

Abstract
Case series
Patient: —
Final Diagnosis: —
Symptoms: Skin lesions
Medication: —
Clinical Procedure: —
Specialty: Dermatology
Objective:
Unusual or unexpected effect of treatment
Background:
Vitiligo, also known as leukoderma, is an autoimmune skin condition that results in the loss of melanin pigment. Vitiligo is not a rare condition but is difficult to treat and is associated with psychological distress.
Case Reports:
A series of 14 cases of vitiligo are presented that were treated with individualized homeopathic remedies that were based on plant, animal, or mineral compounds. There were 13 women and one man in the case series, with a mean age 29.8 years, and a mean follow-up from treatment of 58 months. The mean time between the onset of the appearance of vitiligo and the first consultation at our clinic was 96 months. Homeopathic treatment for patients is holistic and was performed on an individualized basis as described in this case series. Photographic images of the skin are presented before and after treatment.
Conclusions:
In 14 patients with vitiligo treated with individualized homeopathy, the best results were achieved in the patients who were treated in the early stages of the disease. We believe that homeopathy may be effective in the early stages of vitiligo, but large controlled clinical studies are needed in this area.
MeSH Keywords: Autoimmune Diseases, Case Reports, Complementary Therapies, Dermatology, Homeopathy, Vitiligo
Background
Vitiligo is an acquired autoimmune condition that is characterized by the destruction of epidermal melanocytes causing loss of skin pigment [1]. Vitiligo may progress to involve the dermal follicular reserve and to destroy melanocyte stem cells [1]. Although the global prevalence of vitiligo is less than 1%, in some populations, it may be as high as 3% of the population [1]. Classically, vitiligo has been classified into segmental and non-segmental variants, depending on the distribution of skin depigmentation [2]. Vitiligo can cause psychological stress, especially in dark-skinned individuals for whom it causes concerning cosmetic skin changes. Also, in some parts of the world, such as in rural India, vitiligo is considered to be a social stigma, particularly for young girls.
Vitiligo is an autoimmune condition in which multiple immune response genes are believed to be involved [3]. Studies have shown that vitiligo may be caused by a response to oxidative stress, mediated by T-cells and involving mediators such as tumor necrosis factor alpha (TNFα), heat shock protein 70 (Hsp70), and interleukin 1 alpha (IL-1α) [4–6]. Melanocyte destruction is initiated by an imbalance in the production of reactive oxygen species (ROS) that causes free radical damage to the skin melanocytes, leading to protein structural damage, cell apoptosis, activation of cytokines, and damage to cell endoplasmic reticulum (ER) [4–6]. The severity of vitiligo may be assessed by measuring superoxide dismutase, a byproduct of oxidative stress that increases when vitiligo is active but regresses when the lesions become stable [4–6]. Cytokines and chemokines such as C-C chemokine ligand 5 (CCL5), CXC chemokine ligand 12 (CXCL12), interleukin 1 alpha (IL-1α), and tumor necrosis factor alpha (TNFα) have been shown to have a major role in inducing autoantigen presentation and recruitment of antigen-presenting cells (APCs) and activated T-cells and to have a role in destruction of the skin melanocytes, supporting the autoimmune etiology of vitiligo [1,7–11].
Currently, the available treatment options for patients with vitiligo have limited effectiveness, particularly for patients with vitiligo of the acral areas, which are resistant to treatment due to the lack of hair follicles that can serve as reservoirs for melanocytes [1,2]. The criteria for assessing the response to the treatment of vitiligo include: cessation of spread; the appearance of skin re-pigmentation; and overall quality of life during treatment [1,12–14]. However, no therapeutic study has yet shown long-term benefits using these criteria, and further research is required to establish evidence for the effective treatment of vitiligo [1,12–14]. There has been at least one prospective observational clinical study that has investigated the effectiveness of classical homeopathic treatment of vitiligo [15], with a further prospective observational clinical study involving homeopathic treatments given based on characteristic individualized patient symptoms [16,17]. However, to our knowledge, we now report the first retrospective case series describing the long-term effects of the homeopathic treatment of vitiligo.
Case Report
A series of 14 cases of vitiligo are presented that were treated with individualized homeopathic treatments that were based on plant, animal, or mineral compounds (Table 1). There were 13 women and one man in the case series, with a mean age 29.8 years, and a mean follow-up from treatment of 58 months. The mean time between the onset of the appearance of vitiligo and the first consultation at our clinic was 96 months. Homeopathic treatment for patients is holistic and was performed on an individualized basis. Photographic images of the skin are presented before and after treatment (Figures 1–14). All patients were treated were treated according to the laws of classical homeopathy [18,19].
Table 1.
Summary of homeopathic treatments and outcome in 14 patients with vitiligo.
| Case number | Time from onset of vitiligo to homeopathic consultation | Initial presentation | Associated medical conditions | Homeopathic treatment prescribed | Follow-up |
|---|---|---|---|---|---|
| 1 (Figure 1A, 1B) | 2 months | 26-year-old woman with white discoloration on the left brow and cheek | Stramonium (Datura stramonium, or jimsonweed) | 2015 to 2016 (eight months). Still under treatment. Vitiligo patches undergoing re-pigmentation |
|
| 2 (Figure 2A, 2B) | 3 months | 36-year-old man with extensive white discoloration of the skin, spreading very quickly, and itching all over the body. High fever three months before the vitiligo began | Phosphorus. Psorinum. Stramonium |
2010 to 2014 (four years). Vitiligo patches undergoing re-pigmentation |
|
| 3 (Figure 3A, 3B) | 3 months | 28-year-old woman with progressive white discoloration over the face and back. Early menses, but hormonal status could not be confirmed |
Anemia. | Phosphorus. Nitric acid (for painful, ulcerated corns) |
2009 to 2016 (seven years). Vitiligo patches undergoing re-pigmentation. Anemia improved |
| 4 (Figure 4A, 4B) | 18 months | 8-year-old girl with discoloration on the left leg | Stramonium. Sulphur. Natrum muriaticum |
2014 to 2016 (two years). Vitiligo patches undergoing re-pigmentation |
|
| 5 (Figure 5A, 5B) | 18 months | 80-year-old woman with progressive white discoloration on the face, hands, and knees | Hypothyroidism, asthma, rheumatism, and hypertension | Calcarea carbonica. Natrum muriaticum |
2008 to 2010 (two years). Vitiligo patches undergoing re-pigmentation. Thyroid hormones normalizing |
| 6 (Figure 6A–6D) | 2 years | 7-year-old girl with vitiligo patches that appeared all over the body, beginning as inflamed areas that then turned white. Maternal grandfather also had vitiligo |
Recurrent urinary tract infections | Elaps corallines. Crotalus horridus (timber rattlesnake) |
2014 to 2016 (two years) Vitiligo patches undergone re-pigmentation. Urinary tract infections have not recurred |
| 7 (Figure 7A, 7B) | 2 years | 24-year-old woman with bilateral vitiligo on both flanks, first on the right and then on the left. Recurrent severe headaches lasting for several days that were unresponsive to painkillers |
Anemia. | Ferrum metallicum. Belladonna. Lycopodium. Psorinum |
2011 to 2016 (five years and still under treatment). Left hip vitiligo patch fully recovered; right hip recovering. Headaches have improved |
| 8 (Figure 8A, 8B) | 2 years | 17-year-old girl with discolored spots on her face, spreading slowly. Painful menses, urticarial, and recurrent urinary tract infections |
Veratrum album. Gelsemium. Nux moschata |
2009 to 2010 (one year). Vitiligo patches recovered well. Complains of mild pain during menses |
|
| 9 (Figure 9A, 9B) | 3 years | 7-year-old girl with extensive white discoloration, around the ears, eyelid, lips, and chin. Corns removed from the soles of the feet | Allergic rhinitis. | Phosphorus. Stramonium. Lac caninum. Mercurius sulphuratus ruber |
2007 to 2016 (nine years). Slow coverage of vitiligo. Patient still on treatment. Improved rhinitis |
| 10 (Figure10 A, 10B) | 10 years | 30-year-old woman with progressive white discoloration of skin all over the body. Previous tuberculosis 20 years previously. A brother and paternal aunt had vitiligo, and two sisters had hypothyroidism |
Rheumatoid arthritis and hypothyroidism | Phosphorus. Tuberculinum. Stramonium. Carbo vegetabilis (for eruption of herpes zoster). Lyssinum |
2004 to 2016 (12 years) Vitiligo improved slowly. Thyroid hormone levels stabilized. Rheumatism stabilized with the patient returning to her job |
| 11 (Figure 11A, 11B) | 10 years | 35-year-old woman with a vitiligo patch over the right flank, which was slowly spreading | Anemia | Medorrhinum. Ferrum metallicum. Phosphorus. Lachesis. Ptelea trifoliata |
2013 to 2016 (three years, still under treatment). Very slow coverage of the vitiligo |
| 12 (Figure 12A, 12B) | 20 years | 24-year-old woman with vitiligo spreading slowly over the whole of her back | Painful menses. | Phosphorus. Lac caninum. Tuberculinum. Ignatia amara |
2005 to 2008 (three years). Vitiligo recovered fully. Menses became less painful |
| 13 (Figure 13A, 13B) | 25 years | 50-year-old woman with white discoloration of the face and ears. Past medical history of occasional severe headaches |
Nitric acid | 2015 to 2016 (one year, but still under treatment). Vitiligo recovering, but slowly |
|
| 14 (Figure 14A, 14B) | 35 years | 46-year-old woman with extensive white discoloration all over the body | Hypothyroidism | Natrum muriaticum. Fluoricum acidum. Staphysagria. Elaps corallinus |
2009 to 2016 (seven years, still under treatment). Vitiligoi patches repigmenting well; thyroid function has remained normal |
Figure 1.

Case 1. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 2.

Case 2. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 3.

Case 3. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 4.

Case 4. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 5.

Case 5. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 6.
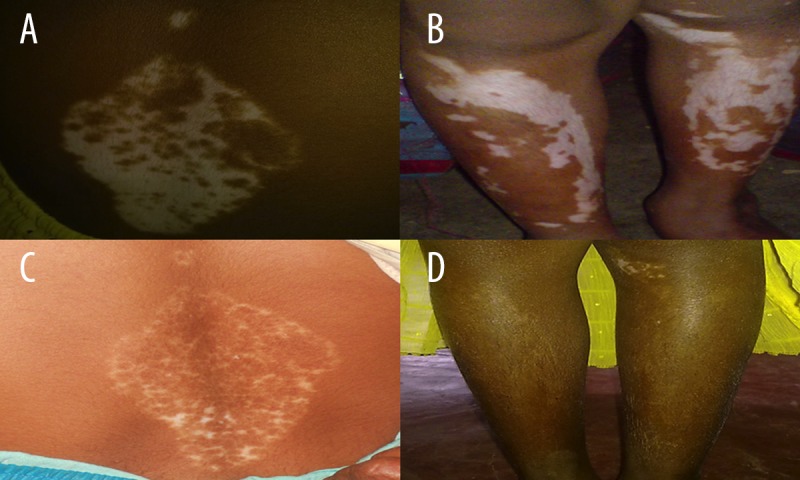
Case 6. (A) The appearance of the skin before treatment. (B) The appearance of the skin before treatment. (C) The appearance of the skin during treatment. (D) The appearance of the skin during treatment.
Figure 7.

Case 7. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 8.

Case 8. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 9.

Case 9. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 10.

Case 10. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 11.

Case 11. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 12.

Case 12. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 13.

Case 13. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
Figure 14.

Case 14. (A) The appearance of the skin before treatment. (B) The appearance of the skin during treatment.
The selection of the homeopathic treatment for these 14 patients was made according to the individual patient symptoms. Initially, each patient was assessed in detail for their psychological and physical symptoms, and the homeopathic treatment was selected for each patient (Table 1). In most 12 out of the 14 cases, more than one homeopathic remedies was prescribed and was used sequentially (Table 1). Patients were followed-up during treatment for a mean time of 58 months. The cases that were treated in the early stages recovered more quickly and completely. However, in other cases, where the skin de-pigmentation had been established for a long period and did not resolve, once the homeopathic treatment began, other health problems improved well while the skin lesion covered very slowly.
Discussion
This retrospective study of a series of 14 cases of vitiligo treated with individualized homeopathic compounds showed that although vitiligo is a primary autoimmune disease of the skin, patients with vitiligo may have involvement of multiple systems of the body. This case series showed that prolonged periods of psychological stress might be involved in the onset and progression of the vitiligo. These associations may support the view that psychological stress and the onset of autoimmune conditions are closely connected [17].
Homeopathic medicine includes a holistic approach to the understanding of the patient and integrates this approach to provide individualized patient treatment [18,19]. Certain diseases may manifest when genetic predisposition combines with stress, and homeopathy recognizes these factors [18]. Homeopathy considers the patient’s susceptibility to certain kind of stress, which means that homeopathy can be more successful during the early development of a disease, even before conventional medicine usually begins [18,19].
The range of action of homeopathic medicine aims to strengthen the action of the immune system through the primary understanding that symptoms are an attempt by the immune system to achieve balance [18,19]. ’Through the application of the principle of resonance, the basis of homeopathic medicine is that if a substance is capable of producing a similar symptom profile in a healthy organism, then the likelihood of its strengthening of the body’s defense mechanisms in a diseased body with the same symptoms is great [18,19]. The fundamental pillar of the science of homeopathy is that ‘like cures like’ [19]. The basis for homeopathy is that any substance (plant, animal, mineral, or metal) that can affect the human health can serve as a medication, when in the right form. Homeopathic medicines are prepared through serial dilutions and using a frictional process called ‘succussion’ or potentization, resulting in no traceable ‘material’ left in the solution, therefore enabling a safe use of toxic substances that may otherwise prove fatal [20]. The symptoms obtained through ‘proving’ of the homeopathic compounds on healthy humans serve as the basis for their prescription in diseased individuals. Because the main therapeutic rule in homeopathy is Similia Similibus Curentur (let like be treated by like), homeopathy has the advantage of taking the causes of diseases and their effects into account [20]. Therefore, homeopathic treatment, when given in a timely fashion, may bring lasting improvement for autoimmune disease, when homeopathy is applied in the early stages [20].
The experience of a homeopath treating vitiligo is that the lesions may firstly stop spreading, and existing lesions do not increase in size, and no new lesions appear. Secondly, re-pigmentation may occur, and the borders of the lesions that were formerly diffuse become more clearly marked, indicating cessation of spread. The quality of life for the patient may improve and the symptoms of associated diseases, such as thyroid dysfunction, may also improve [21,22]. These clinical responses to homeopathic treatment in patients with vitiligo may be considered to be an ideal response to treatment [13]. However, for an optimal response to homeopathic treatment to occur, treatment should begin when the body has not suffered the effects of the disease for long and before the immune response becomes irreversible.
In the 14 cases of vitiligo treated with homeopathy and presented in this case series, the longer the time that elapsed between the onset of vitiligo and the homeopathic consultation, the more difficult it was to obtain a good clinical response. The cases of vitiligo that presented in the advanced stages required more homeopathic remedies and in a correct sequence to see clinical change. An explanation of these findings may have been that the health level of the patients had worsened with time and that the immune system needed more stimulation and time to bring about a positive clinical effect on vitiligo [23].
Conclusions
In 14 patients with vitiligo treated with individualized homeopathy, the best results were achieved in the patients who were treated in the early stages of their disease. We believe that homeopathy may be effective in the early stages of vitiligo, but large controlled clinical studies are needed in this area.
Abbreviations:
- APC
antigen-presenting cell;
- CCL5
C-C chemokine ligand 5;
- CXCL12
CXC chemokine ligand 12;
- ER
endoplasmic reticulum;
- IL-1α
interleukin 1 alpha;
- IL-1
interleukin 1;
- ROS
reactive oxygen species;
- TNFα
tumor necrosis factor alpha
Footnotes
Conflict of interest
None.
References:
- 1.Jain A, Mal J, Mehndiratta V, et al. Study of oxidative stress in vitiligo. Indian J Clin Biochem. 2010;26(1):78–81. doi: 10.1007/s12291-010-0045-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Taieb A. Intrinsic and extrinsic pathomechanisms in vitiligo. Pigment Cell Res. 2000;13(S8):41–47. doi: 10.1034/j.1600-0749.13.s8.9.x. [DOI] [PubMed] [Google Scholar]
- 3.Jin Y, Birlea S, Fain P, et al. Variant of TYR and autoimmunity susceptibility loci in generalized vitiligo. New Engl J Med. 2010;362(18):1686–97. doi: 10.1056/NEJMoa0908547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Alghamdi KM, Khurrum H, Taieb A, Ezzedine K. Treatment of generalized vitiligo with anti-TNF-α agents. J Drugs Dermatol. 2012;11(4):534–39. [PubMed] [Google Scholar]
- 5.Manga P, Elbuluk N, Orlow SJ. Recent advances in understanding vitiligo. F1000Research. 2016;5:F1000. doi: 10.12688/f1000research.8976.1. Faculty Rev-2234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eleftheriadou V, Whitton M, Gawkrodger D, et al. Future research into the treatment of vitiligo: where should our priorities lie? Results of the vitiligo priority setting partnership. Br J Dermatol. 2011;164(3):530–36. doi: 10.1111/j.1365-2133.2010.10160.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Maresca V, Roccella M, Roccella F, et al. Increased sensitivity to peroxidative agents as a possible pathogenic factor of melanocyte damage in vitiligo. J Invest Dermatol. 1997;109(3):310–13. doi: 10.1111/1523-1747.ep12335801. [DOI] [PubMed] [Google Scholar]
- 8.Rezk A, Kemp D, El-Domyati M, et al. Misbalanced CXCL12 and CCL5 chemotactic signals in vitiligo onset and progression. J Invest Dermatol. 2017;137(5):1126–34. doi: 10.1016/j.jid.2016.12.028. [DOI] [PubMed] [Google Scholar]
- 9.Yang L, Wei Y, Sun Y, et al. Interferon-gamma inhibits melanogenesis and induces apoptosis in melanocytes: A pivotal role of CD8+ cytotoxic T lymphocytes in vitiligo. Acta Derm Venereol. 2015;95(6):664–70. doi: 10.2340/00015555-2080. [DOI] [PubMed] [Google Scholar]
- 10.Xie H, Zhou F, Liu L, et al. Vitiligo: How do oxidative stress-induced auto-antigens trigger autoimmunity? J Dermatol Sci. 2016;81(1):3–9. doi: 10.1016/j.jdermsci.2015.09.003. [DOI] [PubMed] [Google Scholar]
- 11.Singh M, Shoab Mansuri M, Parasrampuria MA, Begum R. Interleukin 1-α: A modulator of melanocyte homeostasis in vitiligo. Biochem Anal Biochem. 2016;5:2. [Google Scholar]
- 12.Whitton M, Pinart M, Batchelor J, et al. Interventions for vitiligo. Cochrane Database Syst Rev. 2015;(2):CD003263. doi: 10.1002/14651858.CD003263.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Parsad D. A new era of vitiligo research and treatment. J Cutaneous Aesthetic Surg. 2013;6(2):63–64. doi: 10.4103/0974-2077.112664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Alsubait N, Mulekar S, Al Issa A. Failure of non-cultured melanocyte – keratinocyte transplantation in periungual vitiligo: A case report. J Dermatol Dermatol Surg. 2015;19(2):123–25. [Google Scholar]
- 15.Ganguly S, Saha S, Koley M, Mondal R. Homeopathic treatment of vitiligo: An open observational pilot study. Int J High Dilution Res. 2013;12(45):168–77. [Google Scholar]
- 16.Swami S, Dasgupta S, Basu S, Swarnakar G. Significant remission of vitiligo by ultradiluted alternative medicines. Asian Journal of Pharmaceutical Clinical Research. 2012;5(2):33–35. [Google Scholar]
- 17.Trapp E, Trapp M, Sampogna F, et al. Autonomic nervous tone in vitiligo patients – a case-control study. Acta Derm Venereol. 2015;95(2):169–72. doi: 10.2340/00015555-1896. [DOI] [PubMed] [Google Scholar]
- 18.Vithoulkas G, Carlino S. The “continuum” of a unified theory of diseases. Med Sci Monit. 2010;16(2):SR7–15. [PubMed] [Google Scholar]
- 19.Vithoulkas G. Homeopathy: The Energy Medicine. 1st ed. Athens: International Academy of Classical Homeopathy; 2013. The basic principles of homeopathy. [Google Scholar]
- 20.Vithoulkas G. The science of homeopathy. New York: Grove Press; 1980. pp. 91–92. [Google Scholar]
- 21.van Geel N, Speeckaert M, Brochez L, et al. Clinical profile of generalized vitiligo patients with associated autoimmune/autoinflammatory diseases. J Eur Acad Dermatol Venereol. 2013;28(6):741–46. doi: 10.1111/jdv.12169. [DOI] [PubMed] [Google Scholar]
- 22.Xianfeng C, Yuegen J, Zhiyu Y, et al. Pediatric patients with vitiligo in Eastern China: Abnormalities in 145 cases based on thyroid function tests and immunological findings. Med Sci Monit. 2015;21:3216–21. doi: 10.12659/MSM.894981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Vithoulkas G, Woensel E. Levels of health. Alonissos, Greece: International Academy of Classical Homeopathy; 2010. [Google Scholar]