

Abstract
Introduction:
The burden of stroke has been increasing worldwide, especially in developing countries. Very few data regarding epidemiology of stroke are available in Bosnia and Herzegovina (BH).
Patients and methods:
We undertook a retrospective hospital-based study in all hospitals existing in five cantons and one district of BH. The patients were recruited between January 1st, 2014, and December 31st, 2014, and only first-ever-in-lifetime strokes (FES) were included for evaluation.
Results:
A FES was diagnosed in 1479 patients (age 71.83 ± 11.703 years) during the study period. FES occurred in 709 men (47.9%; age 69.64 ±12.002 years) and 770 women (52.1%; age 73.85± 11.051 years). Stroke was categorized into ischemic stroke (IS), primary intracerebral hemorrhage (PICH), subarachnoid hemorrhage (SAH) and cerebral venous thrombosis (CVT), which was diagnosed in 84%, 12,2%, 3,4% and 0,4% cases respectively. Early 28-day case-fatality was 18.5 % for all patients and both sexes combined. Short-term case-fatality was significantly greater in women (P=0.007). Among all patients with FES, 87% had hypertension, 35% diabetes mellitus, 39% hypercholesterolemia and almost 25 % atrial fibrillation.
Discussion:
This is the first study that provides us with information on epidemiology of stroke in BH. More than 90% of patients had one or more modifiable risk factors and the number would be even higher if we included smoking. The early stroke case-fatality was lower than that observed in other low- to middle-income countries.
Conclusion:
All modifiable stroke risk factors, especially high blood pressure, should be understood as a major public health problem in BH and efforts should be focused on the primary prevention of stroke. Our emphasis is on the designing of a stroke register in BH for a better health planning.
Keywords: Bosnia and Herzegovina, stroke, case-fatality, epidemiology, hospital-based
1. INTRODUCTION
Stroke affects 33 million individuals worldwide every year and two-thirds of all strokes occur in developing countries (1, 2). The burden of stroke has been increasing worldwide, especially in developing countries (3, 4). Very few data regarding epidemiology of stroke are available in Bosnia and Herzegovina (BH), mainly because it is one of the rare countries in Europe that does not have official Stroke register (5-7). In order to describe stroke subtypes, risk factors and case fatality in BH, we preformed a retrospective hospital-based study in five cantons and in one district in BH.
2. SUBJECTS AND METHOD
We studied retrospectively stroke patients hospitalized between January 1st, 2014, and December 31st, 2014, in all hospitals existing in the study area. We used World Health Organization (WHO) definition of stroke: “rapidly developing clinical signs of focal (or global) disturbance of cerebral function, with symptoms lasting 24 hours or longer or leading to death, with no apparent cause other than of vascular origin”. We categorized, based on clinical and cerebral imaging, stroke subtype as ischemic stroke (IS), primary intracerebral hemorrhage (PICH), subarachnoid hemorrhage (SAH) and cerebral venous thrombosis (CVT). Transient ischemic attacks were excluded. Stroke risk factors were identified, including hypertension, blood pressure (BP) ≥160/90 mmHg (or any treatment for high BP); diabetes mellitus, fasting glucose level 7 mmol/L or plasma glucose 11 mmol/L at any time of day (or if treated with insulin or with oral hypoglycemic agents); hypercholesterolemia, total cholesterol level ≥ 5.6 mmol/L; atrial fibrillation (ECG or Holter recordings). The stroke was considered non-fatal if the patient was alive 28 days after stroke onset. All data were extracted from the hospital patient’s records.
3. STUDY AREA
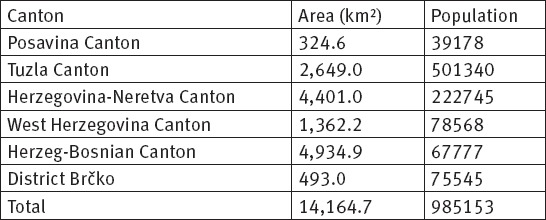
Bosnia and Herzegovina is a country in Southeastern Europe, located on the Balkan peninsula. According to the World Bank, it was an upper middle-income country with Gross Domestic Product (GDP) of 7123 convertible marks (U.S. dollars 3958) in 2014. Life expectancy of population is 73.33 years for males and 79.55 for females (8). The entity of the FBH is divided into ten cantons and all of these cantons have their own cantonal governments, which is under the law of the Federation as a whole (9). This study was conducted in five cantons and in one district, which are presented in Table 1. We detected all hospitals existing in the study area: County Hospital Orašje in Orašje (Posavina Canton); General Hospital „Dr. Mustafa Beganović” in Gračanica and University Clinical Center Tuzla in Tuzla (Tuzla Canton); County Hospital „Dr. Safet Mujić” in Mostar, General Hospital Konjic in Konjic and University Clinical Hospital Mostar in Mostar (Herzegovina-Neretva Canton); County Hospital „Fra Mihovila Sučića” in Livno (Herzeg-Bosnian Canton); General Hospital Brčko in Brčko (District Brčko).
Table 1.
Geographical Area of the Study and its Population
Statistical Analysis
SPSS software for Windows (version 20, SPSS Inc., Chicago, IL, USA) was used for the statistical analysis of the data. Chi-square test was used for the comparison between categorical variables. P < 0.050 was considered statistically significant.
4. RESULTS
Between January 1st, 2014, and December 31st, 2014, 1938 patients with stroke were hospitalized. Mean age was 72.20 (± 11.164 SD) years. Among all identified cases, 930 (48.0 %) occurred in males and 1008 (52.0%) in females. Among all hospitalized patients, 459 (23.7%) had a recurrent stroke. A FES was diagnosed in 1479 (76.3 %) patients (age 71.83 ± 11.703 years; range 19 to 97 years). FES occurred in 709 men (47.9 %; age 69.64 ±12.002 years) and 770 women (52.1%; age 73.85± 11.051 years). In FES, brain imaging was performed in 100% of patients and stroke was categorized into IS, PICH, SAH and CVT, which was diagnosed in 84%, 12.2%, 3.4% and 0.4% cases respectively. CVT were excluded from further analysis. Mean age for IS was 72,7 years; for PICH 70.,2 years and for SAH 58.2. Ischemic patients were significantly older than hemorrhagic ones (P=0.007). Median length of hospital stay for FES was 10.4 days (range 1 to 70 days). Risk factors are summarized in Table 2. Hypertension was the main risk factor, occurring in almost 87 % of patients. Early 28-day case-fatality was 18.5% for all patients and for both sexes combined. Intracerebral hemorrhage at 36% had the overall highest fatality rate (P<0.001) (Table 3). Short-term case-fatality is significantly greater in women (P=0.007).
Table 2.
Risk Factors for Ischemic and Hemorrhagic Stroke IS indicates ischemic stroke; PICH primary intracerebral hemorrhage; SAH, subarachnoid hemorrhage
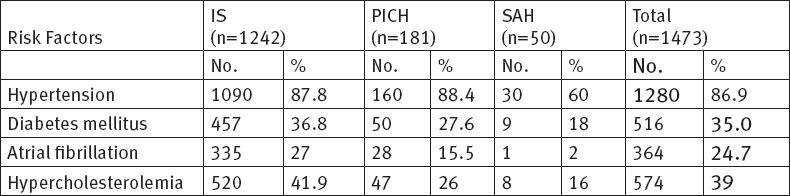
Table 3.
Early (28-day) Fatal Stroke Outcomes of Patients with First-Ever Stroke, Stratified by Pathological Subtype. PICH indicates primary intracerebral hemorrhage; SAH, subarachnoid hemorrhage

5. DISCUSSION
We preformed a retrospective hospital-based study in order to describe stroke subtypes, risk factors and 28-day case fatality of stroke in different cantons of BH. The frequencies of IS, PICH and SAH in our study of 84%, 12.2% and 3.4%, respectively, are similar to those reported by EROS investigators (10).
The median age for FES was 72 years, which is only one year older than in other European countries and conflicts with the finding that average age of FEV incidence is 6 years younger in LMIC than in HIC (10,11, 22). In BH, like in most studies, women got their first stroke on an average 4,2 years later than man (13).
Among all patients with FEV, 87% had hypertension, 35% diabetes mellitus, 39% hypercholesterolemia and almost 25% AF. Only 7 % patients did not have any modifiable risk factors and 65% had two or more. Our data clearly showed a high prevalence of these risk factors. That can be explained by assuming that large segment of BH population still lives in poverty and low socioeconomic status is associated with higher prevalence of vascular risk factors (14). Since most of these risk factors are preventable, our emphasis would be on better stroke prevention strategies.
The early stroke case-fatality (18.5%) is lower than that observed in other low- to middle-income countries (11, 12), but still higher than the goal set for 2015 (15%) in the Helsingborg Declaration 2006 (15). We found no differences in early case-fatality between hospitals and since early case fatality is an indicator of hospital performance, we can say that quality of care is the same in all hospitals (16). Our data show significant sex differences, with higher 28-day case fatality in women than in men. Previous studies have reported conflicting findings with evidence of no sex differences (17, 18) or increased risk in women (5,13, 19). Sex differences are still poorly understood, but it is likely that higher case fatality in women is connected with greater stroke severity in women, which is a strong predictor of short term outcome (17).
Considering that the study was retrospective, data were extracted from medical records and therefore there was a lack of data concerning etiology for ischemic strokes, history of smoking and other risk factors.
6. CONCLUSION
In conclusion, high burden of stroke in BH is related with a high rate of modifiable risk factors. More than 90% of patients had one or more modifiable risk factors and the number would be even higher if we included smoking. All modifiable stroke risk factors, especially high blood pressure, should be understood as a major public health problem in BH and efforts should be focused on the primary prevention of stroke. Our emphasis is on the designing of a stroke register in BH for a better health planning.
Footnotes
• Author Contributions: Bender Marija designed the draft of the study, participated in data collection and writing. Jusufovic Edin, Railic Vesna, Kelava Sima, Tinjak Selma, Dzevdetbegovic Damir, Mott Dario, Tresnjo Mensuda, Lakicevic Sandra and Pejanovic-Skobic Natasa participated in data collection. Sinanovic Osman designed the draft of the study.
• Conflict of interests: the authors declare no conflict of interest in this study.
REFERENCES
- 1.Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Executive summary: heart disease and stroke statistics –2015 update: a report from the American Heart Association. Circulation. 2015;131:434–41. doi: 10.1161/CIR.0000000000000152. [DOI] [PubMed] [Google Scholar]
- 2.Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health. 2013;1:259–81. doi: 10.1016/S2214-109X(13)70089-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Feigin VL, Lawes CMM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–69. doi: 10.1016/S1474-4422(09)70025-0. [DOI] [PubMed] [Google Scholar]
- 4.Hyon L, You-Seon N, Kyoung-Min L. Development-assistance Strategies for Stroke in Low- and Middle-income Countries. J Korean Med Sci. 2015;30:139–42. doi: 10.3346/jkms.2015.30.S2.S139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Salihović D, Smajlović D, Sinanović O, Kojić B. Sex differences in patients with acute ischemic stroke in Tuzla region, Bosnia and Herzegovina. Bosn J Basic Med Sci. 2010;10:116–20. doi: 10.17305/bjbms.2010.2705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vasilj I, Cavaljuga S, Lucić T, Kvesić F. Cerebrovascular insult hospital cases in West Herzegovina Canton from 1998 to 2002. Bosn J Basic Med Sci. 2005;5:49–52. doi: 10.17305/bjbms.2005.3285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Suljic E, Mehicevic A, Gavranovic A. Stroke emergency medical care: initial assessment, risk factors, triage and hospitalization outcome. Mater Sociomed. 2013;25:83–7. doi: 10.5455/msm.2013.25.83-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.The World Factbook-CIA. [(access date:15.01.2016)]. URL: https://www.cia.gov/library/publications/the-world-factbook .
- 9.Constitution of Bosnia and Herzegovina. [(access date:15.01.2016)]. URL: http://www.ccbh.ba/public/down/USTAV_BOSNE_I_HERCEGOVINE_bos.pdf .
- 10.European Registers of stroke (EROS) Investigators. Incidence of stroke in Europe at beginning of the 21st century. Stroke. 2009;40:1557–63. doi: 10.1161/STROKEAHA.108.535088. [DOI] [PubMed] [Google Scholar]
- 11.Kulesh SD, Filina NA, Frantava NM, Zhytko NL, Kastsinevich TM, Kliatskova LA, et al. Incidence and Case-Fatality of Stroke on the East Border of the European Union The Grodno Stroke Study. Stroke. 2010;41:2726–30. doi: 10.1161/STROKEAHA.110.596916. [DOI] [PubMed] [Google Scholar]
- 12.Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–128. doi: 10.1016/S0140-6736(12)61728-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Appelros P, Stegmayr B, Terent A. Sex differences in stroke epidemiology: a systematic review. Stroke. 2009;40:1082–90. doi: 10.1161/STROKEAHA.108.540781. [DOI] [PubMed] [Google Scholar]
- 14.Kelleher CC, Friel S, Nic Gabhainn S, Tay JB. Socio-demographic predictors of self-rated health in the Republic of Ireland: Findings from the National Survey on Lifestyle, Attitudes and Nutrition, SLAN. Soc Sci Med. 2003;57:477–86. doi: 10.1016/s0277-9536(02)00371-4. [DOI] [PubMed] [Google Scholar]
- 15.Kjellstrom T, Norrving B, Shatchkute A. Helsingborg Declaration 2006 on European stroke strategies. Cerebrovasc Dis. 2007;23:231–41. doi: 10.1159/000097646. [DOI] [PubMed] [Google Scholar]
- 16.AHRQ quality indicators - guide to inpatient quality indicators: quality of care in hospitals - volume, mortality, and utilization. AHRQ Quality Indicators. Rockville, MD: AHRQ; 2004. pp. 1–95. [Google Scholar]
- 17.Saposnik G, Hill MD, O'Donnell M, Fang J, Hachinski V, Kapral MK. Variables associated with 7-day, 30-day, and 1-year fatality after ischemic stroke. Stroke. 2008;39:2318–24. doi: 10.1161/STROKEAHA.107.510362. [DOI] [PubMed] [Google Scholar]
- 18.Andersen KK, Jovanovic Andersen Z, Skyhø J, Olsen T. Predictors of Early and Late Case-Fatality in a Nationwide Danish Study of 26 818 Patients With First-Ever Ischemic Stroke. Stroke. 2011;42:2806–12. doi: 10.1161/STROKEAHA.111.619049. [DOI] [PubMed] [Google Scholar]
- 19.Lewsey JD, Gillies M, Jhund PS, Chalmers JWT, Redpath A, Briggs A, et al. Sex Differences in Incidence, Mortality, and Survival in Individuals With Stroke in Scotland, 1986 to 2005. Stroke. 2009;40:1038–43. doi: 10.1161/STROKEAHA.108.542787. [DOI] [PubMed] [Google Scholar]