

Abstract
Motor vehicle crashes are the leading cause of adolescent death. Inattention to the roadway contributes to crash risk and often results from distractions, such as cell phone calls, texting, and peer passengers. We report on the development of a web-based intervention based on the Theory of Planned Behavior that aims to reduce adolescent driver inattention (Let’s Choose Ourselves). In Phase I, we collected qualitative and quantitative data on adolescents’ attitudes, perceived behavioral control and subjective norms about driver inattention through focus groups with newly licensed adolescent drivers. In Phase II, we developed the content in an e-learning delivery system, performed beta and pilot testing, and made refinements. In Phase III, we conducted a randomized controlled trial to evaluate feasibility. The development of Let’s Choose Ourselves provides information for school nurses regarding intervention development strategies, as well as promotion of safe adolescent driving by reducing driver inattention.
Keywords: adolescent, distracted driving, inattention, motor vehicle crash, risky driving, school nursing, Theory of Planned Behavior
Introduction
Motor vehicle crashes (MVCs) are the leading cause of adolescent death (Centers for Disease Control and Prevention (CDC), 2016). In 2014, 2,270 adolescents died and at least another 220,000 were treated for injuries from MVCs in the United States (US) (CDC, 2016). The consequences of adolescent driver crashes have a profound negative impact on the public’s health. In addition, MVCs have a high economic cost, with over 35% of lifetime medical cost for crash injuries in 2012 ($6.5 billion out of $18 billion) attributed to young drivers ages 15 to 29 (CDC, 2014; Sommers, Fargo, Lyons, Shope, & Sommers, 2011). Adolescent drivers are at their highest risk for an MVC in their first year of licensure (Mayhew, Simpson, & Pak, 2003; McCartt, Shabanova, & Leaf, 2003; Williams & Tefft, 2014). Interventions that reduce adolescent crash risk during the first year of licensure have the potential to make significant inroads on reducing adolescent driver crashes (Williams, Tefft, & Grabowski, 2012).
One of the leading causes of adolescent crashes is inattention to the roadway. Driver inattention can be defined as “insufficient or no attention to activities critical for safe driving” (Regan, Hallett, & Gordon, 2011, p. 1775). Distractions inside the vehicle such as cell phone calls, texting, and the behavior of peer passengers, draw attention away from the roadway (Carney, Mcgehee, Harland, Weiss, & Raby, 2015). In the 2011 Youth Risk Behavior Survey, almost 45% of high school adolescents reported texting while driving in the previous 30 days (Olsen, Shults, & Eaton, 2013). The Pew Research Center indicates that 52% of cell phone-owning adolescents ages 16 to 17 have talked on a phone while driving; 48% of all adolescents ages 12 to 17 say they have been in a car when the driver was texting; and 40% say they have been in a car when the driver used a cell phone in a way that put themselves or others in danger (Lenhart, Ling, Campbell, & Purcell, 2010). Adolescent driver crash or near crash risk substantially increases with reaching for or dialing a cell phone (OR= 7.05, 95% CI 2.64–18.83) and sending or receiving text messages (OR=3.87, 95% CI 1.62–9.25) (Klauer et al., 2014).
Cell phones are not the only factor that draws an adolescent’s attention away from driving. Presence of peer passengers is associated with an increase in fatal crash risk (Chen, 2000; Ouimet et al., 2015; Tefft, Williams, & Grabowski, 2012). The presence of risk-accepting peers (e.g., those who exhibit behaviors such as drinking alcohol, drinking and driving, driving in excess of speed limits, not using safety belts) is associated with risky driving behaviors in naturalistic data of adolescent drivers (Simons-Morton et al., 2011). Presence of peer passengers has also been linked with aggressive or illegal driving, speeding, and following the vehicle in front too closely (Curry, Mirman, Kallan, Winston, & Durbin, 2012; Simons-Morton, Lerner, & Singer, 2005; Simons-Morton et al., 2014).
Efforts to decrease adolescent morbidity and mortality from MVCs have centered on public policy changes such as the implementation of Graduated Drivers Licensing (GDL) (Williams et al., 2012). GDL is a staged system which is meant to protect inexperienced young drivers by increasing privileges (such as nighttime driving and carrying unlimited peer passengers) as they gain driving exposure. Most programs include three stages (learner, intermediate and full privilege license) (Governors Highway Safety Association, 2016). Interventions have also been developed that target parental roles, such as feedback and monitoring systems, parental contracts and educational programs to increase diversity and quantity of supervised practice driving (Mirman et al., 2014; B. G Simons-Morton et al., 2006; Zakrajsek et al., 2013). Skills-based interventions such as hazard anticipation training have also shown potential (Fisher et al., 2002). Although these strategies have the potential to decrease adolescent MVCs, the sustained, alarmingly high rates of adolescent MVCs indicate that further work is warranted. Targeted, individual, theory-based behavioral interventions have the potential to fill this gap to help adolescent drivers manage factors to reduce inattention to the road.
The Theory of Planned Behavior (TPB) posits that the attitude toward a behavior, perceived behavioral control (PBC) to perform a behavior, and subjective norms about a behavior shape behavioral intentions, and resultantly, the actual behavior (Ajzen & Fishbein, 1980; Ajzen, 1991). Attitudes are the degrees to which someone has a favorable or unfavorable evaluation of the behavior; PBC is the perceived ease or difficulty in performing a behavior; subjective norms are the perceived social pressures to perform or not perform a behavior (Ajzen, 1991). The TPB has been used successfully with adolescents to guide interventions that lead to behavioral change in other domains of adolescent risk behaviors (e.g. smoking, alcohol use, unsafe sex) and shows promise for addressing adolescent driver inattention (Armitage & Talibudeen, 2010; Brawner et al., 2013; Jemmott, Jemmott, Fong, & Morales, 2010; Koning, van den Eijnden, Verdurmen, Engels, & Vollebergh, 2011).
The purpose of this manuscript is to describe the three-phase approach used to develop, refine and perform initial testing of Let’s Choose Ourselves, a theoretically-grounded web-based intervention to reduce adolescent driver inattention. Let’s Choose Ourselves was developed for newly licensed adolescent drivers to address two critical areas related to inattention to the roadway: distractions related to cell phone use and peer passengers. The TPB guided all steps of intervention development. For the purposes of this manuscript, we will not report on results on the intervention effects of Let’s Choose Ourselves. Instead, we focus on the process, the results of studies that led to the development of the intervention, and relevance to school nursing.
The Intervention Development Process and Outcome: Three Phases
We carried out a multi-phase development approach based on TPB to develop Let’s Choose Ourselves. Applying TPB, we focused on attitudes, PBCs and subjective norms among adolescents as they related to a leading cause of MVCs—inattention to the road (see Figure 1).
Figure 1. Theory of Planned Behavior for Adolescent Driver Inattention.
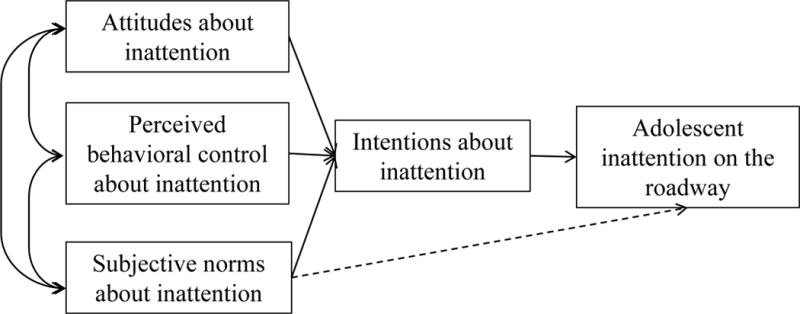
Note: Adapted from Ajzen, 1991
TPB guides pilot work to identify attitudes, control beliefs, and norms. Theory-driven data collection is then used in an intervention targeted to modify predictors of intentions and behaviors (Ajzen, n.d.). We describe our development in three phases. Phase I included collection of focus group and self-report survey data from n=30 adolescent drivers ages 16 to18 years, licensed for less than 1 year in Pennsylvania (PA). Phase II involved integrating Phase I focus group and survey data to develop and carry out beta and pilot testing of the intervention (Let’s Choose Ourselves) with eight adolescents and young adult drivers. In Phase III, we enrolled 60 adolescents (ages 16–17 years, licensed for ≤90 days in PA) in the randomized controlled trial (RCT). We report on the methods and results within each phase. All study procedures were approved by the Institutional Review Board and an administrative agreement with The Children’s Hospital of Philadelphia and the University of Pennsylvania. Informed consent (verbal or written; parental for <age 18) and assent (written) were obtained for participation in all phases of this study.
Phase I Methods (Surveys and Focus Groups)
Phase I involved qualitative focus group and quantitative self-report survey methods. For Phase I, we recruited a purposive sample of adolescents through primary care clinics affiliated with the Children’s Hospital of Philadelphia (CHOP), presentations at schools, flyers, email and word of mouth (Polit, 2004). Adolescents who had a PA driver’s license for ≤1 year were recruited because they could talk about their current experiences as drivers, as well as think back to the different stages of when they were passengers or drivers. Data collection took place in a private room in a community center. Participants were compensated $20. We administered paper and pen surveys to participants in the focus groups immediately prior to the group discussion. For the surveys and focus groups, given the evidence about inattention that cell phones and peer passengers contribute to adolescent driver crash risk (Chen, 2000; Klauer et al., 2014; Ouimet et al., 2015), we specifically targeted perceptions about cell phones (i.e., call, texts, internet use) and peer passengers (i.e., interactions, conversations, passenger limits).
The short survey included items on participant demographics; driving history including permit length and crash history; and questions based on TPB to elicit participants’ individual perceptions about inattention. While some may argue that pre-focus group surveys prime participants for the focus group discussion, this method is consistent with procedures in accordance with the chosen theoretical approach (Fishbein & Ajzen, 2010). The quantitative survey data were double data entered and analyzed using IBM Statistics SPSS 23. Descriptive statistics were used to describe the demographic characteristics and perceptions of the participants about inattention. Bivariate Pearson correlations were used to determine relationships among the constructs and help identify key areas for intervention content.
In the focus group interview guide, we used open-ended questions and probes based on the TPB to examine perceptions of inattention to the road. In addition, we elicited information on how to develop a program that addresses inattention for newly licensed adolescent drivers. We included questions in the focus group guide such as: “What do you think about teens texting (talking on a cell phone/using a mobile device to access the internet) while driving?” (attitudes); “What makes it easy (hard) to text and drive?” (PBC); “Who approves (disapproves) of you texting (talking on a cell phone, using a mobile device to access the internet) while driving?” (subjective norms); “What do you think about the topic of keeping attention on the road for a safe driving program for young drivers?” (program development). We then used directed descriptive content analysis to analyze the focus group data (Hsieh & Shannon, 2005). Based on TPB and the empirical literature, we identified key concepts as coding categories, and developed definitions for attitudes, PBC and subjective norms about inattention to the road (Hsieh & Shannon, 2005). The research team members reviewed transcripts in Atlas.ti (version 7.5) to apply coding categories to the sections of text (participants’ quotes) and developed themes based on the participants’ data in the coding categories.
Phase I Results (Surveys and Focus Groups)
Thirty adolescents participated in seven focus groups, with attendance ranging from 3–6 participants (median=4) in each group. Table 1 describes their demographic information and self-reported behaviors related to driving inattention. Table 2 outlines the mean scores and distribution on attitudes, PBC, subjective norms and intentions (with Cronbach alpha of summed items for intentions) from the self-report survey data. We report on the overall mean of a construct, but also the number and percentage of participants in the sample for each answer option. For example, nearly the entire sample (96.7%) reported that texting was a bad or very bad idea. However, as can be seen in Table 1, 46.7% of the sample reported that in the past 30 days, they had texted while driving. Bivariate Pearson correlations of intentions with the main constructs of TPB (attitudes, PBC and norms) for each specific distraction type were as follows: intentions to talk on a hand-held phone (attitudes: r=0.71*, PBC: r=0.41*, norms: r=0.11); intentions to talk on a hands-free phone (attitudes: r=0.71*, PBC: r=0.70*, norms: r=0.73*); intentions to text (attitudes: r=0.47*, PBC: r=0.70, norms: r=0.29); intentions to access internet (attitudes: r=0.80*, PBC: r=0.72*, norms: r=0.62*) and intentions related to passenger interactions (attitudes: r=0.68*, PBC: r=0.68*, norms: r=0.63*) (*p<0.05).
Table 1.
Self-reported Survey Data Phase I Focus Group Sample (n=30)
| Mean (sd) or n (%) | |
|---|---|
|
| |
| Age | 17.39 (0.52) |
|
| |
| Gender | |
| Male | 15 (50%) |
| Female | 15 (50%) |
|
| |
| Race | |
| White | 27 (90%) |
| Black/African American | 0 |
| Asian/Pacific Islander | 1 (3.3%) |
| Mixed Race | 0 |
| Not reported | 2 6.7%) |
|
| |
| Ethnicity | |
| Hispanic | 1 (3.3%) |
| Non-Hispanic | 29 (96.7%) |
| Not reported | 0 |
|
| |
| Length of licensure (days) | 173.7 (109.2) |
|
| |
| Total crashes while driving since received driver’s license | |
| 0 | 25 (83.3%) |
| 1 | 5 (16.7%) |
| 2 or more | 0 |
|
| |
| In the last month: | |
|
| |
| Driving days | 0 |
| 0 days | 1 (3.3%) |
| 1–7 days | 5 (16.7%) |
| 8–14 days | 5 (16.7%) |
| 15–21 days | 10 (33.3%) |
| 22–28 days | 9 (30%) |
| 29 or more days | |
|
| |
| Talked on a hand-held cell phone while driving | |
| 0 days | 18 (60%) |
| 1–7 days | 10 (33.3%) |
| 8–14 days | 2 (6.7%) |
| 15–21 days | 0 |
| 22–28 days | 0 |
| 29 or more days | 0 |
|
| |
| Talked on a hands-free cell phone while driving | |
| 0 days | 12 (40%) |
| 1–7 days | 14 (46.7%) |
| 8–14 days | 3 (10%) |
| 15–21 days | 1 (3.3%) |
| 22–28 days | 0 |
| 29 or more days | 0 |
|
| |
| Texted while driving | |
| 0 days | 16 (53.3%) |
| 1–7 days | 9 (30%) |
| 8–14 days | 0 |
| 15–21 days | 5 (16.7%) |
| 22–28 days | 0 |
| 29 or more days | 0 |
|
| |
| Used a mobile device to access the internet while driving | |
| 0 days | 20 (66.7%) |
| 1–7 days | 5 (16.7%) |
| 8–14 days | 2 (6.7%) |
| 15–21 days | 2 (6.7%) |
| 22–28 days | 1 (33.3%) |
| 29 or more days | 0 |
Table 2.
Attitudes, Perceived Behavioral Control and Norms Phase I Focus Group Sample (n=30)
| Talk Hand-held | Talk Hands-free | Texting | Accessing Internet | Passenger Interaction | |
|---|---|---|---|---|---|
| M (sd)a | M (sd)a | M (sd)a | M (sd)a | M (sd)a | |
|
| |||||
| n (%) | n (%) | n (%) | n (%) | n (%) | |
|
| |||||
| Attitudes: How do you feel about…while driving? | 2.03 (0.81) | 3.23 (0.94) | 1.20 (0.48) | 1.57 (0.82) | 3.37 (0.93) |
| 1=very bad idea | 8 (26.7%) | 2 (6.7%) | 25 (83.3%) | 18 (60%) | 1 (3.3%) |
| 2=bad idea | 14 (46.7%) | 2 (6.7%) | 4 (13.3%) | 8 (26.7%) | 2 (6.7%) |
| 3=in the middle | 7 (23.3%) | 15 (50%) | 1 (3.3%) | 3 (10%) | 16 (53.3%) |
| 4=good idea | 1 (3.3%) | 9 (30%) | 0 | 1 (3.3%) | 7 (23.3%) |
| 5=very good idea | 0 | 2 (6.7%) | 0 | 0 | 4 (13.3%) |
|
| |||||
| PBC: How easy or hard is it to…while driving? | 2.80 (1.13) | 3.77 (0.86) | 1.80 (1.0) | 1.90 (1.10) | 4.07 (0.91) |
| 1=very hard | 3 (10%) | 0 | 16 (53.3%) | 14 (46.7%) | 1 (3.3%) |
| 2=hard | 11 (36.7%) | 1 (3.3%) | 6 (20%) | 9 (30%) | 0 |
| 3=in the middle | 7 (23.3%) | 12 (40%) | 6 (20%) | 4 (13.3%) | 5 (16.7%) |
| 4=easy | 7 (23.3%) | 10 (33.3%) | 2 (6.7%) | 2 (6.7%) | 14 (46.7%) |
| 5=very easy | 2 (6.7%) | 7 (23.3%) | 0 | 1 (3.3%) | 10 (33.3%) |
|
| |||||
| Subjective Norms: Would most people who are important to you approve or disapprove of you…while driving? | 1.87 (0.78) | 3.27 (0.91) | 1.07 (0.25) | 1.37 (0.77) | 3.27 (0.87) |
| 1=strongly disapprove | 10 (33.3%) | 2 (6.7%) | 28 (93.3%) | 23 (76.7%) | 2 (6.7%) |
| 2=disapprove | 15 (50%) | 3 (10%) | 2 (6.7%) | 4 (13.3%) | 2 (6.7%) |
| 3=in the middle | 4 (13.3%) | 10 (33.3%) | 0 | 2 (6.7%) | 12 (40%) |
| 4=approve | 1 (3.3%) | 15 (50%) | 0 | 1 (3.3%) | 14 (46.7%) |
| 5=strongly approve | 0 | 0 | 0 | 0 | 0 |
|
| |||||
| Intentions: Sum of items about likelihood, being sure and plan | 7.23 (3.16) | 9.60 (3.59) | 7.97 (3.83)* | 6.03 (3.71) | 8.4 (1.57)** |
| α=0.91 | α=0.92 | α=0.92 | α=0.97 | α=0.85 | |
| How likely while driving? | |||||
| 1=very unlikely | 8 (26.7%) | 6 (20%) | 13 (43.3%) | 17 (56.7%) | 0 |
| 2=unlikely | 13 (43.3%) | 6 (20%) | 9 (30%) | 4 (13.3%) | 1 (3.3%) |
| 3=in the middle | 3 (10%) | 4 (13.3%) | 2 (6.7%) | 5 (16.7%) | 2 (6.7%) |
| 4=likely | 5 (16.7%) | 9 (30%) | 6 (20%) | 3 (10%) | 14 (46.7%) |
| 5=very likely | 1 (3.3%) | 5 (16.7%) | 0 | 1 (3.3%) | 13 (43.3%) |
| I am sure (answer call/respond/read/access internet) while driving. | Read/Respond* | ||||
| 1=disagree strongly | 6 (20%) | 1 (3.3%) | 10 (33.3%)/16 (53.3%) | 14 (46.7%) | NA |
| 2=disagree | 9 (30%) | 3 (10%) | 4 (13.3%)/8 (26.7%) | 6 (20%) | NA |
| 3=in the middle | 8 (26.7%) | 9 (30%) | 12 (40%)/5 (16.7%) | 4 (13.3%) | NA |
| 4=agree | 5 (16.7%) | 10 (33.3%) | 3 (10%)/1 (3.3%) | 5 (16.7%) | NA |
| 5=agree strongly | 2 (6.7%) | 7 (23.3%) | 1 (3.3%)/0 | 1 (3.3%) | NA |
| I plan to ….in the next month. | |||||
| 1=disagree strongly | 7 (23.3%) | 5 (16.7%) | 15 (50%) | 16 (53.5%) | 0 |
| 2=disagree | 11 (36.7%) | 8 (26.7%) | 7 (23.3%) | 4 (13.3%) | 2 (6.7%) |
| 3=in the middle | 7 (23.3%) | 5 (16.7%) | 5 (16.7%) | 5 (16.7%) | 5 (16.7%) |
| 4=agree | 4 (13.3%) | 8 (26.7%) | 3 (10%) | 3 (10%) | 11 (36.7%) |
| 5=agree strongly | 1 (3.3%) | 4 (13.3%) | 0 | 2 (6.7%) | 12 (40%) |
Note:
4 items for texting intentions (one item about being sure to read and one item about being sure to respond)
2 items for passenger (being sure not asked of participants);
Mean and standard deviation are reported for overall constructs in italics
For the qualitative data from the focus groups, we previously reported key themes on inattention related to cell phones and passengers (McDonald & Sommers, 2015, 2016). Focus group data also provided information on adolescents’ perceptions of the proposed intervention content and mode of delivery. Participants suggested the intervention show the danger of distractions by using techniques such as driving simulation. They described the need for clear messages about dangers of inattentive driving, as well as strategies to remove distractions. A majority of the participants thought a web-based intervention was a positive way to reach adolescents. Some participants described a desire for an app or including characteristics of gaming. Overall, the participants indicated that the intervention should be interactive, entertaining, and brief.
Participants also debated the timing of the intervention delivery and challenges to intervention completion. They noted that during the learning-to-drive process, it might be advantageous to have adolescents complete an intervention about inattention. However, some conceded that during the learning phase, new drivers are focused on learning skills and how to handle the vehicle, and distractions like phones and peer passengers are not a part of the driving experience. As they become more experienced drivers, participants described scenarios in which they may be more likely to become distracted. Busy schedules were seen as the primary challenge for intervention completion, emphasizing the need to design a medium that adolescents could initiate and complete at their convenience.
Phase II Methods (Building the Intervention)
From the Phase I focus group and survey data and empirical evidence in the literature (Centers for Disease Control and Prevention, 2016; Curry, Hafetz, Kallan, Winston, & Durbin, 2011; Tefft et al., 2012), we developed the intervention for adolescent driver inattention and we named it Let’s Choose Ourselves. Although participants described a desire for an app, given the rapidly changing technology of web-based applications, cost of app development and limitations with data security, we used a lower-cost, flexible option of commercially available e-learning software to develop and deliver the intervention through a secure Learning Management System (LMS). The intervention consisted of six sections (Welcome; General content on adolescent driving; Ideas behind Let’s Choose Ourselves; Cell phone use; Passengers and; Wrap-up). We developed content for Let’s Choose Ourselves that was fact-based, grounded in data from the focus groups, interactive, and provided realistic scenarios of how to deal with cell phone and passenger distractions. The goal was for participants to complete the intervention in one on-line session lasting 30–45 minutes without interaction with a study team member.
To illustrate the content and delivery of the intervention, Table 3 outlines themes from the focus groups from Phase I, examples of content and activities in Let’s Choose Ourselves and mapping to TPB. Let’s Choose Ourselves began with an outline of what to expect; an introduction to the topic of adolescent driving and inattention to the roadway; a section on cell phone calls, texting and social media apps; a section on peer passengers; and lastly a conclusion to bring all of the information together. Let’s Choose Ourselves included free-answer questions (e.g., What are some things you like about driving?), interactive activities (e.g., click and find out), multiple choice questions (e.g., What are some scenarios when you might want to use the phone for texting or social media apps?), and videos from a driving simulator displaying what can happen when an adolescent is talking on the phone, texting, using a social media app or has a passenger that is taking attention away from the roadway. Participants moved through each slide, using the mouse to advance to the next slide. Participants were not able to move to another slide if they did not complete the activity; for example if they did not complete a question.
Table 3.
Example Content in the Intervention Let’s Choose Ourselves Mapped to TPB Theoretical Construct
| Themes from Focus Groups (Phase I) | Example Content in the Intervention (Phase II & III) | TPB Theoretical Construct |
|---|---|---|
| Recognizing danger of cell phones but still engaging while driving |
|
Knowledge Attitudes |
| Considering context on whether to use the phone |
|
Attitudes PBC |
| Formulating safer behaviors that might reduce risk of cell phone use |
|
PBC PBC Subjective Norms |
| “Good and not good” passengers |
|
Knowledge Attitudes |
| Passengers and technology as harmful and helpful |
|
Attitudes PBC |
| The driver is in charge |
|
PBC Subjective Norms |
We addressed attitudes about cell phones and passengers in Let’s Choose Ourselves. For example, participants indicated in the Phase I focus groups that texting and hand-held calls were dangerous, however hands free communication was described as safer. Thus, facts and activities in the intervention reinforced how both hand-held and hands-free communications were unsafe and dangerous. Our focus group discussion results also indicated that participants did not perceive peer passenger interactions to be dangerous. To address this knowledge gap, we included factual information about passengers and activities to demonstrate the danger of being distracted by peer passengers; we described the increase in fatal crash risk, and provided driving simulation video examples of how peers can be distracting.
Relative to PBC, participants described the driver as being in control and therefore Let’s Choose Ourselves provided tools and examples of how they can increase the confidence they have in handling their phone and potentially distracting peers. Participants were given a menu of options with practical solutions about what they could do to avoid using their phones and limit passenger distractions. The menus of options helped to personalize the intervention by giving freedom to choose what worked for them (e.g., let the call go to voicemail, have passengers handle the phone, use parents as an excuse to drive only one friend at a time and developing rules of the car).
With respect to subjective norms (perceived social pressure to perform or not perform a behavior), participants were provided interactive information and opportunities (free answer write-ins) in Let’s Choose Ourselves to share their own thoughts on what they would say to family and friends about not answering calls/text and passenger limits. For example, participants were shown phrases they could say to friends or family about limiting cell phone use and opportunities to develop their own. Within each of the interactive activities for attitudes, PBC and norms, participants were given the option to report that they didn’t like any of the choices.
Phase II Results (Beta and Pilot Testing the Intervention)
Once initial versions of Let’s Choose Ourselves were developed, a new sample of adolescent and young adult drivers helped us carry out beta-testing by reviewing content and provided feedback on how to refine and improve the intervention. We presented the intervention to five adolescents and young adults in individual and small group sessions (20% female; 100% White, 20% Hispanic; mean age 18.53 years (SD=0.69); and mean licensure length 20.50 months (SD=12.44). One session was one-on-one, while the other two sessions occurred in small groups of two. Participants were compensated $20. While study team members took notes, the participants identified problems (technical, content or theory-based), suggested improvements, and recommended clarifications for the intervention.
In response to the beta-testing, participants suggested refinements of language, word choice, and directions of how to use the intervention; correction of programming errors; enhancement of transitions between sections and; edits to pictures, fonts, and colors. Overall, the participants responded positively to Let’s Choose Ourselves, citing it provided tools that might be helpful for driver inattention and was engaging. Not all suggestions could be implemented, such as addressing topics like “road rage,” using technological advances that were not possible (such as high-resolution graphics in video games) and providing adolescents with a print-out of their responses during the intervention.
Once the intervention was refined through beta-testing, we performed pilot-testing of the delivery of the intervention as an e-learning course through a secure LMS with three adolescents. These pilot participants were 2 male, 1 female; 2 White and 1 Black; mean age 17.20 years (SD= 0.30); and the mean length of licensure was 33 days (SD=22.61). The participants were compensated $25. In the pilot testing, our goal was to make sure we could carry out planned procedures and identify any potential challenges, particularly with the intervention. This included completion of consent and assent procedures, surveys, simulated driving assessment and completion of the web-based intervention. Data from the pilot participants in Phase II would not be used in analysis of the effects of the intervention in the larger RCT.
Phase III Feasibility Methods (Randomized Controlled Trial)
Phase I and II led to the production of a web-based intervention that allowed us to track data on participant interactions in the intervention, time spent on the intervention and completion statistics. For Phase III of the development of the intervention, we carried out an RCT with adolescents ages 16–17 licensed for ≤90 days in Pennsylvania. We focus here on the process to establish feasibility of the intervention and we do not report on the outcomes of the RCT. We used the following criteria to determine feasibility: 1) Recruitment rates; 2) Enrollment rates; 3) Completion rates of the web-based intervention activities; and 4) Retention rates.
In the design of the RCT, we planned four study visits over the course of six months: Baseline (Visit 1), 1-month follow-up (Visit 2), 3-month follow-up (Visit 3) and 6-month follow-up (Visit 4). The Baseline and Visit 3 were in-person visits and included self-report questionnaires and a simulated driving assessment with eye tracking device to assess driving behaviors. The intervention was completed at Visit 1 after self-report surveys and the simulated driving assessment with eye tracker. The Visit 2 and Visit 4 included questionnaires on-line through a secure online survey (REDCap®) (Harris et al., 2009). Participants were compensated $25 for each study visit. An a priori power analysis indicated that a sample of 60 participants would yield at least 80% power to detect an effect size as small as 0.30 (Cohen’s d, which is equivalent to an eta-squared of 0.02) for the interaction between group and time in the 2×2 Mixed Design ANOVA, given up to 50% attrition, a correlation of at least 0.50 between baseline and follow-up measurements, and alpha <= 0.05. We also obtained a Certificate of Confidentiality, had an Independent Safety Monitor and registered the trial with Clinicaltrials.gov (NCT02319317).
Phase III Feasibility Results (Randomized Controlled Trial)
Our recruitment efforts for the main RCT included: 5711 recruitment letters and 6385 emails (5501 emails repeated a second time) through the CHOP health care system. We also used strategies related to word of mouth, information sessions at two local high schools and emails to groups expressing interest in the study. We had 409 contacts made to our study team. Of the 409, 34.2% (n=140) did not meet eligibility criteria, 10.8% (n=44) were not interested, 6.1% (n=25) were unable to schedule, 0.7% (n=3) enrolled as the pilot participants and 33% (n=135) were lost to follow up. Sixty-two adolescents (15.2%) were consented and two were found to be ineligible. The final sample included 60 adolescents.
The sample was 66.7% female (n=40); 78.3% White, 15% Black or African American, 1.7% Asian, 3.3% more than 1 race and 1.7% reported other; none reported being Hispanic. The mean age of participants was 16.98 years (SD= 0.35), and the mean length of licensure was 50.77 days (SD=23.68). Participants were randomized to Let’s Choose Ourselves or a control group who received an on-line intervention not related to driving (content focused on healthy eating). Every teen who initiated the risky driving or the control intervention completed intervention activities through the secure LMS. The mean time to complete the risky driving intervention was 27.98 minutes, SD=5.67) (range: 15.03– 39.85 minutes). We had excellent retention in the study: 96.7% at Visit 2, 91.6% at Visit 3, and 93.3% at Visit 4.
Discussion
The development of Let’s Choose Ourselves, a web-based, interactive intervention to reduce adolescent driver inattention to the roadway, was a multi-phase development approach. As guided by TPB, we organized survey data and themes from focus group data by theoretical constructs: attitudes toward inattention to the roadway, risky driving behaviors related to driver inattention, PBCs over those driving behaviors, and subjective norms shaping intentions and driving behaviors. We then integrated these data with scientific literature on safe practices for adolescent drivers to develop an intervention to reduce adolescent driven inattention preparatory for an RCT.
Successful interventions targeting adolescent risk behaviors require theoretical underpinnings that address more than knowledge acquisition (Brawner et al., 2013; Cunningham et al., 2012; Dupont, Lemmens, Adriana, van de Mheen, & de Vries, 2015). Guided by the TPB in the focus group and survey methods, the data were targeted to address the perceptions of adolescent driver inattention of attitudes, PBCs, and norms that could then influence intentions and eventually behavior. The focus group findings helped to contextualize quantitative survey results, as well as provide realistic scenarios and strategies for the intervention participants (Miller, Wickliffe, Jahnke, Linebarger, & Dowd, 2014). For example, adolescents in the study overwhelmingly reported unfavorable attitudes towards texting while driving. Yet, they still reported engaging in texting in the past, as well as intentions to engage in the future. The focus group data indicated circumstances where adolescents described situations in which they would text. Therefore, the intervention specifically addresses this paradox and attempts to give adolescents the tools to change how they control their texting behaviors and intentions to text.
The development of Let’s Choose Ourselves presented certain challenges. First, study terminology was sometimes inconsistent with the adolescents’ terminology. For example, we framed the questions about passengers as “interactions with peer passengers,” a term that may have limitations because it was not specifically denoting negative behaviors. Instead of asking about general interactions with peer passengers, directly eliciting negative behaviors may have yielded more accurate data (e.g., how likely is it that you would be distracted by a peer passenger while driving?). In the focus groups, there was opportunity to expand on the topic, such as how passengers contribute to inattention to the roadway, being purposeful in distracting a driver, and perceptions of control of passenger behavior. Adolescents perceived that sometimes passengers can be helpful in maintaining attention to the roadway, while at other times they caused distractions which led to inattention to the roadway. For example, the focus group participants shared that peer passengers can help to manage texts, calls, or music or assist with directions, navigation programs, or phone apps. However, presence of adolescent passengers increases fatal crash risk for adolescent drivers (Ouimet et al., 2015; Tefft et al., 2012). Given that peer passengers provide both risk and protective factors, we included opportunities for both positive and negative influences when we addressed peer passengers in the intervention.
Distractions that draw attention away from the roadway are a serious public health problem for adolescent drivers. From a primary prevention perspective, multi-pronged approaches are necessary to reduce adolescent MVCs. Policies that restrict passengers and cell phone use, and those that encourage safe driving practices are necessary (Ferdinand et al., 2014; Williams et al., 2012). Technology-driven interventions such as in-vehicle monitoring and parental feedback show promise as well (McGehee, Raby, Carney, Lee, & Reyes, 2007; Simons-Morton et al., 2013). Although policies and technology in the vehicle may be critical to decreasing injury and fatalities related to adolescent MVCs, individualized interventions targeting adolescents’ self-regulation offer an innovative option to augment other public health strategies.
Future research in adolescent driver inattention should consider how individually targeted, behavior change interventions can be improved to address the risk behavior. For example, better understanding of the timing of delivery, as well as the dose and possible booster sessions associated with the intervention are important to consider (Pedlow & Carey, 2003). Adolescents in the focus groups described the learner phase as one optimal delivery timing, though during that process there are many diverse aspects of technical driving skill that adolescents need to master (Mirman et al., 2014; J. Mirman, Lee, Kay, Durbin, & Winston, 2012). It may be difficult to address issues such as attention in a targeted way if adolescents have not yet mastered how to drive.
Limitations
We acknowledge that the sample characteristics in the three phases may limit generalizability, and we are cautious not to over-interpret findings. For example, we had a small sample size in the focus group study, and beta- and pilot testing. However, the self-reported texting behaviors of the adolescents in our focus group sample (46.7%) was consistent with data from the nationally representative sample of the YRBS (45%) (Olsen et al., 2013). In addition, this was a non-representative sample with a lack of diversity. The self-report data, however, indicated that there was heterogeneity in the number of passengers, cell phone use and crash history across participants. Given the identified risk behaviors related to driving, call phones and passengers, we created a theoretically-driven intervention that addresses risk behaviors identified at the national level.
Implications for School Nurses
The implications of this research are two-fold: providing information on how to develop a theoretically based intervention and identifying ways that school nurses can address a major area in health promotion. The step-by-step approach, along with the challenges and limitations, indicate for school nurses how intervention development can be carried out. Given their placement with community, school nurses are in an optimal position to contribute to the design of theoretically based interventions for students (Hoying & Melnyk, 2016; Tucker & Lanningham-Foster, 2015; Zapolski & Smith, 2016). For example, school nurses in rural school districts may identify additional factors related to their geographic location that require attention in MVC prevention interventions. In addition, school nursing is a critical component to the implementation of prevention-based interventions with adolescents. Their role in helping assess feasibility of interventions is particularly important, as school nurses have information on parental engagement in health care issues of students, compliance with health standards, and unique needs of their student populations. As evidenced-based interventions become available, school nurses have the opportunity to be a part of implementation and coordination of efforts related to other services (e.g. psychological services in the school) and programs.
Conclusion
We have outlined a process for a multi-phase development approach to develop and refine a theoretically-grounded intervention to reduce novice driver inattention to the roadway. The necessary steps of beta and pilot testing allowed us to see theoretical and content issues with the intervention. Adolescent driver crashes remain a public health threat. Passengers and cell phones contribute to inattention to the roadway. Individually targeted, theoretically-grounded interventions that address risky behaviors are needed to help minimize adolescent driver crashes associated with inattention. The steps we described for this newly developed intervention aims to aid in school nurses’ efforts to fill this gap in the science.
Acknowledgments
This research was supported by the National Institute of Nursing Research of the National Institutes of Health under Award Number K99/R00NR013548 (PI: McDonald). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors wish to thank Flaura K. Winston, MD, PhD for her contributions. We would also like to thank the Pediatric Research Consortium at the Children’s Hospital of Philadelphia for their assistance in recruitment. Lastly, we thank the participants in this study.
Contributor Information
Catherine C. McDonald, Department of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA; Center for Injury Research and Prevention, The Children’s Hospital of Philadelphia, Philadelphia, PA, USA.
Bridgette M. Brawner, University of Pennsylvania, School of Nursing, Philadelphia, PA 19104-4217.
Jamison Fargo, Utah State University, Department of Psychology, Logan, UT 84322.
Jennifer Swope, The Children’s Hospital of Philadelphia, Philadelphia, PA, USA.
Marilyn S. Sommers, University of Pennsylvania, School of Nursing, Philadelphia, PA 19104-4217.
References
- Ajzen I. Behavioral interventions based on the Theory of Planned Behavior. n.d. Retrieved March 14, 2016, from http://people.umass.edu/~aizen/pdf/tpb.intervention.pdf.
- Ajzen I. The Theory of Planned Behavior. Organ Behav Hum Decis Process. 1991;50:179–211. [Google Scholar]
- Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall; 1980. [Google Scholar]
- Armitage CJ, Talibudeen L. Test of a brief theory of planned behaviour-based intervention to promote adolescent safe sex intentions. British Journal of Psychology. 2010;101(1):155–172. doi: 10.1348/000712609X431728. [DOI] [PubMed] [Google Scholar]
- Brawner BM, Baker JL, Voytek CD, Leader A, Cashman RR, Silverman R, Frank I. The development of a culturally relevant, theoretically driven HPV prevention intervention for urban adolescent females and their parents/guardians. Health Promot Pract. 2013;14(4):624–636. doi: 10.1177/1524839912462389. [DOI] [PubMed] [Google Scholar]
- Carney C, Mcgehee DV, Harland K, Weiss M, Raby M. Using naturalistic driving data to assess the prevalence of environmental factors and driver behaviors in teen driver crashes. Washington DC: 2015. Retrieved from https://www.aaafoundation.org/sites/default/files/2015TeenCrashCausationReport.pdf. [Google Scholar]
- Centers for Disease Control and Prevention. Motor vehicle crash injuries: Costly but preventable. 2014 Retrieved September 29, 2016, from http://www.cdc.gov/vitalsigns/crash-injuries/index.html.
- Centers for Disease Control and Prevention. Teen drivers: Fact sheet. 2016 Retrieved March 2, 2017, from http://www.cdc.gov/Motorvehiclesafety/teen_drivers/teendrivers_factsheet.html.
- Chen LH. Carrying Passengers as a risk factor for crashes fatal to 16- and 17-year-old drivers. JAMA. 2000;283(12):1578–1582. doi: 10.1001/jama.283.12.1578. [DOI] [PubMed] [Google Scholar]
- Cunningham RM, Chermack ST, Zimmerman MA, Shope JT, Bingham CR, Blow FC, Walton MA. Brief motivational interviewing intervention for peer violence and alcohol use in teens: one-year follow-up. Pediatrics. 2012;129(6):1083–90. doi: 10.1542/peds.2011-3419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curry AE, Hafetz J, Kallan MJ, Winston FK, Durbin DR. Prevalence of teen driver errors leading to serious motor vehicle crashes. Accid Anal Prev. 2011;43(4):1285–1290. doi: 10.1016/j.aap.2010.10.019. [DOI] [PubMed] [Google Scholar]
- Curry AE, Mirman JH, Kallan MJ, Winston FK, Durbin DR. Peer passengers: How do they affect teen crashes? J Adolesc Health. 2012;50(6):588–94. doi: 10.1016/j.jadohealth.2011.10.016. [DOI] [PubMed] [Google Scholar]
- Dupont HB, Lemmens P, Adriana G, van de Mheen D, de Vries NK. Developing the Moti-4 intervention, assessing its feasibility and pilot testing its effectiveness. BMC Public Health. 2015;15:500. doi: 10.1186/s12889-015-1826-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferdinand AO, Menachemi N, Sen B, Blackburn JL, Morrisey M, Nelson L. Impact of texting laws on motor vehicular fatalities in the United States. American Journal of Public Health. 2014;104(8):1370–7. doi: 10.2105/AJPH.2014.301894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Predicting and changing behavior: The reasoned action approach. New York: Psychology Press; 2010. [Google Scholar]
- Fisher DL, Laurie NE, Glaser R, Connerney K, Pollatsek A, Duffy SA, Brock J. Use of a fixed-base driving simulator to evaluate the effects of experience and PC-Based Risk Awareness Training on drivers’ decisions. Human Factor. 2002;44(2):287–302. doi: 10.1518/0018720024497853. [DOI] [PubMed] [Google Scholar]
- Governors Highway Safety Association. Teen and Novice Drivers. 2016 Retrieved March 23, 2017, from http://www.ghsa.org/state-laws/issues/Teen-and-Novice-Drivers.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Information. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoying J, Melnyk BM. COPE: A Pilot Study With Urban-Dwelling Minority Sixth-Grade Youth to Improve Physical Activity and Mental Health Outcomes. The Journal of School Nursing. 2016;32(5):347–356. doi: 10.1177/1059840516635713. [DOI] [PubMed] [Google Scholar]
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qualitative Life Research. 2005;15(9):1277–1288. doi: 10.1177/1049732305276687. [DOI] [PubMed] [Google Scholar]
- Jemmott JB, Jemmott LS, Fong GT, Morales KH. Effectiveness of an HIV/STD risk-reduction intervention for adolescents when implemented by community-based organizations: A cluster-randomized controlled trial. American Journal of Public Health. 2010;100(4):720–726. doi: 10.2105/AJPH.2008.140657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klauer SG, Guo F, Simons-Morton BG, Ouimet MC, Lee SE, Dingus TA. Distracted driving and risk of road crashes among novice and experienced drivers. New England Journal of Medicine. 2014;370(1):54–59. doi: 10.1056/NEJMsa1204142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koning IM, van den Eijnden RJ, Verdurmen JE, Engels RC, Vollebergh WA. Long-term effects of a parent and student intervention on alcohol use in adolescents: A cluster randomized controlled trial. American Journal of Preventive Medicine. 2011;40(5):541–547. doi: 10.1016/j.amepre.2010.12.030. [DOI] [PubMed] [Google Scholar]
- Lenhart A, Ling R, Campbell S, Purcell K. Teens and Mobile Phones. 2010 Retrieved September 26, 2016 from http://www.pewinternet.org/2010/04/20/teens-and-mobile-phones/
- Mayhew DR, Simpson HM, Pak A. Changes in collision rates among novice drivers during the first months of driving. Accident Analysis and Prevention. 2003;35(5):683–691. doi: 10.1016/s0001-4575(02)00047-7. [DOI] [PubMed] [Google Scholar]
- McCartt AT, Shabanova VI, Leaf WA. Driving experience, crashes and traffic citations of teenage beginning drivers. Accident Analysis and Prevention. 2003;35(3):311–320. doi: 10.1016/s0001-4575(02)00006-4. [DOI] [PubMed] [Google Scholar]
- McDonald CC, Sommers MS. Teen drivers’ perceptions of inattention and cell phone use while driving. Traffic Injury Prevention. 2015;16(S2):S52–8. doi: 10.1080/15389588.2015.1062886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonald CC, Sommers MS. “Good Passengers and Not Good Passengers:” Adolescent Drivers’ Perceptions About Inattention and Peer Passengers. Journal of Pediatric Nursing. 2016;31(6):e375–e382. doi: 10.1016/j.pedn.2016.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGehee DV, Raby M, Carney C, Lee JD, Reyes ML. Extending parental mentoring using an event-triggered video intervention in rural teen drivers. Journal of Safety Research. 2007;38(2):215–227. doi: 10.1016/j.jsr.2007.02.009. [DOI] [PubMed] [Google Scholar]
- Miller MK, Wickliffe J, Jahnke S, Linebarger JS, Dowd D. Accessing general and sexual healthcare: Experiences of urban youth. Vulnerable Child Youth Studies. 2014;9(3):279–290. doi: 10.1080/17450128.2014.925170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mirman JH, Curry AE, Winston FK, Wang W, Elliott MR, Schultheis MT, Durbin DR. Effect of the teen driving plan on the driving performance of teenagers before licensure: a randomized clinical trial. JAMA Pediatrics. 2014;168(8):764–71. doi: 10.1001/jamapediatrics.2014.252. [DOI] [PubMed] [Google Scholar]
- Mirman J, Lee YC, Kay J, Durbin DR, Winston FK. Development of a web-based parent support program to improve the quantity, quality and diversity of teens’ home-based practice driving. Transportation Research Record: Journal of the Transportation Research Board. 2012;2318:107–115. [Google Scholar]
- Olsen EO, Shults RA, Eaton DK. Texting while driving and other risky motor vehicle behaviors among US high school students. Pediatrics. 2013;131(6):e1708–e1715. doi: 10.1542/peds.2012-3462. [DOI] [PubMed] [Google Scholar]
- Ouimet MC, Pradhan AK, Brooks-Russell A, Ehsani JP, Berbiche D, Simons-Morton BG. Young drivers and their passengers: A systematic review of epidemiological studies on crash risk. J Adolesc Health. 2015;57(1 Suppl):S24–S35.e6. doi: 10.1016/j.jadohealth.2015.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedlow CT, Carey MP. HIV sexual risk-reduction interventions for youth: A review and methodological critique of randomized controlled trials. Behavior Modification. 2003;27(2):135–190. doi: 10.1177/0145445503251562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polit D. Nursing research: Principles and methods. 7th. Philadelphia, PA: Lippincott Williams and Wilkins; 2004. [Google Scholar]
- Regan MA, Hallett C, Gordon CP. Driver distraction and driver inattention: Definition, relationship and taxonomy. Accid Anal Prev. 2011;43(5):1771–1781. doi: 10.1016/j.aap.2011.04.008. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Bingham CR, Falk EB, Li K, Pradhan AK, Ouimet MC, Shope JT. Experimental effects of injunctive norms on simulated risky driving among teenage males. Health Psychology. 2014;33(7):616–27. doi: 10.1037/a0034837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons-Morton BG, Bingham CR, Ouimet MC, Pradhan AK, Chen R, Barretto A, Shope JT. The effect on teenage risky driving of feedback from a safety monitoring system: A Randomized Controlled Trial. The Journal of Adolescent Health. 2013:21–26.e. doi: 10.1016/j.jadohealth.2012.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons-Morton BG, Hartos J, Leaf WA, Preusser DF. The effect on teen driving outcomes of the Checkpoints Program in a state-wide trial. Accidident Analysis and Prevention. 2006;38(5):907–912. doi: 10.1016/j.aap.2006.03.001. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Ouimet MC, Zhang Z, Klauer SE, Lee SE, Wang J, et al. The effect of passengers and risk-taking friends on risky driving and crashes/near crashes among novice teenagers. The Journal of Adolescent Health. 2011;49(6):587–93. doi: 10.1016/j.jadohealth.2011.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons-Morton B, Lerner N, Singer J. The observed effects of teenage passengers on the risky driving behavior of teenage drivers. Accidident Analysis and Prevention. 2005;37(6):973–82. doi: 10.1016/j.aap.2005.04.014. [DOI] [PubMed] [Google Scholar]
- Sommers BD, Fargo JD, Lyons MS, Shope JT, Sommers MS. Societal costs of risky driving: an economic analysis of high-risk patients visiting an urban emergency department. Traffic Injury Prevention. 2011;12(2):149–158. doi: 10.1080/15389588.2010.536599. [DOI] [PubMed] [Google Scholar]
- Tefft BC, Williams AF, Grabowski JG. Teen driver risk in relation to age and number of passengers, United States, 2007–2010. Traffic Injury Prevention. 2012;14(3):283–292. doi: 10.1080/15389588.2012.708887. [DOI] [PubMed] [Google Scholar]
- Tucker S, Lanningham-Foster LM. Nurse-led school-based child obesity prevention. The Journal of School Nursing. 2015;31(6):450–466. doi: 10.1177/1059840515574002. [DOI] [PubMed] [Google Scholar]
- Williams AF, Tefft BC. Characteristics of teens-with-teens fatal crashes in the United States, 2005–2010. Journal of Safety Research. 2014;48:37–42. doi: 10.1016/j.jsr.2013.11.001. [DOI] [PubMed] [Google Scholar]
- Williams AF, Tefft BC, Grabowski JG. Graduated Driver Licensing Research, 2010-Present. Journal of Safety Research. 2012;43(3):195–203. doi: 10.1016/j.jsr.2012.07.004. [DOI] [PubMed] [Google Scholar]
- Zakrajsek JS, Shope JT, Greenspan AI, Wang J, Bingham CR, Simons-Morton BG. Effectiveness of a brief parent-directed teen driver safety intervention (Checkpoints) delivered by driver education instructors. Journal of Adolesc Health. 2013;53(1):27–33. doi: 10.1016/j.jadohealth.2012.12.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TCB, Smith GT. Pilot Study: Implementing a brief DBT skills Program in schools toreduce health risk behaviors among early adolescents. The Journal of School Nursing 2016 [Google Scholar]