

Abstract
The cyclin D–cyclin-dependent kinase (CDK) 4/6–p16–retinoblastoma (Rb) pathway is commonly disrupted in cancer, leading to abnormal cell proliferation. Therapeutics targeting this pathway have demonstrated antitumor effects in preclinical and clinical studies. Ribociclib is a selective, orally bioavailable inhibitor of CDK4 and CDK6, which was granted priority review by the US Food and Drug Administration in November 2016, and is set to enter the treatment landscape alongside other CDK4/6 inhibitors, including palbociclib and abemaciclib. Here we describe the mechanism of action of ribociclib, and review preclinical and clinical data from Phase I, II, and III trials of ribociclib across different tumor types, within the context of other selective CDK4/6 inhibitors. The pharmacokinetics, pharmacodynamics, safety, tolerability, and clinical responses with ribociclib as a single agent or in combination with other therapies are discussed, and an overview of the broad portfolio of ongoing clinical trials with ribociclib across a wide range of indications is presented. Based on the available data, ribociclib has a manageable tolerability profile and therapeutic potential for a variety of cancer types. Its high selectivity makes it an important partner drug for other targeted therapies and it has been shown to enhance the clinical activity of existing anticancer therapies and delay the development of treatment resistance, without markedly increasing toxicity. Ongoing trials of doublet and triplet targeted therapies containing ribociclib seek to identify optimal CDK4/6-based targeted combination regimens for various tumor types and advance the field of precision therapeutics in oncology.
Keywords: ribociclib, LEE011, CDK4/6 inhibitor, cyclin D–CDK4/6–p16–Rb pathway, cancer
Introduction
Cancer development is often characterized by abnormal cellular proliferation and dysregulation of cell cycle control (1). The cell cycle is regulated at different stages by various cyclin–cyclin-dependent kinase (CDK) complexes (Figure 1). The G1 (pre-DNA synthesis) to S (DNA synthesis) cell cycle checkpoint is regulated by the cyclin D–CDK4/6–p16–retinoblastoma (Rb) pathway, which ensures conditions are appropriate for cell growth and division before the cell is irreversibly committed to division (2–4). In this pathway, cyclin D is the key entry point at which various mitogenic and growth arrest signaling pathways converge to regulate the cell cycle (3). In response to mitogenic signaling, levels of D-type cyclins rise and associate with CDK4 or CDK6. The resulting active cyclin D–CDK4/6 complexes phosphorylate Rb, relieving its repression of E2 transcription factors (E2F). The released E2F consequently activates the transcription of genes required for the G1–S transition and cell cycle progression (5, 6). The tumor suppressor and negative regulator of the cyclin D–CDK4/6 complex, p16, is a critical mediator of cellular senescence, limiting the replicative life span of cells (7).
Figure 1.
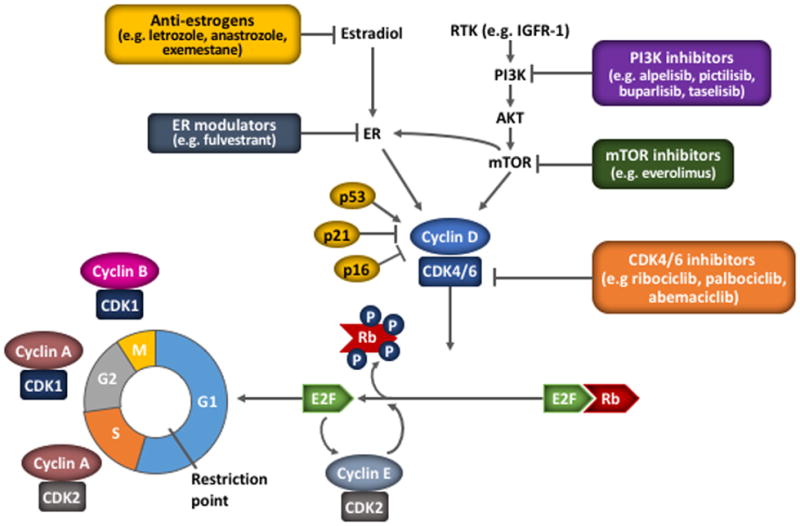
The role of cyclin–CDK complexes and the cyclin D–CDK4/6–p16–Rb pathway in the cell cycle
The cell cycle is regulated by cyclins and checkpoints, with different cyclins (and cyclin–CDK combinations) and checkpoints acting at phase transition of the cell cycle. At the G1–S cell cycle checkpoint, mutiple mitogenic pathways including ER and PI3K/AKT/mTOR promote the synthesis of cyclin D, which associates with and activates CDK4/6. Activated CDK4/6 phosphorylates the Rb protein to disrupt its sequestering interaction with E2F, releasing its transcription effect and allowing the expression of genes necessary for cell cycle progression, including cyclin E. Cyclin E associates with CDK2, which further phosphorylates Rb, resulting in progression of the cell cycle past the restriction point and irreversible S phase entry. Additional cyclin–CDK complexes act at further cell cycle checkpoints; cyclin A–CDK2 enables the S–G2 transition, and cyclin A–CDK1 and cyclin B–CDK1 facilitate the onset and progression of mitosis, respectively (82). Selective inhibitors of CDK4/6, such as ribociclib, act directly on the cyclin D–CDK4/6–p16–Rb pathway to block cell cycle progression. The pathway may also be impacted by inhibitors of other pathways acting upstream of CDK4/6, providing a rationale for dual inhibition.
CDK, cyclin-dependent kinase; ER, estrogen receptor; HER2, human epidermal growth factor receptor-2; IGF1R, insulin-like growth factor 1 receptor; MAPK, mitogen-activated protein kinase; RTK, receptor tyrosine kinase.
In cancer, the cyclin D–CDK4/6–p16–Rb pathway is commonly disrupted in favor of cell cycle progression and continued growth, rendering this pathway a key target for cancer therapeutics (5, 8). In hormone receptor-positive (HR+) breast cancer, CDK4/6 pathway activation has also been associated with resistance to endocrine therapy (9, 10). p16 is frequently inactivated by gene deletion, point mutation, or transcriptional silencing by methylation (5). Amplification of CDK4 and CCND1 (encoding cyclin D1) and overexpression of cyclin D protein (e.g. through chromosome 11 translocations or inversions) are also frequent in human cancers (5, 11). The abnormalities of the cyclin D–CDK4/6–p16–Rb pathway vary across cancer types (Supplementary Table 1). The pathway can also be upregulated as a result of upstream oncogenic mutations (3, 12, 13). This provides a therapeutic potential for targeting CDK4 and CDK6 in the treatment of cancer.
Advent of CDK4/6 inhibitors
Preclinical evidence showing a role for the cyclin D–CDK4/6–p16–Rb pathway in cancer led to the development of a first generation of broad-acting pan-CDK inhibitors (14). The first such inhibitor to enter clinical trials was flavopiridol; however, clinical studies demonstrated poor efficacy, complex pharmacokinetics (PK), and dose-limiting toxicities due to off-target effects (14, 15). The late 1990s/early 2000s saw the development of second-generation CDK inhibitors. These inhibitors showed preferential inhibition of CDK1 and CDK2 and/or increasing overall potency. Of these, dinaciclib, an inhibitor of CDK1, CDK2, CDK5, and CDK9, was most extensively studied in the clinic; however, Phase II trials showed limited efficacy (14, 16, 17).
More recently, inhibitors specific for CDK4 and CDK6 have entered clinical trials. Such selective inhibitors spare CDK2 activity, avoiding inhibition of general S-phase activity. Three selective CDK4/6 inhibitors are in late-stage clinical development: ribociclib (LEE011, Novartis), palbociclib (Ibrance®; PD-0332991; Pfizer), and abemaciclib (LY-2835219; Eli Lilly). Palbociclib combined with letrozole or fulvestrant has demonstrated efficacy in patients with HR+ advanced breast cancer (ABC; Table 1) (18, 19), and is approved in the USA and Europe for use in these combinations (20, 21). Abemaciclib has shown efficacy as a single agent and in combination with endocrine therapies in patients with HR+ ABC, and has entered Phase III development, with an US Food and Drug Administration (FDA) Breakthrough Therapy Designation granted in 2015 for patients with refractory HR+ ABC (Table 1) (22–24).
Table 1.
Key reported clinical trials with palbociclib and abemaciclib.
| Study name/ID | Combination drug | Phase | Population | Common Grade 3/4 AEs (≥10% of patients) | Clinical activity |
|---|---|---|---|---|---|
| Palbociclib | |||||
| Breast Cancer | |||||
| PALOMA-1/NCT00721409 (74) | Letrozole | II | ER+ ABC with no prior treatment for ABC (N=165) | Neutropenia (54%), leukopenia (19%) | Median PFS 20.2 months vs 5.7 months for letrozole monotherapy (HR=0.488; P=0.0004) |
| PALOMA-2/NCT01740427 (18) | Letrozole | III | ER+ ABC with no prior treatment for ABC (N=666) | Neutropenia (66%), leukopenia (25%) | Median PFS 24.8 months vs 14.5 months for letrozole monotherapy (HR=0.58; P<0.000001) |
| PALOMA-3/NCT01942135 (19) | Fulvestrant | III | HR+ ABC after progression on one line of endocrine therapy for ABC (N=521) | Neutropenia (62%), leukopenia (25%) | Median PFS 9.2 months vs 3.8 months for fulvestrant monotherapy (HR=0.42; P<0.001) |
| NCT01037790 (75) | None | II | Metastatic Rb+ breast cancer (N=37; n=33 HR+) | Neutropenia (54%), leukopenia (51%), lymphopenia (30%), thrombocytopenia (19%) |
Total (N=37): 5% PR, 38% SD <6months, 14% SD ≥6 months, CBR 19% HR+ (n=33): 6% PR, 39% SD <6 months, 16% SD ≥6 months, CBR: 21% |
| Solid tumors | |||||
| NCT00141297 (71) | None | I | Rb+ advanced solid tumors (N=41) | Neutropenia (20%), leukopenia (10%) in Cycle 1 | 27% SD for ≥4 cycles, 16% SD for ≥10 cycles (n=37 evaluable) |
| MCL | |||||
| NCT00420056 (76) | None | Ib | CD19+/CD20+, CD5+, CD23− MCL, with cyclin D1 positivity, t(11;14) translocation, or bcl-1/IgH rearrangement (N=17) | Neutropenia (35%), thrombocytopenia (24%), hypophosphatemia (12%) | 6% CR, 12% PR, 41% SD, median PFS 4 months (90% CI 2.0–14.7 months) (n=16 evaluable) |
| Liposarcoma | |||||
| NCT01209598 (77) | None | II | Advanced CDK4− amplified, Rb+ well-differentiated or dedifferentiated liposarcoma (N=30) | Neutropenia (50%), leukopenia (47%), thrombocytopenia (30%), lymphopenia (27%), anemia (17%) | 3% PR, 12-week PFS 66% (90% CI 51–100%), median PFS 18 weeks (n=29 evaluable) |
| NSCLC | |||||
| NCT01291017 (78) | None | II | Previously treated, advanced Rb+, CDKN2A inactivated NSCLC (N=19) | Neutropenia (16%) | 50% SD, median PFS 12.5 weeks |
| Abemaciclib | |||||
| Solid tumors | |||||
| NCT01394016 (79) | None | I | Advanced solid tumors (whole study N=225; escalation phase n=33) | Leukopenia (10%), neutropenia (10%) (n=173) |
Breast cancer (n=47): 23% PR, 47% SD, 23% ORR, 49% CBR, 70% DCR, median PFS 5.8 months NSCLC (n=68): 3% PR, 46% SD, 3% ORR, 49% DCR, median PFS 2 months Melanoma (n=26): 4% PR, 23% SD, 4% ORR, 27% DCR Glioblastoma (n=17): 0% PR, 18% SD, 0% ORR, 18% DCR CRC (n=15): 0% PR, 13% SD, 0% ORR, 13% DCR |
| NCT02014129 (80) | None | I | Japanese patients with advanced cancer (N=12) | 200 mg BID (n=6): leukopenia (33%), neutropenia (17%) | Maximal percent change in tumor size from baseline: −35 to +25% >30% tumor shrinkage in 2 patients (HR−, HER2+ breast cancer and small intestine neuroendocrine carcinoma) |
| Breast cancer | |||||
| MONARCH-1/NCT02102490 (22) | None | II | HR+, HER2− ABC that has progressed on prior endocrine therapy and chemotherapy (N=132) | Diarrhea (20%) and fatigue (13%), white blood cell decreased (28%), neutrophil count decrease (22%) | Confirmed PR 20%, confirmed ORR 20%, CBR 42%, median PFS 6 months |
| NCT02057133 (81) | Endocrine and HER2-targeted therapies | Ib | HR+ metastatic breast cancer (N=110) |
Combination with letrozole (n=20): diarrhea (45%), fatigue (20%), neutropenia (20%), nausea (15%), vomiting (10%) Combination with anastrozole (n=16): diarrhea (31%), leukocyte count reduced (31%), neutrophil count reduced (25%), lymphocyte count reduced (25%), fatigue (19%) Combination with tamoxifen (n=16): diarrhea (31%), fatigue (31%), lymphocyte count reduced (13%), leukocyte count reduced (13%) Combination with exemestane (n=15): diarrhea (27%), abdominal pain (20%), neutrophil count reduced (20%), lymphocyte count reduced (20%), fatigue (13%) Combination with exemestane + everolimus (150 mg BID dose; n=15): neutrophil count reduced (33%), leukocyte count reduced (33%), lymphocyte count reduced (33%), diarrhea (27%), anemia (20%), fatigue (13%), stomatitis (13%), hypokalemia (13%) Combination with exemestane + everolimus (200 mg BID dose; n=4): neutrophil count reduced (75%), diarrhea (25%), leukocyte count reduced (25%), platelet count reduced (25%) Combination with trastuzumab (150 mg BID dose; n=18): diarrhea (17%), fatigue (11%), hypokalemia (11%), lymphocyte count reduced (11%) Combination with trastuzumab (200 mg BID dose; n=6): diarrhea (83%), anemia (33%), neutrophil count reduced (33%), leukocyte count reduced (33%), lymphocyte count reduced (33%), platelet count reduced (17%), fatigue (17%), abdominal pain (17%) |
Combination with letrozole (n=20): 6-month PFS 76% Combination with anastrozole (n=16): 6-month PFS 87% Combination with tamoxifen (n=16): 6-month PFS 73% Combination with exemestane (n=15): 6-month PFS 75% Combination with exemestane + everolimus (150 mg BID dose; n=15): 6-month PFS 89% Combination with exemestane + everolimus (200 mg BID dose; n=4): 6-month PFS 100% Combination with trastuzumab (150 mg BID dose; n=18): 6-month PFS 29% (HR+ breast cancer; n=11); 38% (HR− breast cancer; n=7) Combination with trastuzumab (200 mg BID dose; n=6): 6-month PFS 50% (HR+ breast cancer; n=5); 0 (HR− breast cancer; n=1) |
| NCT01394016 (79) | None | I | Metastatic breast cancer expansion cohort (N=47) | – |
All (N=47): 23% PR, 47% SD, DCR 70%, median PFS 5.8 months HR+ (n=36): 31% PR, 50% SD, DCR 81%, median PFS 8.8 months |
| NCT01394016 (79) | Fulvestrant | I | HR+ ABC (N=19) | Neutropenia (32%), leukopenia (26%), abdominal pain (11%), anemia (11%) | 21% PR, ORR 21%, DCR 79%, CBR 63% |
| NSCLC | |||||
| NCT01394016 (79) | None | I | NSCLC expansion cohort (N=68) | – |
All NSCLC (N=68): 3% PR, 46% SD, 49% DCR, median PFS 2 months KRAS-mutant NSCLC (n=29): 3% PR, 31% SD ≥24 weeks, 55% DCR, median PFS 2.8 months KRAS-wildtype NSCLC (n=33): 3% PR, 12% SD ≥24 weeks, 39% DCR, median PFS 1.9 months |
BID, twice daily; CBR, clinical benefit rate; CDKN2A, cyclin-dependent kinase inhibitor 2A; CI, confidence interval; CR, complete response; CRC, colorectal cancer; DCR, disease control rate; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; HER2+, HER2-positive; HR, hazard ratio; KRAS, V-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog; MCL, mantle cell lymphoma; MRT, malignant rhabdoid tumor; NSCLC, non-small cell lung cancer; ORR, overall response rate; Rb+, Rb-positive.
Ribociclib is a selective CDK4/6 inhibitor, which received FDA Breakthrough Therapy designation in August 2016 and Priority Review in November 2016 in combination with letrozole for the first-line treatment of HR+, human epidermal growth factor receptor 2-negative (HER2−) ABC (25). This review will outline the development of ribociclib, and provide an overview of the preclinical and clinical data for ribociclib across various tumor types.
Characteristics of ribociclib
Ribociclib, palbociclib, and abemaciclib are all orally bioavailable, small molecule inhibitors, that bind to the ATP cleft of CDK4 and CDK6. However, abemaciclib appears to bind more readily to the ATP cleft and forms a hydrogen bond with a catalytic residue (Lys43) that is conserved among kinases, suggesting it binds with less selectivity than ribociclib and palbociclib (26). In contrast, ribociclib and palbociclib appear to have greater lipophilicity (Table 2) and larger binding site side chains than abemaciclib, which might reduce the number of off-target kinase ATP-binding pockets they interact with (26). Indeed, ribociclib, palbociclib, and abemaciclib exhibit varying half maximal inhibitory concentration (IC50) values against different CDK− and non-CDK–cyclin complexes in biochemical assays (Table 2) (26–29). Interestingly, in a chemoproteomics study of CDK4/6 inhibitor activity in lung carcinoma cell lines and primary tumor samples, ribociclib was found to be significantly more selective towards CDK4 and CDK6 than palbociclib, which interacted with more than twice as many kinases than ribociclib (30).
Table 2.
Key characteristics of CDK4/6 inhibitors in clinical development for solid tumors.
| Ribociclib (LEE011) (26, 27, 31, 32) | Palbociclib (Ibrance®; PD-0332991) (20, 26, 28) | Abemaciclib (LY2835219) (26, 29, 70) | |
|---|---|---|---|
|
| |||
| IC50 (nM) – on target CDKs | |||
|
| |||
| CDK4–cyclin D1 | 10 | 11 | 2 |
| CDK6–cyclin D1/2/3 | 39 | 16 | 10 |
|
| |||
| IC50 (nM) – on other CDKs | |||
| CDK1–cyclin B | 113,000 | >10,000 | 1627 |
| CDK2–cyclin A/E | 76,000 | >10,000 | 504 |
| CDK5–p25 | 43,900 | >10,000 | 355 |
| CDK9–cyclin T | NR | NR | 57 |
|
| |||
| Kinase partition index | 0.99 | 0.96 | 0.88 |
|
| |||
| Lipophilicity (cLogP) | 2.3 | 2.7 | 5.5 |
|
| |||
| IC50 against bone marrow mononuclear cells (nM) | 1700 ± 231 | 240 ± 43 | 230 ± 27 |
|
| |||
| Half-life | 33–42 hours | 26–27 hours | 17–38 hours |
|
| |||
| Tmax | 1–5 hours | 6–12 hours | 4–6 hours |
cLogP, calculated Log of the partition coefficient.
Early clinical experience with ribociclib
The first Phase I clinical studies evaluated single-agent ribociclib across a range of Rb-positive advanced solid tumors and lymphomas in US/European (N=132) and Japanese patients (N=17) (31, 32). The recommended Phase II dose (RP2D) of single-agent ribociclib was declared as 600 mg/day on a 3-weeks-on/1-week-off schedule (31, 32). Pharmacokinetic analyses determined that ribociclib is rapidly absorbed, with a time to maximum concentration (Tmax) of 1–5 hours, and a half-life (t1/2) of 33–42 hours (Table 2) (31, 32). In Japanese patients, ribociclib exposure appeared higher on average than in non-Japanese patients, although considerable inter-patient variability was observed (31, 32). In a separate, healthy volunteer study, overall exposure of a single oral dose of 600 mg ribociclib was unaffected in fed versus fasted states, indicating that ribociclib may be taken with or without food (33).
Safety analyses from the Phase I studies indicated that single-agent ribociclib is associated with a manageable safety profile. The most common treatment-related adverse events (AEs) were hematologic, particularly neutropenia, consistent with on-target CDK4/6 inhibitor toxicity (31, 32). Non-hematologic AEs included nausea and fatigue (31, 32). Grade 1/2 QTc prolongation was reported in patients receiving the RP2D and subsequent trials included additional cardiac monitoring (31). AEs were generally mild-to-moderate in severity, and were reversible upon ribociclib interruption (31, 32).
Preliminary antitumor activity was observed in the Phase I studies (31, 32). Among US/European patients, the large majority of whom were heavily pretreated, three had partial responses (PRs) and 41 had stable disease (SD); eight patients had SD for >6 months (31). The PRs occurred in a patient with head and neck acinar carcinoma and CDKN2A loss, another with PIK3CA-mutant, CCND1-amplified, estrogen receptor-positive (ER+) breast cancer, and another with BRAF/NRAS-wild-type, CCND1-amplified melanoma (31). In the Japanese population, who were also heavily pretreated, SD was observed in four patients treated at the RP2D: two with peritoneal cancer, one with esophageal cancer, and one with breast cancer (32). These data suggest that ribociclib, through its specific mechanism of action, has activity in humans.
Preclinical and clinical experience with ribociclib in individual indications
Ribociclib has demonstrated antitumor activity in preclinical and clinical studies of a wide variety of tumor types, including breast cancer, melanoma, and neuroblastoma. While single-agent activity has been demonstrated for ribociclib, it has also been shown to enhance the activity of combination partners and delay the development of treatment resistance in preclinical and clinical studies.
Breast cancer
Preclinical
Breast tumors frequently harbor aberrations of the cyclin D–CDK4/6–p16–Rb pathway (34–36) (Supplementary Table 1), and this pathway is also implicated in resistance to endocrine therapy (3). Therefore, targeting both the cyclin D–CDK4/6–p16–Rb and ER pathways may delay the development of resistance. In a preclinical study of 50 breast cancer cell lines, ribociclib demonstrated inhibitory activity predominantly against ER+ cell lines (37), suggesting that ER+ breast cancer cells might be particularly susceptible to CDK4/6 inhibition. In vivo, ribociclib showed significant tumor growth inhibition in xenograft mouse models of ER+ breast cancer (37). A preclinical study in CDK4/6 inhibitor-resistant breast cancer cell lines suggests that mechanisms of resistance differ between ribociclib and palbociclib. Ribociclib resistant clones demonstrated increased E2F1, compared with increased cycle E protein levels in palbociclib resistant clones (38). Combinations of ribociclib with endocrine therapies was also associated with potent antitumor effects in ER+ breast cancer models compared with the respective single agents (38, 39).
The phosphatidylinositol 3-kinase (PI3K)/AKT/mammalian target of rapamycin (mTOR) pathway has also been widely implicated in breast cancer tumorigenesis and treatment resistance (8). As cyclin D1 is frequently regulated in a PI3K/AKT/mTOR-dependent manner, combinations of upstream and downstream inhibitors might act cooperatively. Indeed, combination of ribociclib with the PI3K inhibitor alpelisib (BYL719) resulted in enhanced tumor regression (−57%) versus single-agent treatments with ribociclib (−9%) and alpelisib (−15%) (39). More recently, large-scale, patient-derived breast cancer xenografts (PDX) were used to evaluate such combinations in mouse preclinical trials. Treatment of 38 PDX mouse models with ribociclib plus alpelisib demonstrated increased response rates and progression-free survival (PFS) with this combination compared with the single agents (40). Interestingly, the ribociclib plus alpelisib combination appeared more active in PDX models than in cell lines, suggesting a possible disconnect between in vitro cell-based assays and in vivo PDX-based results (40). Furthermore, the addition of PI3K inhibitors to ribociclib and either letrozole or fulvestrant demonstrated increased antitumor activity, including some complete regressions, without significant toxicity in mouse models of ER+ breast cancer (37). These regressions were sustained for ~4 weeks post treatment and occurred in both PI3K/PTEN-wild-type and -altered backgrounds. Taken together, the synergistic activity of ribociclib in combination with various anticancer therapies suggest that ribociclib may complement existing breast cancer treatments in the clinic.
Clinical
The combination of ribociclib and endocrine therapies in HR+, HER2− breast cancer is being investigated in Phase Ib–III studies (Table 3 and Supplementary Table 2). These studies have demonstrated that ribociclib exposure is unaffected by combinations with exemestane, letrozole, or fulvestrant in patients with HR+ ABC (41, 42). Similarly, letrozole exposure when combined with ribociclib was within the range of values observed from single-agent letrozole (41, 43). The addition of ribociclib to exemestane, letrozole, or fulvestrant was also associated with manageable tolerability profiles in all studies (Table 3). The most common AEs were hematologic, and Grade 3/4 neutropenia was frequent but uncomplicated (42, 44–46). QT prolongation has been observed following ribociclib treatment in combination with endocrine therapy; cases were predominantly Grade 1–2 in severity with prolongation limited by proactive dose modifications (31, 46). AEs were manageable and reversible upon treatment interruption (46, 47). In the Phase III MONALEESA-2 study of ribociclib plus letrozole in the first-line treatment of postmenopausal women with HR+, HER2− ABC, ribociclib dose intensity was 88% despite dose interruptions, and only 7.5% of patients discontinued ribociclib plus letrozole treatment due to AEs (46).
Table 3.
Clinical experience with ribociclib combinations.
| Study name/ID | Combination drug | Phase | Population | MTD/RP2D/dose | Reported Grade 3/4 AEs | Clinical activity |
|---|---|---|---|---|---|---|
| HR+, HER2− breast cancer | ||||||
| CLEE011X2106/NCT01857193 (44) | Exemestane | Ib | Postmenopausal women with ER+, HER2− ABC previously treated with letrozole or anastrozole (N=14 treated with ribociclib + exemestane) |
Evaluated dose Ribociclib: 600 mg/day (3-weeks-on/1-week-off) Exemestane: 25 mg/day |
Neutropenia (71%), leukopenia (36%), lymphopenia (14%), ALT elevation (14%), AST elevation (14%), and anemia (14%) | 2 unconfirmed PR, 4 SD |
| CLEE011X2107/NCT01872260 (45, 47) | Letrozole | Ib | Pretreated and treatment-naïve postmenopausal women with ER+, HER2− ABC (N=47 treated with ribociclib + letrozole) |
RP2D: Ribociclib: 600 mg/day (3-weeks-on/1-week-off) Letrozole: 2.5 mg/day |
All patients: Neutropenia and neutrophil count reduced (60%), ALT elevation (4%), AST elevation (4%), asthenia (2%), constipation (2%), nausea (2%), UTI (2%), fatigue (1%) First line (n=28): Neutropenia and neutrophil count reduced (64%), ALT elevation (4%), AST elevation (4%), asthenia (4%), nausea (4%) Previously treated (n=19): Neutropenia and neutrophil count reduced (53%), ALT elevation (5%), AST elevation (5%), constipation (5%), fatigue (5%), UTI (5%) |
First line (n=28): 2 CR, 11 PR, 3 unconfirmed PR, 5 SD, 4 NCRNPD, ORR 46%, DCR 89%, CBR 79%, Median PFS 25.3 months Previously treated (n=19): Median PFS 5.5 months |
| CLEE011X2108/NCT02088684 (42) | Fulvestrant | Ib | Postmenopausal women with HR+, HER2− ABC (N=28). |
Ribociclib: 600 mg/day (3-weeks-on/1-week-off) or 400 mg/day (continuous) Fulvestrant: 500 mg on Days 1 and 15 of Cycle 1 and Day 1 of subsequent cycles |
Ribociclib 600 mg/day (3-weeks-on/1-week-off;n=13): Neutropenia (62%), fatigue (15%), leukocyte count reduced (15%), ALT elevation (8%), AST elevation (8%) Ribociclib 400 mg/day (continuous;n=15): Neutropenia (33%), leukocyte count reduced (7%), ALT elevation (7%), AST elevation (7%) |
Ribociclib 600 mg/day (3-weeks-on/1-week-off;n=13): 3 PR, 9 SD, 1 NCRNPD Ribociclib 400 mg/day (continuous;n=15): 2 PR, 7 SD, 5 NCRNPD |
| CLEE011X2106/NCT01857193 (52) | Everolimus + exemestane | Ib | Postmenopausal women with ER+, HER2− ABC previously treated with letrozole or anastrozole (N=77 treated with ribociclib + everolimus + exemestane) |
RP2D: Ribociclib: 300 mg/day (3-weeks-on/1-week-off) Everolimus: 2.5 mg/day Exemestane: 25 mg/day |
Neutropenia (31%), neutrophil count reduced (18%), leukocyte count reduced (12%), anemia (7%), thrombocytopenia (7%), lymphopenia (7%), ALT elevation (5%), AST elevation (4%), and lymphocyte reduced (4%) | ORR 9%, DCR 73%, CBR 26% |
| CLEE011X2107/NCT01872260 (51) | Alpelisib + letrozole | Ib | Pretreated and treatment-naïve postmenopausal women with ER+, HER2− ABC (N=46 treated with ribociclib + alpelisib + letrozole) |
RP2D: Ribociclib: 300 mg/day (3-weeks-on/1-week-off) Alpelisib: 200 mg/day Letrozole: 2.5 mg/day |
Increased ALT (30%), increased AST (26%), hyperglycemia (17%), neutropenia (17%), fatigue (13%), reduced neutrophil count (4%), anemia (4%), thrombocytopenia (2%), vomiting (2%), and nausea (2%) | ORR 16%, DCR 70%, CBR 26% |
| CLEE011A2201/NCT01919229 (43) | Letrozole | II | Postmenopausal women with HR+, HER2− Grade II/III, invasive, early breast cancer who have received no prior breast cancer treatment (N=14) |
Ribociclib: 600 mg/day or 400mg/day Letrozole: 2.5 mg/day |
All AEs were mild/moderate with no Grade 3/4 AEs |
Ribociclib 400 mg/day + letrozole: 96% decrease in Ki67 Ribociclib 600 mg/day + letrozole: 92% decrease in Ki67 Letrozole only: 69% decrease in Ki67 |
| MONALEESA-2/NCT01958021 (46) | Letrozole | III | Postmenopausal women with HR+, HER2− ABC who have received no prior treatment for advanced disease (N=668) |
Ribociclib: 600 mg/day (3-weeks-on/1-week-off) Letrozole: 2.5 mg/day |
Ribociclib + letrozole arm vs placebo + letrozole arm: Neutropenia (59% vs 1%), leukopenia (21% vs 1%), hypertension (10% vs 11%), increased ALT (9% vs 1%), lymphopenia (7% vs 1%), and increased AST (6% and 1%) |
Ribociclib + letrozole arm vs placebo + letrozole arm: Median PFS NR (95% CI, 19.3–NR) vs 14.7 months (95% CI, 13.0–16.5); HR=0.56; P=3.29×10−6 ORR 41% vs 28% (P<0.001) CBR 80% vs 72% (P=0.02) |
| NRAS- or BRAF-mutant melanoma | ||||||
| CMEK162X2114/NCT01781572) (62) | Binimetinib | Ib/II | Patients with advanced NRAS- mutant melanoma (N=22 received ribociclib + binimetinib) |
MTD: Ribociclib: 200 mg/day (3-weeks-on/1-week-off) Binimetinib: 45 mg BID RP2D: ongoing |
CPK elevation (18%), neutropenia (9%), acneiform (4%), dermatitis (4%), and rash (4%) | 7 PR, 11 SD, 33% had 20–30% tumor shrinkage, CBR 86% |
| CLEE011X2105/NCT01777776 (61) | Encorafenib | Ib/II | Patients with advanced BRAFV600-mutant melanoma (N=28 received ribociclib + encorafenib) |
MTD: ongoing RP2D: ongoing |
Hand–foot syndrome (11%), rash (4%), and myalgia (4%) | 2 confirmed PRs, 3 unconfirmed PRs, 10 SD, 1 SD >9 cycles |
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CBR, clinical benefit rate; CR, complete response; DCR, disease control rate; NCRNPD, not complete response nor progressive disease; NR, not reached; ORR, overall response rate; UTI, urinary tract infection.
Clinical activity of ribociclib was observed in studies of HR+ ABC (Table 3) (42, 44–46). In MONALEESA-2, where 668 patients with HR+ ABC were randomized to receive ribociclib plus letrozole or placebo plus letrozole, ribociclib plus letrozole significantly increased PFS relative to placebo plus letrozole in the first-line setting (median PFS: not reached vs 14.7 months; hazard ratio=0.56; P=3.29×10−6) (46). The PFS rate at 12 months was 72.8% versus 60.9% in the ribociclib and placebo groups, respectively (46). A significant hazard ratio benefit for ribociclib plus letrozole was also observed across all pre-specified patient subgroups, including older patients (≥65 years) and those with visceral metastases, bone-only disease, or de novo ABC (46, 48, 49). In the ribociclib plus letrozole arm, decreased tumor size at the initial evaluation (~Week 8) was observed in 76% of evaluable patients with measurable disease (50). In newly diagnosed Grade II/III HR+, HER2− invasive breast cancer, a randomized pre-surgical study demonstrated an enhanced reduction in expression of the Ki67 marker for cell proliferation upon combination of ribociclib and letrozole (≥92%) versus letrozole alone (69%), further supporting a role for ribociclib in enhancing the antitumor effects of its combination partner (43). An ongoing trial (NCT02712723) is investigating ribociclib plus letrozole in the neoadjuvant setting (Supplementary Table 2). Preliminary clinical activity has also been established with ribociclib plus fulvestrant in pretreated HR+, HER2− ABC, and PRs were observed in patients who received prior fulvestrant (42). When evaluating potential biomarkers of response, preliminary clinical activity with ribociclib plus letrozole or fulvestrant was reported in patients with ER+ breast cancer tumors carrying alterations in PI3K/AKT/mTOR or cyclin D–CDK4/6–p16–Rb pathways, suggesting a possible benefit in patients whose tumors carry these alterations (42, 45).
Encouraging preliminary clinical activity has also been demonstrated with triplet therapy of ribociclib, exemestane, and everolimus (mTOR inhibitor), as well as ribociclib, letrozole, and alpelisib (PI3Kα selective inhibitor) in pretreated patients with HR+ ABC (Table 3 and Supplementary Table 2) (47, 51, 52). While ribociclib exposure remained unaltered by combination with everolimus, exposure to everolimus, which is metabolized by cytochrome P450 3A4 (CYP3A4), increased 1.5–3-fold when combined with ribociclib (41). However, use of lower doses of everolimus (e.g. 2.5 mg/day) resulted in exposures within the ranges achieved with single-agent everolimus dosing (e.g. 5–10 mg/day), with potentially lower toxicity (41, 52). Triplet therapy with ribociclib, everolimus, and exemestane in pretreated patients with ER+ ABC was associated with manageable safety (Table 3) (52). During triplet therapy with ribociclib, alpelisib, and letrozole, PK indices for ribociclib and alpelisib were generally consistent with historic single-agent data (51). The combination of ribociclib, alpelisib, and letrozole also demonstrated an acceptable safety profile (Table 3) (51). Both triplet regimens have demonstrated antitumor activity in patients whose ER+ breast cancer tumors harbor PI3K/AKT/mTOR and/or cyclin D–CDK4/6–p16–Rb pathway modifications (51, 52). Further evaluation and validation of biomarkers of response is ongoing.
Melanoma
Preclinical
The now-refined genetic landscape of melanoma has highlighted the centrality of RAS signaling in this disease. Indeed, activating mutations occur in critical components of this pathway, including BRAF V600 (35–50%), NRAS (10–25%), and NF1 (~15%) (53, 54). The cyclin D–CDK4/6–p16–Rb pathway is also commonly dysregulated in melanomas. Mutations, deletions, or hypermethylation of CDKN2A are key driver alterations in melanomas, and CCND1 (cyclin D1) and CDK4 are frequently amplified (Supplementary Table 1) (53–57). Germline mutations in CDKN2A and CDK4 are also linked to familial melanoma (58). High CCND1 and low CDKN2A copy numbers have been associated with reduced PFS with BRAF inhibitors (59).
Approved treatments for BRAF-mutant melanoma include targeted therapy with BRAF and/or MEK inhibitors (60). Binimetinib (MEK162), a MEK inhibitor, and encorafenib (LGX818), a selective BRAF inhibitor, have demonstrated antitumor activity as single agents in NRAS- and BRAF-mutant melanomas, respectively, and in combination in BRAF-mutant melanomas (61–63). The combination of ribociclib and binimetinib demonstrated enhanced tumor regression (34% tumor/control [T/C] ratio) in xenograft models of NRASQ61K-mutant melanoma relative to single-agent binimetinib (12% T/C) or ribociclib (32% T/C) (27, 62). In BRAFV600E-mutant melanoma models, low-dose ribociclib exhibited synergistic activity with encorafenib (27, 61). The addition of ribociclib to encorafenib also appeared to prevent resistance to encorafenib (27, 61), suggesting that simultaneous inhibition of BRAF and cyclin D–CDK4/6–p16–Rb pathways may provide a therapeutic benefit in the clinical setting. The enhanced antitumor activity of ribociclib plus encorafenib relative to single agents was confirmed in a large-scale in vivo screen of PDX melanoma models, where the combination was associated with a 100% response rate, including 87% PR and CR (exceeding the 72% PR and CR for binimetinib plus encorafenib) (40). The combination also resulted in a significant improvement in PFS and delayed the development of resistance in the tumor models (P=1.8×10−3), with no drug–drug interactions (40).
Clinical
The combinations of ribociclib plus binimetinib or encorafenib have been evaluated in two dose-escalation/expansion Phase Ib/II studies of advanced NRAS- and BRAF-mutant melanoma, respectively (Table 3) (61, 62). In patients with advanced NRAS-mutant melanoma, combination of ribociclib and binimetinib did not affect the PK exposures of either drug (41, 62). Common AEs experienced with ribociclib plus binimetinib included creatine phosphokinase (CPK) elevation, acneiform dermatitis, nausea, rash, edema, leukopenia, and creatinine elevation, whereas Grade 3/4 AEs included CPK elevation, neutropenia, acneiform dermatitis, and rash (Table 3) (62). This combination was also associated with preliminary antitumor activity, including cases of PR (33%) and SD (52%) (Table 3) (62). In patients with advanced BRAFV600-mutant melanomas, the combination of ribociclib and encorafenib resulted in reduced ribociclib exposure and increased encorafenib exposure, most likely due to encorafenib-mediated CYP3A4 induction and to ribociclib-mediated CYP3A4 inhibition, respectively (41). The combination of ribociclib and encorafenib demonstrated clinical activity and an acceptable tolerability profile, with AEs consisting of hand–foot syndrome, nausea, pruritus, rash, and myalgia (Table 3) (61). Cases of PR and SD were observed in patients receiving ribociclib plus encorafenib whose tumors exhibited p16 loss or CDK4 mutation (61). There was little evidence of response in patients resistant to BRAF inhibition (61). The use of ribociclib and binimetinib and/or encorafenib combinations in melanoma is being investigated further in ongoing trials (Supplementary Table 2).
Neuroblastoma
Preclinical
Neuroblastoma is frequently driven by oncogenic activation of anaplastic lymphoma kinase (ALK), often resulting in cyclin D1 upregulation and cell proliferation (64). Consistent with this, extensive overexpression of cyclin D–CDK4/6 components have been observed in neuroblastomas (65). Array-based data showed that cyclin D1 expression is 3–8 times higher in neuroblastoma tumors than in libraries of 18 other common malignancies, including breast cancer (65). High expression of CDK4 and CDK6 and deletions of CDKN2A have also been associated with these tumors (Supplementary Table 1) (65–67).
Ribociclib activity has been profiled against >500 cell lines in the Cancer Cell Line Encyclopedia study, whereby neuroblastoma cell lines were identified as particularly sensitive to ribociclib (27). Here, ribociclib induced cytostasis at nanomolar concentrations in 12/17 human neuroblastoma-derived cell lines (67). In sensitive neuroblastoma cell line-derived xenograft mouse models, treatment with ribociclib was accompanied by a reduction in phosphorylated Rb, Ki67, and cell proliferation, leading to significant tumor growth delay throughout the treatment period (P<0.0001) (67). CDK4/6 is therefore an attractive target for neuroblastoma treatment.
Clinical
The efficacy and safety of single-agent ribociclib in patients with neuroblastoma was evaluated as part of the Phase I study investigating ribociclib in 31 pediatric patients (median age [range]: 5 [1–20] years) with malignant rhabdoid tumors (MRT), neuroblastoma, or CDK4/6 pathway-activated tumors (68). Consistent with single-agent data in adults, the maximum tolerated dose (MTD) and RP2D were 470 mg/m2/day (adult equivalent dose ≈800 mg/day) and 350 mg/m2/day (adult equivalent dose ≈600 mg/day), respectively, on a 3-weeks-on/1-week-off dosing schedule (68). Ribociclib was rapidly absorbed with a median Tmax of 2–5 hours, regardless of age (69). As in adults, ribociclib exposure in pediatric patients appeared to accumulate 2–3-fold in plasma, reaching steady state within 8 days (69). Clearance was 2–3 times slower in pediatric patients compared with adults, presumably due to their lower body weight (69). Ribociclib was well tolerated with mild-to-moderate reversible AEs, the majority of which were hematologic (68). Three patients, two with neuroblastoma and one with MRT, received ribociclib for ≥4 cycles; SD was the best overall response (68). Ribociclib remains the only CDK4/6 inhibitor investigated in a clinical trial of neuroblastoma.
Ongoing trials with ribociclib
Multiple trials of ribociclib are ongoing across different tumor types, including BRAFv600- and NRAS-mutant melanoma, non-small cell lung cancer, teratoma, liposarcoma, myelofibrosis, and gynecologic cancers; these are summarized in Supplementary Table 2. The most advanced trials are investigating ribociclib combinations in HR+ breast cancer. MONALEESA-3 is evaluating the addition of ribociclib to fulvestrant in patients with HR+ ABC who have received no or only one line of prior endocrine therapy. MONALEESA-7 is investigating the combination of ribociclib and tamoxifen or non-steroidal aromatase inhibitors plus goserelin in pre/perimenopausal women with HR+ ABC. MONALEESA-7 is the only trial entirely dedicated to investigating CDK4/6 inhibition in the pre/perimenopausal setting. In addition, based on preclinical rationale, a number of additional doublet and triplet combination studies are underway, including combinations of ribociclib with endocrine therapy and PI3K pathway inhibition (Supplementary Table 2).
Ribociclib in perspective
The clinical data for ribociclib adds to the wealth of emerging information supporting use of CDK4/6 inhibitors in the treatment of cancer. Certain differences among ribociclib, palbociclib, and abemaciclib, including PK factors, target selectivity, and toxicities, are likely to influence their activity or utility in individual settings. PK data with ribociclib demonstrate a long half-life compared with palbociclib and abemaciclib (Table 2). While the half-lives of ribociclib and palbociclib enable once-daily, 3-weeks-on/1-week-off dosing (14), the PK/pharmacodynamic profile of abemaciclib favors twice-daily, continuous dosing (29, 70). The convenience of intermittent versus continuous dosing and its impact on treatment adherence and outcomes remains to be explored. Once-daily, continuous dosing of ribociclib in combination with endocrine therapies is being evaluated in ongoing breast cancer trials (NCT02088684, NCT02712723, NCT02732119) (42). PK data indicate that ribociclib can be taken with or without food, whereas palbociclib must be administered with food (20, 33), and that ribociclib may be absorbed more rapidly than palbociclib and abemaciclib (Table 2) (70, 71). Preclinically, ribociclib appears to have less toxicity against bone marrow mononuclear cells compared with palbociclib and abemaciclib (Table 2) (26), which may potentially translate into fewer hematologic toxicities. Hematologic toxicities were reported with ribociclib plus letrozole in MONALEESA-2 and with palbociclib plus letrozole in PALOMA-2 (18, 46). Differences in target selectivity also lead to variations in safety: with abemaciclib demonstrating increased frequency of gastrointestinal AEs versus ribociclib or palbociclib (Table 1) (14). Ribociclib is generally well tolerated, with predictable AEs that are easily manageable by dose adjustment or treatments.
Finally, preclinical data suggest that both ribociclib and abemaciclib can cross the blood–brain barrier, supporting further exploration with central nervous system tumors (72, 73).
Conclusion
Ribociclib is a promising, selective CDK4/6 inhibitor in the late stages of clinical development, demonstrating preclinical and clinical activity across a range of tumor types, including HR+ breast cancer. The preclinical, clinical, and PK profiles of ribociclib in a variety of tumor types make it an important addition to the class of CDK4/6 inhibitors. Given the selectivity of ribociclib towards CDK4/6, the addition of ribociclib to existing anticancer therapies in doublet and triplet combinations has been successful, enhancing efficacy of existing therapies with minimal increases in toxicity in preclinical and clinical studies. This result is being explored extensively across a range of tumor types and in combination with a variety of anticancer agents (Supplementary Table 2). Establishing validated biomarkers of clinical response to ribociclib will help define patient populations who will benefit most from treatment, improve treatment outcomes, and identify effective drug combinations to mitigate treatment resistance. The comprehensive and robust portfolio of unique and ongoing clinical studies of doublet and triplet therapies containing ribociclib are likely to shape the future landscape of cancer therapeutics.
Supplementary Material
Acknowledgments
Financial support
Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals Corporation.
Grant support: The project described was supported in part by award number P30CA014089 from the National Cancer Institute (D. Tripathy). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health. A. Bardia is supported by the National Institutes of Health (4K12CA087723-14).
The authors thank Abbie Saunders PhD for medical editorial assistance with this manuscript.
Footnotes
Conflict of interest disclosure statement
D Tripathy discloses clinical trial grants and editorial support funded by Novartis Pharmaceuticals Corporation in relation to this submitted work. He also discloses consultancy fees from Nektar Therapeutics outside the submitted work. A Bardia discloses participating in an advisory board for Novartis Pharmaceuticals Corporation. W Sellers was previously employed by, and owns shares in, Novartis Pharmaceuticals Corporation.
References
- 1.Abukhdeir AM, Park BH. P21 and p27: Roles in carcinogenesis and drug resistance. Expert Rev Mol Med. 2008;10:e19. doi: 10.1017/S1462399408000744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Caldon CE, Daly RJ, Sutherland RL, Musgrove EA. Cell cycle control in breast cancer cells. J Cell Biochem. 2006;97:261–74. doi: 10.1002/jcb.20690. [DOI] [PubMed] [Google Scholar]
- 3.Lange CA, Yee D. Killing the second messenger: Targeting loss of cell cycle control in endocrine-resistant breast cancer. Endocr Relat Cancer. 2011;18:C19–24. doi: 10.1530/ERC-11-0112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Johnson A, Skotheim JM. Start and the restriction point. Curr Opin Cell Biol. 2013;25:717–23. doi: 10.1016/j.ceb.2013.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shapiro GI. Cyclin-dependent kinase pathways as targets for cancer treatment. J Clin Oncol. 2006;24:1770–83. doi: 10.1200/JCO.2005.03.7689. [DOI] [PubMed] [Google Scholar]
- 6.Baker SJ, Reddy EP. CDK4: A key player in the cell cycle, development, and cancer. Genes Cancer. 2012;3:658–69. doi: 10.1177/1947601913478972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Michaloglou C, Vredeveld LC, Soengas MS, Denoyelle C, Kuilman T, van der Horst CM, et al. BRAFE600-associated senescence-like cell cycle arrest of human naevi. Nature. 2005;436:720–4. doi: 10.1038/nature03890. [DOI] [PubMed] [Google Scholar]
- 8.Hosford SR, Miller TW. Clinical potential of novel therapeutic targets in breast cancer: CDK4/6, src, JAK/STAT, PARP, HDAC, and PI3K/AKT/mTOR pathways. Pharmgenomics Pers Med. 2014;7:203–15. doi: 10.2147/PGPM.S52762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Thangavel C, Dean JL, Ertel A, Knudsen KE, Aldaz CM, Witkiewicz AK, et al. Therapeutically activating RB: Reestablishing cell cycle control in endocrine therapy-resistant breast cancer. Endocr Relat Cancer. 2011;18:333–45. doi: 10.1530/ERC-10-0262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Miller TW, Balko JM, Fox EM, Ghazoui Z, Dunbier A, Anderson H, et al. ERalpha-dependent E2F transcription can mediate resistance to estrogen deprivation in human breast cancer. Cancer Discov. 2011;1:338–51. doi: 10.1158/2159-8290.CD-11-0101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Beroukhim R, Mermel C, Porter D, Wei G, Raychaudhuri S, Donovan J, et al. The landscape of somatic copy-number alteration across human cancers. Nature. 2010;463:899–905. doi: 10.1038/nature08822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kobayashi S, Shimamura T, Monti S, Steidl U, Hetherington C, Lowerll A, et al. Transcriptional profiling identifies cyclin D1 as a critical downstream effector of mutant epidermal growth factor receptor signaling. Cancer Res. 2006;66:11389–98. doi: 10.1158/0008-5472.CAN-06-2318. [DOI] [PubMed] [Google Scholar]
- 13.Solit D, Garraway L, Pratilas C, Sawai A, Getz G, Basso A, et al. BRAF mutation predicts sensitivity to MEK inhibition. Nature. 2006;439:358–62. doi: 10.1038/nature04304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Asghar U, Witkiewicz AK, Turner NC, Knudsen ES. The history and future of targeting cyclin-dependent kinases in cancer therapy. Nat Rev Drug Discov. 2015;14:130–46. doi: 10.1038/nrd4504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dickson MA. Molecular pathways: CDK4 inhibitors for cancer therapy. Clin Cancer Res. 2014;20:3379–83. doi: 10.1158/1078-0432.CCR-13-1551. [DOI] [PubMed] [Google Scholar]
- 16.Mita MM, Joy AA, Mita A, Sankhala K, Jou YM, Zhang D, et al. Randomized phase II trial of the cyclin-dependent kinase inhibitor dinaciclib (MK-7965) versus capecitabine in patients with advanced breast cancer. Clin Breast Cancer. 2014;14:169–76. doi: 10.1016/j.clbc.2013.10.016. [DOI] [PubMed] [Google Scholar]
- 17.Stephenson JJ, Nemunaitis J, Joy AA, Martin JC, Jou YM, Zhang D, et al. Randomized phase 2 study of the cyclin-dependent kinase inhibitor dinaciclib (MK-7965) versus erlotinib in patients with non-small cell lung cancer. Lung Cancer. 2014;83:219–23. doi: 10.1016/j.lungcan.2013.11.020. [DOI] [PubMed] [Google Scholar]
- 18.Finn RS, Martin M, Rugo HS, Jones S, Im S, Gelmon K, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375:1925–36. doi: 10.1056/NEJMoa1607303. [DOI] [PubMed] [Google Scholar]
- 19.Turner NC, Ro J, Andre F, Loi S, Verma S, Iwata H, et al. Palbociclib in hormone-receptor-positive advanced breast cancer. N Engl J Med. 2015;373:209–19. doi: 10.1056/NEJMoa1505270. [DOI] [PubMed] [Google Scholar]
- 20. [Accessed December 2016];IBRANCE® (palbociclib) prescribing information. Available from http://Labeling.pfizer.com/ShowLabeling.aspx?id=2191.
- 21.Pfizer. [Accessed December 2016];IBRANCE® (palbociclib) receives approval in European Union for the treatment of women with HR+/HER2− metastatic breast cancer. Available from: http://www.pfizer.com/news/press-release/press-release-detail/ibrance_palbociclib_receives_approval_in_european_union_for_the_treatment_of_women_with_hr_her2_metastatic_breast_cancer.
- 22.Dickler M, Tolaney S, Rugo H, Cortes J, Diéras V, Patt D, et al. MONARCH 1: Results from a Phase II study of abemaciclib, a CDK4 and CDK6 inhibitor, as monotherapy, in patients with HR+/HER2− breast cancer, after chemotherapy for advanced disease. J Clin Oncol. 2016;34(suppl) Abstract 510 (Oral presentation) [Google Scholar]
- 23.Goetz M, Beeram M, Beck T, Conlin A, Dees E, Dickler M, et al. Abemaciclib, an inhibitor of CDK4 and CDK6, combined with endocrine and HER2-targeted therapies for women with metastatic breast cancer. Cancer Res. 2016;76(4 suppl) Poster P4-13-25. [Google Scholar]
- 24.Lilly. [Accessed December 2016];Lilly receives FDA breakthrough therapy designation for abemaciclib - a CDK 4 and 6 inhibitor - in advanced breast cancer. Available from: https://Investor.lilly.com/releasedetail.cfm?releaseid=935735.
- 25.Novartis. [Accessed December 2016];Novartis LEE011 (ribociclib) granted FDA priority review for first-line treatment of HR+/HER2− advanced breast cancer. Available from: https://www.novartis.com/news/media-releases/novartis-lee011-ribociclib-granted-fda-priority-review-first-line-treatment.
- 26.Chen P, Lee N, Hu W, Xu M, Ferre R, Lam H, et al. Spectrum and degree of CDK drug interactions predicts clinical performance. Mol Cancer Ther. 2016;15:2273–81. doi: 10.1158/1535-7163.MCT-16-0300. [DOI] [PubMed] [Google Scholar]
- 27.Kim S, Loo A, Chopra R, Caponigro G, Huang A, Vora S, et al. LEE011: An orally bioavailable, selective small molecule inhibitor of CDK4/6–reactivating rb in cancer. Mol Cancer Ther. 2013;12(11 suppl) Abstract PR02 (Oral presentation) [Google Scholar]
- 28.Fry DW, Harvey PJ, Keller PR, Elliott WL, Meade M, Trachet E, et al. Specific inhibition of cyclin-dependent kinase 4/6 by PD 0332991 and associated antitumor activity in human tumor xenografts. Mol Cancer Ther. 2004;3:1427–38. [PubMed] [Google Scholar]
- 29.Gelbert LM, Cai S, Lin X, Sanchez-Martinez C, Del Prado M, Lallena MJ, et al. Preclinical characterization of the CDK4/6 inhibitor LY2835219: In-vivo cell cycle-dependent/independent anti-tumor activities alone/in combination with gemcitabine. Invest New Drugs. 2014;32:825–37. doi: 10.1007/s10637-014-0120-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sumi N, Kuenzi B, Knezevic C, Rix L, Rix U. Chemoproteomics reveals novel protein and lipid kinase targets of clinical CDK4/6 inhibitors in lung cancer. ASC Chem Biol. 2015;10:2680–6. doi: 10.1021/acschembio.5b00368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Infante J, Cassier P, Gerecitano J, Witteveen P, Chugh R, Ribrag V, et al. A phase I study of the cyclin-dependent kinase 4/6 inhibitor ribociclib (LEE011) in patients with advanced solid tumors and lymphomas. Clin Cancer Res. 2016;22:5696–705. doi: 10.1158/1078-0432.CCR-16-1248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Yamada Y, Ishikawa N, Kakizume T, Tajima T, Hewes B, Doi T. A phase I study of single-agent ribociclib in japanese patients with advanced solid tumors. Mol Cancer Ther. 2015;14(12 suppl) doi: 10.1111/cas.13428. Abstract B31 (Poster) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Dhuria SV, Siddani R, Kosecki CM, Germa C, Mondal S. A phase I food-effect study of the ribociclib (LEE011) drug-in-capsule (DiC) formulation in healthy subjects. J Clin Oncol. 2015;33(suppl) Abstract e13577. [Google Scholar]
- 34.Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490:61–70. doi: 10.1038/nature11412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Musgrove EA, Caldon CE, Barraclough J, Stone A, Sutherland RL. Cyclin D as a therapeutic target in cancer. Nat Rev Cancer. 2011;11:558–72. doi: 10.1038/nrc3090. [DOI] [PubMed] [Google Scholar]
- 36.Geradts J, Wilson PA. High frequency of aberrant p16(INK4A) expression in human breast cancer. Am J Pathol. 1996;149:15–20. [PMC free article] [PubMed] [Google Scholar]
- 37.O’Brien N, Di Tomaso E, Ayala R, Tong L, Issakhanian S, Linnartz R, et al. In vivo efficacy of combined targeting of CDK4/6, ER and PI3K signaling in ER+ breast cancer. Cancer Res. 2014;74(19 suppl) Abstract 4756. [Google Scholar]
- 38.Lenihan C, Bouchekioua-Bouzaghou K, Abdulghani R, Chupin J, Shia A, Schmid P. CDK4/6 inhibitor resistant ER-positive cells remain dependent on estrogen signalling and retain sensitivity to endocrine therapy. San Antonio Breast Cancer Symposium; 2016. Poster P3-03-12. [Google Scholar]
- 39.Parasuraman S, Caponigro G, Loo A, Cao Z, Kim S, Issa I, et al. LEE011, a potent and selective CDK4/6 inhibitor, under preclinical and clinical investigation. Targeted Anticancer Therapies Congress. 2014 Oral presentation O4.4. [Google Scholar]
- 40.Gao H, Korn J, Ferretti S, Monahan J, Wang Y, Singh M, et al. High-throughput screening using patient-derived tumor xenografts to predict clinical trial drug response. Nat Med. 2015;21:1318–25. doi: 10.1038/nm.3954. [DOI] [PubMed] [Google Scholar]
- 41.Bhansali S, Parasuraman S, Hewes B, Einolf H, Umehara K, Matano A, et al. Application of SimCyp® and real-time pharmacokinetic assessments in defining dose in novel–novel combinations with potential drug–drug interactions in cancer patients. American College of Clinical Pharmacology Congress; 2014. Poster 27. [Google Scholar]
- 42.Tolaney S, Forero-Torres A, Boni V, Bachelot T, Lu Y, Maur M, et al. Ribociclib + fulvestrant in postmenopausal women with HR+, HER2– advanced breast cancer (ABC). San Antonio Breast Cancer Symposium; 2016. Poster P4-22-12. [Google Scholar]
- 43.Curigliano G, Gómez Pardo P, Meric-Bernstam F, Conte P, Lolkema M, Beck J, et al. Ribociclib plus letrozole in early breast cancer: A presurgical, window-of-opportunity study. Breast. 2016;28:191–8. doi: 10.1016/j.breast.2016.06.008. [DOI] [PubMed] [Google Scholar]
- 44.Bardia A, Modi S, Chavez-MacGregor M, Kittaneh M, Marino A, Matano A, et al. Phase Ib/II study of LEE011, everolimus, and exemestane in postmenopausal women with ER+/HER2− metastatic breast cancer. J Clin Oncol. 2014;32:5s(suppl) Abstract 535. [Google Scholar]
- 45.Munster P, Ismail-Khan R, Garcia-Estevez L, Mayer I, Becerra C, Hamilton E, et al. Phase Ib safety, efficacy, and molecular analysis of ribociclib (LEE011) plus letrozole for the treatment of ER+, HER2− advanced breast cancer. San Antonio Breast Cancer Symposium; 2016. Poster P4-22-18. [Google Scholar]
- 46.Hortobagyi G, Stemmer S, Burris H, Yap Y, Sonke G, Paluch-Shimon S, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375:1738–48. doi: 10.1056/NEJMoa1609709. [DOI] [PubMed] [Google Scholar]
- 47.Juric D, Hamilton E, Garcia-Estevez L, De Boer R, Mayer I, Campone M, et al. Phase Ib/II study of LEE011 and alpelisib (BYL719) and letrozole in ER+, HER2–breast cancer: Safety, preliminary efficacy and molecular analysis. Cancer Res. 2014;75(9 suppl) Abstract P5-19-24. [Google Scholar]
- 48.Burris H, Chan A, Campone M, Blackwell K, Winer E, Janni W, et al. First-line ribociclib + letrozole in patients with HR+, HER2− advanced breast cancer (ABC) presenting with visceral metastases or bone-only disease: A subgroup analysis of the MONALEESA-2 trial. San Antonio Breast Cancer Symposium; 2016. Poster P4-22-16. [Google Scholar]
- 49.O’Shaughnessy J, Petrakova K, Sonke G, André F, Conte P, Arteaga C, et al. First-line ribociclib plus letrozole in patients with de novo HR+, HER2− ABC: A subgroup analysis of the MONALEESA-2 trial. San Antonio Breast Cancer Symposium; 2016. Poster P4-22-05. [Google Scholar]
- 50.Andre F, Stemmer S, Hortobagyi G, Burris H, Shimon S, Campone M, et al. Ribociclib + letrozole for first-line treatment of HR+, HER2− ABC: Efficacy, safety, and pharmacokinetics. EORTC-NCI-AACR International Conference on Molecular Targets and Cancer Therapeutics; 2016. Abstract 12LBA. [Google Scholar]
- 51.Juric D, Ismail-Khan R, Campone M, García-Estévez L, Becerra C, De Boer R, et al. Phase Ib study of ribociclib and alpelisib and letrozole in ER+, HER2− advanced breast cancer: Safety, preliminary efficacy, and molecular analysis. Cancer Res. 2016;76(4 suppl) Abstract P3-14-01. [Google Scholar]
- 52.Bardia A, Modi S, Oliveira M, Campone M, Ma B, Dirix L, et al. Triplet therapy with ribociclib, everolimus, and exemestane in postmenopausal women with HR+/HER2− advanced breast cancer. Cancer Res. 2016;76(4 suppl) doi: 10.1158/1078-0432.CCR-20-1068. Abstract P6-13-01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cancer Genome Atlas Network. Genomic classification of cutaneous melanoma. Cell. 2015;161:1681–96. doi: 10.1016/j.cell.2015.05.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Rajkumar S, Watson IR. Molecular characterisation of cutaneous melanoma: Creating a framework for targeted and immune therapies. Br J Cancer. 2016;115:145–55. doi: 10.1038/bjc.2016.195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Maelandsmo GM, Flørenes VA, Hovig E, Øyjord T, Engebraaten O, Holm R, et al. Involvement of the pRb/p16/cdk4/cyclin D1 pathway in the tumorigenesis of sporadic malignant melanomas. Br J Cancer. 1996;73:909–16. doi: 10.1038/bjc.1996.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hodis E, Watson IR, Kryukov GV, Arold ST, Imielinski M, Theurillat JP, et al. A landscape of driver mutations in melanoma. Cell. 2012;150:251–63. doi: 10.1016/j.cell.2012.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Smalley K, McArthur G. The current state of targeted therapy in melanoma: This time it’s personal. Semin Oncol. 2012;39:204–14. doi: 10.1053/j.seminoncol.2012.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Potrony M, Badenas C, Aguilera P, Puig-Butille JA, Carrera C, Malvehy J, et al. Update in genetic susceptibility in melanoma. Ann Transl Med. 2015;3:210. doi: 10.3978/j.issn.2305-5839.2015.08.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Nathanson K, Martin A, Wubbenhorst B, Grescock J, Letrero R, D’Andrea K, et al. Tumor genetic analyses of patients with metastatic melanoma treated with the BRAF inhibitor dabrafenib (GSK2118436) Clin Cancer Res. 2013;19:4868–78. doi: 10.1158/1078-0432.CCR-13-0827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.National comprehensive cancer network guidelines. [Accessed December 2016];melanoma version 1.2017. Available from: https://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf.
- 61.Taylor M, Sosman J, Gonzalez R, Carlino M, Kittaneh M, Lolkema M, et al. Phase Ib/II study of LEE011 (CDK4/6 inhibitor) and LGX818 (BRAF inhibitor) in BRAF-mutant melanoma. Ann Oncol. 2014;25(suppl 4) Abstract 10860. [Google Scholar]
- 62.Sosman J, Kittaneh M, Lolkema M, Postow M, Schwartz G, Franklin C, et al. A phase 1b/2 study of LEE011 in combination with binimetinib (MEK162) in patients with NRAS-mutant melanoma: Early encouraging clinical activity. J Clin Oncol. 2014;32(5s suppl) Abstract 9009. [Google Scholar]
- 63. [Accessed December 2016];Array BioPharma and pierre fabre announce COLUMBUS phase 3 study of encorafenib plus binimetinib for BRAF-mutant melanoma met primary endpoint. Available from: http://www.prnewswire.com/news-releases/array-biopharma-and-pierre-fabre-announce-columbus-phase-3-study-of-encorafenib-plus-binimetinib-for-braf-mutant-melanoma-met-primary-endpoint-300333794.html.
- 64.Wellmann A, Doseeva V, Butscher W, Raffeld M, Fukushima P, Stetler-Stevenson M, et al. The activated anaplastic lymphoma kinase increases cellular proliferation and oncogene up-regulation in rat 1a fibroblasts. FASEB J. 1997;11:965–72. doi: 10.1096/fasebj.11.12.9337149. [DOI] [PubMed] [Google Scholar]
- 65.Molenaar JJ, Ebus ME, Koster J, van Sluis P, van Noesel CJ, Versteeg R, et al. Cyclin D1 and CDK4 activity contribute to the undifferentiated phenotype in neuroblastoma. Cancer Res. 2008;68:2599–609. doi: 10.1158/0008-5472.CAN-07-5032. [DOI] [PubMed] [Google Scholar]
- 66.Molenaar JJ, Koster J, Ebus ME, van Sluis P, Westerhout EM, de Preter K, et al. Copy number defects of G1-cell cycle genes in neuroblastoma are frequent and correlate with high expression of E2F target genes and a poor prognosis. Genes Chromosomes Cancer. 2012;51:10–9. doi: 10.1002/gcc.20926. [DOI] [PubMed] [Google Scholar]
- 67.Rader J, Russell MR, Hart LS, Nakazawa MS, Belcastro LT, Martinez D, et al. Dual CDK4/CDK6 inhibition induces cell-cycle arrest and senescence in neuroblastoma. Clin Cancer Res. 2013;19:6173–82. doi: 10.1158/1078-0432.CCR-13-1675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Geoerger B, Bourdeaut F, Dubois SG, Dewire MD, Marabelle A, Pearson AD, et al. Phase I study of LEE011 (CDK4/6 inhibitor) in patients with malignant rhabdoid tumors, neuroblastoma, and cyclin D–CDK4/6 pathway-activated tumors. Ann Oncol. 2014;25(4 suppl) Abstract 455P. [Google Scholar]
- 69.Bhansali S, Parasuraman S, Matano A, Davis C, Chakraborty A. Pharmacokinetics of LEE011, a CDK4/6 inhibitor, in adult and pediatric patients. American College of Clinical Pharmacy. 2014 Poster 1-10-2000545. [Google Scholar]
- 70.Sherr CJ, Beach D, Shapiro GI. Targeting CDK4 and CDK6: From discovery to therapy. Cancer Discov. 2016;6:353–67. doi: 10.1158/2159-8290.CD-15-0894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Flaherty KT, Lorusso PM, Demichele A, Abramson VG, Courtney R, Randolph SS, et al. Phase I, dose-escalation trial of the oral cyclin-dependent kinase 4/6 inhibitor PD 0332991, administered using a 21-day schedule in patients with advanced cancer. Clin Cancer Res. 2012;18:568–76. doi: 10.1158/1078-0432.CCR-11-0509. [DOI] [PubMed] [Google Scholar]
- 72.Raub TJ, Wishart GN, Kulanthaivel P, Staton BA, Ajamie RT, Sawada GA, Gelbert LM, Shannon HE, Sanchez-Martinez C, De Dios A. Brain exposure of two selective dual CDK4 and CDK6 inhibitors and the antitumor activity of CDK4 and CDK6 inhibition in combination with temozolomide in an intracranial glioblastoma xenograft. Drug Metab Dispos. 2015;43:1360–71. doi: 10.1124/dmd.114.062745. [DOI] [PubMed] [Google Scholar]
- 73.Patel Y, Davis A, Kala A, Roberts J, Jacus M. CNS penetration of the CDK4/6 inhibitor ribociclib (LEE011) in non-tumor bearing mice and mice bearing orthotopic pediatric brain tumors. Neuro Oncol. 2016;18(suppl 6) Abstract PDTB-12. [Google Scholar]
- 74.Finn RS, Crown JP, Lang I, Boer K, Bondarenko IM, Kulyk SO, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): A randomised phase 2 study. Lancet Oncol. 2015;16:25–35. doi: 10.1016/S1470-2045(14)71159-3. [DOI] [PubMed] [Google Scholar]
- 75.DeMichele A, Clark AS, Tan KS, Heitjan DF, Gramlich K, Gallagher M, et al. CDK4/6 inhibitor palbociclib (PD0332991) in rb+ advanced breast cancer: Phase II activity, safety, and predictive biomarker assessment. Clin Cancer Res. 2015;21:995–1001. doi: 10.1158/1078-0432.CCR-14-2258. [DOI] [PubMed] [Google Scholar]
- 76.Leonard JP, LaCasce AS, Smith MR, Noy A, Chirieac LR, Rodig SJ, et al. Selective CDK4/6 inhibition with tumor responses by PD0332991 in patients with mantle cell lymphoma. Blood. 2012;119:4597–607. doi: 10.1182/blood-2011-10-388298. [DOI] [PubMed] [Google Scholar]
- 77.Dickson MA, Tap WD, Keohan ML, D’Angelo SP, Gounder MM, Antonescu CR, et al. Phase II trial of the CDK4 inhibitor PD0332991 in patients with advanced CDK4-amplified well-differentiated or dedifferentiated liposarcoma. J Clin Oncol. 2013;31:2024–8. doi: 10.1200/JCO.2012.46.5476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Gopalan P, Pinder M, Chiappori A, Ivey A, Villegas A, Kaye F. A phase II clinical trial of the CDK 4/6 inhibitor palbociclib (PD 0332991) in previously treated, advanced non-small cell lung cancer (NSCLC) patients with inactivated CDKN2A. J Clin Oncol. 2014;32(5s suppl) Abstract 8077. [Google Scholar]
- 79.Patnaik A, Rosen L, Tolaney S, Tolcher A, Goldman J, Gandhi L, et al. Efficacy and safety of abemaciclib, an inhibitor of CDK4 and CDK6, for patients with breast cancer, non-small cell lung cancer, and other solid tumors. Cancer Discov. 2016;6:740–53. doi: 10.1158/2159-8290.CD-16-0095. [DOI] [PubMed] [Google Scholar]
- 80.Fujiwara Y, Tamura K, Kondo S, Tanabe Y, Iwasa S, Simomura A, et al. Phase I study of abemaciclib, an inhibitor of CDk4 and 6, as a single agent for Japanese patients with advanced cancer. Cancer Chemother Pharmacol. 2016;78:281–8. doi: 10.1007/s00280-016-3085-8. [DOI] [PubMed] [Google Scholar]
- 81.Beeram M, Tolaney S, Beck J, Dickler M, Conlin A, Dees E, et al. A phase 1b study of abemaciclib in combination with endocrine and HER2-targeted therapies for patients with metastatic breast cancer. Annals of Oncology. 2016;27(Supplement 6):vi552–vi587. Abstract LBA18 (Poster LBA774) [Google Scholar]
- 82.Malumbres M, Barbacid M. Cell cycle, CDKs and cancer: A changing paradigm. Nat Rev Cancer. 2009;9:153–66. doi: 10.1038/nrc2602. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.