

Abstract
Purpose of review:
To provide an introduction and review of sleep metrics appropriate for use with an outpatient concussed population.
Recent findings:
Although sleep issues are frequently identified in concussion, sleep disturbance is rarely assessed in outpatient settings. Given that sleep disturbance may be indicative of, or contribute to, delayed neurocognitive recovery, measurement tools for sleep, rest, and activity behavior may be of both practical and research utility.
Summary:
Because sleep disturbance symptoms may vary between or within an individual throughout the course of recovery, it is recommended that sleep be measured at regular intervals over the entirety of recovery. Included is a discussion on how to select appropriate measures based on patient symptomology in addition to common practical concerns. Additional clinical considerations, a review of traditional pencil and paper methods of continuous sleep behavior monitoring, as well as technologies for measuring sleep and activity behavior are also included.
A 43-year-old woman who had a concussion as the result of a motor vehicle accident 4 weeks previously complains of varied sleep disturbances. Although she reports initial hypersomnia immediately after her injury, she states that in the subsequent weeks her symptoms are more indicative of insomnia (e.g., waking up in the middle of the night and trouble falling asleep) and daytime sleepiness (feeling sleepy at work and falling asleep in front of the television). She asks if this pattern of sleep disturbance is typical following concussion.
Sleep disturbance postconcussion
An estimated 30%–70% of post–traumatic brain injury (TBI) patients report difficulty sleeping in the first few weeks postinjury.1 Hypersomnia is likely to be present in 25% of TBI patients within the first few days after injury.2 Following the acute phase of injury, insomnia symptoms are reported in 30% of people3 and circadian rhythm shifts can also present in approximately 36% of those in the postacute phase.4 In addition, 43%–73% of people report symptoms of fatigue.5
Although sleep disturbance is documented among all levels of TBI severity, this article aims to focus on sleep disturbances following concussion. The nomenclature surrounding mild brain injury has been inconsistent and reflects the division between the fields of sports and rehabilitation medicine in mild TBI (mTBI) research. Although concussion falls in the spectrum of mild brain injury and the terms concussion and mTBI are often used interchangeably,6 we refer to the popular consensus definition of sport concussion for the purpose of this article7 due to its wide acceptance among those involved with rehabilitation and sports medicine practice.
The pattern and time frame of sleep disturbance may vary substantially among patients with concussion. For example, many neurologists may receive a report of excessive sleepiness within the first week after injury, followed by sleeplessness or difficulty falling asleep in the subsequent weeks.
People with concussions often report that they are excessively sleepy in the first week following injury and may report taking daytime naps. However, 2 to 3 weeks after their injury, they may report difficulty falling asleep or early morning awakenings, which in turn may be fueling daytime fatigue. It is important that health providers be able to evaluate both nighttime and daytime sleep behavior as these sleep patterns may be ultimately linked to a 24-hour circadian shift or, alternatively, nighttime sleeping difficulties may be the root of daytime sleepiness.
Despite their pervasiveness and consequences, changes in sleep behavior are not often addressed in the course of concussion recovery. This is important as complaints of insomnia, in particular, have been reported to persist from a few weeks to 2 to 3 years after the initial injury.5 Notably, it also appears that people with concussion report greater incidence of sleep disturbance vs those with moderate to severe brain injury.5 This may be because those with concussion return to work and daily schedules sooner despite not being completely recovered, and thus sleep problems persist longer in this population.5
Because neurologists frequently encounter postconcussion patients, it is especially important to develop an awareness of sleep disturbances associated with concussion and to also be familiar with tools to make appropriate assessments. This article provides a general review and guide to selecting sleep-monitoring measures (both low and high technological options) and discusses strategies for behavioral sleep assessment in clinical settings.
Current assessment of sleep, rest, and activity
Following concussion, specific assessment of sleep behavior is often limited. One or two questions may be asked as part of a larger symptom checklist such as the ImPACT.8,9 Many sleep assessment questionnaires are administered one time at patient intake and occasionally repeated at patient discharge. Moreover, these assessments are usually state-based, and are only designed to capture a snapshot of sleep behavior in an abbreviated time span. For example, the ImPACT symptom questionnaire only asks whether one has felt excessively sleepy or has had difficulty falling asleep within the past 7 days. State-based, global measures may provide a gross estimate of sleep behavior within persons with concussion, but may be insufficient in a concussed population whose state may be changing with recovery. Moreover, what may present as a sleep problem may actually be indicative of disruption of the 24-hour circadian system that affects day and nighttime sleepiness. As such, individual monitoring by neurologists of both nighttime sleep and daytime activity/rest is necessary to gain a complete picture of recovery.
Which measures to use?
In conducting a sleep evaluation, neurologists might ask themselves the following questions: (1) What types of sleep issues is the individual reporting? (2) How long has he or she been reporting sleep issues? (3) Have the reported symptoms changed over the course of treatment? (4) Would it be useful or feasible to monitor this individual's sleep habits over time? For example, if a person responds to “I'm sleeping more than usual” on the ImPACT, a follow-up with assessment of daytime sleepiness as well as nighttime patterns would be indicated. Alternatively, if a person indicates that he or she has difficulty falling asleep at night but takes many naps throughout the day, a clinician may choose to implement a sleep and rest diary or daytime activity monitoring to measure daytime vs nighttime sleep behavior.
In addition to a patient's reported sleep symptoms, neurologists may also take practical considerations into account when choosing how to monitor sleep behavior: (1) Will you see the patient once or will he or she return for follow-up appointments? (2) How much time will you have to assess sleep during each individual appointment? (3) How much time will you or an additional clinician have to score or interpret sleep data? (4) Are free or low-cost measures preferred or are more expensive, high-tech options available to you or the patient?
In the event that this patient is seen on a one-time basis, the neurologist may decide to give a few short, state-based sleep questionnaires to assess both insomnia and daytime sleepiness. However, if patient is seen on several occasions over the coming weeks, the neurologist may choose to administer both state-based questionnaires and continuous sleep measures. This would include administering self-report questionnaires at each appointment, based on the patient's reported symptoms. In regards to continuous sleep monitoring, the clinician would present and explain the use of a daily sleep diary that a patient would complete at home, in between appointments, and would bring back on subsequent appointment. Sleep diaries, such as the popular Consensus Sleep Diary, provide data related to nighttime sleep behavior and daytime napping, but can also track other health behaviors such as daily caffeine and alcohol use.10 Alternatively, or in addition to sleep diaries, if a patient owns an actigraphy device such as a FitBit, Jawbone Up bracelet, or Garmin Vivofit, or the facility has access to similar devices, the neurologist may choose to incorporate high-tech options into patient care and continuous sleep and activity monitoring. An added benefit of using objective and automatic sleep/activity monitoring over self-report diaries is the lessened cognitive demand on patients in regards to memory, language, planning, and organizational abilities. Especially in instances when patients are still highly symptomatic, reducing cognitive burden may be of primary concern.
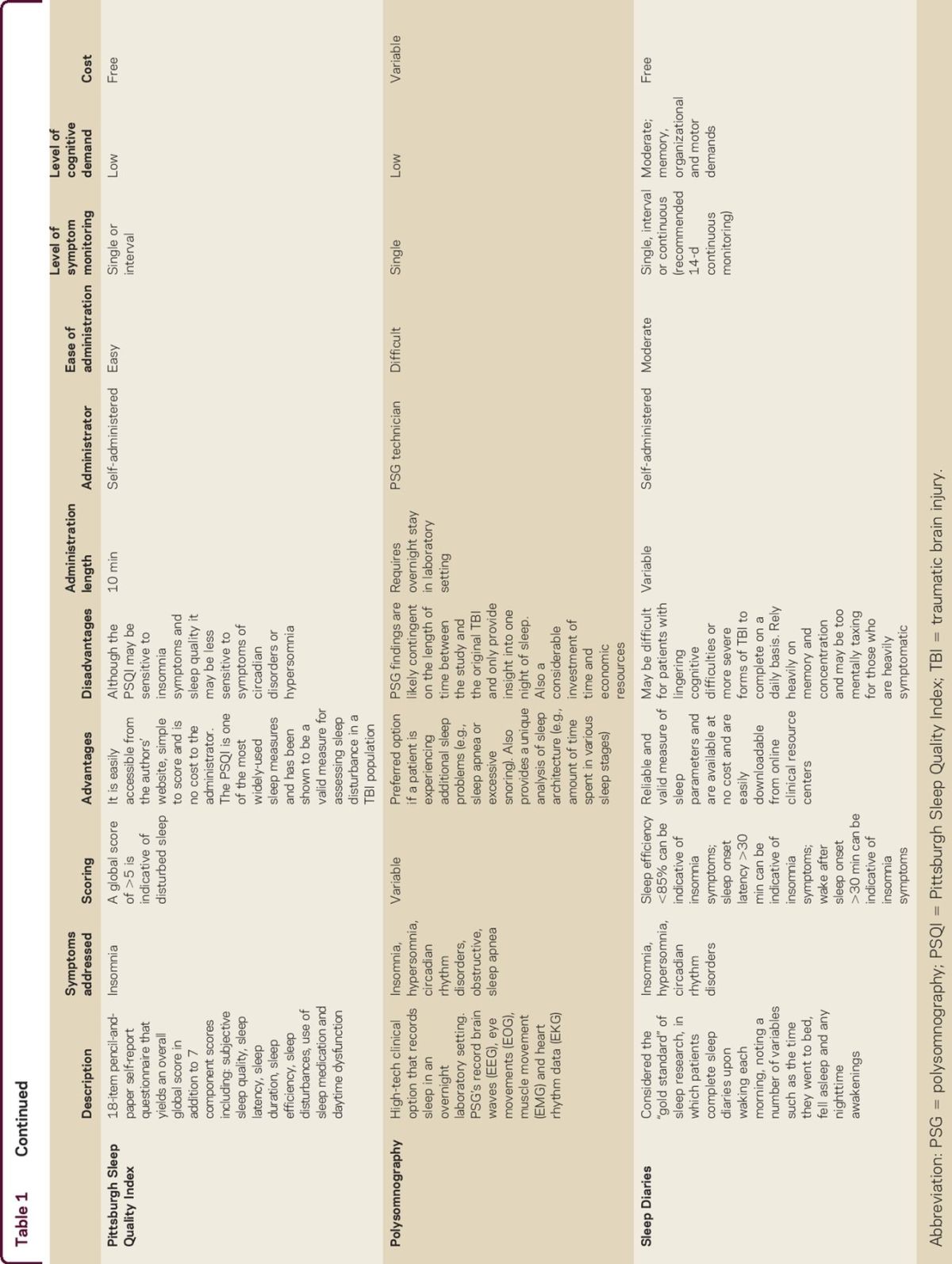
In light of the need for a more complete assessment of sleep behavior in concussed populations, we present a summary of commonly used sleep questionnaires and technologies that can be used with concussion patients (table). These measures were specifically selected due to their user-friendliness, availability, and psychometric soundness, as well as their adaptability to be used with a brain-injured population. Assessment may aim to estimate sleep behavior in an abbreviated time span or may aim to measure sleep behavior on a more long-term basis. The sleep measures discussed will provide both useful and flexible options in regards to cost, availability, and administration time for clinicians aiming to more carefully and systematically assess sleep in concussion patients. We chose to only include measures that are most relevant to reported postconcussion sleep issues (insomnia, hypersomnia, circadian dysrhythmia, and daytime sleepiness). There are a number of additional popular sleep measures, such as the Karolinska sleepiness scale,11 Sleep Timing Questionnaire,12 and additional fatigue measures also available to clinicians.
Table 1.
Summary chart of common sleep measures

Sleep and activity measures
In this section, the measures presented in the table are described specifically.
ImPACT symptom checklist
The symptom checklist in the widely used ImPACT8 for concussion addresses a number of common post-TBI symptoms, including sleep and daytime fatigue. The symptom checklist assesses the following sleep behaviors: (1) drowsiness, (2) trouble falling asleep, (3) sleeping more than usual, and (4) sleeping less than usual. The ImPACT Symptom Checklist and neurocognitive subtests have been shown to be both reliable and valid.13
Pittsburgh Sleep Quality Index (PSQI)
The PSQI14 is an 18-item pencil-and-paper self-report questionnaire that assesses a variety of sleep-related behaviors including time to fall asleep, estimated total amount of sleep last night, sleep disturbances, reported sleep quality, and use of sleep medication. It yields an overall global score ranging from 0 to 21 as well as 7 component scores that assess the following domains: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. It has consistently been shown to be both a reliable (α = 0.83) and valid measure of sleep disturbance.14
Epworth Sleepiness Scale (ESS)
The ESS15 is a quick, simple, reliable (α = 0.82), and attainable self-administered questionnaire aimed to measure general daytime sleepiness. The 8-item questionnaire asks how likely a person is to fall asleep during daily activities such as driving and watching television.
Polysomnography (PSG)
PSG is a more expensive, high-tech clinical option in which a patient's sleep is recorded in an overnight laboratory setting. PSGs record brain waves (EEG), eye movements (electro-oculography), muscle movement (EMG), and heart rhythm (ECG) data. A novel alternative of at-home PSG monitoring, also known as ambulatory PSG, has also recently become available to many sleep specialist clinics. Although PSG can inform clinicians of a patient's sleep architecture or the presence of sleep apnea symptoms, typical PSG patterns of post-TBI patients have been conflictive. While some reports indicate greater slow-wave sleep post-TBI, other studies report no significant changes in sleep architecture.
Actigraphy
Actigraphs are small, noninvasive units usually worn on a patient's wrist aimed to measure gross motor activity. Although traditional actigraphs can be expensive and are mainly used for research purposes, newer devices such as the FitBit can offer activity and rest monitoring at a competitive price point. Actigraph technology varies by device model; while some devices use pedometer technology (usually worn around the waist), accelerometers are usually worn on the wrist or ankle to track movement.
Sleep diaries
Sleep diaries are considered the gold standard of sleep research and offer a simple, low-tech answer to the need for extended sleep behavior monitoring.10 Patients complete sleep diaries upon waking each morning, noting a number of variables such as the time they went to bed and fell asleep and any nighttime awakenings. Patients are usually asked to complete sleep diaries for at least 14 days, though they can continue to be used on an as-needed basis or through the length of treatment. The diaries provide information that can be calculated to estimate total sleep time, time in bed, and sleep efficiency. They also estimate a person's daily napping behavior and caffeine/alcohol use.
Insomnia Severity Index (ISI)
The ISI16 is a 7-item self-report questionnaire aimed to evaluate sleep difficulties related to insomnia. It demonstrates good reliability and validity and is sensitive to perceive changes in sleep behavior over time (e.g., following targeted sleep treatment). The literature suggests that it is a valid tool for use both as an initial screening measure but also as an outcome measure to evaluate posttreatment insomnia symptoms.16
Measures of fatigue
Many health care providers use fatigue questionnaires (such as the Multidimensional Fatigue Inventory17) with concussion patients, who often report symptoms of fatigue, irritability, and daytime sleepiness. However, fatigue questionnaires are not commensurate with reported sleep behavior or daytime sleepiness and additional sleep questionnaires are highly recommended.
Considerations in using traditional and novel sleep technologies in clinical settings
In answering the question regarding the types of sleep measures available to neurologists, there exist a number of both of low-tech and high-tech options. Traditional pencil-and-paper sleep measures provide several benefits to clinicians. Although the majority of standard sleep measures do not provide continuous monitoring of sleep behavior, the measures described above can provide a good overview of clinical sleep symptoms and can alert clinicians to any serious sleep disturbances at an initial intake appointment. If a clinician sees a patient on several occasions, most measures, such as the ESS and ISI, can be readministered to track symptoms or posttreatment outcomes over time. Moreover, for those who wish to address sleep specifically but are new to sleep assessment, most of the previously mentioned traditional sleep measures are user-friendly and easy to obtain from the publisher's Web site at little to no cost. Finally, for those who have concerns regarding the burden of administering self-report questionnaires to a concussed population, most pencil-and-paper questionnaires are short and quick to complete. As an added benefit to the clinician, these assessments are equally as simple to score and scores are often easy to interpret in terms of assessing clinical severity of symptoms.
Newer activity-monitoring technologies such as the FitBit and other devices can be particularly useful in outpatient settings as they fill a notable gap in continuous symptom recovery monitoring. Similarly, they may be appropriate in inpatient rehabilitation settings if the patient's level of insight allows him or her to use the device appropriately. Traditionally, state-dependent symptom measures were all that were available to clinicians. Continued monitoring of symptom recovery including sleep and activity, though extremely important to concussion recovery, is largely absent from current treatment protocols. These newer technologies, however, may serve as a complement to typical treatment in offering continuous sleep and activity monitoring that is independent of a patient's self-report of concussion symptoms. Obtaining continuous, objective data of a patient's sleep and activity is particularly important in concussion patients, where sleepiness and activity level can change on a daily basis and can be indicative of recovery. Moreover, sleep and activity behavior can be assessed outside of the health care facility and can be monitored at home, work, or school. Finally, this technology may have considerable effect on treatment planning. Clinicians can identify specific, objective sleep patterns and aim to adjust any noted sleep disturbance issues. There may also be a greater patient buy-in in that the data are easily accessible to patients and the devices are aimed to promote greater health behavior awareness.
Additional clinical considerations
In treating sleep disturbance in an outpatient concussion population, neurologists may also find themselves asking, “When do I refer to a sleep specialist?” It is important to note that empirical data to guide the answer to this question are limited, making it difficult to determine when a referral is necessary. Anecdotally, neurologists consider the persistence and severity of sleep disturbance symptoms in the context of other postconcussion symptoms. According to DSM-5 criteria,18 insomnia disorder (episodic) would not be diagnosed until after 4 weeks, and chronic insomnia disorder would not be diagnosed unless symptoms persisted for 3 months or longer. At minimum, self-monitoring (via the use of sleep diaries, for example) may be prudent to determine the nature and severity of symptoms over the first few weeks postconcussion. Neurologists might use the following guidelines to aid in their decision: (1) The person's sleep disturbances have not improved or have worsened over the course of treatment. (2) The person's sleep problems are likely indicative of a sleep disorder such as hypersomnia, insomnia, circadian rhythm disorder, or sleep apnea. (3) If the clinician is uncomfortable with treating reported sleep problems, believes the patient's sleep issues are outside the scope of his or her clinical practice, or if patient's self-report sleep measure scores fall within a clinically elevated range (see table), he or she may refer to a sleep specialist. Sleep specialists can provide a comprehensive sleep assessment (including a PSG if indicated), determine the presence and severity of a sleep disorder, and initiate pharmacotherapy or behavioral sleep medicine strategies.
It is also important to note the distinction between the acute phase of concussion recovery and postconcussive syndrome. Literature on acute concussion symptom management is scant and there remain few guidelines for treating postconcussion syndrome. While further research is needed on sleep interventions in concussed patients, such strategies (e.g., cognitive-behavioral therapy for insomnia) are known to both improve sleep and alleviate related symptomatology, even in patients with comorbid medical and mental health conditions (i.e., chronic pain and depression19). Given that emerging literature suggests neuropsychiatric reasons for development of postconcussion syndrome, targeted approach of both concussion and mental health concerns through behavioral and pharmacologic treatments may of particular benefit in those diagnosed with postconcussion syndrome.
Though some of this information may be applied to inpatient rehabilitation patients, this article is largely aimed at concussed outpatients with few other comorbid medical concerns. Additional information on sleep disorders can be found in DSM-5,18 ICD-10,20 or in a number of review articles.21
Take-home points
Sleep disturbance is prevalent and persistent after concussion.
Because duration, pattern, and severity of sleep disturbances are likely to vary among patients, neurologists should become familiar with the breadth of sleep metrics that are currently on the market.
There are a number of options available, both high- and low-tech, which can be used to monitor a patient's disturbed sleep over the course of concussion recovery.
AUTHOR CONTRIBUTIONS
C. Mosti was responsible for the original idea for the paper and for writing the majority of the manuscript. M. Spiers was responsible for continued edits on the paper and for substantial idea contribution. J. Kloss was involved with the ongoing editing process and contributed substantial input to the paper as it related to the sleep measures.
STUDY FUNDING
No targeted funding reported.
DISCLOSURES
The authors report no disclosures. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
REFERENCES
- 1.Ouellet MC, Morin CM. Subjective and objective measures of insomnia in the context of traumatic brain injury: a preliminary study. Sleep Med 2006;7:486–497. [DOI] [PubMed] [Google Scholar]
- 2.Clinchot DM, Bogner J, Mysiw WJ, Fugate L, Corrigan J. Defining sleep disturbance after brain injury. Am J Phys Med Rehabil 1998;77:291–295. [DOI] [PubMed] [Google Scholar]
- 3.Ouellet MC, Savard J, Morin CM. Insomnia following traumatic brain injury: a review. Neurorehabil Neural Repair 2004;18:187–196. [DOI] [PubMed] [Google Scholar]
- 4.Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology 2007;68:1136–1140. [DOI] [PubMed] [Google Scholar]
- 5.Orff HJ, Ayalon L, Drummond SP. Traumatic brain injury and sleep disturbance: a review of current research. J Head Trauma Rehabil 2009;24:155–165. [DOI] [PubMed] [Google Scholar]
- 6.Bodin D, Yeates KO, Klamar K. Definition and classification of concussion. In: Apps JN, Walter KD, eds. Pediatric and Adolescent Concussion: Diagnosis, Management, and Outcomes. Berlin: Springer; 2012:9–19. [Google Scholar]
- 7.McCrory P, Meeuwisse W, Aubry M, et al. Consensus statement on concussion in sport: the 4th international conference on concussion in sport held in Zurich, November 2012. Phys Ther Sport 2013;14:e1–e13. [DOI] [PubMed] [Google Scholar]
- 8.Lovell MR, Collins MW, Podell K, Powell J, Maroon J. ImPACT: Immediate Post-concussion Assessment and Cognitive Testing. Pittsburgh, PA: NeuroHealth Systems, LLC; 2000. [Google Scholar]
- 9.Maroon JC, Lovell MR, Norwig J, Podell K, Powell JW, Hartl R. Cerebral concussion in athletes: evaluation and neuropsychological testing. Neurosurgery 2000;47:659–669. [DOI] [PubMed] [Google Scholar]
- 10.Carney CE, Buysse DJ, Ancoli-Israel S, Edinger JD, et al. The consensus sleep diary: standardizing prospective sleep self-monitoring. Sleep 2012;35:287–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kaida K, Takahashi M, Åkerstedt T, Nakata A, Otsuka Y, et al. Validation of the Karolinska sleepiness scale against performance and EEG variables. Clin Neuropsychol 2006;117:1574–1581. [DOI] [PubMed] [Google Scholar]
- 12.Monk TH, Buysse DJ, Kennedy KS, Potts JM, DeGrazia JM, et al. Measuring sleep habits without using a diary: the sleep timing questionnaire. Sleep 2003;26:208–212. [DOI] [PubMed] [Google Scholar]
- 13.Schatz P, Pardini JE, Lovell MR, Collins MW, Podell K. Sensitivity and specificity of the ImPACT Test Battery for concussion in athletes. Arch Clin Neuropsychol 2006;21:91–99. [DOI] [PubMed] [Google Scholar]
- 14.Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193–213. [DOI] [PubMed] [Google Scholar]
- 15.Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep 1991;14:50–55. [DOI] [PubMed] [Google Scholar]
- 16.Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med 2001;2:297–307. [DOI] [PubMed] [Google Scholar]
- 17.Smets EM, Garssen B, Bonke B, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res 1995;39:315–325. [DOI] [PubMed] [Google Scholar]
- 18.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed Washington, DC: American Psychiatric Association ; 2013. [Google Scholar]
- 19.Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25:559–592. [DOI] [PubMed] [Google Scholar]
- 20.World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva, Switzerland: World Health Organization; 1992. [Google Scholar]
- 21.Panossian LA, Avidan AY. Review of sleep disorders. Med Clin North Am 2009;93:407–425, ix. [DOI] [PubMed] [Google Scholar]