

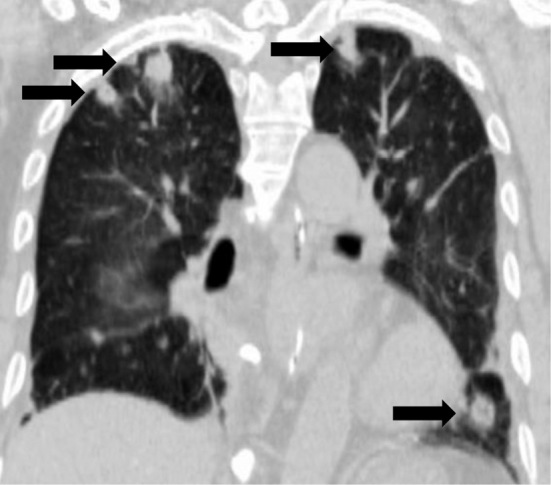
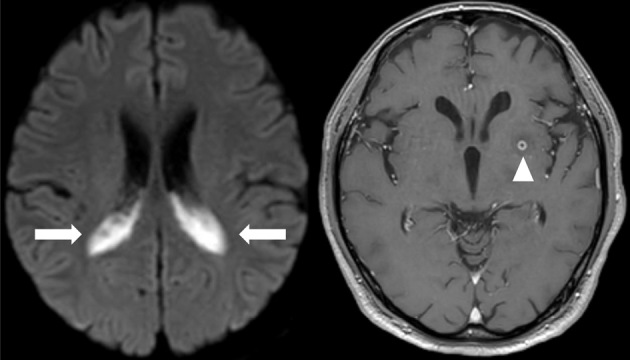
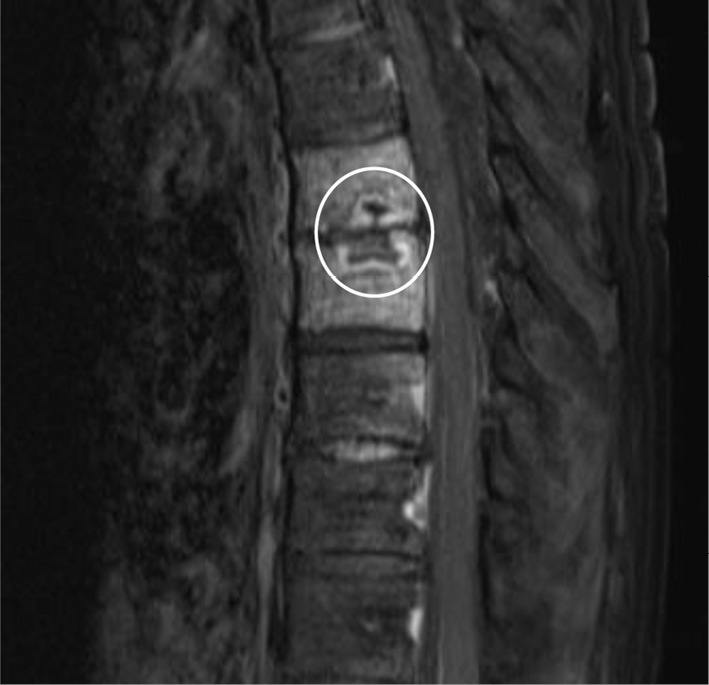
A 68-year-old man with a rapidly progressing loss of consciousness and neck stiffness was transferred to our hospital. He had no remarkable history except for an elevated HbA1c level of 6.9%. Computed tomography (CT) revealed a 55-mm low-density area in segment 4 of the liver (Picture 1) and multiple lung nodules (Picture 2; black arrows). Magnetic resonance imaging revealed abscess formation in the lateral ventricles (Picture 3; white arrows) and an 8-mm brain abscess (Picture 3; white arrowhead). We diagnosed him with invasive liver abscess syndrome accompanied by meningitis, brain abscess, and septic pulmonary embolism and performed percutaneous liver abscess drainage and administered meropenem. Klebsiella pneumoniae was detected in the cultures of the liver abscess, blood, and cerebrospinal fluid specimens, so meropenem was replaced with ceftoriaxone. Three months later, CT revealed intervertebral discitis (Picture 4; white circle), so ceftoriaxone was replaced with levofloxacin. While K. pneumoniae is common, a new hypervirulent K. pneumoniae variant associated with a high mortality rate is emerging as a global disease (1,2). The present patient was discharged 168 days after admission without severe sequelae.
Picture 1.

Picture 2.
Picture 3.
Picture 4.
Author's disclosure of potential Conflicts of Interest (COI).
Shuji Terai: Honoraria, Otsuka Pharmacy.
References
- 1. Siu LK, Yeh KM, Lin JC, Fung CP, Chang FY. Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis 12: 881-887, 2012. [DOI] [PubMed] [Google Scholar]
- 2. Qian Y, Wong CC, Lai SC, et al. Klebsiella pneumoniae invasive liver abscess syndrome with purulent meningitis and septic shock: A case from mainland China. World J Gastroenterol 22: 2861-2866, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]