

Abstract
Although respiratory muscle functions can influence swimming performance, respiratory muscle training (RMT) is not routinely used for improving fin-swimmers´ performance. The aim of our study was to verify the benefit of a one month of RMT in young fin-swimmers. We assessed the effect of this training on respiratory muscles and on maximal underwater swimming distance. 28 fin-swimmers were randomly divided into an experimental group (EG) and a control group (CG). The study finished with 20 fin-swimmers (EG: n = 12; average age 12.0; weight 47.4 kg; height 1.58 m; CG: n = 8; age 11.5; weight 49.6 kg; height 1.53 m). Both group performed regular swimming training, during which the EG used Threshold PEP (positive expiratory pressure) and IMT (inspiratory muscle trainer) for RMT for one month. After one-month washout period, the CG also performed RMT. RMT showed significant improvement of inspiratory muscles in both groups (Z = <1.96; 2.59>; p < 0.05). Significant improvement was observed also in apnoea (AP) max (ZCG = 2.03; p < 0.05; ZEG=2.93; p < 0.01). A long-term effect was observed in the respiratory muscle strength and AP max in the EG (ZEG = 2.52; p < 0.05). RMT in fin-swimmers improves both respiratory muscle strength and the performance in AP max.
Key points.
This study investigated the effect of respiratory muscle training on swimming performance in apnea max discipline in young finswimmers.
Combination of respiratory muscle training with standard finswimming training showed beneficial effect on finswimming performance.
A long-term effect was observed after two months in experimental group of young finswimmers.
Key words: Respiratory muscles, muscle strength, ventilatory parameters, fin swimming, experiment, young athlete
Introduction
Swimming with fins is sport discipline that is carried out both on the surface and under water at 1-2 metres depth. Fin-swimmers practice apnoea performance with a breathing tube or pressurised bottles that they use for a breathing lung regulator. All these methods of swimming put great demands on breathing, the flexibility of the rib cage (Illi et al., 2012), and the strength of the respiratory muscles (Lindholm et al., 2007).
Fin-swimmers need inspiratory power for sufficient inspiration. Expiratory muscle strength is important for breath out against water resistance. Respiratory muscles are not only essential for breathing but they are also involved in the body movement. The auxiliary respiratory muscles are active only when the main respiratory muscles are tired (Pendergast et al., 2015). However, the auxiliary muscles are involved in locomotion and cannot expend all their activity for respiratory functions.
Another important aspect that also affects the respiratory mechanics of fin-swimmers is the racing swimsuit (Pendergast et al., 2006). This type of swimsuit should encircle the body of a fin-swimmer as much as possible, thus causing considerable muscle compression. However, this feature further increases the work the inspiratory muscles must perform. The inspiratory muscles should overcome not only the hydrostatic resistance, but also the resistance from the swimsuit.
Fin swimming is a specific discipline that has been rapidly evolving. The coaches continuously improve training methods and expand the range of resources to improve the athletic performance of their charges (HajGhanbari et al., 2013; Kilding et al., 2010).
Respiratory muscle training (RMT) is mainly used in the field of pulmonary rehabilitation (Elbouhy et al., 2014; Lacasse et al., 1996) but recently it is used more often also in athletes in various types of sports (HajGhanbari et al., 2013; Kilding et al., 2010; Wylegala et al., 2007). Studies have confirmed that RMT also improves RMS and endurance in healthy people and in athletes (Aspenes and Karlsen, 2012; Illi et al., 2012), but fin-swimmers had not been studied yet. From this point of view, if the use of additional RMT can increase the strength of the breathing muscles, it will be easier for fin-swimmers to overcome hydraulic resistance and thus also delay inspiratory muscle fatigue. Another advantage may be an increased expansion of the rib cage, which affects the overall upward push of water on a fin-swimmer. This is especially relevant for the discipline of swimming on the water surface with bi-fins. Swimmers in this discipline aim among others to swim as fast as possible on the water surface where the resistance of the environment, which acts on the swimmers, is the lowest. If a fin-swimmer manages to stretch more of the ribcage, he or she will be more buoyed to the surface. Higher chest expansion associated with increased inspiration can be also beneficial for underwater swimming. We think that our pilot study can uncover new possibilities for training in young fin-swimmers. It is known that the strength of respiratory muscles as well as the strength of other skeletal muscles increases with increasing age during childhood (Wilson et al., 1984). Therefore, RMT can have potential positive effect on their sports performance.
The hypothesis of this study was that RMT applied to standard fin-swimmer training would have a beneficial effect on fin-swimmers´ performance. Therefore, the main aim of our study was to assess the response to RMT in fin-swimmers on their performance in the apnoea (AP) max. The second aim was focused on comparison of maximal inspiratory and expiratory mouth pressures with predicted values for healthy children and on the influence of RMT on RMS in fin-swimmers.
Methods
This randomised, evaluator-blinded, controlled crossover experiment was conducted at the Faculty of Physical Culture, Palacky University in Olomouc, Czech Republic.
Participants
A group of young Czech fin-swimmers learned in advance basic information about the experimental procedure and the purpose of the present study. We obtained signed approval from the participants and their parents together with completed personal questionnaires and the study was approved by the Faculty Ethical Committee.
The mixed-gender group of 28 youth swimmers was randomly divided into an experimental (EG; n = 14) and a control group (CG; n = 14). Each fin-swimmer had to choose an envelope, which contained either number 1 or number 2. Fin-swimmers who chose an envelope with number 1 were assigned to the experimental group while fin-swimmers who chose an envelope with number 2 were assigned to the control group. Inclusion criterion for both groups was participating in fin-swimming training in a swimming Club twice a week for at least two years. The exclusion criteria for both groups were any kind of chronic or acute diseases to avoid the possible effect of diseases on fin-swimmers’ performance and RMS which could negatively affect the results of this study.
After a preliminary examination and the first month of training, they were reduced to 20 participants (EG: n = 12; average age: 12.0 ± 1.7 years; height: 1.58 ± 0.11 m; weight: 47.4 ± 10.5 kg) (CG: n = 8; average age: 11.5 ± 2.4 years; height: 1.53 ± 0.18 m; weight: 49.6 ± 17.0 kg) (Figure 1).
Figure 1.
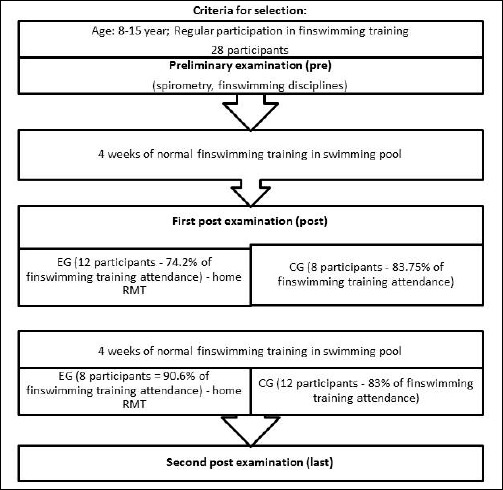
Scheme of experiment design (EG – experimental group; CG – control group).
Those in the EG performed regular swimming training with daily RMT for 1 month. Participants in the CG had only regular swimming training. After the EG finished the experimental training, ventilatory parameters and fin-swimmer discipline were measured in both groups. After 1-month washout period, the CG started the experimental 1-month training with breathing devices during regular swimming training. Final assessment was same in both groups as the initial assessment.
Measurements
Pulmonary function tests: Ventilatory parameters were measured with a Zan 100 USB Spirometer (nSpire Health Inc., Oberthulba, Germany) according to the guidelines of the American Thoracic Society (American Thoracic Society, 1991). The vital capacity (VC), forced vital capacity (FVC), inspiratory capacity (IC), forced expiratory volume in 1 second (FEV1), and peak expiratory flow (PEF) were measured in both groups. The values were expressed as a percentage of the predicted values.
Maximal inspiratory and expiratory mouth pressures: RMS was assessed in both groups 1 week before the experiment started (preliminary examination) and 1 week after it finished (post examination) and 1 week after the crossover experiment (last examination) using the Zan 100 Spirometer in both groups. Maximal inspiratory and expiratory mouth pressures were used for the RMS evaluation. Every participant was individually instructed on how to perform the correct breathing manoeuvres for the maximal mouth inspiratory (PImax) and expiratory (PEmax) pressure measurements. The measurements were performed in an upright sitting position with maximal respiratory effort and with a pause between each test. At least 3 acceptable measurements were taken and the measurement was finished when we had the 2 highest values that had less than 10% of variation. The best value from these was used for further analysis. The PImax and PEmax values were expressed as a percentage of the predicted normal values for further analysis (Wilson et al., 1984).
Swimming performance: In this present study, a 50 m long indoor pool was used. In the same interval (pre, post, and last), the coach measured the maximal length of underwater swimming that swimmers were able to swim for one inspiration. This test is called apnoe max test (AP max). Because underwater swimming could be influenced by pre-dive hyperventilation, it was controlled in each subject. The length was measured using signs in metres on the edge of the pool. During the month of training, both groups practiced the same amount with training loads 3 to 5 times per week (3 for younger swimmers and 5 for older ones) in a 50 m swimming pool. We also collected evidence of their attendance at training sessions.
Respiratory muscle training: The EG used Threshold IMT (inspiratory muscle trainer) and Threshold PEP (positive expiratory pressure) devices (Philips Respironics, Andover, MA, USA) daily for 1 month of respiratory muscle endurance training (RMET) and respiratory muscle strength training (RMST) at home. The resistances on the devices were adjusted at 30 % of their maximum measured values PImax and PEmax during the initial assessment (Sasaki et al., 2005). Every week the initial value of resistance was increased by 2 cm H2O. When the participants reached the maximal possible resistance on the devices, they trained at this maximal resistance on the devices for the rest of the training period.
Each participant used both respiratory devices every day. RMST involved 10 repetitions of maximal inspiration with the Threshold IMT and 10 repetitions of maximal expiration with the Threshold PEP wherein the participant had to overcome a given threshold and sustain to generate flow (McConnell and Romer, 2004). RMET lasted 15 minutes for each device and the task was to breathe continuously against the resistance.
Participants recorded each training day into a dairy with notes about their feelings during RMT.
Data analysis
We obtained data from preliminary, post, and last examinations of maximal inspiratory and expiratory mouth pressures and analysed the average values. Data were expressed as a percentage of the norm. For underwater swimming, we analysed the length in metres (median and interquartile range). For comparison of the values from the same group (repeated) we used the Wilcoxon signed-rank test and the effect size coefficient d [d ≥ 0.80 – large effect; d ϵ < 0.50-0.80 ) – moderate effect; d ϵ < 0.20-0.50 ) – small effect] (Cohen, 1988). For comparison of the values between EG and CG we used Mann-Whitney U test.
Results
Ventilatory parameters
Ventilatory parameters reached normal values in both groups. In the EG, all ventilatory parameters were higher after RMT but the improvement was not significant (Table 1). Similarly, forced expiratory volume in 1 second and peak expiratory flow were higher after RMT in the CG but the difference was not significant (Table 1).
Table 1.
Changes in ventilatory parameters in the EG and CG after RMT.
| Ventilatory parameters (% of predicted) | EG | CG | ||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| VC | 103.8 | 105.1 | 112.6 | 110.6 |
| IC | 107.2 | 107.6 | 117.4 | 116.4 |
| FVC | 102.8 | 104.5 | 114.9 | 112.6 |
| FEV1 | 104.5 | 104.8 | 115.6 | 118.3 |
| PEF | 87.9 | 95.3 | 91.1 | 100.3 |
VC – vital capacity, IC – inspiratory capacity, FVC – forced vital capacity, FEV1 – forced expiratory volume in 1 second, PEF – peak expiratory flow
Maximal inspiratory and expiratory mouth pressures
From the preliminary examination and the comparison with predicted values for a healthy population, 75% of participants reached the values above 100% of PImax and 46% of participants reached the values above 100% of PEmax. Only 7% of participants reached lower PImax values than 80% of predicted values, and 21% of participants had reduced strength of expiratory muscles.
In the EG, after a month of RMT PImax value increase significantly (20.8%) and PEmax value increased by 10.6%, which meant that strength of inspiratory and expiratory muscles improved (Table 2). We also found significant differences in PImax (13.4%) and PEmax (23.1%) parameters in the CG, which used RMT in the next training period.
Table 2.
Differences in average results in pre, post and last examination of respiratory muscles parameters in the EG and CG.
| EG (n = 12) | CG (n = 8) | |||||
|---|---|---|---|---|---|---|
| Mdn (IR) | Z | d | Mdn (IR) | Z | d | |
| PImax % pre | 124.13 (52.80) | 2.401* | 1.451### | 147.46 (48.21) | 0.281 | 0.141 |
| PImax % post | 167.47 (64.75) | 1.332 | 0.802## | 145.13 (43.22) | 1.962* | 0.982### |
| PImax % last | 157.80 (64.73) | 2.583** | 1.563### | 171.22 (54.17) | 2.103* | 1.483### |
| PEmax % pre | 99.48 (28.07) | 1.691 | 1.021### | 100.78 (30.34) | 0.561 | 0.281# |
| PEmax % post | 110.86 (46.96) | 0.272 | 0.162 | 99.63 (37.40) | 2.102* | 1.052### |
| PEmax % last | 108.13 (42.94) | 1.693 | 1.023### | 121.96 (48.30) | 1.823 | 1.293### |
PImax – maximal inspiratory mouth pressure; PEmax – maximal expiratory mouth pressure; % – percentage of predicted value; Mdn – median; IR – interquartile range; 1 difference between pre and post examination; 2 differences between post and last examination; 3 difference between pre and last examination; Z – Wilcoxon pair test; d – Cohen’s coefficient of effect size;
* p < 0.05
# small effect
## moderate effect
### large effect.
In the CG, after the first month of normal water training, we observed a non-significant increase in the inspiratory parameters PImax, but a small negative effect in the expiratory parameters PEmax that decreased.
When we compared all values of PImax and PEmax (pre, post and last) between EG and CG we found large effect in PImax parameters after first month (post: d = 1.28) and small effect after the second month (last: d = .49); in PEmax parameters we found medium and large effect in post and last measurements (post: d = .49; last: d = 1.19).
Sport performance results
Differences in the AP max in EG were significant, had a large effect size between the pre- and post-measurements. The length the fin-swimmers were able to swim for one inspiration increased by 11.36 metres (27.4%). At the last measurement, the results were slightly worse but compared to the preliminary and last measurements, the difference was significant, with a large effect size (9.45 metres) (Table 3).
Table 3.
Differences in average results of pre, post and last examination of sport performance in finswimming discipline in the EG and CG.
| EG (n = 12) |
CG (n = 8) |
|||||||
|---|---|---|---|---|---|---|---|---|
|
Mdn (IR) |
M (SD) |
Z | d |
Mdn (IR) |
M (SD) |
Z | d | |
| AP max pre [m] | 35.00 (13.00) |
41.55 (13.20) |
28.50 (28.00) | 40.63 (18.67) | ||||
| AP max post [m] | 50.00 (22.00) |
52.91 (16.32) |
2.931** 2.032* 2.203* |
1.691### 1.172### 1.273### |
45.00 (14.00) | 44.00 (11.49) | 2.031* 1.412 1.463 |
1.431### 1.002### 1.033### |
| AP max last [m] | 50.00 (16.00) |
51.00 (15.52) |
45.00 (22.00) | 49.75 (13.59) | ||||
AP – apnoea finswimming; Mdn – median; IR – interquartile range; M – mean; SD – standard deviation; 1 difference between pre and post examination; 2 differences between post and last examination; 3 difference between pre and last examination; Z – Wilcoxon pair test; d – Cohen’s coefficient of effect size
* p < 0.05
** p<0.01
### large effect.
In the CG during the first month of training only in the swimming pool, we observed significant improvement in the average length, by 3.37 metres. When comparing preliminary testing and the last measurement after a month of additional respiratory training in the CG, the difference was even more significant, with a large effect size. The length of the distance increased by 9.12 metres (20.7%).
Despite a small sample, we tested also gender differences in AP max. In EG we did not find any significant differences between girls and boys, small differences were found only in CG in second measurement (post) in AP max (p = 0.047). This small variety cannot be probably attributed to gender and hormone influence.
From the diaries recorded by participants every training day, we gathered information that the EG met 95.67% of the training requirements for RMT and the CG met 87.43% of them (the maximum was 28 times). The reasons for not completing the 100% were forgetting, illness, not enough time, school duties, fatigue, and holidays.
Discussion
To our knowledge, this is the first study to determine the effect of RMT in young fin-swimmers. The main aim of our study was to examine the response to RMT in young fin-swimmers on their performance in AP max. Our study confirmed the positive effect of RMT on swimming performance under water and on respiratory muscle strength of young fin-swimmers.
It is important to note that even if RMT is not a standard part of training for fin-swimmers, their breathing is very important. It is well documented that RMT as a part of comprehensive treatment in patients with breathing problems improves exercise tolerance, increases fitness, increases RMS, improves ventilatory parameters and reduces breathing problems (McConnell, 2013). The effect of RMT on RMS and sport performance has also been confirmed in a number of previous studies that have focused on this type of training in healthy athletes, but there has not been performed any study in young fin-swimmers yet (Aspenes and Karlsen, 2012; Markov et al., 2001; McConnell and Romer, 2004; Stuessi et al., 2001; Wilson et al., 1984).
Impact of respiratory muscle training on respiratory muscle strength
Although we assumed that RMS would be sufficient in fin-swimmers, not all participants reached PImax and PEmax values higher than 80% of predicted ones. From this perspective, it can be very beneficial to assess RMS in fin-swimmers to be able to prepare targeted individual training programs for them. We confirmed that RMT improved RMS in young fin-swimmers. All of them reached normal values of PImax after RMT. Only two persons (10%) had slightly decreased PEmax after RMT in comparison with results at baseline assessment, which confirmed decreased PEmax in 21% of fin-swimmers. PImax increased by 20.8% in the EG group after RMT and PEmax increased by 10.6%, whereas in the CG, only 1.5% change was noted for PImax. Furthermore, PEmax decreased by 5.15% in the CG. Contrarily, 13.4% and 23.1% were noted for PImax and PEmax, respectively, in the CG after finishing their RMT program. Significantly improved RMS remained in the EG also after two months, when the experiment had finished.
Our results are in accordance with results of previous studies, which confirmed the positive effect of RMT on RMS in competitive swimmers and divers (Kilding et al., 2010; Lindholm et al., 2007; Wylegala et al., 2007). From our results, we can conclude that RMT is beneficial and useful in top young fin-swimmers.
Impact of respiratory muscle training on swimming performance
We confirmed not only a significant improvement of RMS after RMT, but also an improvement in AP max after a combination of RMT with regular swimming training. The level of physical fitness does not play any role because respiratory muscle performance improves to a similar extent with all the levels of fitness (Illi et al., 2012; Wylegala et al., 2007). Illi et al. (2012) also discussed the age regarding the improvement after RMT and found that the level of fitness is more important than age in affecting the amount of improvement in performance after RMT.
EG significantly improved the length of AP max not only immediately after the 1-month experiment (27.4% and 20.7%) but the effect lasted for a longer time (23% in the EG). Similarly, Lindholm et al. (2007) confirmed that resistive RMT improves underwater fin-swimming endurance in 20-30-year-old fin-swimmers. According to our results respiratory muscular strength training and respiratory muscle endurance training helped fin-swimmers improve respiratory muscle performance and underwater swimming performance, which was confirmed with sustaining in swimming for longer time. We can dispute what type of RMT was more efficient but the results from the studies are not clear, either (Illi et al., 2012). In addition, RMT effectiveness is not dependent on the type of sports.
The effect of improved sport performances could have been also influenced by the duration of the training period or the training intensity. We did not study improvement in each participant separately as some could have showed greater improvement than others could. Their training regime was the same but some other factors, such as age or physical fitness level (Illi et al., 2012) could influence our findings.
The results of this study indicate that targeted RMT improves underwater fin-swimming performance in AP max according to increased RMS and improved respiratory muscle performance.
For fin-swimmers, the experiment extended the possibilities for targeted sport training that was focused not only on swimming performance and general physical fitness but also on respiratory performance. The number of participants corresponded with the size of a sport club in this age category. Even though the sample was not large to obtain reliable results, we randomised participants into two groups and the crossover study was evaluator-blinded. In addition, young age category can be seen as an advantage of our research. Further work can focus on other age categories with regard to gender.
Conclusions
In conclusion, 4 weeks of respiratory muscle endurance and strength training increased respiratory muscle strength and had a positive effect on the swimming performance in fin-swimmers. This study enables coaches and others interested in fin-swimming training to expand their knowledge and training methods, which can positively influence the athletic performance of young fin-swimmers.
Acknowledgements
We would like to thank Mrs Jitka Dostalova for preparation of fin-swimming training program. The study was in accordance with the ethical and law standards on human experimentation and the institutional ethical board approved the study. Authors declare that there is no conflict of interest. The study was supported by the project No. CZ.1.07/2.3.00/30.0004.
Biographies

Jana VASICKOVA
Employment
Associate Professor of Physical Education, Department of Social Science in Kinanthropology, Faculty of Physical Culture, Palacký University Olomouc, Czech Republic
Degree
MSc, PhD
Research interest
Physical activity in youth, physical literacy, sport pedagogy, statistics, sport training.
E-mail: jana.vasickova@upol.cz

Katerina NEUMANNOVA
Employment
Assistant, Department of Physiotherapy, Faculty of Physical Culture, Palacky University Olomouc, Czech Republic
Degree
MSc, PhD
Research interest
The effect of pulmonary rehabilitation on lung function, exercise tolerance and physical activity
E-mail: katerina.neumannova@upol.cz

Zbynek SVOZIL
Employment
Associate Professor of Physical Education, Department of Social Science in Kinanthropology, Faculty of Physical Culture, Palacký University Olomouc, Czech Republic
Degree
PhDr, PhD
Research interest
Physical activity in youth, sport pedagogy, finswimming, sport training.
E-mail: zbynek.svozil@upol.cz
References
- American Thoracic Society. (1991) Lung function testing: Selection of reference values and interpretative strategies. American Review of Respiratory Disease 144, 1202-1218. [DOI] [PubMed] [Google Scholar]
- Aspenes S.T., Karlsen T. (2012) Exercise-training intervention studies in competitive swimming. Sports Medicine 42, 527-543. [DOI] [PubMed] [Google Scholar]
- Cohen J. (1988) Statistical power analysis for the behavioral sciences. 2nd edition. New York, NY: Lawrence Erlbaum Associates. [Google Scholar]
- Elbouhy M.S., AbdelHalim H.A., Hashem A.M.A. (2014) Effect of respiratory muscles training in weaning of mechanically ventilated COPD patients. Egyptian Journal of Chest Diseases and Tuberculosis 63, 679-687. [Google Scholar]
- HajGhanbari B., Yamabayashi C., Buna T.R., Coelho J.D., Freedman K.D., Morton T.A., Palmer S.A., Toy M.A., Walsh C., Sheel A.W., Reid W.D. (2013) Effects of respiratory muscle training on performance in athletes: A systematic review with meta-analyses. Journal of Strength & Conditioning Research 27, 1643-1663. [DOI] [PubMed] [Google Scholar]
- Illi S.K., Held U., Frank I., Spengler C.M. (2012) Effect of respiratory muscle training on exercise performance in healthy individuals. Sports Medicine 42, 707-724. [DOI] [PubMed] [Google Scholar]
- Kilding A.E., Brown S., McConnell A.K. (2010) Inspiratory muscle training improves 100 and 200 m swimming performance. European Journal of Applied Physiology 108, 505-511. [DOI] [PubMed] [Google Scholar]
- Lacasse Y., Wong E., Guyatt G.H., King D., Cook D.J., Goldstein R.S. (1996) Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. Lancet 348, 1115-1119. [DOI] [PubMed] [Google Scholar]
- Lindholm P., Wylegala J., Pendergast D.R., Lundgren C.E.G. (2007) Resistive respiratory muscle training improves and maintains endurance swimming performance in divers. Undersea and Hyperbaric Medicine 34, 169-180. [PubMed] [Google Scholar]
- Markov G., Spengler C.M., Knöpfli-Lenzin C., Stuessi C., Boutellier U. (2001) Respiratory muscle training increases cycling endurance without affecting cardiovascular responses to exercise. European Journal of Applied Physiology 85, 233-239. [DOI] [PubMed] [Google Scholar]
- McConnell A. (2013) Respiratory muscle training. Oxford: Churchill Livingstone. [Google Scholar]
- McConnell A.K., Romer L.M. (2004) Respiratory muscle training in healthy humans: Resolving the controversy. International Journal of Sports Medicine 25, 284-293. [DOI] [PubMed] [Google Scholar]
- Pendergast D.R., Mollendorf J.C., Cuviello R., Termin A.C. (2006) Application of theoretical principles to swimsuit drag reduction. Sports Engineering 9, 65-76. [Google Scholar]
- Pendergast D.R., Moon R.E., Krasney J.J., Held H.E., Zamparo P. (2015) Human physiology in an aquatic environment. Comprehensive Physiology 5, 1705-1750. [DOI] [PubMed] [Google Scholar]
- Sasaki M., Kurosawa H., Kohzuki M. (2005) Effects of inspiratory and expiratory muscle training in normal subjects. Journal of the Japanese Physical Therapy Association 8, 29-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stuessi C., Spengler C.M., Knöpfli-Lenzin C., Markov G., Boutellier U. (2001) Respiratory muscle endurance training in humans increases cycling endurance without affecting blood gas concentrations. European Journal of Applied Physiology 84, 582-586. [DOI] [PubMed] [Google Scholar]
- Wilson S.H., Cooke N.T., Edwards R.H., Spiro S.G. (1984) Predicted normal values for maximal respiratory pressures in caucasian adults and children. Thorax 39, 535-538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wylegala J.A., Pendergast D.R., Gosselin L.E., Warkander D.E., Lundgren C.E.G. (2007) Respiratory muscle training improves swimming endurance in divers. European Journal of Applied Physiology 99, 393-404. [DOI] [PubMed] [Google Scholar]