

Abstract
Rationale:
Povidone-iodine is a broad-spectrum antiseptic applied topically to treat wounds and prevent their infection. There have been several case reports of acute kidney injury (AKI) in burn patients after povidone-iodine irrigation and in patients receiving the substance as a sclerotherapy agent for management of lymphocele after renal transplantation. However, biopsy-confirmed AKI after ingestion of povidone-iodine has not previously been described.
Patient concerns:
A 47-year-old man who had apparently ingested povidone-iodine solution and presented with nausea, vomiting, and reduced urine output. Laboratory data revealed blood urea nitrogen of 124 mg/dL, serum creatinine of 6.3 mg/dL, impaired liver function, and leukocytosis. Urine iodine/creatinine ratio was markedly elevated.
Diagnoses:
Acute tubular necrosis and interstitial nephritis secondary to povidone-iodine ingestion.
Interventions:
The patient was admitted to the intensive care unit and underwent continuous venovenous hemodiafiltration. Kidney biopsy showed acute tubular necrosis and interstitial nephritis. Unstained sections showed tan objects in the tubular lumina that were suspected to be povidone-iodine casts. Corticosteroid therapy (1 mg/kg/day) was started after kidney biopsy.
Outcomes:
Renal function recovered after hemodialysis and corticosteroid medication, but not completely.
Lessons:
We have reported the first case of biopsy-confirmed AKI accompanied by increased urine iodine concentration following povidone-iodine ingestion.
Keywords: acute kidney injury, biopsy, povidone-iodine, steroid
1. Introduction
Povidone-iodine is a broad-spectrum antiseptic applied topically to treat wounds and prevent their infection. Its active ingredient, iodine is effective against yeasts, molds, fungi, viruses, and protozoans; in the form of the H2OI+ cation, it also acts against bacteria by breaking down their cell membrane proteins.[1] Consequently, povidone-iodine is widely used as a surgical scrub, for preoperative and postoperative skin cleansing, and for the treatment of wound infections and burns. It can also be used in pleurodesis for malignant pleural effusions, in percutaneous transcatheter sclerotherapy of lymphoceles occurring after kidney transplantation (a well-known surgical complication), and as a contrast agent. However, several cases have been reported of acute kidney injury (AKI) due to iodine toxicity. In one case, AKI developed in a patient who attempted suicide by ingesting iodine tincture.[2] AKI has also been recorded in a patient who underwent hysteroscopy for diagnosis of primary sterility using povidone-iodine as the contrast agent,[3] in burn patients treated topically with povidone-iodine,[4,5] in a kidney allograft recipient with recurrent lymphoceles treated with povidone-iodine instillations,[6] and in patients undergoing mediastinal irrigation with povidone-iodine.[7,8] Some cases were accompanied by increased serum iodine concentration. However, biopsy-confirmed AKI following ingestion of povidone-iodine has not previously been described. Herein, we report a case of severe AKI that occurred after ingestion of povidone-iodine and was accompanied by elevated urine iodine concentration. The authors obtained approval from the institutional review board of Chonnam National University Hospital, South Korea (CNUH-EXP-2017-275), and informed consent was waived by the institutional review board.
2. Case presentation
A 47-year-old man with a hearing impairment presented to the emergency department with nausea, vomiting, general weakness, and reduced urine output. The patient had been suffering from depressive episodes for about 1 month. One day before visiting our hospital, he had apparently ingested a 10% povidone-iodine solution. On physical examination, he was found to have pitting edema of the lower extremities, but his tongue was not dry. On admission, his pulse was 110 beats/min and his blood pressure was 140/90 mm Hg. Echocardiography showed sinus tachycardia. Laboratory data revealed a white blood cell count of 37 × 109/L, hemoglobin of 9.8 g/dL, blood urea nitrogen of 124 mg/dL, serum creatinine of 6.3 mg/dL, serum sodium of 138 mEq/L, impaired liver function (aspartate transaminase 213 U/L, alanine transaminase 33 U/L), lactic dehydrogenase of 4939 U/L, creatine kinase of 449 U/L, γ-glutamyl transpeptidase of 9 U/L, and amylase of 206 U/L. Arterial blood gas analysis revealed a pH of 7.44, a pCO2 of 31.3 mm Hg, a pO2 of 76.7 mm Hg, HCO3- levels of 20.8 mmol/L, and 95.2% O2 saturation. Ultrasound examination revealed increased size of both kidneys and prominent medullary hypoechogenicity, compatible with a diagnosis of AKI. The patient was admitted to the intensive care unit, where we performed hemodiafiltration and kidney biopsy. Unstained and hematoxylin-stained sections showed tan objects in the renal tubules, which were putatively identified as povidone-iodine casts (Fig. 1). Periodic acid–Schiff staining revealed tubular cell flattening, various types of casts in the distal tubules, and interstitial infiltration of neutrophils and lymphocytes, but the glomeruli and vessels appeared unremarkable (Fig. 2). Findings on immunofluorescence staining and electron microscopy were also unremarkable. Urine iodine/creatinine ratio was elevated at 233,126 μg iodine/g creatinine (reference range 45–2922 μg/g). These findings were consistent with acute tubular necrosis and interstitial nephritis secondary to povidone-iodine ingestion. Over time, urine output improved, but serum creatinine level had increased to 9.6 mg/dL. Corticosteroid therapy (1 mg/kg/day) was started at that time. At discharge, the patient's serum creatinine levels had fallen to 4.2 mg/dL and urine iodine/creatinine ratio had decreased to 511 μg iodine/g creatinine. Four months after discharge, the patient's serum creatinine had dropped further to 1.9 mg/dL, although he had not completely recovered (Fig. 3).
Figure 1.
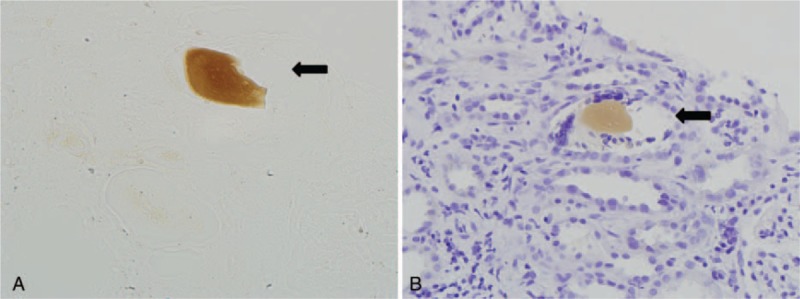
Unstained (A) and hematoxylin-stained (B) kidney biopsy sections showed tan objects in the tubular lumina in a homogeneous pattern (arrow); they were suspected to be povidone-iodine casts (original magnification 400×).
Figure 2.
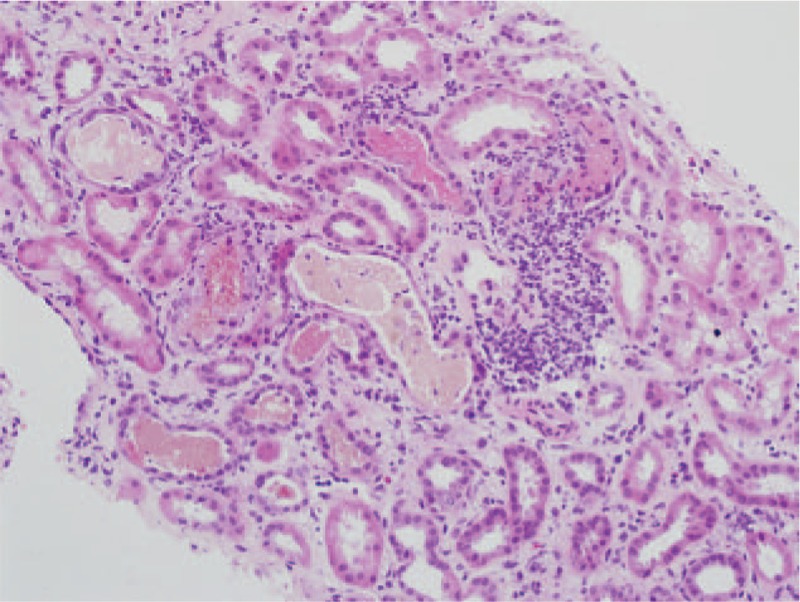
Kidney section showing tubular atrophy, various casts (erythrocyte, leukocyte, and epithelial cell casts) in the distal tubules, and inflammatory cell infiltration in the interstitium (periodic acid–Schiff stain; original magnification 200×).
Figure 3.
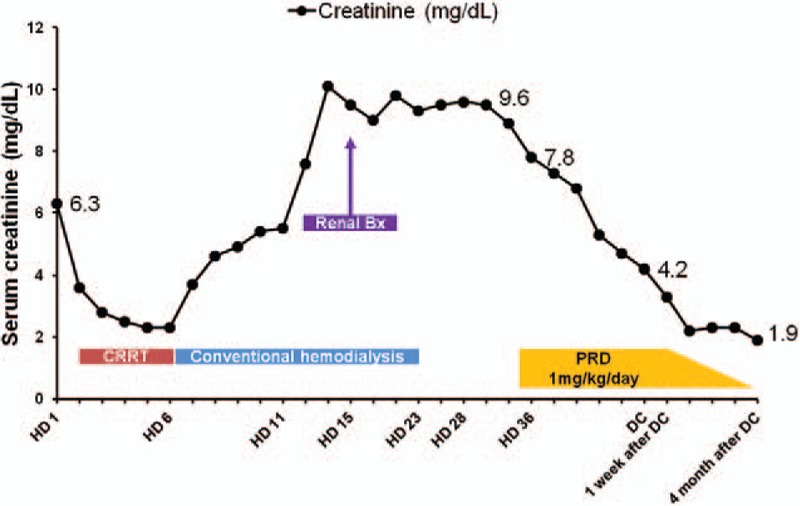
Serial change of serum creatinine during follow-up period. CRRT = continuous renal replacement therapy, Bx = biopsy, DC = discharge, HD = hospital day, PRD = prednisolone.
3. Discussion
Povidone-iodine is a widely used and generally safe antiseptic, sclerotherapy, and contrast agent. However, its absorption into the systemic circulation (e.g., through damaged skin in burn patients or as a result of internal administration for treatment of lymphocele after renal transplantation[5,6]) may lead to toxicity. Povidone-iodine toxicity is generally indicated by increased serum iodine level and usually manifests as AKI, often in the form of tubular necrosis. Indeed, a recent experimental study showed that povidone-iodine exposure induced time- and concentration-dependent apoptosis and necrosis in cultured human epithelial cells and rat oral mucosal tissue.[9] AKI may be accompanied by metabolic acidosis, anemia, or hypernatremia[2,6,10,11]; our patient presented with AKI and anemia, but showed no definite metabolic acidosis or hypernatremia.
In literature, there are only one report about ingestion of iodine tincture led to increase of aspartate aminotransferase 545 U/L, alanine transaminase 51 U/L and lactic dehydrogenase of 5563 U/L, which are similar to our case.[2] Pattern of elevated aspartate aminotransferase compared with alanine transaminase accompanied with increased lactic dehydrogenase might be supposed to be a nonspecific liver injury due to iodine toxicity. Also, in our case, creatine kinase was increased on admission, but γ-glutamyl transpeptidase was reported to be normal. Although it is difficult to exclude from rhabdomyolysis, liver injury caused by alcohol could be ruled out in this case.
A remarkable thing about our case is that unstained and hematoxylin-stained sections showed tan casts in the tubular lumina in a homogeneous pattern. These casts were differentiated from lipofuscin, myoglobin, and hemoglobin casts by their lack of pigment and were putatively identified as iodine casts. Unfortunately, to the best of our knowledge, there is no proven method for confirming such identification. Therefore, while formation of iodine casts in the renal tubules is a plausible etiology for our case, further studies are necessary to better establish the pathogenesis and characteristics of povidone-iodine-induced AKI.
In several previous cases of iodine toxicity, hemodialysis and hydration were sufficient to reduce serum iodine concentration and produce a favorable renal outcome.[3,5,6] Unlike previous patients, our patient had acute interstitial nephritis as well as acute tubular necrosis, so corticosteroid therapy was used to treat the nephritis and succeeded in reducing serum creatinine. Although no specific treatment for iodine toxicity is available, reversible recovery from AKI may be induced through hemodialysis and/or corticosteroid therapy as deemed appropriate based on kidney biopsy findings.
In conclusion, we have reported the first case of biopsy-confirmed acute tubular necrosis and interstitial nephritis after povidone-iodine ingestion. Increased urine iodine concentration and tan casts in the renal tubules may be helpful diagnostic characteristics of such cases. Our patient partially recovered from AKI through hemodialysis and corticosteroid treatment, which were carried out based on kidney biopsy results of acute interstitial nephritis. Therefore, we recommend kidney biopsy as a useful tool for diagnosing povidone-iodine toxicity and guiding treatment.
Footnotes
Abbreviation: AKI = acute kidney injury.
Funding: This study was supported by the National Research Foundation of Korea funded by the Ministry of Science, ICT & Future Planning (2015R1C1A1A01051769), by the Bio & Medical Technology Development Program of the NRF funded by the Korean government, MSIP (2017M3A9E8023001), and by a grant (HCRI17901-21) Chonnam National University Hwasun Hospital Institute for Biomedical Science.
The authors have no conflicts of interest to disclose.
References
- [1].Hsu YC, Nomura S, Kruse CW. Some bactericidal and virucidal properties of iodine not affecting infectious RNA and DNA. Am J Epidemiol 1965;82:317–28. [DOI] [PubMed] [Google Scholar]
- [2].Mao YC, Tsai WJ, Wu ML, et al. Acute hemolysis following iodine tincture ingestion. Hum Exp Toxicol 2011;30:1716–9. [DOI] [PubMed] [Google Scholar]
- [3].Beji S, Kaaroud H, Ben Moussa F, et al. [Acute renal failure following mucosal administration of povidone iodine]. Presse Med 2006;35(1 Pt 1):61–3. [DOI] [PubMed] [Google Scholar]
- [4].Lavelle KJ, Doedens DJ, Kleit SA, et al. Iodine absorption in burn patients treated topically with povidone-iodine. Clin Pharmacol Ther 1975;17:355–62. [DOI] [PubMed] [Google Scholar]
- [5].Pietsch J, Meakins JL. Complications of povidone-iodine absorption in topically treated burn patients. Lancet 1976;1:280–2. [DOI] [PubMed] [Google Scholar]
- [6].Manfro RC, Comerlato L, Berdichevski RH, et al. Nephrotoxic acute renal failure in a renal transplant patient with recurrent lymphocele treated with povidone-iodine irrigation. Am J Kidney Dis 2002;40:655–7. [DOI] [PubMed] [Google Scholar]
- [7].Campistol JM, Abad C, Nogue S, et al. Acute renal failure in a patient treated by continuous povidone-iodine mediastinal irrigation. J Cardiovasc Surg (Torino) 1988;29:410–2. [PubMed] [Google Scholar]
- [8].Ryan M, Al-Sammak Z, Phelan D. Povidone-iodine mediastinal irrigation: a cause of acute renal failure. J Cardiothorac Vasc Anesth 1999;13:729–31. [DOI] [PubMed] [Google Scholar]
- [9].Sato S, Miyake M, Hazama A, et al. Povidone-iodine-induced cell death in cultured human epithelial HeLa cells and rat oral mucosal tissue. Drug Chem Toxicol 2014;37:268–75. [DOI] [PubMed] [Google Scholar]
- [10].Moudden MK, Labaye J, Sarret D, et al. [Acute renal failure following internal administration of povidone iodine: a case report]. Rev Med Interne 2007;28:556–8. [DOI] [PubMed] [Google Scholar]
- [11].Hunt JL, Sato R, Heck EL, et al. A critical evaluation of povidone-iodine absorption in thermally injured patients. J Trauma 1980;20:127–9. [DOI] [PubMed] [Google Scholar]