

Abstract
Alcohol consumption among secondary school students is a major public health issue worldwide; however, the extent of consumption among secondary school students and their understanding of its effects on human health remain relatively unknown in many Nigerian States. This study aimed to determine the extent of alcohol consumption and of the awareness of its negative effects on human health among secondary school students.
The study used a cross-sectional survey design. Self-report questionnaire developed by the researchers was administered to representative sample (N = 1302) of secondary school students in the study area. The data collected from the respondents were analyzed using means and t test.
The results showed that male secondary school students moderately consumed beer (55.2%) and local cocktails (51.5%), whereas their female counterparts reported rare consumption of these 2 alcoholic drinks (44.8%; 48.5% respectively). The findings also indicated rare consumption of distilled spirits among both male and female students in the investigated area, whereas wine, liquor, local spirits, and palm wine were consumed moderately, regardless of gender. Finally, male and female secondary school students differed significantly in their awareness of the negative effects of alcohol consumption on health.
There is a need to intensify efforts to further curtail the extent of alcohol consumption and increase awareness of the negative effects of alcohol use on human health among secondary school students.
Keywords: alcohol, consumption, health, Nigeria, secondary school, students
1. Introduction
Alcohol consumption is a serious public health challenge worldwide, including in Nigeria. Although the level of alcohol consumption differs widely around the world, the burden of disease and death remains significant in most regions, with Europe and America having the highest alcohol attributable fractions at 6.5% and 5.6%, respectively.[1] Recent evidence also indicates that alcohol consumption is now the world's third largest risk factor for disease and disability; almost 4% of all deaths globally are attributed to alcohol.[2] However, alcohol is the most commonly used psychoactive drug in both young people and adults in Nigeria.[3–5] Some of the factors contributing to alcohol consumption among Nigerians include the absence of alcohol policies, easy access to alcoholic drinks, and lack of implementation of a minimum drinking age by both the government and the brewers.[6]
According to Bada and Adebiyi,[7] it is not rare for Nigerian secondary school students to consume alcoholic drinks; this consumption could be due to their curiosity as adolescents, an irresistible urge, emotional disturbances such as anxiety, the subculture, and the influence of advertisements. Several previous studies have shown the prevalence of alcohol consumption among the Nigerian population, but they did not explore adolescent students’ understanding of its negative health effects. For instance, Lasebikan and Ola[8] found that the prevalence of lifetime alcohol use was 57.9% and that of current alcohol use was 27.3% among a sample of Nigerian semirural community dwellers. Through in-person interviews with Nigerian adults, previous research by Gureje et al[3] revealed that the lifetime prevalence of alcohol consumption was 56%. A recent study by Alex-Hart et al[9] showed that the prevalence of current alcohol consumption among a sample of Nigerian secondary school students was 30.6% and that 38.1% of current drinkers had also been drunk in the past 30 days, with 17.2% being drunk very frequently.
Alcohol consumption negatively affects human health across the lifespan. Previous studies show that alcohol consumption is associated with a burden of diseases such as cancer,[10] pancreatitis, liver cirrhosis, tuberculosis, pneumonia, diabetes mellitus, alcohol use disorder, malignancies, psychiatric morbidity, and injury.[11] Although 18 years of age is the legal limit for alcohol consumption per policy in many parts of the world, sociocultural influences[12,13] seem to hinder strict adherence to this public health policy in Nigerian society. The objective of the present study was therefore to investigate the level of alcohol consumption and knowledge of its negative effects on health among secondary school students in Nigeria. Specifically, the study sought to determine the responses of secondary school students regarding the extent of their alcohol consumption and the extent to which students are aware of the negative health effects of alcohol consumption.
2. Methods
2.1. Ethical consideration
Ethical committee approval was obtained by the authors for this study (Ethical Approval Number: VTE/ERA/0023). Furthermore, parents of the selected participants signed an informed consent form to indicate their approval. School principals of the selected students provided informed consent and conveyed their approval to the researchers in writing. Participants were informed that they were free to participate or to decline participation in the study.
2.2. Study design
The current study adopted a cross-sectional survey design.
2.3. Study setting
This study was conducted in public secondary schools in Ebonyi and Enugu States, Nigeria.
2.4. Study participants
The participants comprised 1302 senior secondary school students who were purposively selected to participate in the study. The study sample size was determined using G∗Power 3.1 software[14,15] based on a statistical power of 0.95. Brown[16] stated that if the observed statistical power is large enough (≥0.80), the sample size can be considered adequate for the study. Figure 1 shows the results of the sample size determination. Table 1 summarizes the characteristics of the participants.
Figure 1.
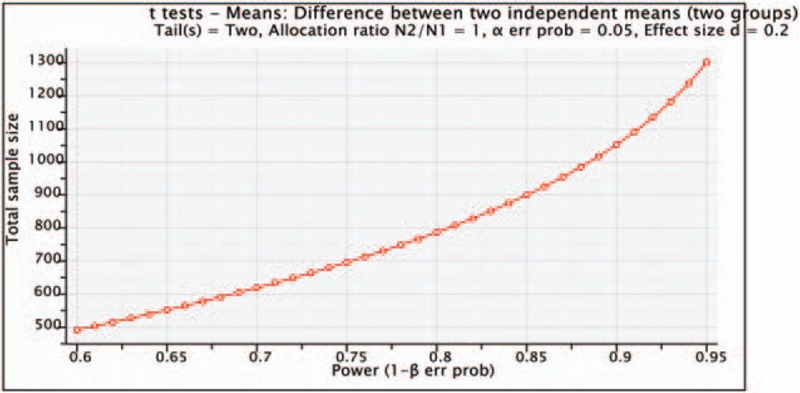
Sample size determination using G∗power software.
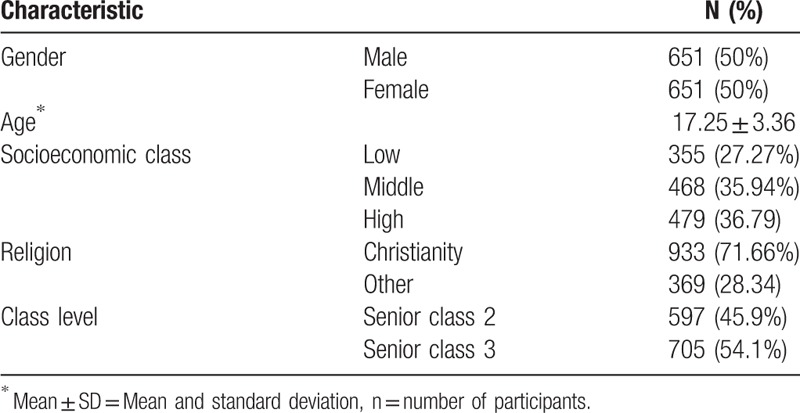
Table 1.
Demographic characteristics of the participants.
2.5. Assumptions about the sample size calculations
We conducted an a priori analysis to determine the study sample size based on the assumptions that a required sample size can be computed as a function of user-specified values for the required significance level α, the desired statistical power 1–β, and the to-be-detected population effect size.[14,15,17,] According to Uzoagulu,[18] researchers should endeavor to make use of statistical technique to determine sample size, and should be aware that the fewer a sample size is, the greater the possibility of sampling error. Thus, the assumptions underlying the use of a priori analysis for sample size calculations were considered appropriate for the current study.
2.6. Sampling strategy
Before sampling, the researchers and assistants purposively visited 40 secondary schools each in the surveyed States to seek for the school principals’ approval, and to explain to them the purpose of the study, and possibility of being included or excluded from the study later on due to certain criteria. All the school principals visited gave their informed consent, and their schools were therefore qualified for sampling. Through multistage sampling technique, the researchers selected the current study sample. First, the simple random sampling technique (balloting without replacement) was used to select only 31 school secondary schools from each State, making a total of 62 secondary schools surveyed. This technique was used in order to give each of the secondary schools the opportunity of being selected and thus eliminate selection bias. Furthermore, 21 senior students from each of the selected schools in the 2 States were selected to participate in the study through stratified random sampling. The samples were stratified by gender (male, n = 651, 50%; female, n = 651, 50%) and other demographics as summarized in Table 1. Both the schools and their students were selected on the basis of certain inclusion criteria set by the researchers.
2.7. Inclusion and exclusion criteria
The inclusion criteria included that the school principal must provide informed consent in writing; the respondent (student) must be in senior secondary school class two or three, agree to participate freely, inform their parents/guardians about the study, and provide a letter of consent from them. A participant must also be at least 16 years of age and above. Those who did not meet these criteria were excluded from the current study.
2.8. Measures
The Alcoholic Drinks Consumption Questionnaire for Secondary School Students (ADCQSSS) is a structured questionnaire developed by the researchers based on previous literature.[2,8,19] The ADCQSSS consists of 22 items divided into 2 major sections (A and B). Section A assesses respondents’ personal data (age, gender, religion, socioeconomic background, and educational class level). Section B has 2 parts; part one contains 7 items that evaluate the extent to which students consume alcohol with regard to a variety of alcoholic drinks (i.e., Beer, Distilled Spirits, Wine, Liquor, Local Spirits, Local Cocktails, and Palm Wine), and part two contains 15 items that ask respondents about their awareness of the negative effects of alcoholic drinks on human health. The ADCQHSS has a 5-point rating scale from Do not consume/Not aware (0) to Highly Consume/Extremely aware (4). The ADCQSSS was validated by 2 experts in Home Economics and Hospitality Management Education and 2 other independent experts in Educational Research, Measurement, and Evaluation. Cronbach alpha reliability coefficient of the ADCQSSS was 0.72 for part one, 0.76 for part two, and 0.85 for the entire scale, based on data from the current study sample.
2.9. Data collection
To overcome the challenges of participant attrition and nonretrieval of instruments, which are common to many cross-sectional surveys, the questionnaires were distributed and retrieved from each respondent on the spot with the help of 4 research assistants. Respondents met with the researchers and assistants in school halls to complete the questionnaire during long break periods in school. The respondents were guided appropriately and given sufficient time (15–20 minutes) to avoid incomplete responses. Respondents were encouraged to call the attention of any of the researchers or assistants if they need additional clarification on any item or how to complete the questionnaire. Given these measure, responses and return rates were 100%.
2.10. Data entry, management procedure, and analysis
The data collected from the respondents were analyzed using means, percentage, and t test. Item scores were included as the dependent variables and sex as the independent variables. Using purposively determined mean benchmark values, the item scores for the first part of the ADCQHSS section B (the extent to which students consumed alcoholic drinks) were interpreted as follows: Highly Consume (HC) = 3.50 to 4.00; Moderately Consume (MC) = 3.00 to 3.49; Rarely Consume (RC) = 2.50 to 2.99; and Does Not Consume (DNC) = 1.00 to 2.49. Using similarly purposively set mean benchmark values, the item scores for the second part of the ADCQHSS section B (awareness of the negative effects of alcoholic drinks on health) were interpreted as follows: Extremely Aware (EA) = 3.50 to 4.00; Moderately Aware (MA) = 3.00 to 3.49; Slightly Aware (SA) = 2.50 to 2.99; and Not Aware (NA) = 1.00 to 2.49. The t test was used to examine the differences between male and female students at a 0.05 level of significance. To perform the t tests, item scores were treated as test variables, whereas sex was used as the grouping variable. During coding, the numerical value of 1 was used as the label for male students, whereas the value of 2 was applied for female students. Before performing the t tests, the normality of the distribution of the data was assessed using Shapiro–Wilks normality test. The data were found to be normally distributed (P = .95). Furthermore, we described the percentage (%) of students scoring below or above given thresholds (seeTables 2 and 3). A database created from Microsoft Excel was used for data management, which involved compiling, organizing, defining, and managing data. Thereafter, the statistical software used for analysis was the Statistical Package for the Social Sciences (SPSS) version 21 (IBM Corp., Chicago, IL).[20] To assure quality, we checked for missing data and violation of assumptions using the IBM SPSS statistical software. There were no missing data.
Table 2.
Means, percentages, and t tests of Students responses on the extent of alcoholic drink consumption.
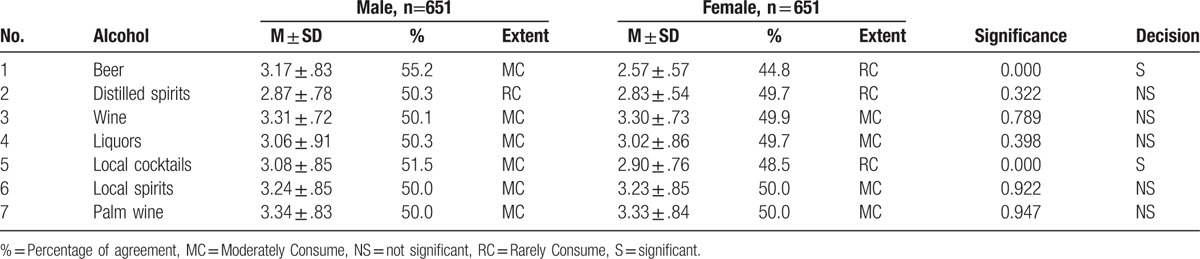
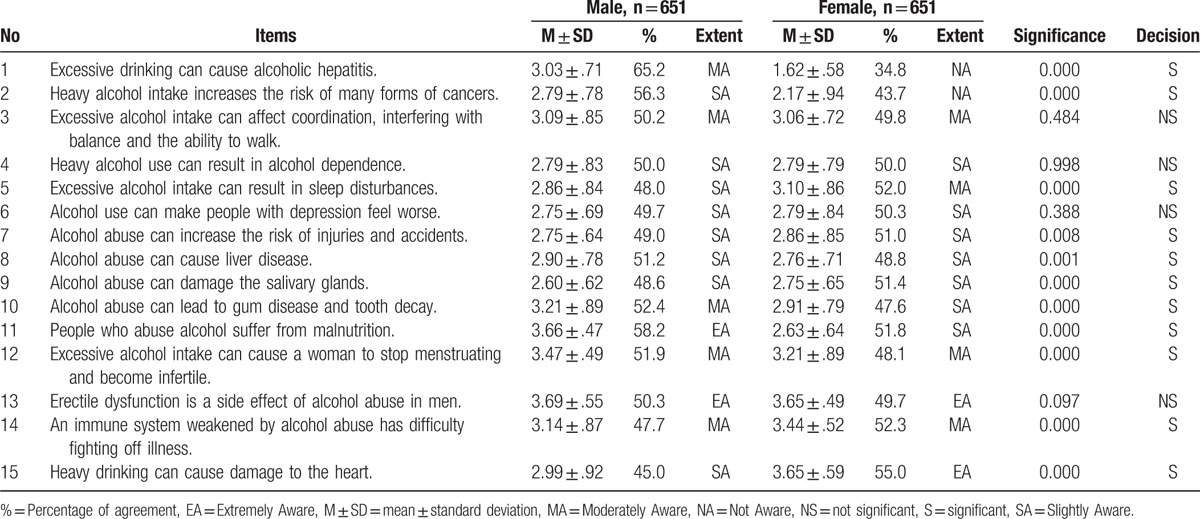
Table 3.
Means, percentages, and t tests of the extent to which students are aware of the negative effects of alcohol consumption on human health.
3. Results
The results in Table 2 reveal the extent of participants’ consumption of alcoholic drinks by gender. Male secondary school students (55.2%) in this study reported moderate consumption of beer (M ± SD = 3.17 ± .83), while females (44.8%) reported rare consumption of beer (2.57 ± .57). In addition, distilled spirits (male=50.3%; female=49.7%) were rarely consumed by both genders, whereas wine, liquors, local spirits, and palm wine were moderately consumed by both (see Table 2). These results imply that secondary school students in the study area consumed different types of alcoholic beverages. In addition, the results in Table 2 reveal a significant difference between male and female students in their extent of consumption of beer [t = -15.25, P = .000, 95% confidence interval (95% CI) -0.676 to 0.522] and local cocktails (t = -3.92, P = .000, 95% CI -0.263 to -0.088) at 1300 degrees of freedom, as the corresponding P values were lower than the chosen level of significance (.05). This finding means that male and female students in the investigated area consumed these alcoholic drinks unequally due to gender. Male secondary school students moderately consumed beer and local cocktails, whereas their female counterparts were rare consumers of these 2 alcoholic drinks (see Table 2).
Furthermore, the results in Table 2 reveal nonsignificant differences between male and female students in the extent to which they consume distilled spirits (t = -0.991, P = .322, 95% CI -0.109 to 0.036], wine (t = -0.268, P = .789, 95% CI -0.089 to 0.068), liquor (t = -0.846, P = .398, 95% CI -0.138 to 0.055), local spirits (t = -0.098, P = .922, 95% CI -0.097 to 0.088), and palm wine (t = -0.066, P = .947, 95% CI -0.094 to 0.088), given that the P values for all t tests ranged from .32 to .95 at 1300 degrees of freedom and were therefore higher than the chosen level of significance (.05). This finding suggests that male and female students in the investigated area consumed these alcoholic drinks similarly regardless of gender (see Table 2).
Table 3 summarizes the extent to which students were aware of the negative effects of alcohol consumption on health. The results show that male and female students differed significantly in their awareness of the following negative effects of alcohol consumption on human health: excessive drinking can cause alcoholic hepatitis (t = 39.39, P = .000, 95% CI 1.347–1.488); heavy alcohol intake increases the risk of many forms of cancers (t = 12.92, P = .000, 95% CI 0.526–0.715); excessive alcohol intake can result in sleep disturbances (t = -5.01, P = .000, 95% CI -0.329 to 0.144); alcohol abuse can increase the risk of injuries and accidents (t = -2.65, P = .008, 95% CI -0.193 to 0.029); alcohol abuse can cause liver disease (t = 3.38, P = .001, 95% CI 0.059–0.221); alcohol abuse can damage the salivary glands (t = -4.14, P = .000, 95% CI -0.215–0.077); alcohol abuse can lead to gum disease and tooth decay (t = 6.23, P = .000, 95% CI 0.201–0.386); people who abuse alcohol suffer from malnutrition (t = 32.98, P = .000, 95% CI 0.972–1.095); excessive alcohol intake can cause a woman to stop menstruating and become infertile (t = 6.44, P = .000, 95% CI 0.179–0.337); an immune system weakened by alcohol abuse has difficulty fighting off illness (t = -7.66, P = .000, 95% CI -0.382 to 0.226); and heavy drinking can cause damage to the heart (t = -15.46, P = .000, 95% CI -0.748 to 0.579) (see Table 3).
Finally, the results in Table 3 further show that male and female students were similarly aware of the following effects of alcohol on human health, in that no significant differences were found: excessive alcohol intake can affect coordination, interfering with balance and the ability to walk (t = 0.70, P = .484, 95% CI -0.055 to 0.117); heavy alcohol use can result in alcohol dependence (t = 0.00, P = .998, 95% CI -0.088 to 0.088); alcohol use can make people with depression feel worse (t = -0.86, P = .388, 95% CI -0.121 to 0.047); and erectile dysfunction is a side effect of alcohol abuse in men (t = 1.66, P = .097, 95% CI -0.009 to 0.104) (see Table 3).
4. Discussion
The current study determined the extent of alcoholic drink consumption and of awareness of its negative effects on human health among secondary school students in Nigeria. First, our findings showed that male secondary school students moderately consume beer and local cocktails, whereas their female counterparts were rare consumers of these 2 alcoholic drinks. These findings support those of Lasebikan and Ola,[8] who found that current alcohol drinking was highly related to male gender. In addition, the current study showed that both male and female students in the investigated area rarely consumed distilled spirits, whereas wine, liquor, local spirits, and palm wine were consumed moderately by the students regardless of their gender. According to the authors, more than two-thirds of the current drinking population are moderate drinkers.[8] Bada and Adebiyi[7] noted that it is not difficult to identify Nigerian secondary school students who consume alcohol. Despite what literature might suggest as reasons for students’ alcohol consumption, Cox et al[21] indicate that negative reasons for alcohol consumption are stronger determinants of drinking problems than are positive reasons among both secondary-level school students. Sociocultural factors may also explain the reason for the differences as well as similarities on the extent of alcoholic drink consumption in Nigerian population.[12,13]
Furthermore, the present study showed that male and female secondary school students differed significantly in their awareness of the following negative effects of alcohol consumption on health: excessive drinking can cause alcoholic hepatitis; heavy alcohol intake increases the risk of many forms of cancers; excessive alcohol intake can result in sleep disturbances; alcohol abuse can increase the risk of injuries and accidents; alcohol abuse can cause liver disease; alcohol abuse can damage the salivary glands; alcohol abuse can lead to gum disease and tooth decay; people who abuse alcohol suffer from malnutrition; excessive alcohol intake can cause a woman to stop menstruating and become infertile; an immune system weakened by alcohol abuse has difficulty fighting off illness; and heavy drinking can cause damage to your heart. Finally, our findings also showed that male and female students had similar levels of awareness of the following effects of alcohol on human health, as no significant differences were found: excessive alcohol intake can affect coordination, interfering with balance and the ability to walk; heavy alcohol use can result in alcohol dependence; alcohol use can make people with depression feel worse; and erectile dysfunction is a side effect of alcohol abuse in men. These outcomes support previous studies,[1,9] which show that alcohol increases the risk of numerous diseases and all injury outcomes. According to the WHO,[2] alcohol consumption is now the world's third largest risk factor for disease and disability, with almost 4% of all global deaths attributed to alcohol.
5. Limitations
Our study has several limitations. First, this study used a cross-sectional survey design, which does not enable conclusions regarding causality. However, a cross-sectional survey was considered necessary because previous studies did not investigate the extent of alcohol consumption or of awareness of its negative effects on human health among secondary school students. In the future, longitudinal studies are needed to determine the causal relationship between alcoholic drink consumption and awareness of its negative effects on students’ health. Second, all participants were recruited from secondary schools in 2 States in Nigeria. This approach may have limited the ability to generalize these findings to other populations. Third, our study used self-reported assessments. The instrument showed good validity; however, future research may need to use observational assessments and interview.
6. Implications
If no further research or action is implemented to determine the extent of alcohol consumption and awareness of its negative effects on human health among secondary school students in Nigeria, in other parts of the country in particular, then alcohol consumption among adolescent students may be associated with increased school-based violence, student neglect and abuse, and absenteeism in school, among other social issues. In addition, policy interventions and other actions to reduce the patterns of alcohol use among the student population may not be realistic. Therefore, further research is needed to examine the patterns and prevalence of alcohol consumption and of awareness of its negative effects on human health among secondary school students across the globe.
7. Conclusion
The present study suggests that male secondary school students moderately consume beer and local cocktails, whereas their female counterparts are slight consumers of these 2 alcoholic drinks. Furthermore, both male and female students in the investigated area slightly consumed distilled spirits, whereas wine, liquor, local spirits, and palm wine were consumed moderately by students regardless of gender. Finally, male and female secondary school students significantly differed in their awareness of some of the negative effects of alcohol consumption on health. Overall, secondary school students are not very aware of some of the negative effects of alcohol on human health. Accordingly, health education teachers, school health counselors, and school administrators should combine their professional experiences to promote health education interventions and health counseling programs aimed at reducing students’ engagement in alcohol consumption. Schools should organize seminars for students to provide education on the health-related issues surrounding alcohol consumption. Addiction counselors should also organize awareness campaigns to orient Nigerian secondary school students to the damages caused by alcohol consumption. Parents should properly monitor and counsel their adolescent students on matters relating to alcohol consumption and its effect on their health.
Acknowledgments
We would like to thank the editor and anonymous reviewers for their constructive remarks regarding this work. We also are thankful to AuthorAID and American Journal Experts (AJEs) for their editing support. We are very much grateful to the research assistants and all the schooling adolescents who made this study a success.
Footnotes
Abbreviations: % = Percentage, ADCQSSS = Alcoholic Drinks Consumption Questionnaire for Secondary School Students, CI = confidence interval, DNC = does not consume, EA = extremely aware, HC = highly consume, M ± SD = means and standard deviation, MA = moderately aware, MC = moderately consume, NA = not aware, RC = rarely consume, SA = slightly aware, t = t test statistic.
Authorship: NME, CE, UCU, and HAN conceived the study. NME, BNA, HAN, CE, JIO, and BAE designed the study procedure. All the authors were involved in the data collection. CE, BNA, UCU, NME, JIO, and BAE carried out the analysis and interpretation of these data. NME, CE, UCU, HAN, BNA, JIO, and BAE drafted the manuscript. CE, HAN, BNA, NME, JIO, UCU, and BAE critically revised the manuscript for intellectual content. All authors read and approved the final manuscript.
The authors report no conflicts of interest.
References
- [1].Rehm J, Baliunas D, Borges GLG, et al. The relation between different dimensions of alcohol consumption and burden of disease: an overview. Addiction 2010;105:817–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].World Health Organization. Global Status Report on Alcohol and Health. Geneva: WHO Press; 2011. [Google Scholar]
- [3].Gureje O, Degenhardt L, Olley B, et al. A descriptive epidemiology of substance use and substance use disorders in Nigeria during the early 21st century. Drug Alcohol Depend 2007;91:1–9. [DOI] [PubMed] [Google Scholar]
- [4].Makajuola AB, Aina OF, Onigbogi L. Alcohol and other psychoactive substance use among Tanker drivers in Lagos, Nigeria. Eur Sci J 2014;10:545–59. [Google Scholar]
- [5].Adekeye OA, Adeusi SO, Chenube OO, et al. Assessment of alcohol and substance use among undergraduates in selected private universities in Southwest Nigeria. IOSR-JHSS 2015;20:1–7. [Google Scholar]
- [6].Dumbili E. Changing patterns of alcohol consumption in Nigeria: an exploration of responsible factors and consequences. Med Sociol Online 2013;7:20–33. [Google Scholar]
- [7].Bada FO, Adebiyi DR. Alcohol consumption behaviour among high school students in Nigeria. J Educ Soc Res 2014;3:507–10. [Google Scholar]
- [8].Lasebikan VO, Ola BA. Prevalence and correlates of alcohol use among a sample of Nigerian semirural community dwellers in Nigeria. J Addict 2016;2016:article ID 2831594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Alex-Hart BA, Opara PI, Okagua J. Prevalence of alcohol consumption among high school students in Port Harcourt, Southern Nigeria. Niger J Paediatr 2015;42:39–45. [Google Scholar]
- [10].Schütze M, Boeing H, Pischon T, et al. Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study. BMJ 2011;342:d1584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Rehm J, Mathers C, Popova S, et al. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009;373:2223–33. [DOI] [PubMed] [Google Scholar]
- [12].Olley BO, Ajiteru AA. Determinants of alcohol use among female university students in Nigeria. J Soc Sci 2001;5:161–7. [Google Scholar]
- [13].Bello S, Fatiregun A, Ndifon WO, et al. Social determinants of alcohol use among drivers in Calabar. Niger Med J 2011;52:244–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Faul F, Erdfelder E, Buchner A, et al. Statistical power analyses using G∗Power 3.1: tests for correlation and regression analyses. Behav Res Methods 2009;41:1149–60. [DOI] [PubMed] [Google Scholar]
- [15].Faul F, Erdfelder E, Lang AG, et al. G∗Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 2007;39:175–91. [DOI] [PubMed] [Google Scholar]
- [16].Brown JD. Statistics Corner: Questions and answers about language testing statistics: Sample size and power. Shiken: JALT Testing & Evaluation SIG Newsletter 2007; 11: 31–35. Available at: http://hosted.jalt.org/test/bro_25.htm [Google Scholar]
- [17].Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Erlbaum; 2nd ed.; 1988. [Google Scholar]
- [18].Uzoagulu AE. Practical Guide to Writing Research Project Reports in Tertiary Institutions. Enugu, Nigeria: Cheston; 2011. [Google Scholar]
- [19].IBM Corp. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp; 2011. [Google Scholar]
- [20].Pietrangelo A. How Alcohol Affects the Body. 2014. Available at: http://www.healthline.com/health/alcohol/effects-on-body. Accessed January 15, 2016. [Google Scholar]
- [21].Cox W, Hosier S, Crossely S, et al. Motives for drinking alcoholic beverages among British high school and university students. Addict Behav 2006;31:2147–57. [DOI] [PubMed] [Google Scholar]