

Abstract
In this study we analyzed patients glucose levels taken before and after coronary artery bypass surgery. The data are taken from University of Sarajevo Clinics Centre-medical documentation of Heart Center from January 1st, 2007 to October 31st, 2007. Therefore, the entire study is done retrospectively. The patients considered in this analysis were divided into three groups. The patients in the first group were treated with peroral antidiabetics. The second group included patients treated with insulin while the third group consisted of patients without diabetes and acted as control group. All the patients had increased BMI. In the first two groups glucose levels were elevated before the surgery. Data analysis showed that three patients from the first group changed from peroral antidiabetics to insulin during postoperative period, and they were dismissed from hospital with this therapy. In the control group, peroral antidiabetis were introduced in four patients. The study results show that all the three groups have had high glycaemia on the first postoperative day. This may be caused by a number of reasons: inadequate pre-operative antidiabetic therapy, the impact of stress during surgery, inadequate pre-operative treatment of glycaemia or avoidance of the proscribed therapy by patients themselves. Stress during operation and administration of several medications after operation may also cause increased insulin resistance and distort glycaemia control.
Keywords: diabetes, coronary artery bypass grafting
INTRODUCTION
Diabetes mellitus is one of the main risk factors for cardiovascular disease (1). Patients with diabetes have increased risk of coronary artery disease. When these patients are affected coronary artery disease, they frequently require coronary artery bypass grafting surgery. It is estimated that between 20%-30% of all patients who had CABG also have diabetes. Research in Canada showed that more than 16% of all patients with CABG have diabetes (1). Diabetes or increased levels of blood sugar before and after surgery influence the outcome of surgical intervention. Increased blood sugar level is present predictive factor for deep sternal wound infection (2), long postoperative recovery, stroke or cardiac status (3). The aim of this paper is to examine the levels of blood sugar before and after surgical intervention in the patients with CABG surgery.
MATERIALS AND METHODS
The data used in this study are taken from University of Sarajevo Clinics Centre - medical documentation of Heart Center from January 1st, 2007 to October 31st, 2007. Therefore, the entire study is done retrospectively. The patients considered in this analysis were divided into three groups. The first group consisted of patients treated with peroral antidiabetics (n=41). The second group included patients treated with insulin (n=29), while the third group consisted of patients without diabetes and served as a control group (n=70). Patients who had valve replacement along CABG and patients whose diabetes was treated with diet were excluded from the study. We used clinical and laboratory parameters: sex, age, body mass index, blood sugar levels measured before the operation and on the first, second, third and sixth day postoperative. The data were analyzed using standard methods of descriptive statistics. Arcus Quick Stat program was used for data analysis (4).
RESULTS
Demographic characteristics of subjects are outlined in Table 1.
TABLE 1.
Demographic characteristics of patients

The first group included 41 patients: 26 males and 15 females. This group had average body mass index of 28,5±3,7. The second group included 29 patients: 18 males and 11 females with average BMI 28,51±4,30. The control group included 70 patients: 51 males and 19 females with average BMI 27,4±2,7. On average, patients in both test groups were older than the control group subjects (61,3±9,7 against 60,41±7,95). All patients had increased body mass index. Glycaemia levels before and after surgery are shown in Table 2.
TABLE 2.
Glycaemia levels before and after surgery
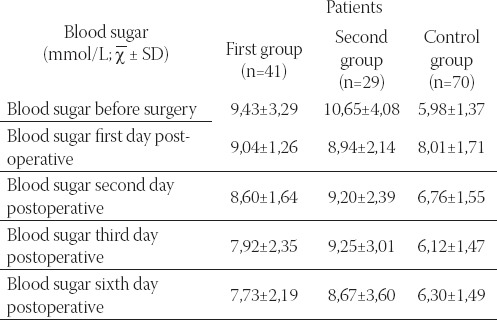
The Table 2. indicates that values of glycaemia were increased in the two first groups. During postoperative treatment these values were reduced in comparison with preoperative values. However, postoperative values were still outside the normal range of 3,3-6,5 μmol/l. In the control group glycaemia levels were within normal range before the operation (5,98±1,37). During the first day after operation these values increased to 8,01±1,71 and then fell within normal range six days after the surgery 6,30±1,49.
The values can also be shown graphically:
FIGURE 1.

Glycaemia values before and after operation
Outcome of the coronary artery bypass surgery is shown in the Table 3.
TABLE 3.
Outcome of the coronary artery bypass surgery

The data analysis showed that three patients (7,32%) in the first group changed from peroral antidiabetics to insulin during postoperative period, and were dismissed from hospital with this therapy. In the case of four patients from the control group peroral antidiabetics were introduced.
DISCUSSION
Nowadays, diabetes mellitus is one the main risk factors for cardiovascular disease. Successful diabetes control is very important for the patients in the need of CABG. Hyperglycaemia is in correlation with many side effects which in turn affect the heart. Effects of acute hyperglycaemia on vascular endothelium may cause poor surgical result (9). This retrospective study shows postoperative blood sugar levels in patients who had CABG. Three groups of patients were considered. The first group included patients who had diabetes before surgical intervention and were treated with peroral antidiabetic. The second group included patients already taking insulin, while the third group consisted of patients without diabetes and served as the control. The results show that all three groups had increased values of blood sugar on the first postoperative day. The importance of glycaemia control on the first postoperative day was also analyzed in previous studies. Mc Alister et al. (5) proved that it is very important to decrease the levels of glycaemia on the first postoperative day. This is due to the fact that during this day, the values of glycaemia increase by 1 μmol/l which in turn relates to17% greater risk of unwanted side effects. Hyperglycaemia can lead to dehydration, electrolyte disbalance and arrhythmia. It is considered that these complications occur when glycaemia values exceed 11 μmol/l (6). Certain studies indicate that continuous insulin infusion following CABG exerts better control of glycaemia than insulin injections (7, 8). Patients with better glycaemia control stay shorter period of time in intensive care unit, they do not develop sternal wound infections and thus, the cost of treatment is lower. Study shows that the patients from the first group, who receive peroral therapy, need insulin after surgical intervention to treat diabetes. Stress during operation and administration of several medications after operation may also cause increased insulin resistance and distort glycaemia control.
CONCLUSION
Preoperative diabetes is very important for outcome of surgical intervention. It is necessary that all patients with diabetes go through special preoperative protocol with diabetologists and bring glycaemia levels within normal. In order to improve this research a greater number of patients should be taken into consideration.
REFERENCES
- 1.Ghali W.A, Quan H, Brant R. Coronary artery bypass grafting in Canada: national and provincial mortality trends 1992-1995. Can Med Assoc J. 1998;159:25–31. [PMC free article] [PubMed] [Google Scholar]
- 2.Carson J, Schloz P, Chen A, et al. Diabetes mellitus increases Short-term mortality and Morbidity in patients undergoing coronary artery bypass graft surgery. JACC. 2002;40:418–423. doi: 10.1016/s0735-1097(02)01969-1. [DOI] [PubMed] [Google Scholar]
- 3.Lauruschkat A.H, Arnrich B, Albert A.A, Walter J.A, et al. Prevalence and risks of undiagnosed diabetes mellitus in patients undergoing coronary artery bypass grafting. Circulation. 2005;18(112(16)):2397–2402. doi: 10.1161/CIRCULATIONAHA.105.534545. [DOI] [PubMed] [Google Scholar]
- 4.Buchan I.E. Arcus QuickStat Biomedical version. 1st ed. Cambridge: Adisson Wesley Longman Ltd; 1997. [Google Scholar]
- 5.McAlister F, Amad H, Man J, Tandon P. Bistritz. Diabetes and coronary artery bypass surgery. Diabetes care. 2003;26:1518–1524. doi: 10.2337/diacare.26.5.1518. [DOI] [PubMed] [Google Scholar]
- 6.McMahon M.M, Bistrian B.R. Host defenses and susceptibility to infection in patients with diabetes mellitus. Infect. Dis. Clin. North. Am. 1995;9:1–9. [PubMed] [Google Scholar]
- 7.Furnary A.P, Zerr K.J, Grunkemeier G.L, Starr A. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann. Thorac. Surg. 1999;67(2):352–360. doi: 10.1016/s0003-4975(99)00014-4. [DOI] [PubMed] [Google Scholar]
- 8.Li J.Y, Sun S, Wu S.J. Continuous insulin infusion improves postoperative glucose control in patients with diabetes mellitus undergoing coronary artery bypass surgery. Tex. Heart Inst. J. 2006;33(4):445–451. [PMC free article] [PubMed] [Google Scholar]
- 9.Menaka R, Sabeer T.K, Naveen A, Joshi R.R, Bhattacharya A. Glycemic control after coronary artery bypass grafting: Closure of the audit loop. Int. J. Diab. Dev. Ctrie. 2007;27:69–72. [Google Scholar]