rank sum test). There was also a significant reduction in the density of basal corneal epithelial cells from 1039.3 ± 19.4 cells/μm2 in controls to 981.5 ± 18.0 cells/μm2 in the diabetic group (P = 0.04, Fig. 2D, t-test). The mean concentration of IGFBP-3 in diabetic tears was 26.1 ± 7.2 μg/μL (Fig. 3A). This was significantly lower in the control group (7.5 ± 1.6 μg/μL, P < 0.05, t-test). HbA1c was not correlated with IGFBP-3 (R = 0.318, P = 0.062, power = 0.463, Fig. 3B). As expected, there was a strong correlation between nerve fiber length and nerve fiber branching, with shorter nerves having fewer branches (R = 0.767, P < 0.001, power = 1.000, Fig. 4A). Comparison of tear IGFBP-3 levels against nerve morphologic parameters showed strong correlations between nerve fiber length and IGFBP-3 (R = 0.522, P = 0.001, power = 0.906, Fig. 4B) and nerve branch density and IGFBP-3 (R = 0.481, P = 0.003, power = 0.842, Fig. 4C). Nerve fiber length was moderately correlated with HbA1c (R = 0.469, P = 0.004, power = 0.821, Fig. 5A), whereas nerve branch density was only weakly correlated with HbA1c (R = 0.394, P = 0.019, power 0.655, Fig. 5B).
Figure 2.

Corneal nerve structure and function. (A) Corneal sensitivity was assessed in the inferior mid-peripheral cornea, approximately 3 mm above the limbus. There was no detectable difference in corneal sensitivity between groups (P = 0.421, t-test). (B) Nerve fiber length was significantly reduced in the diabetic group compared to controls (P = 0.012, t-test). (C) Nerve branch density was also significantly reducted in the diabetic group (P = 0.024, Mann-Whitney rank sum test). (D) Basal corneal epithelial cell density had a small, but significant reduction in the number of cells per μm2 (P = 0.04, t-test).
Figure 1.
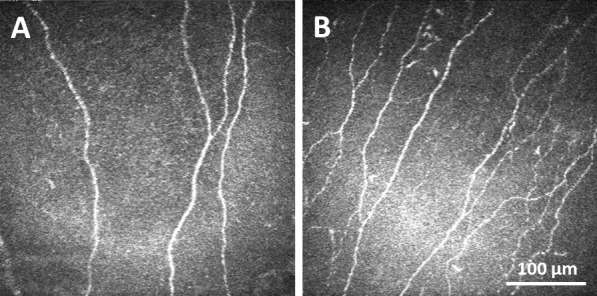
Representative in vivo confocal images of the subbasal nerve plexus. (A) Confocal image showing few corneal nerve fibers in a patient with diabetes. (B) Confocal image of the subbasal nerve plexus in the control cornea. Scale bar: 100 μm.
Figure 3.
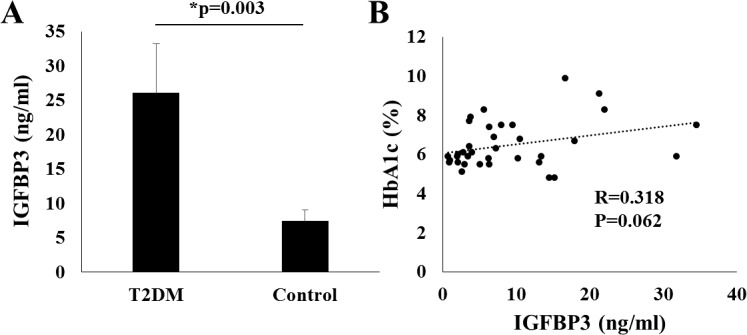
Tear levels of IGFBP-3. (A) ELISA analysis of basal tears showed an increase in IGFBP-3 from patients with diabetes compared to nondiabetic controls (P = 0.003, t-test). (B) Linear regression analysis showed no correlation between HbA1c levels and tear concentration of IGFBP-3 (R = 0.318, P = 0.062).
Figure 4.
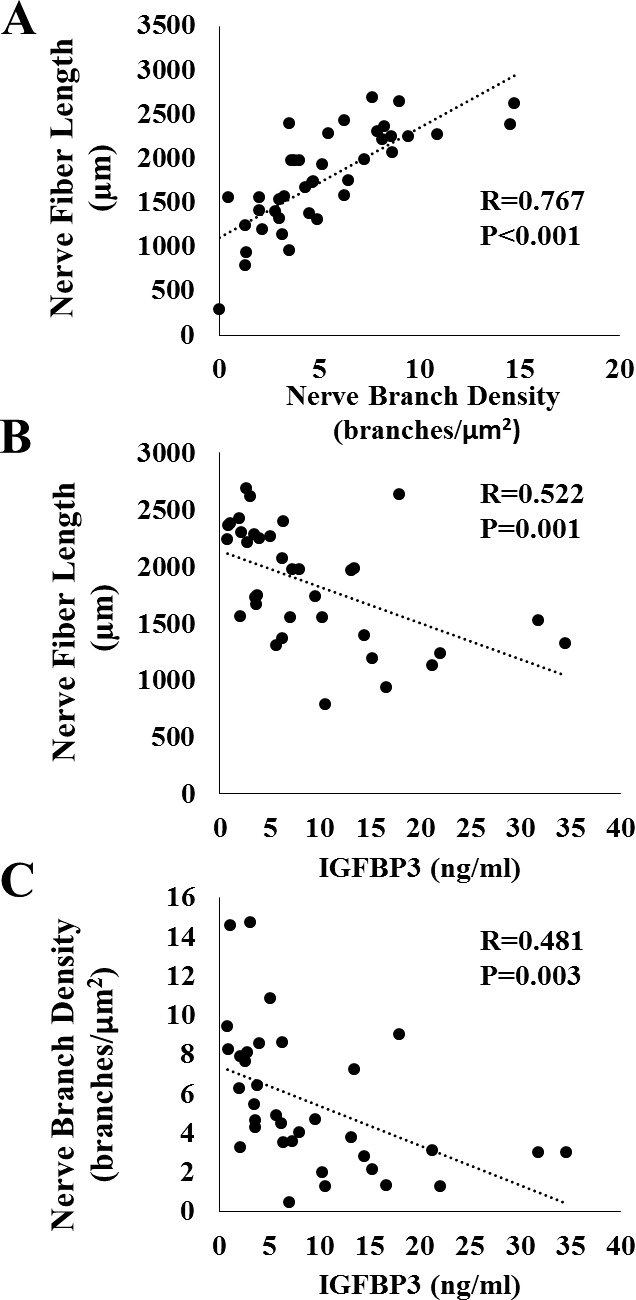
The relationship between nerve fiber morphology and tear levels of IGFBP-3. (A) Regression analysis revealed a high correlation between nerve fiber length and nerve branch density (R = 0.767, P < 0.001). (B) There was a strong correlation between nerve fiber length and IGFBP-3 (R = 0.522, P = 0.001). (C) There was also a good correlation between nerve branch density and IGFBP-3 (R = 0.481, P = 0.003).
Figure 5.
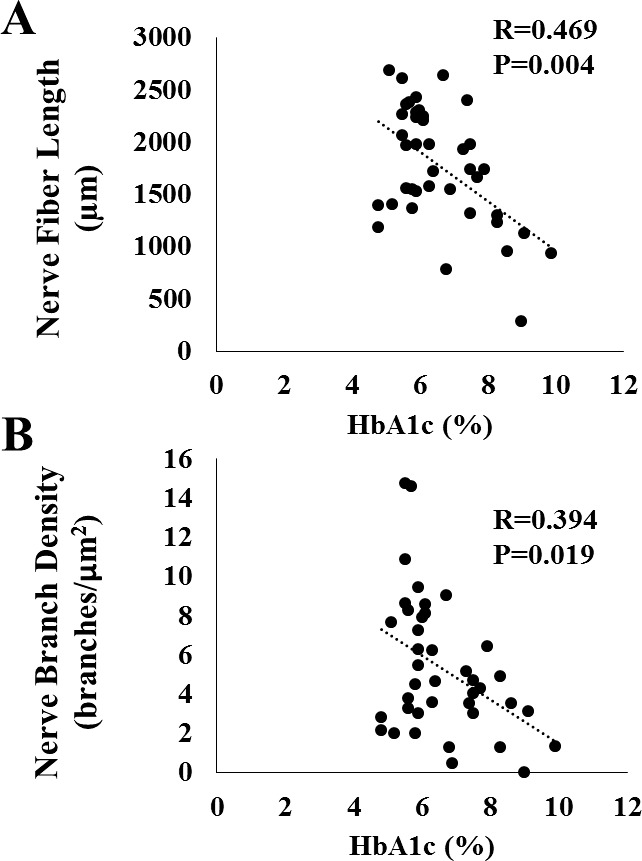
The relationship between nerve fiber morphology and HbA1c. (A) Regression analysis showed a moderate correlation between nerve fiber length and HbA1c (R = 0.469, P = 0.004). (B) The was a weak correlation between nerve branch density and HbA1c (R = 0.394, P = 0.019).
Discussion
This study showed, for the first time, a direct relationship between tear levels of IGFBP-3 and corneal nerve loss in patients with type 2 diabetes mellitus. We have previously shown that tears levels of IGFBP-3 are elevated in patients with diabetes.30 In that pilot study, we reported that the tear concentration of IGFBP-3 is approximately 3-fold higher in diabetics compared to nondiabetic controls. Limitations to that study included a small sample size, a mixed population of type 1 and type 2 diabetic participants, and the absence of any dry eye testing that may account for the differences in tear concentration of IGFBP-3. Clinical signs of dry eye, such as reduced tear production, have been reported in diabetes.28,36–38 Thus, in this study we extended our prior results to exclude dry eye as the underlying cause for elevated IGFBP-3 levels. While the scores on the Ocular Surface Disease Index trended toward being slightly higher in the diabetic group compared to controls, reduced TFBUT measurements were borderline for both groups, suggesting mild dry eye may be present in a few patients in both the diabetics and controls. Importantly, there were no significant differences in any of the other dry eye parameters tested. The absence of retinopathy in the diabetic cohort presented here also suggests that these are somewhat well-controlled diabetics and may account the lack of significant dry eye findings.
Consistent with other laboratories, using in vivo confocal microscopy we demonstrated a reduction in nerve fiber length and nerve fiber branching in subjects with diabetes.17–19,21–23 We also found a significant reduction in the density of basal corneal epithelial cells. This finding is in agreement with work done by our laboratory reporting a decrease in the density of basal corneal epithelial cells in a streptozotocin mouse model of type 1 diabetes mellitus.39 In that study, we used three-dimensional corneal nerve modeling and found a significant decrease in nerve fiber length in the subbasal nerve plexus. While corneal sensitivity was not tested using our animal model, we did not detect any differences in the length of the terminal epithelial nerves. The terminal epithelial nerves are small nerve fibers that branch from the subbasal nerve plexus and course toward the corneal epithelial surface. From our imaging data, it appeared that only a subset of nerve fibers in the subbasal nerve plexus had terminal epithelial nerves that branched and ran toward the corneal surface. Based upon those findings, we hypothesized that a robust amount of nerve fiber damage in the subbasal nerve plexus was required before corneal sensitivity was affected. That hypothesis was consistent with data from other studies that failed to show correlations between loss in corneal sensitivity and the reduction in nerve fiber length in the subbasal nerve plexus and is consistent with the findings presented here.22
In the corneal epithelium, IGFBP-3 is upregulated in response to cellular stress. We have shown that IGFBP-3 increases in response to hyperglycemia.30 In proximal tubular epithelial cells, oxidative stress from hyperglycemic culture upregulates IGFBP-3 and potentiates apoptotic cell death.8 Similarly, increased levels of IGFBP-3 have been associated with apoptotic cell death in human mesangial cells following stress induced by the loss of growth factors during serum withdrawal.40 We hypothesize that the increased secretory levels of IGFBP-3 may promote apoptosis or necrosis of corneal sensory nerves. In addition to direct effects by IGFBP-3 on corneal sensory nerves, IGFBP-3 is the principal binding protein for IGF-1, which is known to have potent neuroprotective actions.41 Sequestration of IGF-1 by IGFBP-3 may increase susceptibility of neuronal cell loss in the presence of hyperglycemia, inflammation, and oxidative stress, all known mediators of diabetic complications.42,43 IGF-1 has also been shown to be present in human tear fluid; however, IGF-1 levels are independent of the changes in IGFBP-3 in diabetes. Thus, the shift in the IGF-1:IGFBP-3 ratio in diabetes may account for the reduction in corneal nerve fiber length and corneal nerve fiber branching through IGF-1 dependent and independent mechanisms. This contrasts with the effects of IGFBP-3 on corneal epithelial cells, where treatment with IGFBP-3 abrogates cell proliferation through IGF-1 inhibition.44 This perturbation in the proliferative status of basal corneal epithelial cells is a likely contributor to the alteration in basal corneal epithelial cell density reported here. It is important to note, however, that ELISAs were used to measure tear concentration of IGFBP-3. Thus, from the data presented, we cannot conclude whether the measurement of IGFBP-3 represents the whole, intact protein as opposed to cleavage fragments. IGFBP-3 is highly subject to proteolytic cleavage and cleavage will likely impact function. Further studies are necessary to investigate the state of IGFBP-3 in human tear fluid.
The relationship between HbA1c and loss of the subbasal nerve plexus is not well-defined. Confocal microscopic analysis of the increased tortuosity of the subbasal nerve plexus in diabetes is not associated with increasing levels of HbA1c.14 However, in healthy subjects HbA1c levels were inversely correlated with length of the subbasal nerve plexus.45 Likewise, studies have shown that in diabetic subjects, an improvement in HbA1c either from well-controlled medical therapy or simultaneous pancreas and kidney transplantation, there is a corresponding improvement in the subbasal nerve plexus from corneal nerve fiber regeneration.27,46,47 The present data show a weak to modest correlation between HbA1c and nerve fiber branch density and nerve fiber length. Furthermore, HbA1c failed to show any relationship with tear concentration of IGFBP-3. This suggests that while IGFBP-3 may be an indicator of ocular damage in diabetes, it is not directly related to blood sugar control. This is not altogether unsurprising since unlike type 1 diabetes mellitus, where tight glycemic control prevents long-term nerve damage, other factors than hyperglycemia alone contribute to diabetic complications, including ocular complications, in patients with type 2 disease.
As discussed above, IGFBP-3 levels were not affected by the objective dry eye parameters studied. While mild dry eye was suspect in both groups based on the shortened tear film break-up time, the difference between groups was not significant. Moreover, the trend toward an increase in the OSDI index score was higher in the diabetic group compared to the control. This too was not significant. Not surprisingly, analysis of the differences between sexes for dry eye parameters suggested potential mild dry eye among females. This sex effect was not reflected in differences in the nerve fiber layer of nerve fiber branching between groups and suggests that dry eye was not the driving factor for reduced nerve fiber length and nerve fiber branching between diabetics and controls in this study. Assessment of the subbasal nerve plexus in dry eye has shown significant alterations in both evaporative and aqueous deficient dry eye.48,49 This includes decreases in both the nerve fiber length and branch density. Importantly, the severity of the dry eye is known to correlate with the extent of the structural changes in the subbasal nerve plexus.50 Most prior studies have not compensated for the potential effects of diabetes-induced dry eye on the subbasal nerve plexus and this may account, in part, for the large variation in normative values reported in diabetic in vivo confocal microscopy studies. Another difference between the current and prior studies is that volunteers in the current study were also matched for smoking status and obesity, conditions that have deleterious effects on the body through the increase of oxidative stress and inflammation.
In summary, the results presented here confirm our prior work demonstrating that the concentration of IGFBP-3 in human tear fluid is increased approximately 3-fold in diabetes. A limitation to this work is that we did not measure total protein, but reported levels of IGFBP-3 based upon the measured concentration. While total tear protein may be altered in diabetes, the marked increase in the concentration of IGFBP-3 reported in this study was significantly correlated with nerve fiber loss and a reduction in nerve fiber branching in the corneal subbasal nerve plexus. Taken together, these data suggest that tear concentration of IGFBP-3 may be an indicator for early diabetic corneal nerve damage. Further studies are underway to determine the exact function of IGFBP-3 in human corneal epithelium and the corresponding effects on trigeminal sensory nerves in the cornea as well; and to evaluate tear IGFBP-3 in diabetic patients that are stratified by severity of disease.
Acknowledgments
Supported by National Institutes of Health/National Eye Institutes Grants R21 EY024433 (DMR); R01 EY024546 (DMR); National Institutes of Health Core Grant P30 EY020799; and an unrestricted grant from Research to Prevent Blindness (New York, NY, USA).
Disclosure: W.L. Stuard, None; R. Titone, None; D.M. Robertson, None
References
- 1. DelMonte DW, Kim T. . Anatomy and physiology of the cornea. J Cataract Refract Surg. 2011; 37: 588– 598. [DOI] [PubMed] [Google Scholar]
- 2. Marfurt CF, Cox J, Deek S, Dvorscak L. . Anatomy of the human corneal innervation. Exp Eye Res. 2010; 90: 478– 492. [DOI] [PubMed] [Google Scholar]
- 3. Schimmelpfennig B. . Nerve structures in human central corneal epithelium. Graefes Arch Clin Exp Ophthalmol. 1982; 218: 14– 20. [DOI] [PubMed] [Google Scholar]
- 4. Muller LJ, Pels L, Vrensen GF. . Ultrastructural organization of human corneal nerves. Invest Ophthalmol Vis Sci. 1996; 37: 476– 488. [PubMed] [Google Scholar]
- 5. Muller LJ, Vrensen GF, Pels L, Cardozo BN, Willekens B. . Architecture of human corneal nerves. Invest Ophthalmol Vis Sci. 1997; 38: 985– 994. [PubMed] [Google Scholar]
- 6. Ueda S, del Cerro M, LoCascio JA, Aquavella JV. . Peptidergic and catecholaminergic fibers in the human corneal epithelium. An immunohistochemical and electron microscopic study. Acta Ophthalmol Suppl. 1989; 192: 80– 90. [DOI] [PubMed] [Google Scholar]
- 7. Petroll WM, Robertson DM. . In vivo confocal microscopy of the cornea: new developments in image acquisition, reconstruction, and analysis using the HRT-Rostock corneal module. Ocul Surf. 2015; 13: 187– 203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Allgeier S, Zhivov A, Eberle F,et al. . Image reconstruction of the subbasal nerve plexus with in vivo confocal microscopy. Invest Ophthalmol Vis Sci. 2011; 52: 5022– 5028. [DOI] [PubMed] [Google Scholar]
- 9. Patel DV, McGhee CNJ. . Mapping of the normal human corneal sub-basal nerve plexus by in vivo laser scanning confocal microscopy. Invest Ophthalmol Vis Sci. 2005; 46: 4485– 4488. [DOI] [PubMed] [Google Scholar]
- 10. Oliveira-Soto L, Efron N. . Morphology of corneal nerves using confocal microscopy. Cornea. 2001; 20: 374– 384. [DOI] [PubMed] [Google Scholar]
- 11. Patel DV, McGhee CN. . In vivo confocal microscopy of human corneal nerves in health, in ocular and systemic disease, and following corneal surgery: a review. Br J Ophthalmol. 2009; 93: 853– 860. [DOI] [PubMed] [Google Scholar]
- 12. Rosenberg ME, Tervo TM, Immonen IJ, Muller LJ, Gronhagen-Riska C, Vesaluoma MH. . Corneal structure and senstivity in type 1 diabetes mellitus. Invest Ophthalmol Vis Sci. 2000; 41: 2915– 2921. [PubMed] [Google Scholar]
- 13. Hossain P, Sachdev A, Malik RA. . Early detection of diabetic peripheral neuropathy with corneal confocal microscopy. Lancet. 2005; 366: 1340– 1343. [DOI] [PubMed] [Google Scholar]
- 14. Kallinikos P, Berhanu M, O'Donnell C, Boulton AJ, Efron N, Malik RA. . Corneal nerve tortuosity in diabetic patients with neuropathy. Invest Ophthalmol Vis Sci. 2004; 45: 418– 422. [DOI] [PubMed] [Google Scholar]
- 15. Petropoulos IN, Green P, Chan AW,et al. . Corneal confocal microscopy detects neuropathy in patients with type 1 diabetes without retinopathy or microalbuminuria. PLoS One. 2015; 10: e0123517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Papanas N, Ziegler D. . Corneal confocal microscopy: recent progress in the evaluation of diabetic neuropathy. J Diabetes Investig. 2015; 6: 381– 389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Chang P-Y, Carrel H, Huang J-S,et al. . Decreased density of corneal basal epithelium and subbasal corneal nerve bundle changes in patients with diabetic retinopathy. Am J Ophthalmol. 2006; 142: 488– 490. [DOI] [PubMed] [Google Scholar]
- 18. Stem MS, Hussain M, Lentz SI,et al. . Differential reduction in corneal nerve fiber length in patients with type 1 or type 2 diabetes mellitus. J Diabetes Complications 2014; 28: 658– 661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ziegler D, Papanas N, Zhivov A,et al. . Early detection of nerve fiber loss by corneal confocal microscopy and skin biopsy in recently diagnosed type 2 diabetes. Diabetes. 2014; 63: 2454– 2463. [DOI] [PubMed] [Google Scholar]
- 20. Edwards K, Pritchard N, Vagenas D, Russell A, Malik RA, Efron N. . Utility of corneal confocal microscopy for assessing mild diabetic neuropathy: baseline findings of the LANDMark study. Clin Exp Optom. 2012; 95: 348– 354. [DOI] [PubMed] [Google Scholar]
- 21. Tavakoli M, Quattrini C, Abbott C,et al. . Corneal confocal microscopy: a novel noninvasive test to diagnose and stratify the severity of human diabetic neuropathy. Diabetes Care. 2010; 33: 1792– 1797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Messmer EM, Schmid-Tannwald C, Zapp D, Kampik A. . In vivo confocal microscopy of corneal small fiber damage in diabetes mellitus. Graefes Arch Clin Exp Ophthalmol. 2010; 248: 1307– 1312. [DOI] [PubMed] [Google Scholar]
- 23. Quattrini C, Tavakoli M, Jeziorska M,et al. . Surrogate markers of small fiber damage in human diabetic neuropathy. Diabetes. 2007; 56: 2148– 2154. [DOI] [PubMed] [Google Scholar]
- 24. Malik RA, Kallinikos P, Abbott CA,et al. . Corneal confocal microscopy: a non-invasive surrogate of nerve fibre damage and repair in diabetic patients. Diabetologia. 2003; 46: 683– 688. [DOI] [PubMed] [Google Scholar]
- 25. Hertz P, Bril V, Orszag A,et al. . Reproducibility of in vivo corneal confocal microscopy as a novel screening test for early diabetic sensorimotor polyneuropathy. Diabet Med. 2011; 28: 1253– 1260. [DOI] [PubMed] [Google Scholar]
- 26. Jiang MS, Yuan Y, Gu ZX, Zhuang SL. . Corneal confocal microscopy for assessment of diabetic peripheral neuropathy: a meta-analysis. Br J Ophthalmol. 2016; 100: 9– 14. [DOI] [PubMed] [Google Scholar]
- 27. Tavakoli M, Kallinikos P, Iqbal A,et al. . Corneal confocal microscopy detects improvement in corneal nerve morphology with an improvement in risk factors for diabetic neuropathy. Diabet Med. 2011; 28: 1261– 1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Goebbels M. . Tear secretion and tear film function in insulin dependent diabetics. Br J Ophthalmol. 2000; 84: 19– 21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Manaviat MR, Rashidi M, Afkhami-Ardekani M, Shoja MR. . Prevalence of dry eye syndrome and diabetic retinopathy in type 2 diabetic patients. BMC Ophthalmol. 2008; 8: 10– 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Wu YC, Buckner BR, Zhu M, Cavanagh HD, Robertson DM. . Elevated IGFBP3 levels in diabetic tears: a negative regulator of IGF-1 signaling in the corneal epithelium. Ocul Surf. 2012; 12: 100– 107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kelley KM, Oh Y, Gargosky SE,et al. . Insulin-like growth factor-binding proteins (IGFBPs) and their regulatory dynamics. Int J Biochem Cell Biol. 1996; 28: 619– 737. [DOI] [PubMed] [Google Scholar]
- 32. Butt AJ, Williams AC. . IGFBP-3 and apoptosis - a license to kill? Apoptosis. 2001; 6: 199– 205. [DOI] [PubMed] [Google Scholar]
- 33. Granata R, Trovato L, Garbarino G,et al. . Dual effects of IGFBP-3 on endothelial cell apoptosis and survival: involvement of the sphingolipid signaling pathways. FASEB J. 2004; 18: 1456– 1458. [DOI] [PubMed] [Google Scholar]
- 34. Janssen PT, van Bijsterveld OP. . Origin and biosynthesis of human tear fluid proteins. Invest Ophthalmol Vis Sci. 1983; 24: 623– 630. [PubMed] [Google Scholar]
- 35. Petroll WM, Cavanagh HD. . Remote-controlled scanning and automated confocal microscopy through focusing using a modified HRT rostock corneal module. Eye Contact Lens. 2009; 35: 302– 308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Zhang X, Zhao L, Deng S, Sun X, Wang N. . Dry eye syndrome in patients with diabetes mellitus: prevalence, etiology, and clinical characteristics. J Ophthalmol. 2016; 2016: 8201053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Baek J, Doh SH, Chung SK. . Assessment of the tear meniscus using optical coherence tomography in patients with type 2 diabetes mellitus. Cornea. 2015; 34: 1534– 1540. [DOI] [PubMed] [Google Scholar]
- 38. Liu H, Sheng M, Liu Y,et al. . Expression of SIRT1 and oxidative stress in diabetic dry eye. Int J Clin Exp Pathol. 2015; 8: 7644– 7653. [PMC free article] [PubMed] [Google Scholar]
- 39. Cai D, Zhu M, Petroll WM, Koppaka V, Robertson DM. . The impact of type 1 diabetes mellitus on corneal epithelial nerve morphololgy and the corneal epithelium. Am J Pathol. 2014; 184: 2662– 2670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Mishra R, Emancipator SN, Kern T, Simonson MS. . High glucose evokes an intrinsic proapoptotic signaling pathway in mesangial cells. Kidney Int. 2005; 67: 82– 93. [DOI] [PubMed] [Google Scholar]
- 41. Zheng WH, Kar S, Dore S, Quirion R. . Insulin-like growth factor-1 (IGF-1): a neuroprotective trophic factor acting via the Akt kinase pathway. J Neural Transm Suppl. 2000; 261– 272. [DOI] [PubMed]
- 42. Brownlee M. . The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005; 54: 1615– 1625. [DOI] [PubMed] [Google Scholar]
- 43. Rolo AP, Palmeira CM. . Diabetes and mitochondrial function: role of hyperglycemia and oxidative stress. Toxicol Appl Pharmacol. 2006; 212: 167– 178. [DOI] [PubMed] [Google Scholar]
- 44. Wu YC, Zhu M, Robertson DM. . Novel nuclear localization and potential function of insulin-like growth factor-1 receptor/insulin receptor hybrid in corneal epithelial cells. PLoS One. 2012; 7: e42483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Wu T, Ahmed A, Bril V,et al. . Variables associated with corneal confocal microscopy parameters in healthy volunteers: implications for diabetic neuropathy screening. Diabet Med. 2012; 29: e297– e303. [DOI] [PubMed] [Google Scholar]
- 46. Tavakoli M, Mitu-Pretorian M, Petropoulos IN,et al. . Corneal confocal microscopy detects early nerve regeneration in diabetic neuropathy after simultaneous pancreas and kidney transplantation. Diabetes. 2013; 62: 254– 260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Mehra S, Tavakoli M, Kallinikos PA,et al. . Corneal confocal microscopy detects early nerve regeneration after pancreas transplantation in patients with type 1 diabetes. Diabetes Care. 2007; 30: 2608– 2612. [DOI] [PubMed] [Google Scholar]
- 48. Zhang M, Chen J, Luo L, Xiao Q, Sun M, Liu Z. . Altered corneal nerves in aqueous tear deficiency viewed by in vivo confocal microscopy. Cornea. 2005; 24: 818– 824. [DOI] [PubMed] [Google Scholar]
- 49. Villani E, Magnani F, Viola F,et al. . In vivo confocal evaluation of the ocular surface morpho-functional unit in dry eye. Optom Vis Sci. 2013; 90: 576– 586. [DOI] [PubMed] [Google Scholar]
- 50. Labbe A, Liang Q, Wang Z,et al. . Corneal nerve structure and function in patients with non-sjogren dry eye: clinical correlations. Invest Ophthalmol Vis Sci. 2013; 54: 5144– 5150. [DOI] [PubMed] [Google Scholar]