

Abstract
Transitions of care have emerged as an important point of vulnerability in the health care system where medical errors and clinical deterioration can occur. Most research in the area has focused on non-neurologically ill patients in the postdischarge transition from the inpatient to outpatient clinical environment in part due to the emergence of hospital readmissions reduction programs. A multidisciplinary strategy that addresses several common opportunities for improvement can mitigate the risk to patients during these periods and can serve as an opportunity for neurologists to take the lead in developing systems-based solutions that can ultimately enhance the quality of care for our patients.
Improving transitions of care represents a systems-based approach to quality and safety that remains understudied in patients with neurologic illness, many of whom have unique challenges distinct from other patient populations. Although there are many transitions that can lead to poor patient experience, complications, and outcomes, the transition between the inpatient and outpatient environment remains the focus of most research, with some studies finding up to one-fifth of patients experience an adverse event within 2 weeks of hospital discharge, many of which could be prevented or mitigated with timely intervention.1 These adverse events, which include those related to medication errors, falls, and infections, are costly to the health care system, on the order of $12–$44 billion annually in the United States.2
Challenges in postdischarge transitions
Although not a precise (or even well-validated) measure of assessing the quality of inpatient to outpatient transitions, 30-day hospital readmission rates have focused hospitals and physicians on improving transitions due to looming financial penalties for high readmission rates as well as public reporting of hospital- and disease-specific performance.3 The emergence of a neurohospitalist model as a model of inpatient care in the United States has led to additional challenges since many patients chronically seen in an outpatient neurology practice will not be cared for directly by that same provider during hospitalization.4 This group of physicians, some of whom in academics focus their research on these systems-based problems, stands poised to help develop novel approaches to improving neurologic transitions of care; in turn, this will help minimize the risk of adverse events upon discharge for patients with neurologic conditions including cognitive impairment, a common comorbidity in hospitalized elderly.
The period between discharge and first outpatient appointment is recognized as a particularly vulnerable time for patients when adverse events can occur; patients may be unaware of where to seek help if a question arises or a new event occurs, leading to overuse of emergency department resources or not bringing important clinical changes to medical attention. Following discharge, patients may have tests such as laboratories that will require follow-up and action; therefore, assuring which provider is responsible for addressing these follow-up items in a timely fashion is an important element of safe discharge. Medications, many of which have been changed or started during the hospitalization, remain an important safety concern, with as many as 50% of patients being found to have a clinically important medication error after discharge.5 Studies have suggested that a formal medication reconciliation strategy should be a key element of improving transitions of care, and neurologists should consider partnering with pharmacists and nurses to assure this process takes place before discharge.6
In a world of limited access to busy practitioners in outpatient neurology, especially in underserved communities, simply scheduling a timely appointment upon discharge can be a challenge leading to poor transitions of care. This issue is amplified for evening and weekend discharges, when outpatient offices are closed and the patient cannot be given a specific follow-up plan. Although early postdischarge appointments with primary care physicians are commonly substituted for outpatient neurology visits, these providers lack the expertise to manage complex neurologic problems that have met the bar for inpatient admission and may not be equipped to recognize neurologic changes that require intervention in order to avoid deterioration and possible readmission.
Communication between providers in the form of handoffs remains the primary method to assure continuity, and the potential for error remains substantial. The discharge summary has been shown to be commonly incomplete and may not be dictated in a timely enough fashion to be useful for outpatient providers who see a patient in an expedited manner or receive a call with a postdischarge question. In a systematic review, availability of the discharge summary was low at the first postdischarge visit (12%–34%) and often lacked important information including test results (33%–63%), pending results (65%), and a complete and accurate discharge medication list (2%–40%).7 Standards regarding timeliness, length, and content of these summaries remain undefined in neurology. Ideally, handoffs should take both a written and verbal form at discharge, such as a brief phone call to outpatient providers, although these time-consuming activities continue to disincentivize some physicians from making this practice routine.
Patients with neurologic illness are often not discharged to home. Inpatient rehabilitation and skilled nursing facilities feature physicians and nurses often available on site to help with medication administration and patient monitoring. However, many of these providers lack the expertise in neurologic disorders required to recognize a neurologic change that should prompt a call to the specialty provider. Increasingly, hospitals are attempting to solve this problem by partnering with preferred rehabilitation and skilled nursing facilities to share protocols and establish direct lines of communication with discharging physicians and outpatient specialists in the hopes of minimizing complications and readmissions.
Systems-based solutions to challenging transitions
Most efforts to optimize transitions of care have focused on multicomponent solutions, which include individual providers but are generally spearheaded by the hospital system to address overriding themes that lead to poor outcomes. Key root causes of failed transitions include poor provider communication, ineffective education of the patient and caregivers, lack of timely outpatient follow-up, failure to address comorbid chronic conditions, and lack of community support with inadequate access to care.8 Many models have been published that purportedly address these problems, including the Better Outcomes by Optimizing Safe Transitions project, which includes evidence-based interventions for identifying patients at high risk on hospital admission, targeting risk-specific situations, improving information flow between inpatient and outpatient providers, focusing on patient and caregiver education, and ensuring timely postdischarge follow-up (table 1).9
Table 1.
Examples of potential patient risk factors for adverse events and interventions
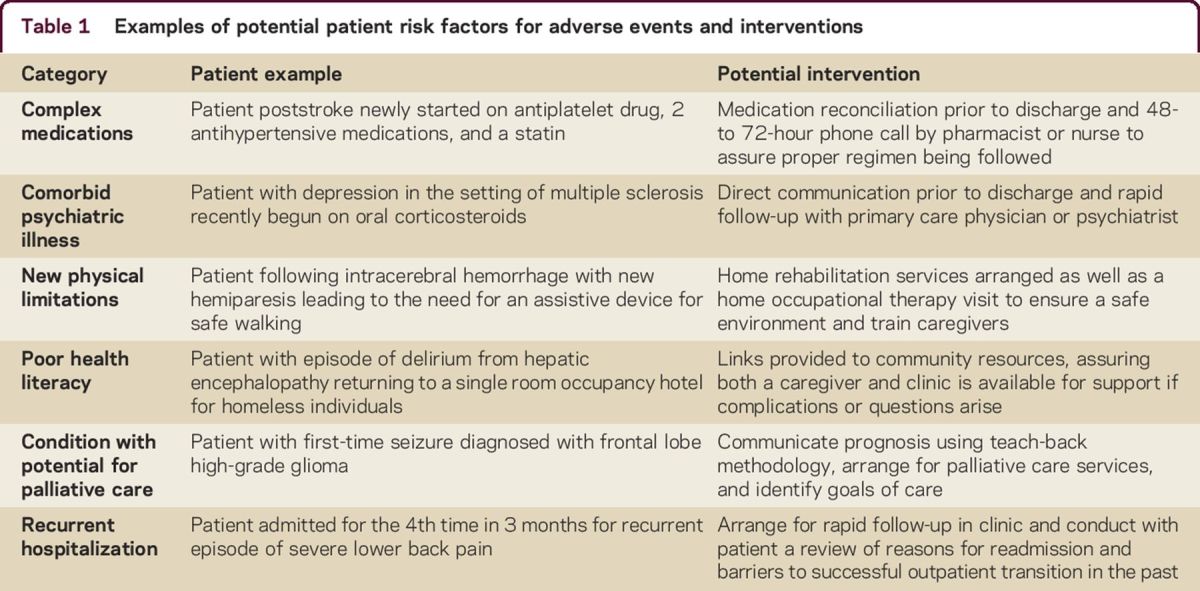
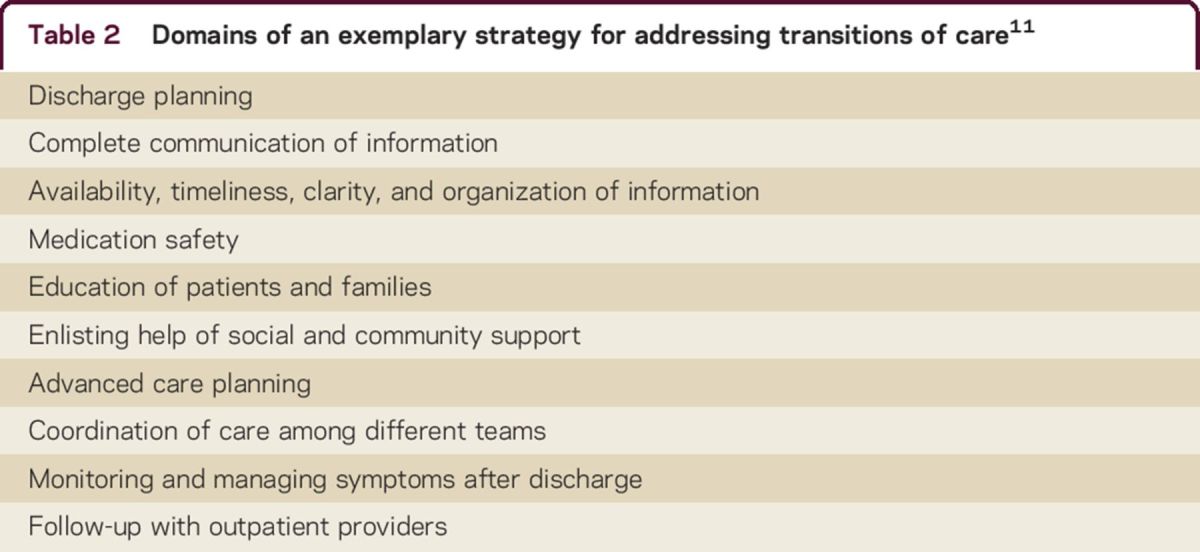
Regardless of the specific method chosen, key elements of any attempt to improve transitions should include institutional support, a multidisciplinary team-based effort, data collection for monitoring achievement of goals, patient and family engagement and education, and standardized discharge pathways. Studies of these programs have been shown in systemic reviews to be limited by sample size and methodologic issues, but moderate evidence exists that these programs can be successful in improving transitions (e.g., health care utilization, patient and caregiver satisfaction, quality of life) when implemented in full.10 An Ideal Transition of Care framework has been developed using expert guidelines and an analysis of the existing literature (table 2).11 A study of available interventions using this framework demonstrated that many attempts to reduce readmissions were unsuccessful because they only targeted a subset of these domains.12 Those elements found to be most associated with reducing readmissions were monitoring and managing systems after discharge, enlisting the help of social and community supports, and educating patients to promote self-management, all aspects that are rarely the focus of neurologists in practice.
Table 2.
Domains of an exemplary strategy for addressing transitions of care11
Although patient education is typically part of inpatient and outpatient neurology visits, standardized approaches and study of their effectiveness is lacking. Refinement of these methods is especially important in a patient population that might not have full capacity to understand complex disorders and explanations due to recent neurologic injury or underlying cognitive impairment. Many neurologic subspecialties including movement disorders, multiple sclerosis, and epilepsy often feature patient and community support groups; however, these groups are not typically part of the inpatient experience nor are they identified upon discharge as an element that can be used to assure patient well-being during transitions.
A number of strategies have been tried in neurologic patients to improve these transitions of care with relatively limited study. Partnerships between inpatient and outpatient practices in community-based and academic settings have attempted to provide continuity and standardize methods of handoffs following discharge. Identification of a single group or single provider in the community who will be able to see patients rapidly can facilitate appointments and allow for a streamlined approach to verbal and written communication regarding the hospital course, medications, and pending results. In situations where the outpatient provider may not have rapidly available access, discharge clinics have been piloted where the inpatient provider oversees 1 or 2 outpatient visits following hospitalization to follow up on tests, assure proper medication administration, and serve as a bridge to establishing or reestablishing care with an outpatient neurologist in the community.13
The day of discharge has been an increasing focus of efforts to improve transitions. Patients should receive education regarding their diagnosis and expected course, including detailing symptoms that should prompt a call to their physician. For example, a patient with newly diagnosed myasthenia gravis should understand warning signs of deterioration including shortness of breath, dysphagia, and increased weakness when brushing hair or walking up steps. Nurses or physicians may utilize a teach-back method whereby patients are asked to summarize the educational information that they have been presented to assure understanding. Medication reconciliation with the patient and family should assure that medications that are to be stopped from admission and those were started during the inpatient stay are recognized by the patient and the family and are promptly available at a local pharmacy for pickup.
Since the day of discharge can be a particular time of information overload, some institutions have piloted discharge phone calls to the patient within 48–72 hours of their last hospital day. During these calls, a nurse or other provider checks in on patients to ensure they are stable and taking their correct medications; patients are asked if they have further questions for their physicians and then put in touch with the discharging team if any information cannot be answered by the caller. If, for example, a patient with stroke has been unable to fill a prescription for antihypertensive medications, the nurse can connect the patient with a pharmacist to rectify the situation. This opportunity also assures that patients have appropriate outpatient follow-up scheduled and that they know how to reach the appropriate provider if a need arises.
Some providers have begun using transitional care management codes to help achieve a higher reimbursement for these postdischarge activities (although substantial regional and payor variability exists). These codes, available since 2013, require physicians to communicate with the patient or caregiver within 2 business days of discharge followed by a face-to-face visit within 7 or 14 days depending on the medical complexity of decision-making.14 Complexities to the coding, including that the bills for these services must typically be submitted on the 30th day after discharge and that only one physician can claim such a code, have limited widespread adoption in practice among neurologists and other specialists.
In internal medicine, common inpatient conditions such as pneumonia, myocardial infarction, and congestive heart failure exacerbations lend themselves well to pathways that can span both the inpatient and outpatient epochs of care, assuring a smooth transition.15 However, neurologic inpatients include a wide range of diverse conditions (e.g., encephalitis, peripheral nerve injury, back pain, metabolic delirium), with few patients having identical diagnoses.16 While pathways may be feasible in stroke or Parkinson disease, our field needs to define common elements of diverse inpatient neurologic conditions that may not be frequent enough to lend themselves to pathway development at individual institutions.17,18 One can imagine a framework, for example, where common neuromuscular admissions for myasthenia gravis, Guillain-Barré syndrome, and rhabdomyolysis share a common pathway and transition to a single outpatient provider or clinic with interest in neuromuscular diseases.
Additional areas of transition
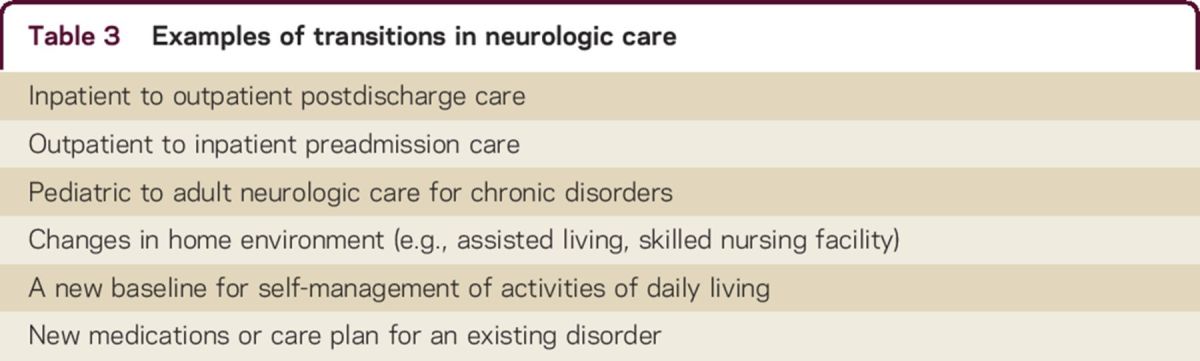
While much of the available literature has focused on these inpatient to outpatient transitions, other types of transitions are equally important and relevant to neurologically ill patients (table 3). The transition from pediatric to adult outpatient care is particularly challenging for young adults with chronic neurologic conditions and remains another point in time when patients are vulnerable due to inadequate handoffs or changing care plans.19 For the patient with a neurologic condition, changes in home environment (e.g., transition to a nursing home) or new adjustments to their independence in activities of daily living (e.g., beginning to use a new assistive device) become transitions that need to be managed effectively by a multidisciplinary group of providers that may include occupational and physical therapists, social workers, nurses, case managers, and physicians.18 Common to all these transitions is an increased potential for emotional distress for the patient, a feature often inadequately addressed by existing interventions.
Table 3.
Examples of transitions in neurologic care
A path forward
Transitions of care have not been the focus of much research or emphasis in neurology until recently. With insurers and governmental agencies identifying transitions as periods where quality of care is assessed and tracked, we as a field need a renewed focus on elements of transitions that are unique to our patient population. As has been the case with other so-called quality markers, initial emphasis nationally has involved only patients with more common medical and surgical disorders, and it remains unclear which of these lessons can be directly applied to our patient population and which require revision when focusing on a specific neurologic patient cohort. Neurologists must take the lead in refining these practices rather than leaving it to policymakers without specialty-specific knowledge and expertise.
Questions that need to be addressed by research include determining the expected rates of readmission among patients with a wide range of neurologic disorders, defining predictors of readmission among these patients, and understanding the proportion of readmissions that are planned vs those that are unplanned and therefore potentially preventable. Examination of international readmission rates may allow us to distinguish between health system–related and disease- or patient-specific contributions to poor transitions of care.20 Other unanswered questions involve which of the proposed multicomponent frameworks for addressing readmissions will be readily adaptable for neurologically ill patients and whether different strategies will be required for a unique patient population.
Practically, physicians caring for patients in the inpatient and outpatient environment alike will need to begin to consider some of these systems-based solutions to transitions of care as an important part of their daily clinical practice along with tracking patients who have had poor transitions of care leading to adverse outcomes. Identifying patients who are at high risk for deterioration following discharge and developing a strategy of intervening proactively to prevent adverse outcomes is an important goal.
Nearly always, these approaches will involve a multidisciplinary team within a larger health care system in which the neurologist plays a central role. For patients with chronic neurologic diseases such as Parkinson disease or multiple sclerosis, the cause of the index admission may not directly be the underlying neurologic disorder, but the neurologist will still need to play an essential part of the transitions process to avoid adverse outcomes. While this team-based approach to care was once considered frequent only in particular neurologic populations (e.g., those with dementia residing in long-term care facilities), it is now increasingly clear that all of our patients deserve a renewed multidisciplinary focus on these times when they are most vulnerable to errors that can contribute to poor quality of life and disease progression. This challenge of managing transitions remains an important one that we all must embrace in the coming years to assure continued high quality care of our patients.
AUTHOR CONTRIBUTIONS
Dr. Josephson designed the study and wrote the initial draft.
STUDY FUNDING
No targeted funding reported.
DISCLOSURES
S.A. Josephson receives personal compensation as Editor-in-Chief of NEJM Journal Watch Neurology and in an editorial capacity for Continuum Audio. Full disclosure form information provided by the author is available with the full text of this article at Neurology.org/cp.
REFERENCES
- 1.Forster AJ, Murff HJ, Peterson JF, Ganghi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med 2003;138:161–167. [DOI] [PubMed] [Google Scholar]
- 2.Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day rehospitalization: a systematic review. Ann Intern Med 2011;155:520–528. [DOI] [PubMed] [Google Scholar]
- 3.Josephson SA, Johnston SC, Hauser SL. The neurologic revolving door: time to pay attention to readmissions. Ann Neurol 2013;73:A5–A6. [DOI] [PubMed] [Google Scholar]
- 4.Josephson SA. Inpatient neurologic care: continued challenges of a neurohospitalist model. JAMA Neurol 2013;70:825–826. [DOI] [PubMed] [Google Scholar]
- 5.Kripalani S, Roumie CL, Dalal AK, et al. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med 2012;157:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kwan JL, Lo L, Sampson M, Shojania KG. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med 2013;158:397–403. [DOI] [PubMed] [Google Scholar]
- 7.Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA 2007;297:831–841. [DOI] [PubMed] [Google Scholar]
- 8.Li J, Young R, Williams MV. Optimizing transitions of care to reduce rehospitalizations. Cleve Clin J Med 2014;81:312–320. [DOI] [PubMed] [Google Scholar]
- 9.Society of Hospital Medicine. Overview: Project BOOST® implementation toolkit. Available at: http://www.hospitalmedicine.org/Web/Quality_Innovation/Implementation_Toolkits/Project_BOOST/Web/Quality___Innovation/Implementation_Toolkit/Boost/Overview.aspx?hkey=09496d80-8dae-4790-af72-efed8c3e3161. Accessed October 15, 2015. [Google Scholar]
- 10.Dy SM, Apostol C, Martinez KA, Aslakson RA. Continuity, coordination, and transitions of care for patients with serious and advanced illness: a systematic review of interventions. J Palliat Med 2013;16:436–445. [DOI] [PubMed] [Google Scholar]
- 11.Burke RE, Kripalani S, Vasilevskis EE, Schnipper JL. Moving beyond readmission penalties: creating an ideal process to improve transitional care. J Hosp Med 2013;8:102–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Burke RE, Guo R, Prochazka AV, Misky GJ. Identifying keys to success in reducing readmissions using the ideal transitions in care framework. BMC Health Serv Res 2014;14:423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Burke RE, Ryan P. Postdischarge clinics: hospitalist attitudes and experiences. J Hosp Med 2013;8:578–581. [DOI] [PubMed] [Google Scholar]
- 14.AAFP. Frequently Asked Questions: Transitional Care Management. Available at: http://www.aafp.org/dam/AAFP/documents/practice_management/payment/TCMFAQ.pdf. Accessed October 15, 2015. [Google Scholar]
- 15.Tingley J, Dolansky MA, Walsh MN. Team-based transitions of care in heart failure. Heart Fail Clin 2015;11:371–378. [DOI] [PubMed] [Google Scholar]
- 16.Douglas VC, Josephson SA. A proposed roadmap for inpatient neurology quality indicators. Neurohospitalist 2011;1:8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Maygers J, Lawrence E, Woolford C, Llinas RH, Marsh EB. Transitions of care: increasing follow-up and decreasing readmission rates after hospitalization for acute ischemic stroke. Stroke 2015;46:ATP341. [Google Scholar]
- 18.Plouvier AO, Olde Hartman TC, van Weel C, Bloem BR, Lagro-Janssen AL. Transitions in Parkinson's disease in primary care: protocol of a longitudinal mixed methods study. BMJ Open 2015;5:e007171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Camfield P, Camfield C. Transition to adult care for children with chronic neurological disorders. Ann Neurol 2011;69:437–444. [DOI] [PubMed] [Google Scholar]
- 20.Kociol RD, Lopes RD, Clare R, et al. International variation in and factors associated with hospital readmission after myocardial infarction. JAMA 2012;307:66–74. [DOI] [PubMed] [Google Scholar]