

CASE REPORT
A 15-year-old female patient underwent in 2012 a right hip surgical dislocation to treat a painful hip affecting her quality of life. Her presenting history, clinical examination and radiological investigations culminated to a diagnosis of intra-articular hip pathology: femoroacetabular impingement which included a femoral head with cam-type morphology and associated labrum tearing extending to the lateral acetabular rim as well as minor subspinal impingement.
Pre-operative plain film radiograph of the patient’s pelvis (Fig. 1) and intra-operative clinical photograph documenting her right hip surgical dislocation and treatment including iatrogenic complete rupture of the ligamentum teres (LT) (Fig. 2).
Fig. 1.

Anteroposterior radiograph of the pelvis.
Fig. 2.
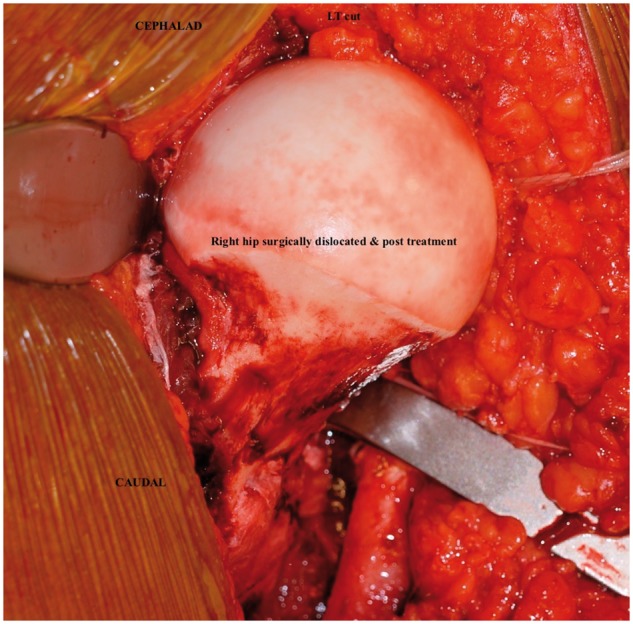
Intraoperative photographs demonstrating the right hip surgical dislocation necessitating complete iatrogenic LT rupture and the femoral head treatment.
Post-operative plain film radiograph of the patient’s pelvis were taken after the procedure (Fig. 3).
Fig. 3.

Plain film depicting both hips. Note the standard two screws in the greater trochanter of right femur after the surgical dislocation.
She went on to have an uneventful recovery immediately after her operation. The trochanteric screws were removed 6 months after the index operation. Regular follow up documents a pain free period of about 3½ years post the right hip surgical dislocation with return to sporting activities and satisfactory quality of life.
In early 2016, the patient started experiencing some pain but mainly limitation in her range of motion of her right hip. Plain film of her pelvis was unremarkable (Fig. 4).
Fig. 4.

Anteroposterior radiograph depicting both hips. Note the absence of the trochanteric screws from the right femur.
The deterioration progressed over time as per serial clinical examinations. Radiological studies supported the suspected clinical suspicion of intra-articular adhesions (Fig. 5), a known complication following surgical hip dislocation [13, 14].
Fig. 5.
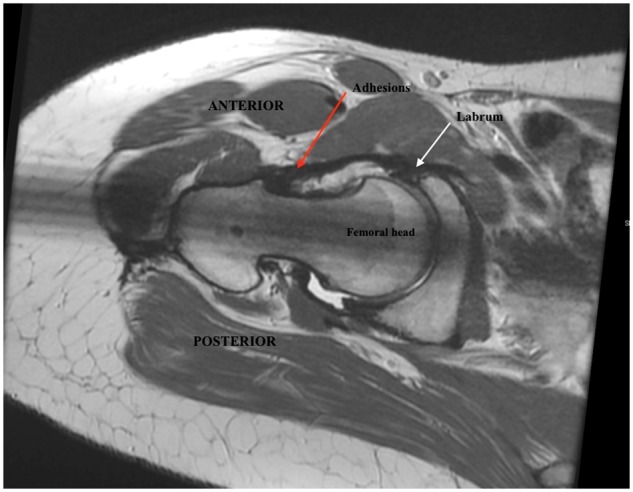
MRI of right hip (sagittal plane) demonstrating adhesions.
Interestingly, the same magnetic resonance imaging (MRI) in a coronal plane demonstrated an LT in continuity (Fig. 6).
Fig. 6.
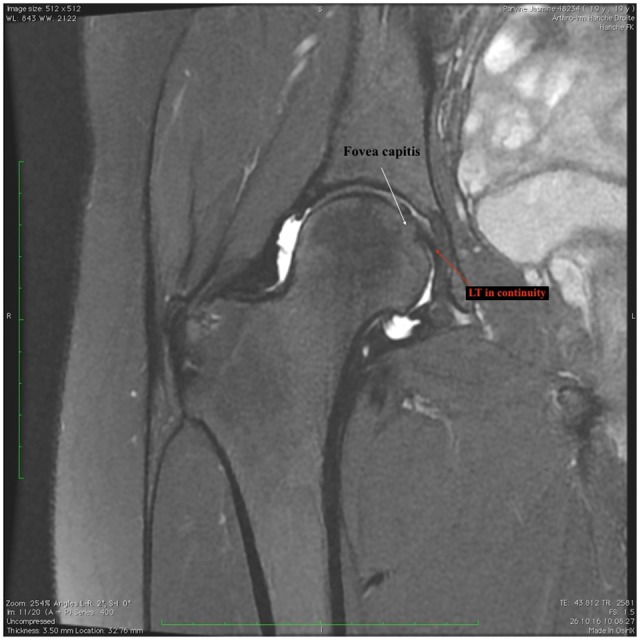
MRI of right hip (coronal plane) demonstrating LT in continuity.
By the end of 2016 symptom progression and clinical deterioration of the patient mandated a second look through an arthroscopic procedure.
The patient underwent a right hip arthroscopy on November 2016, 4 years after the index operation. The diagnosis was confirmed and the adhesions were released arthroscopically. The intra-operative range of movement, specifically the internal and external rotation improved significantly. The patient has had so far an uneventful recovery and was discharged from the hospital the day after her operation.
During her hip arthroscopy, the LT was actually attached and there was no evidence of the initial lesion necessitated by the surgical dislocation (Figs 7 and 8).
Fig. 7.
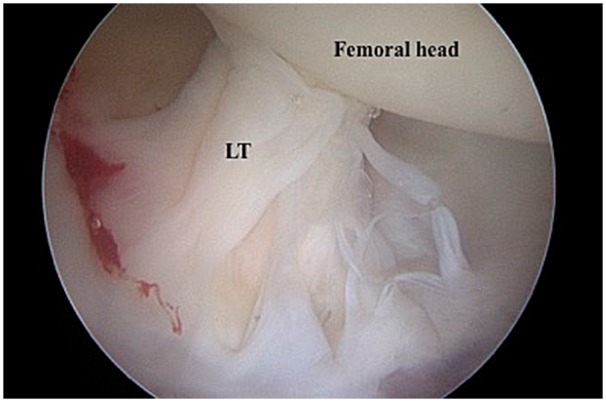
Intra-operative right hip arthroscopy demonstrating LT in continuity.
Fig. 8.
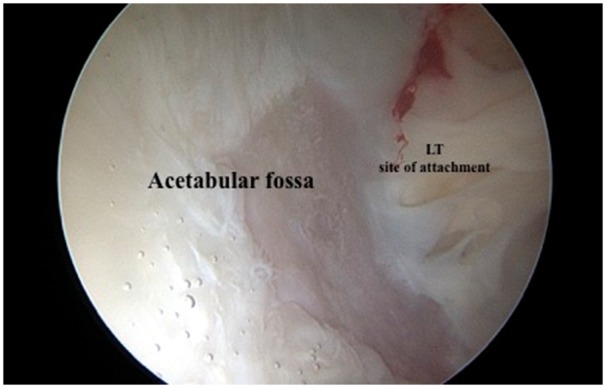
Intra-operative right hip arthroscopy demonstrating satisfactory LT reattachment at the acetabular fossa.
The iatrogenically sectioned LT was in continuity with intact attachments both at the femoral and acetabular sides. The intra-operative photos depict even a somewhat bundled LT appearance as it is described for its native anatomy.
DISCUSSION
This is a case report of an LT in continuity after sectioning by us during surgical dislocation 4 years prior.
Bardakos and Villar [15] reported that Villar had seen four cases of an LT in anatomical continuity after severe injury, including dislocation. O’Donnell et al. [16] have also seen three cases of an apparently intact LT after known rupture and total excision performed previously by them.
This would suggest that the LT does have the potential to heal and reattach. Such ability would reaffirm LT’s greater role in hip kinematics and stability. Yet the biological milieu and mechanical environment required for such regeneration are unknown.
Nowadays, diagnostic or therapeutic arthroscopic hip surgery allows us to take a closer look at this ligament. As we encounter the LT more frequently, we have changed our thinking about its role in hip function.
Our case demonstrates that the LT has the ability to reconstitute after injury. In order to delineate the factors that may lead to this healing potential, we need to focus our attention and understand better the native LT anatomy. And of course define precisely the LT’s role in normal hip joint function and stability at all developmental stages including early development, and during the journey to maturity. That will require better insight at an embryonic state and greater understanding at a molecular level of the makeup of this ligament.
Only then we will be able to speculate with greater confidence on the sequelae of injury of the LT and on those cases where it exhibits abnormal function or it is completely absent. And of course, only then we will be able to design more targeted experiments where the LT is involved in a traumatic insult or it is part of a disease state (i.e. Perthe’s or developmental hip dysplasia).
Finally, the inherent limitations of cases reports are well known. In the background of the anecdotal similar cases from the landmark papers on the topic from Villar et al. and O’Donnell et al. [16] our report is depicting the reconstituted LT during hip arthroscopy 4 years after the index operation. A dynamic video stretching the LT through the range of motion of the hip to determine its functionality would have been interesting. Additionally, we believe that our case report adds validity to these anecdotal aforementioned cases and points to a regenerating/healing pattern of response of the LT to insult when in the appropriate biological and mechanical environment. In the future those conditions remain to be defined more accurately with further scientific experiments and clinical research.
CONCLUSION
Prior to this publication, there have been only anecdotal reports of LT in continuity after severe injuries including dislocation. This is a report of LT in continuity documented during hip arthroscopy 4 years after an index procedure which had required surgical hip dislocation and LT sectioning.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1. Rao J, Zhou YX, Villar RN.. Injury to the ligamentum teres: mechanism, findings, and results of treatment. Clin Sports Med 2001; 20: 791–9. [DOI] [PubMed] [Google Scholar]
- 2. Demange MK, Kakuda CMS, Pereira CAM. et al. Influence of the femoral head ligament on hip mechanical function. Acta Orthop Bras 2007; 15: 187–90. [Google Scholar]
- 3. Walker JM. Growth characteristics of the fetal ligament of the head of the femur: significance in congenital hip disease. Yale J Biol Med 1980; 53: 307–16. [PMC free article] [PubMed] [Google Scholar]
- 4. Chen H-H, Li AF-Y, Li K-C. et al. Adaptations of ligamentum teres in ischemic necrosis of human femoral head. Clin Orthop 1996; 328: 268–75. [DOI] [PubMed] [Google Scholar]
- 5. Brewster SF. The development of the ligament of the head of the femur. Clin Anat 1991; 4: 245–55. [Google Scholar]
- 6. Keene GS, Villar RN.. The arthroscopic anatomy of the hip: an in vivo study. Arthros- Copy 1994; 10: 392–9. [DOI] [PubMed] [Google Scholar]
- 7. Gray AJ, Villar RN.. The ligamentum teres of the hip: an arthroscopic classification of its pathology. Arthroscopy 1997; 13:575–8. [DOI] [PubMed] [Google Scholar]
- 8. Baber YF, Robinson AHF, Villar N.. Is diagnostic arthroscopy of the hip worth- while? A prospective review of 328 adults investigated for hip pain. J Bone Joint Surg [Br] 1999; 81-B: 600–3. [DOI] [PubMed] [Google Scholar]
- 9. Byrd JWT, Jones KS.. Traumatic rupture of the ligamentum teres as a source of hip pain. Arthroscopy 2004; 20: 385–91. [DOI] [PubMed] [Google Scholar]
- 10. Hankenson KD, Turek JJ.. Porcine anterior cruciate ligament fibroblasts are similar to cells derived from the ligamentum teres, another non-healing intra-articular ligament. Connect Tissue Res 1999; 40: 13–21. [DOI] [PubMed] [Google Scholar]
- 11. Wenger D, Miyanji F, Mahar A, Oka R.. The mechanical properties of the ligamentum teres. A pilot study to assess its potential for improving stability in children’s hip surgery. J Pediatr Orthop 2007; 27: 408–10. [DOI] [PubMed] [Google Scholar]
- 12. Leunig M, Beck M, Stauffer E. et al. Free nerve endings in the ligamentum capitis femoris. Acta Orthop Scand 2000; 71: 452–4. [DOI] [PubMed] [Google Scholar]
- 13. Beck M. Groin pain after open FAI surgery: the role of intraarticular adhesions. Clin Orthop Relat Res 2009; 467: 769–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Papavasiliou AV, Bardakos NV.. Complications of arthroscopic surgery of the hip. Bone Joint Res 2012; 1: 131–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Bardakos NV, Villar RN.. The ligamentum teres of the adult hip. J Bone Joint Surg Br 2009; 91: 8–15. [DOI] [PubMed] [Google Scholar]
- 16. O’Donnell JM, Pritchard M, Porthos Salas A. et al. The ligamentum teres—its increasing importance. J Hip Preserv Surg 2014; 1: 3–11. [DOI] [PMC free article] [PubMed] [Google Scholar]