

Abstract
Background
To evaluate the efficacy and safety of an extemporaneous preparation of 2% ganciclovir topical eye drops in cytomegalovirus (CMV) anterior uveitis because many studies have confirmed the benefits of topical ganciclovir in varying concentrations.
Design
The study employed a retrospective cohort design.
Methods
This study enrolled 11 eyes (11 patients) with CMV anterior uveitis. All cases were proved by positive PCR for CMV DNA from aqueous tapping and received topical 2% ganciclovir, applied every 2 hours daily as induction therapy then tapered off and stopped based on clinical response. Outcome measures were best-corrected visual acuity, anterior chamber cell, coin-shaped and other keratic precipitates, intraocular pressure (IOP), the number of antiglaucoma drugs used, the frequency of steroid eye drops used daily and side effects over a 12-month follow-up period. Side effects after applying topical 2% ganciclovir were recorded using questionnaires and eye examination.
Results
Mean age was 49.0±17.8 years. IOP, number of antiglaucoma drugs used and keratic precipitates decreased significantly at first week (p<0.013, p<0.024 and p<0.031, respectively) followed by decreased anterior chamber cells and significantly reduced frequency of applying steroid eye drops at 4 weeks (p<0.034 and p<0.017, respectively). Visual acuity significantly improved at 5 months continuously. All clinical improvement was maintained to 12 months, and keratic precipitates were eliminated in 90% of all cases. However, in 27% of discontinued medicine cases, inflammation was recurrent. No significance was observed in all factors between recurrent and non-recurrent groups. The most common side effect was eye irritation (27.27%). No severe complications from the medicine was detected.
Conclusion
Extemporaneous preparation topical 2% ganciclovir was effective and safely controlled CMV anterior uveitis. The medication is non-invasive, economical and convenient for hospitals where commercial topical ganciclovir is unavailable.
Keywords: cytomegalovirus, anterior uveitis, glaucoma, topical ganciclovir
Key messages.
The treatment of cytomegalovirus (CMV) anterior uveitis with topical ganciclovir gained more popularity. The concentration of this medicine was variedly used.
We reported the efficacy of topical 2% ganciclovir in timeline with safety information in these patients.
The findings suggest that the use of extemporaneous preparation topical 2% ganciclovir could be alternatively employed where commercial topical ganciclovir is unavailable.
Introduction
In the past, the known causes of infectious anterior uveitis in the herpesviridae family1 were only varicella zoster and herpes simplex types 1 and 2. Currently, cytomegalovirus (CMV) anterior uveitis and corneal endotheliitis were increasingly found among immunocompetent patients.2 This increase is probably due to advanced modern investigations such as PCR that are able to detect and confirm the diagnosis of infectious uveitis.3 4 CMV anterior uveitis and corneal endotheliitis present anterior chamber inflammation, increased intraocular pressure (IOP), coin shaped lesions or other keratic precipitates (KPs) and iris atrophy.5–7 The diagnosis of CMV anterior uveitis is based on clinical manifestations and PCR results from the aqueous humour.8–11
To treat CMV anterior uveitis, ganciclovir is a well-known medication used to suppress the replication of the herpes virus.12In the beginning, systemic ganciclovir, such as intravenous ganciclovir2 11 and oral valganciclovir,13 14 were recommended for CMV anterior uveitis. However, they are expensive and present the risk of systemic side effects like granulocytopaenia, thrombocytopaenia, anaemia, azoospermia and rising serum creatinine levels.15 Local ganciclovir therapy has become more popular for producing fewer systemic side effects including intravitreal ganciclovir16 and topical ganciclovir. Many studies have confirmed the benefits of topical ganciclovir in varying concentrations from 0.15% ganciclovir17 18 and 0.5% ganciclovir16 19 to 2% ganciclovir.20 21 Commercial topical 0.15% ganciclovir gel is available in many countries; however, in some countries such as Thailand, it has not been imported yet. Therefore, we aimed to evaluate the efficacy of an extemporaneous preparation of 2% ganciclovir eye drops and to determine its safety features as well.
Methods
Medical records in the Ophthalmology Department of Phramongkutklao Hospital were retrospectively reviewed from January 2013 to August 2016. We enrolled 11 patients presented with anterior uveitis, coin-shaped lesions and other KPs, IOP including subjects with a history of using topical steroids and topical antiglaucoma drugs. All patients underwent aqueous tapping using PCR for seven types of herpes, and the results showed only positive for CMV. Patients had a diagnosis of CMV anterior uveitis or corneal endotheliitis based on clinical manifestations and positive PCR results for CMV DNA from the aqueous humour. Patients were treated with topical 2% ganciclovir prepared from 500 mg of Cymevene IV lyophilised powder (Roch, Basel, Switzerland) in 25 mL of sterile water, at 20 mg/1 mL. The price per bottle was 57 GBP. Because this medicine comprises preservative-free eye drops, it expires within 1 month. Furthermore, patients were informed to keep their medication in a brown medicine bottle and in a cool place (2°C–8°C) all the time. Topical 2% ganciclovir was prescribed to be applied every 2 hours daily as induction therapy for 2 weeks and after that tapering off to every 4 hours, four times daily, three times daily, twice a day, once daily every week and finally stopped based on clinical response.
The collected patient data comprised demographics as well as underlying disease and previous ocular treatment including number of topical steroids and antiglaucoma drugs used. Ophthalmic examinations included best-corrected visual acuity (BCVA) using a Snellen eye chart, anterior chamber inflammation, KPs and IOP using Goldman applanation tonometry before and after treatment monthly. BCVA was converted to logMar to record. In addition, anterior chamber cells were graded using SUN classification.22 Antiglaucoma drugs were recorded by counting the number of medications used while steroid use was recorded by counting the frequency of topical 1% prednisolone acetate or loteprednal eye drops in 1 day.
After the patients had used topical 2% ganciclovir for at least 6 months, they completed questionnaires asking about unexpected symptoms including irritation, redness, foreign body sensation, photophobia, dry eye, blurred vision, abnormal discharge and tearing together with questionnaires asking about characteristics of medication change including change in colour or sedimentation. Side effects from using topical eye drops including discharge, conjunctival reaction, punctate epithelial erosion and epithelial defect were also recorded every visit.
The primary outcome was to evaluate the efficacy of topical 2% ganciclovir, while the secondary outcome was to evaluate its safety. All data were recorded using the STATA/MP V.12 Program. Statistical analysis was performed using IBM SPSS statistics, V.23.
This research was approved by the Phramongkutklao Institutional Review Board. Informed consent was obtained from all patients after receiving protocol information.
Results
Clinical responses to topical 2% ganciclovir
Eleven eyes in 11 patients were enrolled in this study. Patient characteristics and demographic data are summarised in tables 1 and 2. The patients comprised eight men and three women, 28–81 years old (49.0±17.8 years). They had the disease before CMV was detected for a mean of 54.0±54.9 months. Two patients underwent penetrating keratoplasty from unknown corneal decompensate; however, they experienced graft rejection and poor visual outcome later. Three of 11 patients (cases 1, 4 and 8) had previously been treated with another route of ganciclovir before quitting because of financial problems.
Table 1.
Characteristics of patients
| Patient no. | Age/gender | Affected eye |
History of ocular disease | Duration before CMV detection (months) | History of antiviral medication | History of topical antiviral medication |
| 1 | 76/M | Left | – | 57 | Valganciclovir oral | 0.15% Ganciclovir gel |
| 2 | 38/M | Left | – | 12 | – | – |
| 3 | 28/M | Left | – | 18 | – | – |
| 4 | 59/M | Left | Corneal decompensate | 57 | IV ganciclovir | 0.15% Ganciclovir gel |
| 5 | 50/F | Right | – | 204 | – | – |
| 6 | 53/M | Left | Primary open angle glaucoma | 62 | – | – |
| 7 | 52/M | Right | – | 62 | – | – |
| 8 | 41/M | Left | Behcet’s disease on cyclophosphamide | 1 | IVT ganciclovir | – |
| 9 | 33/F | Left | – | 48 | – | – |
| 10 | 81/M | Left | S/P PKP | 60 | – | – |
| 11 | 29/F | Right | S/P PKP | 14 | – | – |
M, male; F, female; IV, intravenous; IVT, intravitreous; S/P PKP, post penetrating keratopathy.
Table 2.
Characteristics of baseline
| n | Mean±SD | Median (min–max) | n (%) | |
| Baseline | ||||
| Age | 11 | 49.09±17.78 | 50 (28–81) | |
| Duration (months) | 11 | 54.09±54.94 | 57 (1–204) | |
| Visual acuity | 11 | 0.61±0.59 | 0.2 (0–1.4) | |
| Cell | 11 | 0.73±1.13 | 0.5 (0–4) | |
| KPs | ||||
| No | 1 (9.10) | |||
| Yes | 10 (90.9) | |||
| IOP | 11 | 26.73±10.42 | 28 (14-44) | |
| Antiglaucoma drug | 11 | 3.00±1.67 | 3 (0–6) | |
| Steroid | 11 | 5.45±4.20 | 4 (2–16) |
IOP, intraocular pressure; KP, keratic precipitate.
Regarding initial clinical presentations (table 3), the average BCVA was 0.2, ranging from 0 to 1.4. Coin-shaped and stellate KPs were detected in 10 eyes (90.9%); mild anterior chamber inflammation was observed in eight eyes (72.7%), while hypopyon was present in one eye (9%) of case 8 receiving oral 2 mg/kg/day of cyclophosphamide therapy. Fundus examinations were normal in all patients. Topical antiglaucoma medications, acetazolamide tablets and 50% glycerine solution were used in 10 patients (90.9%) with an average of three bottles (0.5% timolol, brimonidine and 1% brinzolamide). However, elevated IOPs were still present in six eyes (55%). All cases were using topical steroids, mostly 1% prednisolone acetate except cases 4 and 10 using loteprednal, but at various frequencies, 2–16 times daily to control inflammation.
Table 3.
Clinical manifestations of patients with CMV anterior uveitis included number of antiglaucoma drugs and frequency of steroid eye drops in a day before and after topical 2% ganciclovir therapy
| Patient no. | Clinical before topical 2% ganciclovir |
Clinical after topical 2% ganciclovir 12 months |
Status of topical ganciclovir at 12 months | No. of recurrent | Trabeculectomy with mitomycin C | ||||||||||
| Visual acuity |
Cell | KPs | IOP | G | S | Visual acuity | Cell | KPs | IOP | G | S | ||||
| 1 | 20/25 | 1+ | + | 17 | 3 | 4 | 20/25 | 0 | 17 | 2 | 0 | Off | 1 | ||
| 2 | 20/32 | 0.5 | + | 30 | 4 | 4 | 20/20 | 0 | − | 16 | 1 | 1 | Once a day | 2 | |
| 3 | 20/20 | 0.5 | + | 32 | 2 | 10 | 20/20 | 0 | − | 12 | 0 | 0 | Off | 0 | |
| 4 | 20/60 | 1 | + | 28 | 4 | 2 | 20/25 | 0 | − | 11 | 1 | 0 | Once a day | 0 | |
| 5 | 20/40 | 0.5 | + | 13 | 4 | 4 | 20/25 | 0 | − | 10 | 0 | 2 | Off (at 6 months) |
1 | 9th month |
| 6 | 20/32 | 0.5 | + | 40 | 3 | 6 | 20/20 | 0 | + | 13 | 0 | 0 | Three times a day | 1 | |
| 7 | 20/25 | 0 | + | 14 | 2 | 4 | 20/20 | 0 | − | 8 | 0 | 0 | Three times a day | 1 | |
| 8 | HM | 4+ | − | 33 | 6 | 16 | 20/200 | 0.5 | − | 16 | 2 | 4 | Once a day | 0 | |
| 9 | 20/100 | 0.5 | + | 44 | 4 | 4 | 20/50 | 0 | − | 6 | 0 | 0 | Off | 0 | 2nd month |
| 10 | FC2 | 0.5 | + | 15 | 1 | 4 | HM | 0 | − | 1 | 1 | 1 | Off | 0 | |
| 11 | FC1 | 0 | + | 15 | 0 | 4 | FC1’ | 0 | − | 17 | 2 | 4 | Once a day (6 months) | 1 | |
G, the number of antiglaucoma drugs.
S, the frequency of steroid drops per day.
CMV, cytomegalovirus; FC, finger count; HM, hand motion; IOP, intraocular pressure; KP, keratic precipitate.
Clinical response to topical 2% ganciclovir therapy at 12 months compared with clinical manifestations before starting medication is shown in table 3. All cases showed positive responses to therapy either improved BCVA, decreased anterior chamber cells from 0.5 to 0, eliminated KPs, decreased IOP from 28 to 12 mm Hg, reduced number of antiglaucoma drugs from 3 to 0 bottles and reduced frequency using steroid eye drops from 4 to 0 times daily (tables 4 and 5). Two cases (cases 5 and 9) underwent trabeculectomy with mitomycin C because of uncontrolled IOP and visual field defect progression (18.18%). One case (case 5) discontinued topical 2% ganciclovir at 6 months after the patient decided to choose commercially available 0.15% ganciclovir gel after filtering surgery. One case was lost to follow-up after 6-month visit. At 12 months, 4 of 11 eyes (36%) could discontinue topical 2% ganciclovir, while 5 of 11 eyes (45%) were treated three to four times daily for maintenance therapy. In addition, 6 of 11 eyes (0.55%) used antiglaucoma drugs (0.5% timolol and 1% brinzolamide) long term as well.
Table 4.
Clinical response of 2% ganciclovir eye drop compared with baseline 1 week–6 months
| Baseline | 1 week | 4 weeks | 2 months | 3 months | 4 months | 5 months | 6 months | |
| Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
|
| Visual acuity | 0.2 (0–1.4) | 0.3 (0–1.4) | 0.5 (0–1.1) | 0.2 (0–1.3) | 0.4 (0–1.3) | 0.2 (0–1.1) | 0.2 (0–1.1) | 0.1 (0–1.1) |
| p = 0.031 | p = 0.095 | p = 0.078 | p = 0.065 | p= 0.065 | p= 0.020 | p= 0.011 | ||
| Cell | 0.5 (0–4) | 0 (0–3) | 0 (0–1) | 0 (0–1) | 0 (0–0.5) | 0 (0–2) | 0 (0–1) | 0 (0–1) |
| p = 0.058 | p = 0.034 | p = 0.020 | p = 0.007 | p= 0.008 | p= 0.034 | p= 0.007 | ||
| IOP | 28 (14–44) | 13 (12–20) | 15 (8–18) | 14 (8–16) | 11 (8–24) | 14 (8–16) | 14 (9–29) | 14 (7–18) |
| p = 0.013 | p = 0.012 | p = 0.006 | p = 0.11 | p= 0.005 | p= 0.012 | p= 0.003 | ||
| Antiglaucoma drug | 3 (0–6) | 2 (0–5) | 2 (0–4) | 2 (0–4) | 1 (0–3) | 1 (0–4) | 1 (0–4) | 1 (0–3) |
| p = 0.024 | p = 0.010 | p = 0.011 | p = 0.007 | p= 0.011 | p= 0.011 | p= 0.007 | ||
| Steroid | 4 (2–16) | 4 (0–16) | 2 (0–8) | 2 (0–4) | 2 (0–4) | 2 (0–8) | 2 (0–4) | 1 (0–4) |
| p = 0.176 | p = 0.017 | p = 0.018 | p = 0.11 | p= 0.005 | p= 0.007 | p= 0.005 | ||
| KPs present 10 (90.9%) | 4 (36.36%) | 0 | 0 | 0 | 0 | 1 (9.09%) | 0 | |
| p = 0.031 | NA | NA | NA | NA | p= 0.004 | NA | ||
Wilcoxon signed-rank test.
McNemar test.
Significant (p<0.05).
IOP, intraocular pressure; KPs, keratic precipitates.
Table 5.
Response of 2% ganciclovir eye drop compared with baseline 7 months–12 months
| n | Baseline | 7 months | 8 months | 9 months | 10 months | 11 months | 12 months | |
| Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
Median (min–max) |
||
| Visual acuity | 9 | 0.2 (0–1.4) | 0 (0–1.1) | 0 (0–1.1) | 0 (0–1.1) | 0 (0–1.1) | 0 (0–1.1) | 0 (0–1.1) |
| p = 0.017 | p = 0.017 | p = 0.017 | p= 0.017 | p= 0.017 | p= 0.017 | |||
| Cell | 9 | 0.5 (0–4) | 0 (0–1) | 0 (0–1) | 0 (0–0.5) | 0 (0–0) | 0 (0–0.5) | 0 (0–0.5) |
| p = 0.034 | p = 0.008 | p = 0.021 | p= 0.008 | p= 0.014 | p= 0.008 | |||
| IOP | 9 | 28 (14–44) | 14 (8–17) | 12 (6–18) | 12 (9–17) | 15 (1–24) | 14 (1–24) | 12 (1–17) |
| p = 0.013 | p = 0.011 | p = 0.008 | p= 0.021 | p= 0.018 | p= 0.012 | |||
| Antiglaucoma drug | 9 | 3 (1–6) | 1 (0–2) | 1 (0–2) | 1 (0–2) | 1 (0–2) | 0 (0–2) | 0 (0–2) |
| p = 0.011 | p = 0.011 | p = 0.011 | p= 0.012 | p= 0.007 | p= 0.007 | |||
| Steroid | 9 | 4 (2–16) | 0 (0–6) | 0 (0–4) | 0 (0–4) | 0 (0–4) | 0 (0–4) | 0 (0–4) |
| p = 0.024 | p = 0.012 | p = 0.012 | p= 0.011 | p= 0.016 | p= 0.011 | |||
| KPs present | 9 | 10 (90.9%) | 1 (11.11%) | 0 | 1 (11.11%) | 2 (22.22%) | 2 (22.22%) | 2 (22.22%) |
| p = 0.016 | NA | p = 0.016 | p= 0.031 | p= 0.031 | p= 0.031 |
Wilcoxon Signed-rank test.
McNemar test.
Significant (p<0.05).
IOP, intraocular pressure; KPs, keratic precipitates.
After administering topical 2% ganciclovir, IOP and KPs were rapidly controlled in 1 week with significance (p<0.013 and p<0.031) compared with baseline leading to a decrease in antiglaucoma medication and thereafter significantly (p<0.024) as well (table 4). Anterior chamber cells were significantly controlled at 4 weeks (p<0.034) simultaneously as the frequency of steroid eye drops was significantly reduced (p<0.017). BCVA was the last to improve significantly at 5 months (p<0.020).
At 4 weeks of administering topical 2% ganciclovir, IOP and anterior chamber inflammation were significantly controlled compared with baseline every month regularly. The details of each case are shown in figures 1–11.
Figure 1.
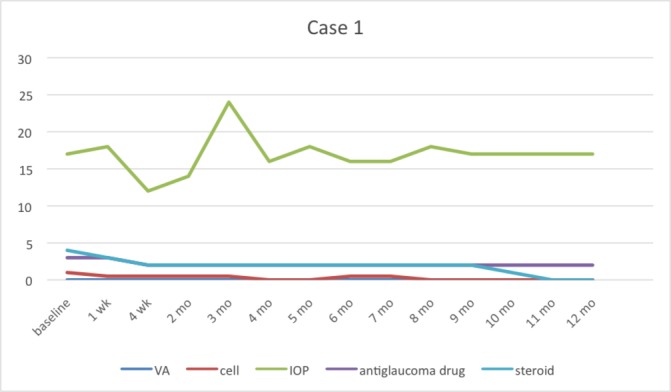
Case 1 had recurrent symptoms at the 3rd month then we stopped using topical 2% ganciclovir at 11th month. IOP, intraocular pressure; VA, visual acuity.
Figure 2.
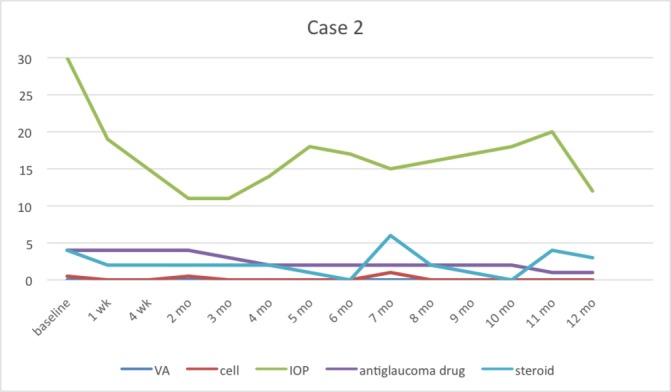
Case 2 had recurrent symptoms at the 7th and 11th months while tapering 2% topical ganciclovir. IOP, intraocular pressure; VA, visual acuity.
Figure 3.
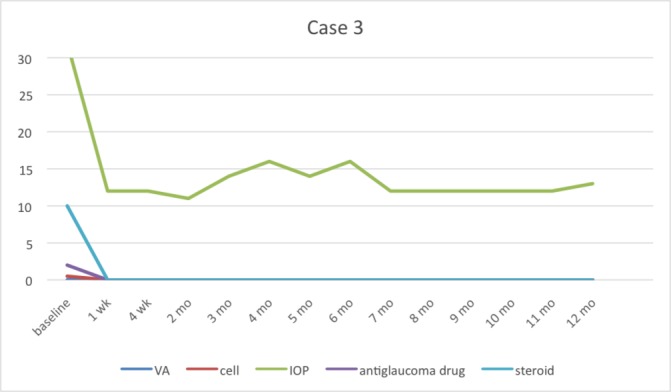
Case 3 could be stopped using 2% topical ganciclovir at 3rd month without any recurrent symptoms. IOP, intraocular pressure; VA, visual acuity.
Figure 4.
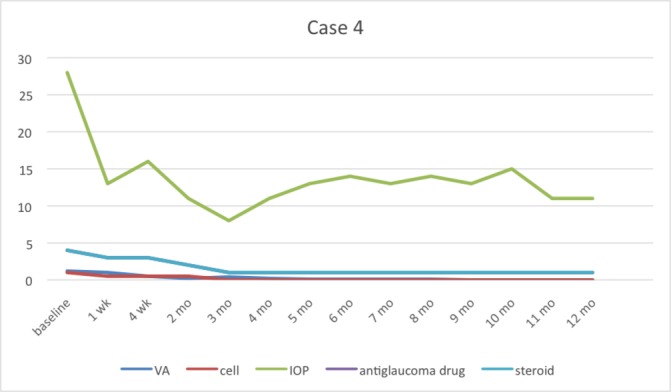
Case 4 (corneal decompensate) still continues topical ganciclovir four times a day for undergoing penetrating keratoplasty in the future. IOP, intraocular pressure; VA, visual acuity.
Figure 5.
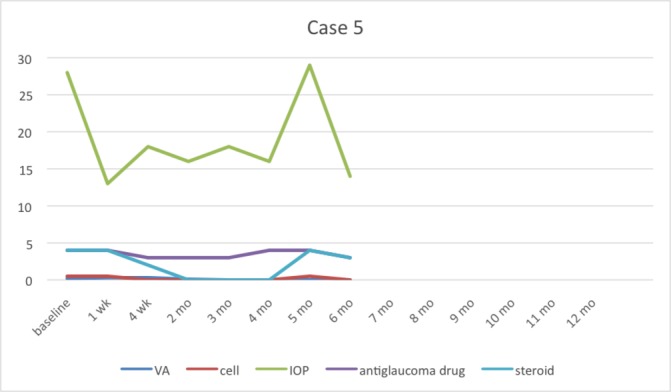
Case 5 had recurrent symptoms at fifth month and then finally the patient stopped taking medicine. IOP, intraocular pressure; VA, visual acuity.
Figure 6.
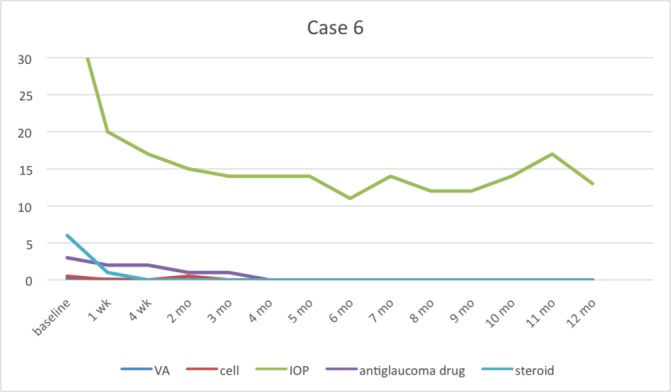
Case 6 stopped taking 2% topical ganciclovir at 7th month. After that the recurrent symptoms occurred at 10th month by the presenting of keratic precipitates. IOP, intraocular pressure; VA, visual acuity.
Figure 7.
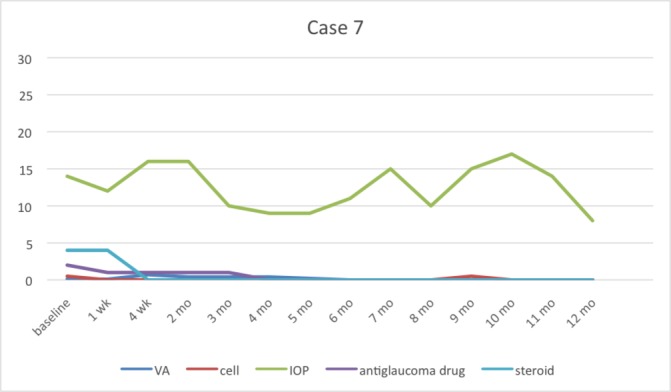
Case 7 stopped taking topical 2% ganciclovir at 6th month then recurrent symptoms occurred at 9th month. IOP, intraocular pressure. VA, visual acuity.
Figure 8.
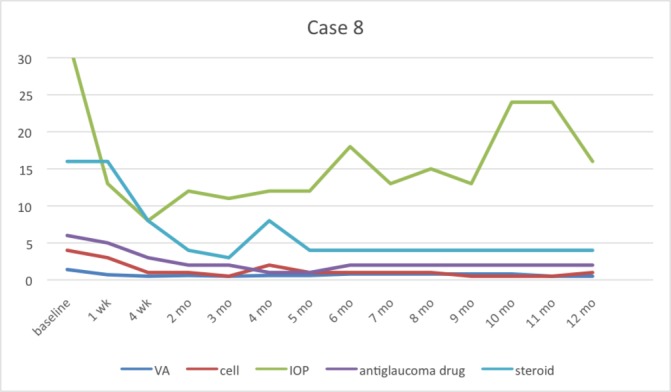
Case 8 had no recurrence; however he was still on medicine. At 10th month follow-up, the patient had poor compliance to take antiglaucoma medicine. IOP, intraocular pressure; VA, visual acuity.
Figure 9.
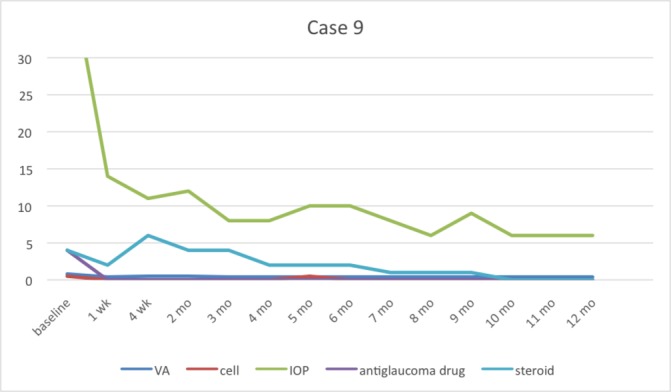
Case 9 could be stopped using 2% topical ganciclovir at 11th month without any recurrent symptoms. IOP, intraocular pressure; VA, visual acuity.
Figure 10.
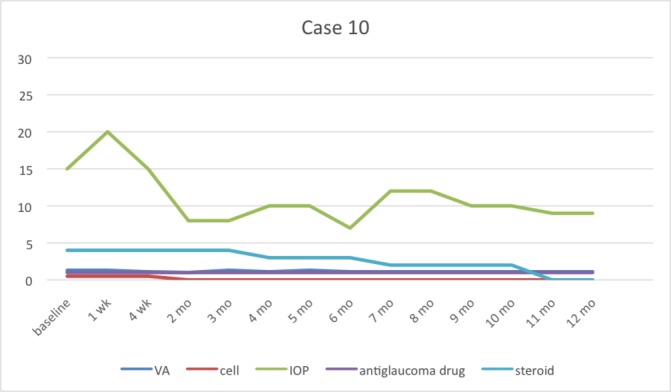
Case 10 could be stopped using 2% topical ganciclovir at 11th month without any recurrent symptoms. IOP, intraocular pressure; VA, visual acuity.
Figure 11.
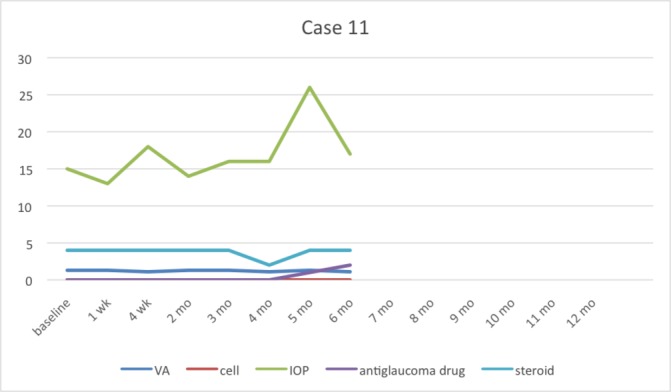
Case 11 stopped taking medicine by herself at 2 weeks then the recurrent symptoms occurred at 5th month. After that topical 2% ganciclovir was restarted. IOP, intraocular pressure; VA, visual acuity.
Six of 11 cases were recurrent: three cases were recurrent when they stopped using topical steroid eye drops but were still using topical 2% ganciclovir three times daily,while three cases were recurrent after stopping topical 2% ganciclovir (27%). They tended to present poorer VA, less anterior chamber cells and more KPs in the recurrent group; however, no significance was observed in all factors between the recurrent and non-recurrent groups (table 6).
Table 6.
Factors between recurrent and non-recurrent group
| Non-recurrent | Recurrent | p Value | |
| Median (min–max) | Median (min–max) | ||
| No. Age |
5 (45%) 41.00 (28.00–81.00) |
6 (55%) 51.00 (29–76) |
0.855* |
| Duration (months) | 48.00 (1.00–60.00) | 59.50 (12–204) | 0.313* |
| Visual acuity | 1.20 (0–1.40) | 0.20 (0–1.30) | 0.195* |
| Cell | 0.50 (0.50–4.00) | 0.25 (0–1.00) | 0.159* |
| KPs | 0.182† | ||
| No | 1 (20.00) | – | |
| Yes | 4 (80.00) | 6 (100.00) | |
| IOP | 32.00 (15–44) | 22.5 (14–40) | 0.314* |
| Antiglaucoma drug | 4 (1–6) | 3 (0–4) | 0.511* |
| Steroid | 4 (2–16) | 4 (4–6) | 0.672* |
*Mann-Whitney U test.
†Fisher's exact test.
Significant (p<0.05).
In case 8, recurrent CMV uveitis was defined as unilateral, high IOP, coin-shaped KPs, localised corneal oedema and normal retina while recurrent in Behcet’s disease should be bilateral, low IOP, fine KPs or some retinitis progression.
CMV, cytomegalovirus; IOP, intraocular pressure; KPs, keratic precipitates.
Side effects of topical 2% ganciclovir treatment (tables 7 and 8)
Table 7.
Clinical manifestations after using topical 2% ganciclovir treatment
| No | Yes | |||
| n | % | n | % | |
| Red eye | 10 | 90.91 | 1 | 9.09 |
| Foreign body sensation | 10 | 90.91 | 1 | 9.09 |
| Eyelid swelling | 10 | 90.91 | 1 | 9.09 |
| Photophobia | 11 | 100.00 | – | |
| Dry eye | 11 | 100.00 | – | |
| Blurred vision | 10 | 90.91 | 1 | 9.09 |
| Yellowish discharge | 11 | 100.00 | – | |
| Tearing | 9 | 81.82 | 2 | 18.18 |
| Irritated eye | 8 | 72.73 | 3 | 27.27 |
| Others | 11 | 100.00 | – | |
Table 8.
Ocular examination after using topical 2% ganciclovir treatment
| No | Yes | |||
| n | % | n | % | |
| Discharge | 11 | 100.00 | – | |
| Conjunctival reaction | 11 | 100.00 | – | |
| Punctate epithelial erosion | 11 | 100.00 | – | |
| Epithelial defect | 11 | 100.00 | – | |
The most common complaint of symptoms was irritated eye (27.27%), lasting 1–2 min after applying eye drops. The second symptom was tearing (18.18%). Other symptoms including red eye, foreign body sensation, eyelid swelling and temporary blurred vision were also recorded (9.09%). No systemic or serious complications were observed in any of the patients.
Regarding medication (table 9), 2 of 11 patients (18.18%) complained about a small amount of white sediment appearing even though the medication was stored in a cool place. It returned to clear after shaking. Any colour change in medication was undetected.
Table 9.
Characteristic of medication change
| Medications change | No | Yes | ||
| n | % | n | % | |
| White sediment | 9 | 81.82 | 2 | 18.18 |
| Change colour | 11 | 100 | – | |
| Others | 11 | 100 | – | |
Discussion
Ganciclovir is a synthetic purine nucleoside, an analogue of quanosine23 and a well-known medication against CMV. Topical forms of ganciclovir have shown effective penetration through the cornea including the aqueous humour24 25 and comprise the first treatment option in CMV anterior uveitis and CMV endotheliitis.
Most studies have demonstrated the efficacy of systemic and topical ganciclovir, but not in timeline details. In particular, ours was the first study to evaluate the response of topical ganciclovir in the first week and then monthly. Although our study showed reduced IOP was the first response when using topical 2% ganciclovir, 18.18% of cases required a trabeculectomy with mitomycin C. In addition, Wong et al reported 21.2% of cases developed uncontrolled IOP and underwent glaucoma surgery.
Some studies18 19 have specified that KPs and anterior chamber inflammation improved after a 4-week administration of topical ganciclovir similar to our study. Tapering off topical steroid eye drops needs to be slow along with anterior chamber inflammation. That is why at 12th month, some patients were still using once to twice daily. However, BCVA did not improve significantly at 12 weeks, while our study showed it improved significantly at 5 months. Hence, even though other anterior chamber inflammation was controlled, BCVA was the last significant continuous response.
Chee and Jap found that topical ganciclovir had lower recurrence rates than systemic ganciclovir.26 In this study, we found 27% of discontinued medication was recurrent in anterior uveitis, similar to Koizumi et al reporting 36% of cases showed recurrence of inflammation and anti-CMV treatment was repeated14 as well. Wong et al reported topical ganciclovir reduced the number of episodes of recurrent anterior uveitis17 while using and suggested that maintenance therapy may be required to prevent recurrences27 because ganciclovir, a virustatic agent, does not eradicate viruses in the latent phase.
Our study found unexpected symptoms after using topical ganciclovir; however, they were insignificant and improved by adding artificial tears. No studies reported significant side effects such as ocular discomfort or corneal toxicity from topical ganciclovir 0.15%,17 18 0.514 or 2%20 as well. White sediment appeared in some bottles. We recommend shaking the medicine while mixing very well because ganciclovir has relatively small-sized molecules with high lipophilicity causing ganciclovir to be poorly soluble in water.25
Limitations in this study included being a relatively small case series and retrospective non-randomised study. Furthermore, the study should compare the efficacy and safety of other concentrations of topical ganciclovir in a randomised control trial requiring longer term follow-up.
Conclusion
Topical 2% ganciclovir alone is a safe and effective medicine to control inflammation in CMV anterior uveitis. The first response is reduced IOP and KPs, and then decreased anterior inflammation. Therefore, extemporaneous preparations of topical 2% ganciclovir are non-invasive, economical and convenient for the hospital where commercial topical ganciclovir is unavailable.
Footnotes
Competing interests: None declared.
Patient consent: Obtained.
Ethics approval: The Phramongkutklao Institutional Review Board.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Skuta GL, Cantor LB, Weiss JS. Basic and clinical science Course 2012-2013: intraocular inflammation and uveitis. 77 Canada: American Academy of Ophthalmology, 2012. [Google Scholar]
- 2.Koizumi N, Suzuki T, Uno T, et al. Cytomegalovirus as an etiologic factor in corneal endotheliitis. Ophthalmology 2008;115:292–7. doi:10.1016/j.ophtha.2007.04.053 [DOI] [PubMed] [Google Scholar]
- 3.Laaks D, Smit DP, Harvey J. Polymerase chain reaction to search for Herpes viruses in uveitic and healthy eyes: a South African perspective. Afr Health Sci 2015;15:748–54. doi:10.4314/ahs.v15i3.7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Santos FF, Commodaro AG, Souza AV, et al. Real-time PCR in infectious uveitis as an alternative diagnosis. Arq Bras Oftalmol 2011;74:258–61. doi:10.1590/S0004-27492011000400006 [DOI] [PubMed] [Google Scholar]
- 5.Woo JH, Lim WK, Sl H, et al. Characteristics of CytomegalovirusUveitis in immunocompetent patients. Ocul Immunol Inflamm 2014;10:1–6. [Google Scholar]
- 6.Choi JA, Kim KS, Jung Y, et al. Cytomegalovirus as a cause of hypertensive anterior uveitis in immunocompetent patients. J Ophthalmic Inflamm Infect 2016;6:32 doi:10.1186/s12348-016-0100-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Accorinti M, Gilardi M, Pirraglia MP, et al. Erratum to: Cytomegalovirus anterior uveitis: long-term follow-up of immunocompetent patients. Graefes Arch Clin Exp Ophthalmol 2014;252:2029 doi:10.1007/s00417-014-2844-7 [DOI] [PubMed] [Google Scholar]
- 8.Bloch-Michel E, Dussaix E, Cerqueti P, et al. Possible role of cytomegalovirus infection in the etiology of the Posner-Schlossmann syndrome. Int Ophthalmol 1987;11:95–6. doi:10.1007/BF00136737 [DOI] [PubMed] [Google Scholar]
- 9.Teoh SB, Thean L, Koay E. Cytomegalovirus in aetiology of Posner-Schlossman syndrome: evidence from quantitative polymerase chain reaction. Eye 2005;19:1338–40. doi:10.1038/sj.eye.6701757 [DOI] [PubMed] [Google Scholar]
- 10.Markomichelakis NN, Canakis C, Zafirakis P, et al. Cytomegalovirus as a cause of anterior uveitis with sectoral iris atrophy. Ophthalmology 2002;109:879–82. doi:10.1016/S0161-6420(02)00961-2 [DOI] [PubMed] [Google Scholar]
- 11.Chee SP, Bacsal K, Jap A, et al. Clinical features of Cytomegalovirus anterior uveitis in immunocompetent patients. Am J Ophthalmol 2008;145:834–40. doi:10.1016/j.ajo.2007.12.015 [DOI] [PubMed] [Google Scholar]
- 12.Villarreal EC. Current and potential therapies for the treatment of herpes-virus infections. Prog Drug Res 2003;60:263–307. [DOI] [PubMed] [Google Scholar]
- 13.de Schryver I, Rozenberg F, Cassoux N, et al. Diagnosis and treatment of cytomegalovirus iridocyclitis without retinal necrosis. Br J Ophthalmol 2006;90:852–5. doi:10.1136/bjo.2005.086546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Koizumi N, Inatomi T, Suzuki T, et al. Clinical features and management of cytomegalovirus corneal endotheliitis: analysis of 106 cases from the Japan corneal endotheliitis study. Br J Ophthalmol 2015;99:54–8. doi:10.1136/bjophthalmol-2013-304625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Crumpacker CS. Ganciclovir. N Engl J Med 1996;335:721–9. doi:10.1056/NEJM199609053351007 [DOI] [PubMed] [Google Scholar]
- 16.Choi WS, Cho JH, Kim HK, et al. A case of CMV endotheliitis treated with intravitreal ganciclovir injection. Korean J Ophthalmol 2013;27:130–2. doi:10.3341/kjo.2013.27.2.130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wong JX, Agrawal R, Wong EP, et al. Efficacy and safety of topical ganciclovir in the management of cytomegalovirus (CMV)-related anterior uveitis. J Ophthalmic Inflamm Infect 2016;6:10 doi:10.1186/s12348-016-0078-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Koizumi N, Miyazaki D, Inoue T, et al. The effect of topical application of 0.15% ganciclovir gel on Cytomegalovirus corneal endotheliitis. Br J Ophthalmol 2016. [DOI] [PubMed] [Google Scholar]
- 19.Fan NW, Chung YC, Liu YC, et al. Long-Term Topical Ganciclovir and corticosteroids preserve corneal endothelial function in Cytomegalovirus corneal endotheliitis. Cornea 2016;35:596–601. doi:10.1097/ICO.0000000000000791 [DOI] [PubMed] [Google Scholar]
- 20.Su CC, Wang IJ, Chen WL, et al. Topical ganciclovir treatment in patients with cytomegalovirus endotheliitis receiving penetrating keratoplasty. Clin Exp Ophthalmol 2013;41:339–4. doi:10.1111/j.1442-9071.2012.02888.x [DOI] [PubMed] [Google Scholar]
- 21.Su CC, Hu FR, Wang TH, et al. Clinical outcomes in cytomegalovirus-positive Posner-Schlossman syndrome patients treated with topical ganciclovir therapy. Am J Ophthalmol 2014;158:1024–31. doi:10.1016/j.ajo.2014.08.007 [DOI] [PubMed] [Google Scholar]
- 22.The Standardization of Uveitis Nomenclature (SUN) Working Group. standardization of uveitis nomenclature for reporting clinical data. results of the First International Workshop. Am J Ophthalmol 2005;140:509–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chou TY. Hong BY: ganciclovir ophthalmic gel 0.15% for the treatment of acute herpetic keratitis: background, effectiveness, tolerability, safety, and future applications. The Clin Risk Manag 2014;10:665–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Colin J. Ganciclovir ophthalmic gel, 0.15%: a valuable tool for treating ocularherpes. ClinOphthalmol 2007;4:441–53. [PMC free article] [PubMed] [Google Scholar]
- 25.Castela N, Vermerie N, Chast F, et al. Ganciclovir ophthalmic gel in herpes simplex virus rabbit keratitis: intraocular penetration and efficacy. J Ocul Pharmacol 1994;10:439–51. doi:10.1089/jop.1994.10.439 [DOI] [PubMed] [Google Scholar]
- 26.Chee SP, Jap A. Cytomegalovirus anterior uveitis: outcome of treatment. Br J Ophthalmol 2010;94:1648–52. doi:10.1136/bjo.2009.167767 [DOI] [PubMed] [Google Scholar]
- 27.Faulds D, Heel RC. Ganciclovir. A review of its antiviral activity, pharmacokinetic properties and therapeutic efficacy in cytomegalovirus infections. Drugs 1990;39:597–638. [DOI] [PubMed] [Google Scholar]