

Abstract
Introduction:
Musculoskeletal disorders (MSD) have become significant problems for all health care workers especially dentists. This systematic review provides prevalence of MSD in dentists of Iran.
Material and Methods:
In this study all published literatures about MSD in Iranian dentists were selected without any time limits or other restrictions. However, it was found that the studies about MSD among Iranian dentist are very low.
Results:
The results of literatures investigations show that the prevalence was between 0.5% and 70%. The prevalence of pain in different regions includes; neck pain (0.7- 0.15), back pain (0.08 - 0.55), wrist pain (0.005-0.48), shoulder pain (0.08-0.5), knee pain (0.03- 0.25) and elbow pain (0.01- 0.2). The gender has no influence on the prevalence. Compare the results with other similar studies shows that the prevalence of MSD is an important issue in other area too.
Conclusion:
Results show that the prevalence of musculoskeletal problems is high in Iran. Therefore it is necessary conduct reliable and comprehensive epidemiological studies in this field to determine the causes of the problem more consciously; and propose appropriate solutions.
Keywords: prevalence, musculoskeletal, disorder, dentist, Iran
1. INTRODUCTION
Occupation influences on health, social and economic development of a society is very critical. Musculoskeletal disorders (MSD) are work related diseases and many factors can cause it (1, 2). MSD are injuries of muscles, ligaments, tendons, nerves, blood vessels, bones and joints, that cause pain in the neck, shoulder, arm, wrist, hands, upper and lower back, hips, knees and feet (3). They affect the musculoskeletal system including the nerves, tendons, muscles, and supporting structures such as intervertebral discs (4). In recent decades musculoskeletal disorders have been grown globally (5, 6). Health care workers face a wide range of hazards on the job including musculoskeletal diseases and the prevalence of musculoskeletal diseases among them is significant (7). According to WHO there are over 59 million workers on healthcare facilities who are exposed to a wide range of occupational hazards in result the incidence of work-related injuries and diseases is high in this group (8). These diseases lead to physical, emotional, economical and social consequences on healthcare workers and their families (9). Studies show that wide variety of workplace hazards such as infections, eye injuries, vibration, percutaneous exposure incidents, exposure to radiation, dental materials, noise, psychological conditions and musculoskeletal disorders exists in dental practice (10). Dentistry is a high-risk profession in MSD (11-13) and it has large effect on their practices (14). According to research wrong position of the body and lack of body movement of dentists are the major ergonomic factors involved in the development of musculoskeletal disorders (15). Uncomfortable and static position with repetitive movements of arms and hands in combination with postural loads of upper back and head, during the dental work for long time and also psychological stress have important role in engaging dentists with these musculoskeletal symptom (6,16-18). These occupational hazard causing absence from work and finally reduce the quality and productivity of their practices (19).
Due to high incidence of MSD among dentists in different areas of Iran and also the high impact of musculoskeletal disorders on dentist’s practices, this study investigated MSD among dentists in Iran.
2. MATERIALS AND METHODS
Data and analysis
In order to estimate the prevalence of musculoskeletal disorders including low back (LBP), shoulder and neck pain among Iranian dentists in the included studies, homogeneous items of data were analyzed. The core elements collected by the authors were information about sample size, gender, age, city and prevalence of LBP, shoulder and neck pain. Acceptable methodological quality was determined as the central tendency of the frequency distribution of methodological scores. The LBP, shoulder and neck pain prevalence data extracted from the methodologically acceptable studies were analyzed.
Search strategy
This study is a systematic review; meta-analysis of all published literatures has been done simultaneously and without any time limits or other restrictions. The papers were searched using the MEDLINE (PubMed) 1989 to 2014, Google scholar, Scopus, CINAHL (for English language) and the Iranian search engine included SID (Scientific Information Database, www.sid.ir) 2014, Irandoc (Iranian Research Institute for information Science and Irandoc.ac.ir) 2014, Iran-medex (www.iranmedex.com) 2014, Magiran (www.magiran.com) 2014 (for Persian [Farsi] language).
The search was done based on keyword in English for all motor engines and Persian phrase only for Persian electronic databases. The keywords included ‘‘dentist’’ combined with ‘‘musculoskeletal disorders’’ and ‘‘Iran’’ including all subheadings. Because of high frequency of unrelated search results we concluded to search with the word of “dentist” and then extract papers related to MSD. The Persian key words were equivalent to their English words, and all probable combinations were considered. All keywords searched electronically by three Boolean operators with explained search strategy separately. After completed search, reviewed all search result in databases separately based on title or running title of studies and related articles were selected. Then we excluded duplicated articles in English or Persian language.
Inclusion criteria
All studies included in this study, if had criteria including LBP prevalence report in any gender, without any limitations for study design in Persian or English languages. Clinical intervention articles and studies with explanation of technical details were excluded.
Methodological appraisal
Articles were reviewed separately by two reviewers. After excluding those who didn’t had inclusion criteria, data from the review entered in to the data collection forms. Then articles have been divided to 5 categories including infection problems, MSD, radiation problems, psychological problems and other problems. At all stages the disagreements between reviewers was addressed by group discussion. Cross sectional and analytical articles have been appraised with Modified STROBE questionnaire based on our purpose in this study.
Data extraction
Some data such as articles and author`s names, year of publication, region of the study, type of study, sample size, sampling methods, age and gender of participants, statistical method, confounders, inclusion criteria, prevalence of LBP, prevalence of shoulder and neck pain, assessment tool and variables were identified. All data that extracted into Office Excel sheets that created for this purpose.
Data analysis
All information was entered in the Excel 2012 and analyzed using STATA software (version 11), we examined homogeneity of data. The mean, frequency, distribution of SD (standard deviation) and inter-quartile range (IQR) with 95% confidence intervals were used for data analysis. Significant heterogeneity was determined for the pooled estimate. In order to compare the prevalence statistics reported in the included studies, the primary elements for homogeneity of data were analyzed. A standard test for heterogeneity examined the null hypothesis that the true prevalence is identical in every study. Articles heterogeneity was investigated in two stages by observing Forest plot and calculating I2.I2 defines the proportion of variation in prevalence estimates that is due to genuine variation in prevalence rather than sampling error. The essential quality reporting elements were established by the authors, which included information on gender, age and recall period (8). Acceptable methodological quality was determined as the central tendency of the frequency distribution of methodological scores. The LBP prevalence data extracted from the methodologically sound studies were analyzed.
Forest plots were showed the distribution of the data in rank order for prevalence estimate (lowest to highest ranks) and a vertical reference at the line of unity.
We estimated the potential influence of covariates on the prevalence estimates by a random effects regression model, using the Metaregression command in STATA. The Metaregression represented log odds ratios, which are presented as odds ratios with 95% confidence intervals.
A multivariate meta-regression model was constructed to investigate which covariates were associated with prevalence estimates if there was adjustment for other study covariates. The models were created by using a forward stepwise procedure and described in the results section.
Ethical considerations
In this study, published articles that examined dental health problems have been analyzed. To select articles has been made any restrictions on language, type of study, Journal and others; all searched papers have been checked. Researchers at all stages of the research were considered ethical instructions.
Limitations
Inclusion was limited to published reports as scientific papers in Iranian and international journals, and we did not look at the thesis and dissertation due to access restrictions. However, it is unlikely the details from those would have changed our overall conclusions.
3. RESULTS
In this review, 137 articles were included from database (SID, Iranmedex and Magiran, PubMed, CINAHL, Scopus and Web of science). 113 studies excluded after title and abstracts of articles reviewing (unrelated to this purpose and duplicated) then, 7 papers excluded after assessing for eligibility criteria. At the end, 17 articles were included (Figure 1). A total of 17 discrete studies were identified that investigated 2067 dentists for MSD. Characteristics of reviewed studies are presented in Table 1 and Figure 1.
Figure 1.
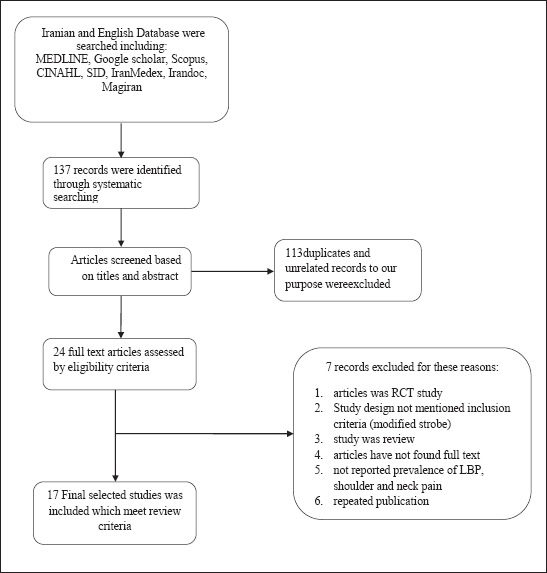
Search result flowchart
Table 1.
Methodological description of dentists MSD studies
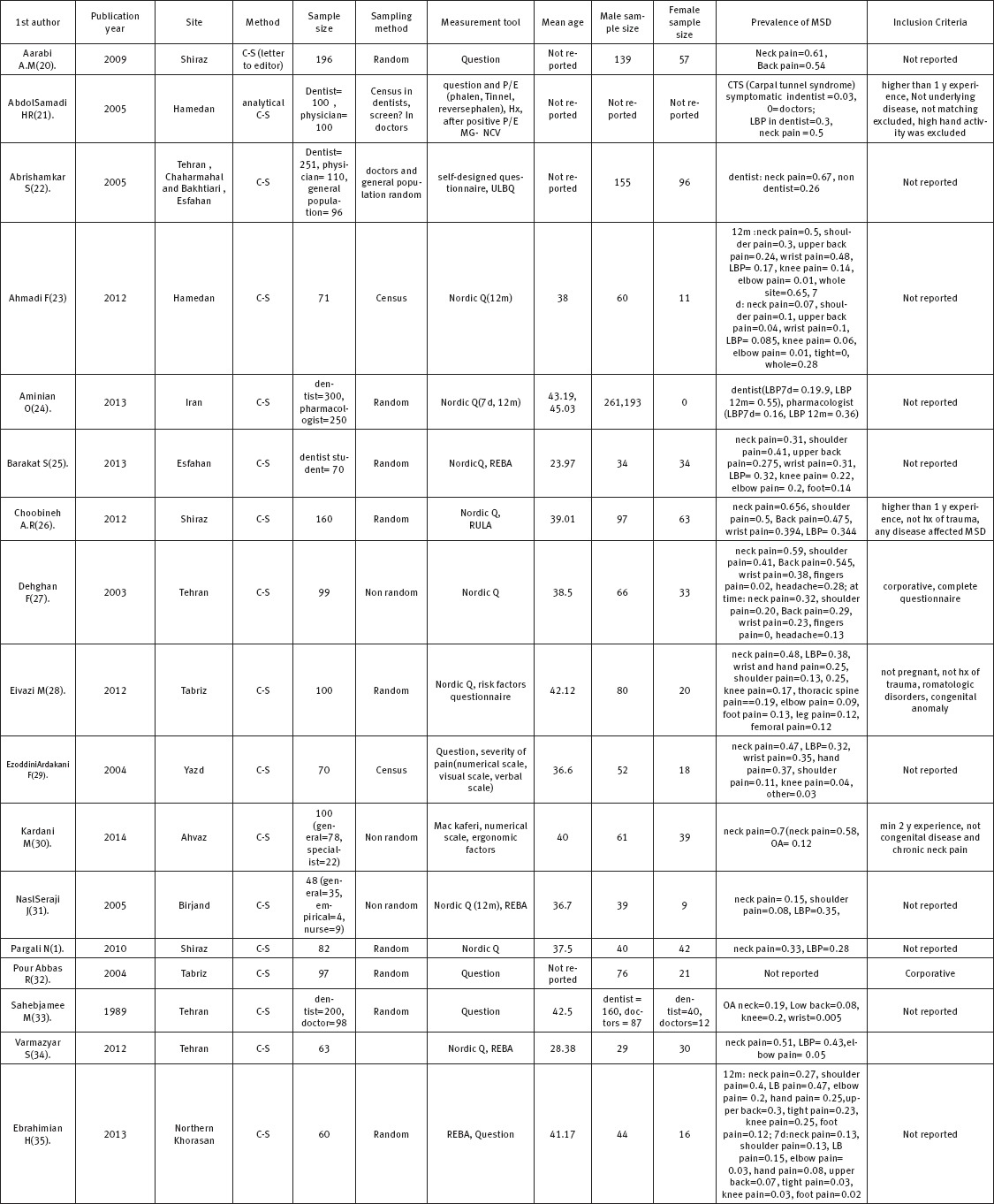
All papers studied the prevalence of MSD disorders in both sexes except one (472 men vs. 204 women). And 13 studies have been stated the mean age. The studies have been done according to Nordic or self-designed questionnaire.
Seventeen accepted studies in this review were between 1989 and 2013; and 9 studies reported musculoskeletal disorders with Nordic questionnaire. Among all musculoskeletal disorders every paper have been studied a part of MSD including neck pain in 15 studies, back pain in 14 studies, wrist pain in 7 studies, shoulder pain in 8 studies, knee and elbow pain in 6 studies, hand pain in 3 studies, foot pain in 2 studies, Carpal tunnel syndrome, thoracic spine, leg, femoral and finger pain in 1 study. The prevalence of pain in different regions including; neck pain (0.7-0.15), back pain (0.08-0.55), wrist pain (0.005-0.48), shoulder pain (0.08-0.5), knee pain (0.03-0.25) and elbow pain (0.01-0.2) (showed in Table 1).
Due to significant heterogeneity in the prevalence of musculoskeletal disorders, analyzes were conducted using Random Effect Model. Nine articles used Nordic questionnaire for assessment of MSD in dentists (Table 1).
Overall prevalence of neck pain in workers calculated 51% (I-squared= 98.6%, P=0.000) (Figure 2).
Figure 2.
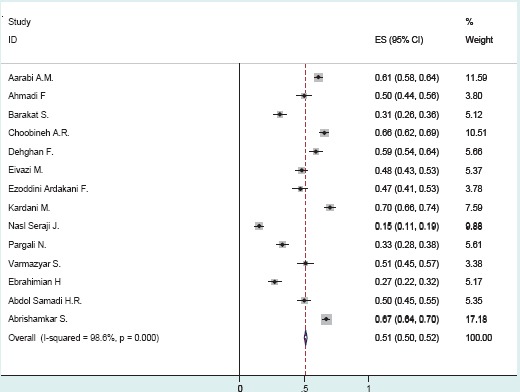
Forest plot of prevalence estimates and 95% confidence intervals from studies of prevalence of neck pain in workers
Gender was associated to prevalence of neck pain (P =-0.04, SE=-0.003) while mean age was not associated to prevalence of neck pain among dentists (p= 0.01, SE=0.01) (Table 2).
Table 2.
Association between prevalence of neck pain and gender of participants and Mean age
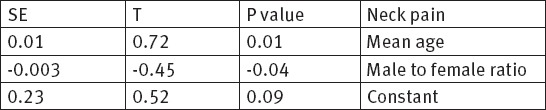
Table 2. Association between prevalence of neck pain and gender of participants and Mean age
Overall prevalence of low back pain in dentists calculated 42% (I-squared= 96.1%, P=0.000) (Figure 3).
Figure 3.
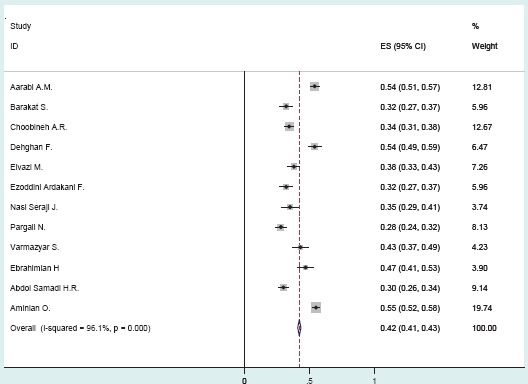
Forest plot of prevalence estimates and 95% confidence intervals from studies of prevalence of low back pain in workers
Gender was associated to prevalence of low back pain (P =-0.003, SE=0.017) while mean age was not associated to prevalence of low back pain among dentists (p= -0.05, SE= -0.001) (Table 3).
Table 3.
Association between prevalence of low back pain and gender of participants and Mean age
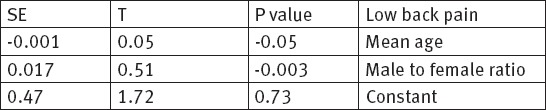
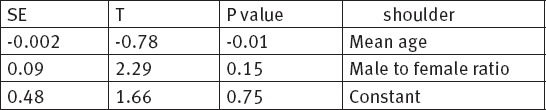
Table 3.
Association between prevalence of shoulder pain and gender of participants and Mean age
Overall prevalence of shoulder pain in workers calculated 18% (I-squared= 99.0%, P=0.000) (Figure 4).
Figure 4.
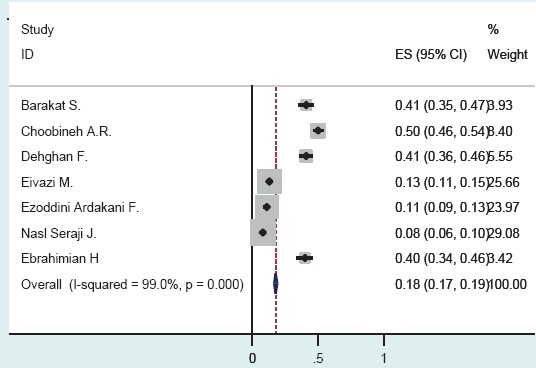
Forest plot of prevalence estimates and 95% confidence intervals from studies of prevalence of shoulder pain in workers
Gender was associated to prevalence of shoulder pain (p= 0.15, SE= 0.09) while mean age was not associated to prevalence of shoulder pain among dentists (p= -0.01, SE= -0.002) (Table 3).
The prevalence of neck pain, shoulder pain and back pain among dentists is obtained 51%, 18%, 42% respectively. That is not related to gender and age.
4. DISCUSSION AND CONCLUSION
Musculoskeletal problems, especially work-related ones are growing increasingly; one of the occupations that are encountering with these problems are medical workers such as dentists (35, 36). Although many studies have been done in this field globally but there are not comprehensive studies in Iran. Also most published studies are in Persian; therefore, a systematic review of these literatures was conducted.
According to the results of Meta-analysis the range of MSD problems in dentists were 0.5% to 70%. In similar studies such as Hay et al this range was reported 64%- 78% in dentists and 78% - 93% in dental staff and dental hygienist (3). The differences in the prevalence of musculoskeletal problems reported in various studies can be stem from individual and social varieties.
The highest reported problem in MSD was neck pain with the prevalence of 51% that is similar to studies in Queensland, Saudi Arabia and Netherlands (36). But this prevalence shows different results in other studies including Lalumandier et al in USA with 28%, Akesson in Sweden with 73%, Rucker in Canada with 61% Alexopoulos in Greek with 26%.
The variations in reported prevalence may be due to issues such as various measurement tools, cultural differences and the individual’s tasks. In some of these studies, in addition to dentists the sample includes dental staff and hygienists, but this study only include General dentists and specialists. High level of incidence in this group may be related to ergonomic problems such as unsuitable repetitive movements (37, 38), using vibrating instruments, bending forward at an angle of 15 degrees or sometimes up to 30 degrees for a long time (in 86% of the working time) with keeping up shoulder that caused a lot of pressure on the neck and shoulder (39). Psychosocial factors are another effective items, but detection the rate of impacts of every one of these factors is very difficult (37, 38).
Back pain with the prevalence of 42% (in different studies is reported 28%-55%) is the second, and shoulder pain with the prevalence of 18% (In different studies is reported 8%-50%) is the third high prevalence MSD among dentists. Hey et all in their systematic review study are reported back pain and neck pain as the most MDS complaints among dentists with the prevalence rates of 36.3%-60.1% and 19.8%-70% respectively. The results of Gupta et al study shows the neck pain with the most prevalence rate (57.5%) and back pain with moderate prevalence rate (53.7%). Results of our study are similar to the range reported in other studies.
In this study, neck pain and back pain is seen more in women than men, which is similar to other studies (3,39, 40). But in this study the effect of gender on the prevalence of neck pain has not been considered, which can be caused by sample size women than men in this study (407 men vs. 204 women). In only 13 of the mentioned studies in this study, the mean age was mentioned. However, our study found a correlation between aging and neck pain, that shows with increasing more dental neck pain have been reported. But with increasing age, lower back pain and shoulder pain, less has been reported. Also in study of Hays the negative relationship between musculoskeletal problems and aging has been seen (3). The differences can be seen in the reports comes from a variety of issues, including individual, cultural and social differences. In addition, items such as measurement tools, methods of asking question about the problems, economical issues and tools used by the dentists could be effective on the MSD problems (41). With the attention to the high prevalence of musculoskeletal problems reported in our country, and based on the results of this study, it seems there is a need to do more epidemiological studies in this area, and look more closely at the causes of the problem.
Footnotes
• Author Contribution: All authors participated in each step of research. N.S.S.H. revised it critically. All authors gave confirmation for final revised version to be submitted.
• Conflict of interest: none declared.
REFERENCES
- 1.Pargali N, Jowkar N. Prevalence of musculoskeletal pain among dentists in Shiraz, Southern Iran. The international journal of occupational and environmental medicine. 2010;1(2 April) [PubMed] [Google Scholar]
- 2.Mehrdad R, Dennerlein JT, Haghighat M, Aminian O. Association between psychosocial factors and musculoskeletal symptoms among Iranian nurses. American journal of industrial medicine. 2010;53(10):1032–9. doi: 10.1002/ajim.20869. [DOI] [PubMed] [Google Scholar]
- 3.Hayes M, Cockrell D, Smith D. A systematic review of musculoskeletal disorders among dental professionals. International journal of dental hygiene. 2009;7(3):159–65. doi: 10.1111/j.1601-5037.2009.00395.x. [DOI] [PubMed] [Google Scholar]
- 4.Osborne A, Blake C, Fullen BM, Meredith D, Phelan J, McNamara J, et al. Prevalence of musculoskeletal disorders among farmers: a systematic review. American journal of industrial medicine. 2012;55(2):143–58. doi: 10.1002/ajim.21033. [DOI] [PubMed] [Google Scholar]
- 5.Alexopoulos EC, Stathi I-C, Charizani F. Prevalence of musculoskeletal disorders in dentists. BMC musculoskeletal disorders. 2004;5(1):16. doi: 10.1186/1471-2474-5-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Alghadir A, Zafar H, Iqbal ZA. Work-related musculoskeletal disorders among dental professionals in Saudi Arabia. Journal of physical therapy science. 2015;27(4):1107. doi: 10.1589/jpts.27.1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mehrdad R, Morshedizadeh M. Musculoskeletal disorders and ergonomic hazards among Iranian physicians. Archives of Iranian medicine. 2012;15(6):370. [PubMed] [Google Scholar]
- 8.WHO. Health worker occupational health WHO2016. [[cited 2016]]. Available from: http://www.who.int/occupational_health/topics/hcworkers/en/
- 9.Dembe AE. The social consequences of occupational injuries and illnesses. American journal of industrial medicine. 2001;40(4):403–17. doi: 10.1002/ajim.1113. [DOI] [PubMed] [Google Scholar]
- 10.Hodacova L, Sustova Z, Cermakova E, Kapitan M, Smejkalova J. Self-reported risk factors related to the most frequent musculoskeletal complaints among Czech dentists. Industrial health. 2015;53(1):48. doi: 10.2486/indhealth.2013-0141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Leggat PA, Smith DR. Musculoskeletal disorders self reported by dentists in Queensland, Australia. Australian dental journal. 2006;51(4):324–7. doi: 10.1111/j.1834-7819.2006.tb00451.x. [DOI] [PubMed] [Google Scholar]
- 12.Hayes MJ, Smith DR, Taylor JA. Musculoskeletal disorders and symptom severity among Australian dental hygienists. BMC research notes. 2013;6(1):250. doi: 10.1186/1756-0500-6-250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Puriene A, Janulyte V, Musteikyte M, Bendinskaite R. General health of dentists. Literature review. Stomatologija. 2007;9(1):10–20. [PubMed] [Google Scholar]
- 14.Rafie F, Zamani Jam A, Shahravan A, Raoof M, Eskandarizadeh A. Prevalence of Upper Extremity Musculoskeletal Disorders in Dentists: Symptoms and Risk Factors. Journal of Environmental and Public Health. 2015;2015 doi: 10.1155/2015/517346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Szymańska J. Disorders of the musculoskeletal system among dentists from the aspect of ergonomics and prophylaxis. Ann Agric Environ Med. 2002;9(2):169–73. [PubMed] [Google Scholar]
- 16.Feng B, Liang Q, Wang Y, Andersen LL, Szeto G. Prevalence of work-related musculoskeletal symptoms of the neck and upper extremity among dentists in China. BMJ open. 2014;4(12):e006451. doi: 10.1136/bmjopen-2014-006451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Finsen L, Christensen H, Bakke M. Musculoskeletal disorders among dentists and variation in dental work. Applied ergonomics. 1998;29(2):119–25. doi: 10.1016/s0003-6870(97)00017-3. [DOI] [PubMed] [Google Scholar]
- 18.Kumar VK, Kumar SP, Baliga MR. Prevalence of work-related musculoskeletal complaints among dentists in India: a national cross-sectional survey. Indian Journal of Dental Research. 2013;24(4):428. doi: 10.4103/0970-9290.118387. [DOI] [PubMed] [Google Scholar]
- 19.Kierklo A, Kobus A, Jaworska Mg, Botuliñski Bo. Work-related muculoskeletal disorders among dentists-a questionnaire survey. Annals of Agricultural and Environmental Medicine. 2011;18(1) [PubMed] [Google Scholar]
- 20.Aarabi A, Zamiri B, Mohammad C, Rahmanian F, Mahmoudi H. Musculoskeletal disorders in dentists in Shiraz, Southern Iran (letter to the editor) Iranian Red Crescent Medical Journal (Ircmj) 2009;11:464–5. [Google Scholar]
- 21.Abdol Samadi H, Yavari Kia A. Symptomatic Carpal Tunnel syndrome frequency among dentists working rather than physicians in Hamadan. Scientific Journal Of Hamadan University of Medical Sciences And Health Services. 2005;12(1):65–70. [Google Scholar]
- 22.Abrisham Kar S, Mosharaf R, Aslani Y, Parvin M, Sadri M. Early cervical degenerative changes among dentists. Majallah-I-Dandanpizishki. 2005;17(1):13–9. [Google Scholar]
- 23.Ahmadi Motemayel F, Abdolsamadi H, Roshanaei G, Jalilian S. Prevalence of Musculoskeletal Disorders among Hamadan General Dental Practitioners. Scientific Journal of Hamadan University of Medical Sciences And Health Services. 2012;19(3):61–6. [Google Scholar]
- 24.Aminian O, Banafsheh Alemohammad Z, Sadeghniiat Haghighi K. Comparative assessment of low back pain and its determinants among Iranian male general dentists and pharmacists. Journal of Dental Medicine-Tehran University of Medical Sciences. 2013;26(2):108–14. [Google Scholar]
- 25.Barakat S, Javan M, Dehghan H, Habibi E. Ergonomic assessment of body posture during work using the Rapid Entire Body Assessment method and prevalence of musculoskeletal disorders in dental students. J Isfahan Dent Sch. 2013;9(5):423–32. [Google Scholar]
- 26.Choobineh A, Soleimani E, Daneshmandi H, Mohamadbeigi A, Izadi K. Prevalence of musculoskeletal disorders and posture analysis using RULA method in Shiraz general dentists in 2010. The Journal of Islamic Dental Association of Iran. 2012;24(4):310–7. [Google Scholar]
- 27.Dehghan MF, Amiri Z, Rabiei M. Prevalence of Musculoskeletal Pain Among A Group of Iranian Dentists, (Tehran-1999) Journal of Dental School Summer. 2003;21(2):185–92. [Google Scholar]
- 28.Eivazi M, Rezaei M, Eteraf Oskuei MA, Zolghadr M, Parand Avar H, Sadeghi N, et al. Prevalence of Musculoskeletal Disorders and Related Risk Factors among Dentists. Medical Journal of Tabriz University. 2012;34:81–7. [Google Scholar]
- 29.Ezoddini Ardakani F, Haerian Ardakani A, Akhavan Karbasi M, Dehghan Tezerjani K. Assessment of musculoskeletal disorders prevalence among dentists. Journal of Dental Medicine. 2005;17:52–60. [Google Scholar]
- 30.Kardani M, Elahi N, Rezaei M. Assessment of Relationship Between Ergonomic Factors And Neck Pain Among Dentist. Jundishapur Scientific Medical Journal. 2007;6:93–9. [Google Scholar]
- 31.Nasl Saraji J, Hosseini M, Shahtaheri S, Golbabaei F, Ghasemkhani M. Evaluation of ergonomic postures of dental professions by Rapid Entire Body Assessment (REBA), in Birjand, Iran. Journal of Dental Medicine. 2005;18(1):61–7. [Google Scholar]
- 32.Pourabbas R, Shakouri K, Haji dizaji R. Prevalence and Risk Factors of Musculoskeletal Disorders among Dentists in Tabriz. Medical Journal of Tabriz University. 2005;26:34–9. [Google Scholar]
- 33.Saheb Jami M, Farahani S. Statistical evaluation of osteoarthritis prevalence in Dentists of Tehran. Journal of Dental Medicine. 1989;3(1):71–7. [Google Scholar]
- 34.Varmazyar S, Amini M, Kiafar M. Ergonomic evaluation of work conditions in Qazvin Dentists by REBA method and its association with musculoskeletal disorders in 2008. Majallah-I-Dandanpizishki. 2008;24:229–37. [Google Scholar]
- 35.Ebrahimian H, Hokmabadi R, Shoja E. Evaluation of Ergonomic Posture of Dental Professions by REBA in North Khorasan, Iran. Journal of North Khorasan University of Medical Sciences. 2013 2013;Student Research committe Issue: p961-7. [Google Scholar]
- 36.Droeze EH, Jonsson H. Evaluation of ergonomic interventions to reduce musculoskeletal disorders of dentists in the Netherlands. Work. 2005;25(3):211–20. [PubMed] [Google Scholar]
- 37.Lake J. Musculoskeletal dysfunction associated with the practice of dentistry - proposed mechanisms and management: literature review. University of Toronto dental journal. 1994;9(1):9–11. [PubMed] [Google Scholar]
- 38.Ylipää V, Arnetz B, Preber H. Factors that affect health and well-being in dental hygienists;a comparison of Swedish dental practices. Journal of dental hygiene: JDH/American Dental Hygienists' Association. 1998;73(4):191–9. [PubMed] [Google Scholar]
- 39.Leggat PA, Kedjarune U, Smith DR. Occupational health problems in modern dentistry: a review. Industrial health. 2007;45(5):611–21. doi: 10.2486/indhealth.45.611. [DOI] [PubMed] [Google Scholar]
- 40.Gupta A, Ankola AV, Hebbal M. Dental ergonomics to combat musculoskeletal disorders: a review. International Journal of Occupational Safety and Ergonomics. 2013;19(4):561–71. doi: 10.1080/10803548.2013.11077005. [DOI] [PubMed] [Google Scholar]
- 41.Baradaran HR, Shams-Hosseini N, Noori-Hekmat S, Tehrani-Banihashemi A, Khamseh ME. Effectiveness of diabetes educational interventions in Iran: A systematic review. Diabetes technology and therapeutics. 2010;12(4):317–31. doi: 10.1089/dia.2009.0118. [DOI] [PubMed] [Google Scholar]