

INTRODUCTION
Advances in treatment and care have made HIV a chronic disease for nearly one million people in the U.S. who have been infected with the virus (CDC, 2015). Many people living with HIV (PLWHIV) have achieved viral suppression because of effective treatments (Phillips et al., 2001), thereby preventing HIV-related morbidity and mortality while also reducing their risk of transmitting the virus by as much as 95% (Attia, Egger, Muller, Zwahlen, & Low, 2009). Yet HIV is still a deadly and costly epidemic, with nearly 40,000 new infections in the country each year for nearly the past decade (CDC, 2015). Contributing to new infections is the dual dynamic that includes asymptomatic PLWHIV who pass on the virus while unaware of their HIV status and those who are diagnosed but not virally suppressed and still highly infectious.
Government and community responses to this dual dynamic have been to promote a continuum of HIV testing and treatment (T&T), focusing attention on HIV case-finding, rapid linkage of infected persons to care and anti-retroviral treatments, and sustained medical care of PLWHIV to achieve and maintain viral suppression in order to prevent new infections at the population level (Dodd, Garnett, & Hallett, 2010; Granich, Gilks, Dye, De Cock, & Williams, 2009). Many states and local communities are also articulating sweeping goals to eliminate the HIV epidemic, such as “Getting to Zero” (zero discrimination, zero HIV/AIDS deaths, zero new HIV infections) (Haghdoost & Karamouzian, 2012; Joint UN Programme on HIV/AIDS, 2010), “90/90/90” (90% of PLWHIV know their status, 90% of those are linked to care, 90% of those linked to care are virally suppressed) (Joint UN Programme on HIV/AIDS, 2014), and reducing “community viral load” (CVL), or the sum of all virus in the community (Granich et al., 2010; Montaner et al., 2006). Making community-level improvements to reduce new infections and retain infected people in care requires a coordinated and highly effective local HIV T&T service system.
Despite efforts to tackle it, the HIV epidemic endures because HIV services at the community level are often fragmented and under resourced, and because forces that break down T&T effectiveness are rooted in complex behavioral and social determinants. In most communities, the full T&T continuum is an amalgam of agents and institutions with different structures and policies. Competing pressures, time lags, and other complex processes shape experiences across the continuum and disrupt service coordination (Lounsbury, Schwartz, Palma, & Blank, 2015). Achieving community-level goals to eliminate the HIV epidemic requires coordinated efforts through community consortia (Foster-Fishman, Berkowitz, Lounsbury, Jacobson, & Allen, 2001; Roussos & Fawcett, 2000; Weeks et al., 2013) with a common purpose and effective tools to guide the change process. To do this, it is necessary to build trusting, respectful relationships among diverse stakeholders in the care continuum, including both service providers and consumers of those services, so that truly novel, creative, and efficient strategies for addressing HIV prevention can be discovered and put forward (Stith et al., 2006).
Participatory system dynamics (SD) modeling offers conceptual, methodological and analytical tools to achieve these goals (Batchelder, Gonzalez, Palma, Schoenbaum, & Lounsbury, 2015; Foster-Fishman & Behrens, 2007; Foster-Fishman, Nowell, & Yang, 2007; Hirsch, Levine, & Miller, 2007; Homer & Hirsch, 2006; Hovmand, 2014). SD modeling is a unique approach to engage a broad group of community stakeholders in a process of systems examination and critique and to build their capacity as a coalition to address problems in the system that interfere with or undermine achieving community-level health outcomes. SD modeling uses a deliberative group process (Pesce, Kpaduwa, & Danis, 2011) to build visual and computational models and that allow coalition members to illustrate factors that generate and affect the structural and dynamic properties of the system. They can then use these models to hypothesize and simulate the likely effects of specific interventions anticipated to improve system behavior and achieve community-level health goals (Foster-Fishman et al., 2007; Stave, 2002; Zimmerman et al., 2016). SD modeling can simultaneously reflect the many interactive variables (inputs) that interact in complex ways and generate feedback loops and time delays that lead to patterns of unintended consequences of policy change or counterintuitive system behavior (outputs) (Richardson, 1999; Sterman, 2000). Engaging stakeholders who are deeply involved in the system and invested in its outcomes in a participatory model building process increases the validity of the model, coalition members’ trust of each other, and their sense of ownership of the model they build together. It can also increase their commitment to using the model for collaborative policy and program decision making for systems change (Hovmand, 2014).
We conducted a study of the HIV T&T care continuum in one northeast U.S. small metropolitan area using a combination of qualitative, quantitative, and SD modeling methods. To use SD modeling, we built and engaged a coalition of community-based organizations (CBOs), public and private health institutions, and community members who provide or utilize HIV-related services to participate in SD modeling to examine and address the problems of their local HIV T&T service system. In partnership with our research team, the coalition was tasked with building a “systems” understanding of the local T&T care continuum and provider inter-organizational networks using SD modeling both to uncover flaws and fractures in the HIV care system and to seek leverage points and opportunities to improve system functioning that could contribute to reducing CVL. While CVL is an abstract construct and ultimately unknowable, it is worthy of consideration and study via community participatory SD modeling and simulation to examine dynamics that contribute to increased or decreased virus at the community level.
This paper describes how we used a SD modeling process to build and engage a local stakeholder coalition to identify and unpack characteristics of and flaws in their local T&T system and the complex, dynamic systemic contributors to CVL in their community. We used participatory SD group model building methods in an iterative and deliberative process of systems critique and visual mapping of the local care continuum. The paper presents our methods and some of the resulting visual maps of the T&T system the coalition generated. We discuss implications of these visual models for subsequent computational and simulation modeling of the T&T system. We also discuss the potential of the project-developed stakeholder coalition for longer term efforts to use the SD models collaboratively for strategic decision making to achieve greater effectiveness of their local T&T care continuum to reduce CVL.
METHODS
Context of the Study Coalition and Research Site
Providers of HIV related prevention and care services in the small, northeast metropolitan area in which we conducted this study have forged a variety of relationships with each other over the past 30 years. Thus, we began our SD modeling effort in a community with a history of various types of short- and long-term collaborations. Further, given the relatively small size of the metropolitan area in which we conducted this study, many of the players (health and service organization directors, front-line staff, advocates, and other HIV infected or affected community members) were familiar with each other, even if not through direct interaction.
Our community-based research institute has a three-decade history of building community coalitions to conduct research on public health and social justice issues. Throughout that time, we have worked directly with local social service, health and public health agencies that provide services to people at high risk of contracting HIV and other blood-borne and sexually transmitted infections (STIs) and people infected with HIV to conduct research on HIV prevention, among other health and social issues. This facilitated our ability to bring together local collaborators to engage in this community-level effort. Our interdisciplinary project research team included researchers in anthropology, community and clinical/experimental psychology, human development and family studies, epidemiology, system dynamics and social network modeling, and community outreach interviewers. This research team shared responsibilities for recruitment of community consortium members, designing and facilitating SD model building, and process evaluation of the study.
Upon initiating this study, we had already established a project Steering Committee that included directors of two regional HIV/AIDS service organizations, a lesbian/gay/bisexual/transgender (LGBT) health cooperative, a substance abuse clinic, a federally qualified community health clinic, the city’s Department of Health and Human Services, and the state Department of Public Health division responsible for HIV/AIDS. Over the first year of the study, we augmented this Steering Committee by inviting leaders of several additional organizations, including medical or clinic unit directors from two local hospital HIV outpatient clinics, a children’s medical center, and the city’s health clinic, as well as the region’s Ryan White Part A program manager. Thus, the project’s twelve-member Steering Committee included leadership of the primary organizations responsible for delivering HIV-related health and social services in the urban center and most of the city’s ring towns. As such, the Steering Committee brought to the table significant experience with the problems facing those affected by and infected with HIV in the region.
The local community they serve includes the primarily African American and Hispanic residents of two urban centers (the larger city, population 125,000; the smaller city, population 73,000), as well as the surrounding suburban and peripheral rural towns whose residents are predominantly white. The overall metropolitan area includes a population of about 1.2 million residents. In the urban centers, low-income primarily heterosexual people of color as well as heroin and cocaine injection and non-injection drug users are the primary clientele of the health and social service organizations represented on the Steering Committee. These organizations also serve men who have sex with men (MSM), including MSM of color, from both the urban centers and the ring towns. Many of those in need of HIV prevention and treatment services in the region are challenged with poverty and joblessness, limited or no health insurance, language barriers, substance use disorders, mental health and other co-morbidities, unstable housing, and stigma related to their HIV status, gender identity or orientation, racial or ethnic identity, and/or economic status.
Over the past three decades, the community and public health organizations represented on our Steering Committee have made great efforts to provide comprehensive, culturally appropriate, compassionate, and effective evidence-based HIV prevention and treatment programs. They have done so in a context of chronically limited resources and fluctuating federal, state, and local funding streams to pay for these services. Despite these challenges, they are highly motivated and committed to ending the HIV epidemic and caring for those already infected with the virus. Steering Committee members expressed significant enthusiasm for using a new approach to examine, critique, and improve the local T&T care continuum through SD modeling.
System Dynamics Modeling Coalition Development and Member Composition
Despite the knowledge this Steering Committee brought to the project as directors of key organizations and clinical institutions, the group lacked representation of several important sectors in the HIV T&T system of actors. This included front-line service providers, who are directly involved in the daily activities of providing services and responding to the many challenges encountered in that process. Also missing was the clientele they serve, whose perspectives are necessary to ensure deep understanding of the layered barriers to accessing, using, and benefitting from whatever services are available and identifying gaps in needed services. We therefore expanded membership of the coalition to build an inclusive and more representative group to engage in the SD modeling process and critique of the full T&T service system. We recruited several direct service providers, including nurses, nurse practitioners, social workers, case managers, prevention program directors, and early intervention specialists who seek patients lost to care. Additionally, we invited several community members into the coalition, primarily including people with HIV, comprising members of local racial and ethnic groups, genders and gender identities, and people at risk or infected with HIV through different risk factors.
The expanded 25-member coalition was named the HIV CVL System Dynamics Modeling Task Force. The primary role of the Task Force was to engage in a participatory systematic assessment and visual mapping of the dynamics of the local HIV T&T service system using SD modeling methods. They brought their own knowledge and experiences to the task as well as their understanding of and perspectives on others’ experiences with local services and service coordination. We asked them to participate in a series of SD model building workshops. These workshops were designed to provide an introduction to participatory SD modeling and then to elicit their understanding of factors that generate delays, accelerations, and feedback complexity in the T&T service system. After building the model, we anticipated that they would commit to sharing it with the community and consider its potential applications, for example to inform policy and program decisions about how to improve the overall local HIV service system.
When possible, members of the Task Force were compensated for their time to participate in these activities. City and state public health staff were ineligible for such compensation, and staff of the local hospital clinics were also restricted from receiving compensation for these activities. However, the local CBOs were compensated for the time of their staff who attended sessions through Memoranda of Agreement with the organization. Specifically, CBOs whose director sat on the Steering Committee received $1000 per year for their time, and those organizations whose front-line staff were members of the Task Force received $50 for each session their staff attended. Likewise, HIV-positive community members on the Task Force were compensated $50 for each session they attended.
Though SD modeling sessions (described below) focused on a critique of the local T&T system in general, participation and sharing of personal experiences could potentially raise and reveal some sensitive information about Task Force members themselves or the organizations they represented. Therefore, we sought written informed consent from all Task Force members (including Steering Committee members) before initiating the modeling process to inform them of potential risks of disclosure and our protocols to protect their sensitive information. All study protocols and informed consent procedures received full review and approval by the Institute for Community Research’s Institutional Review Board.
Overview of Group System Dynamics Model Building Sessions
Best practices participatory SD modeling uses a group model building (GMB) approach to stakeholder engagement (Martinez-Moyano & Richardson, 2013; Richardson & Andersen, 1995). GMB is a multi-stepped, iterative series of stakeholder group “systems thinking” workshops (Best, Trochim, Haggerty, Moor, & Norman, 2008; Leischow & Milstein, 2006; Palma & Lounsbury, 2017). These workshops often incorporate co-occurring activities that include problem identification, system conceptualization, model formulation, deliberative feedback, evaluation, and in some cases model simulation (Hovmand, 2014; Martinez-Moyano & Richardson, 2013). Model development is facilitated with GMB session “scripts,” which are designed to guide Facilitators in the participatory modeling elicitation process (Andersen & Richardson, 1997; Hovmand, 2014; Hovmand et al., 2012; Hovmand, Rouwette, & Andersen, 2011). Scripts often include language and procedures to identify variables related to the problem, introduce SD concepts and thinking, elicit dynamic stories and causal structures through system mapping (e.g., causal loop diagrams—CLDs), and determine capacity and needs of the community to manage the problem. Participants are guided to build components of the model iteratively. While critiquing, revising, and re-conceptualizing the structure as it is diagramed, variables are assigned positive and negative relationships. In computational model building, information is also elicited to identify data or participant estimations to assign numeric values to variables in the model so it can be simulated during development.
We developed scripts for each of the stakeholder group workshops using existing materials (Hovmand et al., 2011) and our own designs in order to structure the sessions around three tasks. First, sessions included activities to build group members’ familiarity with each other in an effort to increase trust and break down barriers to communication and collaboration based on social hierarchies (organizational leaders working closely with front line workers and community members/clients) and other potential divisions by race/ethnicity, gender, age, education level, and so on. These activities are necessary to ensure full engagement of all stakeholders, increase group members’ confidence to contribute, and generate consensus. Second, scripts were designed to build group capacity to use SD modeling language and techniques to critique and diagram the local T&T system. These scripts incorporated generally didactic presentations of key SD modeling concepts, terminology and methodology with group practical exercises that applied the terms and concepts. Third, scripts were designed to build the model itself. This required iterative large and small model development tasks that built upon each other, thereby generating increasingly refined and specific modules, or small models, that would be integrated and synthesized into the large model of the full T&T continuum. All sessions ended by asking if anyone had had any “ah-ha” moments that day. In addition to getting immediate feedback on the session, this was designed to encourage developing a shared vision and eliciting everyone’s contribution to the modeling process, as well as to acknowledge and normalize SD modeling as a learning process.
Coalition Trust Building Exercises
An open exchange of ideas was encouraged at all GMB sessions. This open exchange was supported by reiterating the need for diverse input into critiquing and modeling the local HIV care system if together they were to build a valid, useful, and effective tool for improving it. To increase Task Force members’ comfort in exchanging ideas and perspectives during the initial SD modeling sessions, scripts included small group exercises designed to break down communication barriers, increase members’ general familiarity with each other, and build their confidence to work together on challenging problems of the T&T system critique and modeling process. For example, in Session 1, we included a simple small-group ice-breaker exercise to find things in common about each other, as well as a more complex small-group exercise to define selected key variables for inclusion in the model. The ice breaker was set up as a fun competition between groups and created a relaxed and comfortable interaction among and within small mixed groups of diverse stakeholders. For the variable definition and other break-out group exercises in later sessions, we purposively created small groups of 3–6 participants that included people from different organizations and roles in the T&T system, paired with a project research staff Facilitator and Documenter, in order to ensure different perspectives were represented in each group for those exercises and that all voices were recorded. A combination of large group and small group activities facilitated information sharing while ensuring full member participation in the complex modeling and iterative feedback processes.
Systems Thinking and Causal Loop Diagramming Exercises
We began building Task Force member capacity to engage in systems critique and SD modeling of their local HIV T&T care continuum at initial Steering Committee meetings during the study development phase and at a two-hour introductory session with the new members at the time of their recruitment into the Task Force. All coalition members were introduced to the project goals to engage in a community participatory in-depth examination of the local T&T service system. We described the plan to use SD modeling methods to build a model of the local care continuum to understand how systemic processes affect HIV CVL, which can then be used to build “systemic interventions” to reduce it. The need to conduct this systems critique and model building by incorporating multiple stakeholders’ perspectives was also emphasized.
In the pre-modeling orientation sessions, we provided coalition members with basic information about systems thinking, with a focus on the concept of ‘reinforcing’ (positive) and ‘balancing’ (negative) feedback loops. We also discussed the uses of SD modeling for understanding community-level dynamics that lead to inefficiencies and unanticipated delays or other unfavorable outcomes that impede their efforts to achieve their prevention and treatment goals. These sessions included introducing them to many of the key concepts and terms used in SD modeling in order to prepare them for the modeling process and to bring all Task Force members to the same knowledge base. Concepts common in SD modeling were defined and explained, such as stocks (i.e., accumulations of people, things, or information) and flows (transitions of stocks to different statuses over time), feedback loops, time delays, reference modes (i.e., graphs showing variable changes over time), and causal loop diagrams (CLDs), which are visual maps that display feedback structures and other relationships among variables in the dynamics system (Batchelder et al., 2015; Batchelder & Lounsbury, 2016). We developed easily understandable handouts describing and illustrating the primary terms and concepts used in SD modeling for their continued reference throughout the model building process. Handouts were also created to accompany each model simulation demonstration that offered step-by-step explanations of the simulation process as well as comparison of different inputs and output options. These and all other handouts were compiled in three-ring binders for each Task Force member’s use during all modeling sessions.
System Dynamics Model Building Exercises
Early GMB workshops with the Task Force focused on identifying key elements of the system (variables in the model), defining those key variables, and specifying their relationships to each other. We used an iterative process working with them to specify model constructs and relationships among them. Over time, work with the variables they identified became more sophisticated and focused in order to specify those critical for representing the T&T system as they perceive it and possible strategies to improve it. Our goal was to elicit the most parsimonious but complete representation of the system that reflects their perspectives and understanding of how it works and what interferes with system performance.
In between model building sessions, the research team compiled the narrative data and visual representations of their conceptual efforts, including their definitions and prioritization of the variables as well as visual maps, or models, in the form of CLDs. These were then brought back to the Task Force for further deliberation and conceptual development in subsequent sessions. This process of model co-construction, reflection, critique, and re-construction generated the structure and components for building a full visual model of the system and the needed conceptual structure for development of a computational model to simulate it.
Table 1 summarizes the design and components of the iterative GMB process we used to elicit, specify, refine, and validate the Task Force members’ conceptual SD model of their local HIV T&T service system and its effectiveness to reduce CVL. We used a combination of full group and smaller break-out group sessions and activities to facilitate engagement of all Task Force members in each stage of conceptual SD model development and refinement. At an early stage of the model development process, the Task Force was temporarily divided into two equivalent Teams (A and B) that included similar representation of professionals and community members. Team A addressed case finding, getting HIV tested, and getting PLWHIV linked to care; Team B addressed treatment and care maintenance and achieving and sustaining viral suppression. In later sessions, teams were integrated within small groups or as the full Task Force when models were being refined. At the time of this writing, the Task Force and Research Team had finalized building the conceptual model (visual maps) in the form of CLDs of the full T&T system and prepared the small models for simulation (Sessions 1–7). (The process of model computation, parameterization, and simulation will be reported elsewhere.)
Table 1.
Participatory System Dynamics Group Model Building Stages and Activities of the Modeling Task Force and Research Team
| Pre-modeling Session |
|
|
Session 1 (Full Task Force: Teams A and B) |
|
|
Session 2 (Teams A and B meet separately) |
|
| Research Team data synthesis |
|
|
Session 3 (Full Task Force) |
|
| Research Team data synthesis |
|
| Sessions 4 and 5 (Full Task Force) |
|
| Research Team data synthesis |
|
|
Session 6 (Full Task Force) |
|
| Research Team data synthesis |
|
|
Session 7 (Full Task Force) |
|
SD = system dynamics
T&T = HIV test and treatment
CLD = causal loop diagram, a visual system dynamics map of system variables and their relationships.
Group Model Building Session Evaluation Design
To document and evaluate these GMB sessions, we used a combination of qualitative and quantitative process evaluation methods. These included audio recording all sessions and written observational documentation of each session by at least two members of the research team using a standardized observation form. We also asked Task Force members to complete a semi-structured exit survey at the end of each session, which was a modified version of a tool designed by Zimmerman and colleagues (Zimmerman et al., 2016). The brief survey assessed participants’ comprehension of the session’s content, their perspective on the quality of the session and group dynamics, attitudes on the potential effectiveness of the process to address problems of the T&T system, and their concerns about the session or the modeling process. We used these brief surveys to monitor concerns and recommendations derived from each session and to track Task Force members’ evolving knowledge and attitudes regarding the SD modeling process. Other products tracked as part of the process evaluation were the visual maps developed iteratively throughout the model building sessions that represented Task Force members’ systems thinking about the T&T service continuum and factors they hypothesized to affect its dynamic properties.
FINDINGS
Attendance and Participation in Group Model Building Sessions
Task Force member attendance at model building sessions was consistently high, despite the challenges of competing schedules of members who worked in different professions or who had difficult personal situations. After the initial introductory session, average attendance at all model building sessions was 83.7% (range 70–100%) of Task Force members.
Participation from all members was also very high, particularly in smaller break-out group activities, and increased over time. Purposive small-group member composition was designed for each session in which small-group tasks were conducted. This planned group composition changed at each session, but always included professionals and community members in each small group and, when possible, people representing different roles in the T&T care continuum (front-line staff, directors, etc.). We initiated each small group activity with a brief exercise to get to know the people at the table better. Facilitators were instructed to elicit views of each person and to encourage “talkers” to elicit views of others as well. We observed initial reticence to speak out among some Task Force members in early sessions, which dissipated over time. Increased comfort with participation in small groups extended to greater participation in large group activities in later sessions, as well.
Task Force members’ changing participation rates and the quality of their self-perceived participation over time were reflected in their responses on the session evaluation surveys, reported in Table 2 (items 2 and 5). Session observation notes also documented increased participation from nearly all members in deliberations about complex system processes and model components and structures, particularly in small working group activities. This improvement in participation may be a reflection of Task Force members’ increased perception over time that their ideas were understood and acknowledged (item 3 in Table 2), and that the research team was responsive to their questions (item 4), as well as their increased understanding of the model building process (item 6) and the components of system dynamics models (item 7).
Table 2.
Meana (Standard Deviation) Responses of HIV CVLb Modeling Task Force Members (N=25) on Anonymous Post-Session Evaluation Surveys at Pre-Modeling Introductory Session (T1)c and Group Model Building Sessions 1–6 (T2–T7)c
| Survey Evaluation Question | T1 N=24 |
T2 N=20 |
T3 N=16 |
T4 N=19 |
T5 N=15 |
T6 N=14 |
T7 N=16 |
|---|---|---|---|---|---|---|---|
| 1. The overall quality of today’s session was: | 4.96 (.81) |
5.16 (.83) |
5.31 (.87) |
5.32 (1.20) |
5.57 (.51) |
5.71 (.61) |
5.00 (.73) |
| 2. In general, the level of group member participation today was: | 4.92 (.78) | 5.20 (.62) |
5.25 (.86) |
5.63 (.60) |
5.60 (.50) |
5.64 (.50) |
5.50 (.73) |
| 3. The degree to which group members’ ideas were understood and acknowledged during today’s session was: | 5.22 (.85) |
5.05 (1.00) |
5.31 (.70) |
5.32 (1.16) |
5.60 (.63) |
5.71 (.47) |
5.38 (.72) |
| 4. Responsiveness to questions group members asked today was: | 5.54 (.72) |
5.35 (.75) |
5.50 (.73) |
5.32 (1.25) |
5.53 (.64) |
5.79 (.43) |
5.44 (.63) |
| 5. You felt the quality of your participation in today’s session was: | 4.79 (1.06) |
4.94 (.94) |
5.19 (.83) |
5.21 (1.18) |
5.20 (.86) |
5.64 (.75) |
5.64 (.75) |
| 6. At the present time, your understanding of the model building process is: | 4.67 (1.01) |
4.63 (.96) |
4.94 (.68) |
5.00 (1.25) |
5.47 (.64) |
5.50 (.76) |
5.00 (.90) |
| 7. At the present time, your understanding of the components of system dynamics models (e.g., feedback loops, stocks & flows) is: | 4.54 (.98) |
4.68 (1.06) |
4.88 (1.03) |
4.95 (1.22) |
5.20 (.78) |
5.43 (.94) |
5.00 (.93) |
| 8. Based on plans described in today’s session, opportunities for group member input and participation in model building will be: | 5.08 (.88) |
4.85 (.93) |
5.25 (.68) |
5.11 (1.24) |
5.53 (.52) |
5.64 (.63) |
5.25 (.68) |
| 9. The potential for the group to develop a useful system dynamics model about the full HIV test-and-treatment care continuum for this county is: | 5.04 (.77) |
4.95 (.95) |
5.06 (.77) |
5.05 (1.39) |
5.33 (.90) |
5.64 (.63) |
5.44 (.73) |
| 10. The potential for the group to identify the necessary data to simulate the model is: | 5.00 (.85) |
4.85 (.99) |
5.00 (.82) |
4.89 (1.33) |
5.13 (1.06) |
5.57 (.65) |
5.13 (.72) |
| 11. The potential of modeling to inform decision-making to improve community health by getting providers and policy makers on the same page (as compared to decision-making without modeling) is: | 4.59 (1.26) |
4.75 (1.07) |
4.81 (.98) |
4.74 (1.37) |
5.00 (1.00) |
5.11 (1.18) |
4.88 (.81) |
| 12. The potential of modeling to save time and effort by running model simulations before we make changes (as compared to implementing changes without modeling) is: | 4.88 (1.04) |
4.95 (1.10) |
5.06 (.77) |
4.74 (1.37) |
5.13 (.92) |
5.50 (.76) |
5.19 (.75) |
| 13. The overall potential of participatory system dynamics modeling to be useful to our community is: | 4.83 (1.11) |
4.95 (1.00) |
5.13 (.81) |
4.79 (1.36) |
5.20 (.86) |
5.46 (.80) |
5.31 (.70) |
Range 1 (very poor) to 6 (excellent).
CVL = community viral load
T1, T2… = Time 1, Time 2… surveys time points.
System Dynamics Modeling to Create Visual Maps of the Local HIV T&T Care System
The iterative conceptual model building sessions using GMB scripts resulted in Task Force development of multiple CLDs of their local T&T care continuum and of the challenges and programs that contribute to the weaknesses and strengths of that system. We present here limited samples of those CLDs in order to illustrate the conceptual model building process and to describe how we worked with Task Force members to define and refine their models iteratively in order most succinctly and effectively to represent the T&T system and embedded dynamic processes that generate and could potentially reduce CVL.
To begin model building, we presented the Task Force with 20 key variables extracted from a series of 11 elicitation group interviews, including 5 with HIV service providers (N=29 providers) and 6 with PLWHIV (N=44 PLWHIV) conducted during an earlier stage of the study. These focused group interviews explored factors that generate facilitators and barriers to successful implementation or utilization of the HIV T&T care continuum locally. The 20 key variables included (in no order): fear; denial; HIV knowledge; stigma; cultural values; motivation; substance use; housing status; mental health; medical providers; language and cultural competence; medical insurance; social support; transportation; HIV service providers; navigating the system; medication; life complications; case management; and accessibility of services. Our variable prioritization and definition exercises in Session 1 engaged Task Force members to examine these factors critically, begin to build common definitions and language for describing these variables, and start to identify which factors might be more important in the functioning of the T&T system. However, early exercises to introduce variables and their meaning did not result in a circumscribed set of variables to use for later modeling. Rather, the benefit appeared to be to encourage Task Force members to understand the need for specificity in thinking about key components of the system and how they might be represented as variables in the model.
After initial brainstorming, defining, and prioritizing key variables, we facilitated deliberative discussions about how the variables related to each other and to the overall T&T care continuum of services. Teams A and B (described above) met separately for this exercise. Each team was tasked with generating a CLD that reflected processes and factors that characterized their segment of the T&T continuum. Modelers on the research team drew those variables and their relationships in real time using Vensim software (Ventana Systems, 2015). This allowed Task Force members to see ties they were describing among variables and to correct and deliberate how to reflect them in the model. The resulting CLD from Team A is reproduced in Figure 1, and that produced by Team B is Figure 2.
Figure 1.
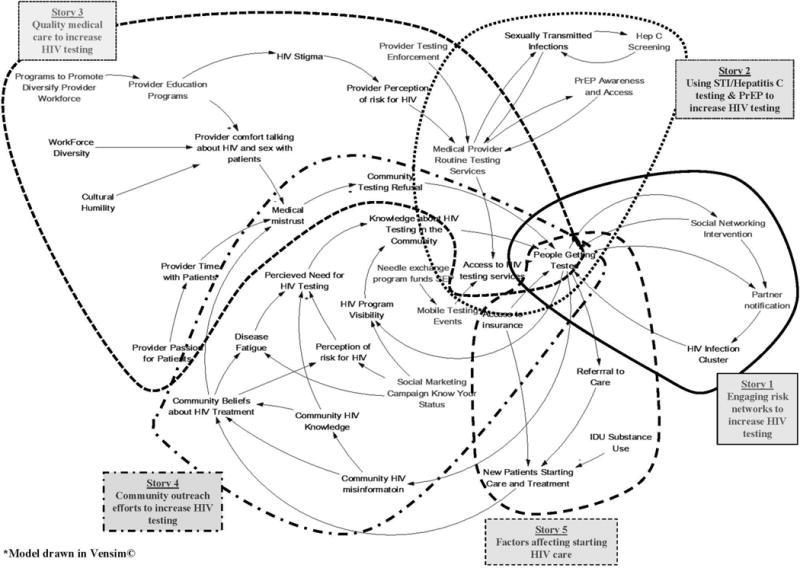
Casual Loop Diagram (CLD) of People Getting Tested, Linked to Care, and New Patients in Care with Stories Indicated*
Figure 2.

Casual Loop Diagram (CLD) of Patients in Care, Lost to Care, and Patients Virally Suppressed with Stories Indicated*
Documenting each team’s narrative through note taking and audio-recording while drawing the model with them provided the research team with data to review between modeling sessions. We used these data to extract Task Force members’ definitions of terms and to seek close associations among subsets of variables needed for building out the model. Through this process, we began to identify sub-narratives, or “stories,” within the larger narrative about the whole system, which we could then construct as small models in order to begin to manage the complexity of conceptualizing and modeling the full T&T care system. Initially, we segregated eight stories from the two CLDs generated by Teams A and B (see boundaries around model segments and segment titles in Figures 1 and 2). We then used subsequent GMB small-group exercises to validate, clarify, and further specify these stories with Task Force members. Specifically, we identified from the narrative of each story an action strategy and problem statement that defined that story, a list of possible programs, policies and other strategies to implement the action strategy, and contact points at which each story impacts the dynamic structure of the larger T&T model. The original stakeholder-developed story titles, their action strategies, impact points on the T&T continuum, and socio-ecological level of effect are summarized on Table 3. These small models were then available for further specification and parameterization in order to create small and large linked simulation models. Each one represents a potential leverage arena for action to improve functioning, efficiency, and effectiveness of the T&T care system to reduce CVL.
Table 3.
Stories Embedded in Stakeholder-Developed HIV Test & Treat (T&T) System Dynamics Causal Loop Diagrams and Action Strategies to Address Community Viral Load (CVL)
| Story # | HIV CVL Modeling Task Force Story Title | Action-Oriented Strategy to Achieve Story Goals | T&T Domain | Ecological Level |
|---|---|---|---|---|
| 1 | Involving individuals and groups of people “at risk” to increase HIV testing | Personalized outreach to promote HIV testing in at-risk networks | Outreach and screening | Community |
| 2 | Supporting providers to increase testing and awareness | Providers offering routine sexual health care service to improve access to HIV testing | Outreach and screening | Clinic |
| 3 | Quality medical care to improve HIV testing | Leveraging primary care for HIV prevention, testing, and referral to care | Access to testing and care | Clinic |
| 4 | Community outreach efforts to increase HIV testing | Engaging community leadership to promote HIV testing | Outreach and screening | Community |
| 5 | Factors affecting starting HIV care and medication | Supporting newly diagnosed persons to start HIV medical care and medication | Care initiation | Clinic |
| 6 | Services within the community to identify, connect, and keep people in care | Engaging family, friends, partners, and community to support the health and wellness of people living with HIV (PLWHIV) | Care retention | Community |
| 7 | PLWHIV empowerment to stay in care, on medications and virally suppressed | Peer leadership to empower PLWHIV to stay in care, on medications, and virally suppressed | HIV treatment | Community |
| 8 | Patient/provider relationships to adhere to care and treatment | Improving quality of HIV medical care in primary care settings through clinical supports and linkage to specialist resources | HIV treatment | Clinic |
We will use Story 6 to illustrate the evolution of the small models (stories) for the purpose of specifying problems and action domains in the T&T care continuum. The original stakeholder-developed title of Story 6 was “Services within the community to identify, connect, and keep people in care.” Their description of the story was paraphrased as follows:
Case management and support services are like a “hub” for the management of HIV care in the community. Case management is one avenue for implementing programs that can educate families, friends, and partners and help these important people build awareness, acceptance, and support for those with HIV in their lives. These efforts can help people with HIV to feel comfortable sharing their status with their support system. In addition, case management is key to accessing housing, which is instrumental for keeping people in care. Also, some shelters offer HIV testing, which may help: (1) identify or connect people to care and (2) involve partners and friends in case management and supportive services. Building partnerships between community-based institutions, such as churches, and publically funded services, such as case management, can improve support for people with HIV and their families, friends and partners. Some churches are already cultivating these kinds of partnerships.
The research team used this summary to derive an action-oriented strategy to inform SD simulation modeling of the story, which was, “Engaging family, friends, partners, and community to support the health and wellness of people with HIV.” We also used their narrative to develop a problem statement reflected in the story as follows:
Building partnerships between community-based institutions, e.g., churches, and publically funded services, e.g., case management, can improve support for people with HIV and their families, friends, and partners. These partnerships will help reduce the stigma of HIV in the community, which promotes greater acceptance of people with HIV by their families, friends and partners and helps them stay engaged in HIV medical care.
We then hypothesized the potential impact of this story on the T&T system, namely, that these efforts would increase patients in care and on ART, most of whom would become and stay virally suppressed, thereby reducing HIV incidence. Several possible programs, policies and practices were evident in the narrative to implement this action-oriented strategy, including:
Increase case management services;
Offer HIV testing in shelters;
Build more partnerships between community-based institutions, like churches, and publically funded services, like case management, to increase support for people with HIV and their families, friends and partners.
Mounting these efforts will require resources to hire more case managers, to support coalition-building, and to assist shelters to provide more HIV supportive services.
Finally, we revised the CLD representing this story using Vensim© (Ventana Systems, 2015). We focused on the action-oriented strategy and identification of important feedback loops likely to generate complex dynamics related to the story and its ties to the basic T&T system reproduced in Figure 3. The large balancing (B) feedback loop represents the T&T continuum of services, starting from HIV incidence, showing hypothesized positive associations with the number of diagnosed HIV+ persons, the HIV test positive rate, diagnosed HIV+ persons not in care and patients in care, on ART, adherent to ART, and virally suppressed, all of which is negatively associated with subsequent HIV incidence over time. This is undermined by reinforcing (R) feedback loops generated by patients being lost to care and stopping ART, which reduces the number virally suppressed and increases HIV incidence. However, new reinforcing feedback loops are generated by more case management services and community partnerships. These are hypothesized to promote community programming to help family, friends, and partners support PLWHIV to stay in care and on ART. They are also expected to reduce stigma in the community, which in turn generates greater acceptance of PLWHIV. Such programs also increase housing access, a key problem known to interrupt healthcare maintenance.
Figure 3.
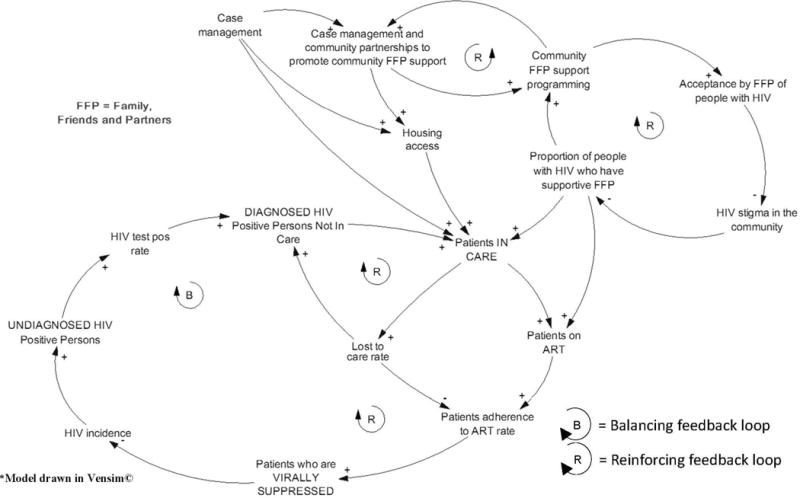
Story 6 “Engaging family, friends, partners, and community to support the health and wellness of people living with HIV” Causal Loop Diagram*
The remaining seven stories embedded within the large CLDs of the care continuum (illustrated in Figures 1 and 2) were similarly delineated and modeled by the research team based on Task Force model development and narratives, then validated in subsequent sessions with the Task Force. Structural validity of the models was increased by the iterative process of stakeholder deliberation and initial visual modeling, researcher analysis and refined modeling, and re-evaluation by stakeholders to produce small and large models reflecting the primary strengths and weaknesses of the T&T system. These models will subsequently be parameterized by assigning numeric values to the variables in the equations. They can then be simulated to further validate behavioral validity of the models through community applications, for example as an aid to inform policy and program decisions (Barlas, 1996; Roberts, Anderson, Deal, Garet, & Shaffer, 1983).
Task Force Member Evaluation of Group Model Building Sessions
Responses to most post-session evaluation survey questions improved steadily over the 6-month period between the pre-modeling sessions (time 1 [T1]) through Session 7 (time 7 [T7]) (see Table 2). This included an improved understanding of the modeling process over time, their growing belief in their capacity to develop an accurate SD model of the local T&T system, and their increasing confidence that this effort will result in a useful decision-making tool for the community to make improvements to their T&T care continuum, though responses to the latter were generally lower than for other statements.
Initial responses to an open-ended question on the post-session evaluations regarding their biggest concern about the modeling process focused on whether they would be able to understand the modeling process and language, that the model would be too big and the problem too complex, that it would not be used, or that it would not impact the behavior of doctors or policy makers. Though less commonly mentioned at later sessions, concerns about whether the model would be used and how effective it would be to implement policy and programmatic changes remained among some Task Force members. Also, while they indicated less concern about their own understanding of the model over time, at least one person mentioned concern that people not involved in the model building process would be unable to understand the model and its potential uses.
Task Force members were also asked an open ended question on the post-session survey regarding what they believed the most useful aspect of the modeling process was likely to be. Responses included: concretely documenting and finding gaps in the system; how to improve the system; the possibility of impacting many PLWHIV; and collaboration, communication, and shared discussion among team members during the process. Midway through the modeling process, they also recognized the benefits of their own input and the visual diagrams of the system components and problems. In later sessions, participants indicated the benefits of being able to see the impact of different possible actions or scenarios, and future planning and decision making based on past information. Members also mentioned benefits of promoting understanding of the barriers to care and “getting everyone on the same page.” Several Task Force members indicated that just coming together for the purpose of critiquing and modeling the local and regional HIV care continuum in the SD capacity building sessions was a positive step toward cross-organizational communication, information sharing, collaboration, and trust building among members.
Finally, we ended each session by asking Task Force members if they had had any “ah-ha” moments that day. The most commonly noted observation was the importance of having people with different perspectives and different expertise on the HIV T&T continuum in the room to facilitate the systems critique and modeling process. Insights came from hearing the priorities, experiences, and viewpoints of stakeholders who play very different roles and interact differently with the service system. Comments in later sessions also included recognition of their own increasing capacity to understand the HIV care continuum from a systems perspective, to model factors that constitute that system and its dynamic properties, and to consider what might be priority areas to mitigate ongoing problems with the system.
DISCUSSION
SD modeling has been used as a tool to bring stakeholders together to examine complex problems at the community level, from environmental concerns (Arquitt & Johnstone, 2004; Stave, 2010; Van den Belt, 2004), to urban and rural development (Hoard et al., 2005; Richardson, 2011), to public health problems (Gillen et al., 2014; Hirsch, Homer, Evans, & Zielinski, 2010; Hovmand & Ford, 2009; Lounsbury, Hirsch, Vega, & Schwartz, 2014), including HIV and AIDS (Batchelder et al., 2015; Lounsbury et al., 2015; Martin et al., 2015). The unique mechanism by which SD modeling supports community solutions to tackle systemic problems is through the engagement of stakeholders in a “systems thinking” process (Best et al., 2008; Trochim, Cabrera, Milstein, Gallagher, & Leischow, 2006). Through this process, stakeholders most directly engaged in the system are facilitated and capacitated both to hear and to share divergent perspectives and come to consensus through the group model building process (Hovmand et al., 2012; Rouwette, Vennix, & van Mullekom, 2002). Because SD modeling is a group problem solving task, it promotes trust building and buy-in from participants to engage in the effort while proposing explanations of the problem, system structure, and leverage points to produce solutions.
Both the Steering Committee and the new Task Force members expressed initial interest in the concept of SD modeling to understand and improve the local T&T system and were enthusiastic about the idea of a multi-stakeholder coalition to engage in the process and to seek solutions together. The introduction to analytical concepts common in SD modeling presented initial challenges for some participants, though these dissipated over time with continued use of the terms and our explication and demonstration of their application in subsequent model building sessions. Clearer to most participants from the start was the value of this collaborative review of the T&T system and the idea of building a visual and simulation model of the care continuum in order to seek leverage points to enhance efficient use of limited resources.
The clear and common goal of using this process to improve the local and regional HIV T&T continuum in order to reduce CVL, improve the health of PLWHIV, and reduce potential new infections was a rallying point for Task Force members. We anticipate that this common cause would be crucial for future model validation sessions and later efforts to use the collaboratively developed SD model as a policy and program decision-making tool. Likewise, we observed increasing trust, comfort, and sharing of ideas and viewpoints over time, particularly by community members. Consumers of HIV health and social services rarely have the opportunity to express their perspectives and experiences of the system in the same room with service providers and policy makers. It is particularly challenging to create an atmosphere that facilitates their open communication in the presence of doctors, organizational directors, and other decision makers. We also noted some skepticism in the group about the potential for this process and the resulting tool to be accurate, valid, and useful to the community. However, this skepticism has been important for moving the thinking and modeling process forward by generating group responses to clarify and improve understanding and conceptual maps of the system.
In addition to Task Force member engagement in the systems critique, we observed increasing familiarity with SD modeling terminology and mapping as well as improved understanding of the stages and procedures involved in creating a SD model of their HIV T&T care system. Furthermore, all Task Force members indicated greater confidence over time that the resulting model would be able to incorporate and reflect all the complex issues of the T&T care system, despite its complexity. This greater confidence in the product increases the potential for the models to be used to aid in decision making to advance group-proposed solutions to the systems problems.
This study has several limitations. First, it is being conducted in only one metropolitan area. Historical or other conditions in this region may have made this city more ready for this kind of multi-stakeholder community collaborative systems critique. We cannot speak to the generalizability or replicability of this process nor the resulting SD models for other cities. However, we believe that many small to mid-sized urban areas in the U.S. could successfully engage in this type of effort, and that the conceptual (visual) SD models generated by this study are likely to reflect common characteristics of T&T care systems elsewhere. These assumptions need further testing in other settings. Because the project is ongoing, the Task Force’s final models of the T&T care continuum, their plans for its use, and their ultimate responses to the model building process are not yet known. Furthermore, coalition organizational capacity to implement community changes together with guidance provided by the SD model or resulting from the model-building process could not be known at the time of this writing. A more formal and sustainable organizational structure for the Modeling Task Force may be necessary for a coordinated effort to use the model as a decision-making tool (Foster-Fishman et al., 2001). However, ensuring diversity in the Task Force membership provided a strong foundation for inclusiveness, thereby increasing the likelihood that strategies they propose to improve the system will be culturally appropriate and will address the real problems of the community.
The HIV T&T continuum of care, with the treatment cascade (Hull, Wu, & Montaner, 2012) and resulting effects on community viral load, can benefit greatly from participatory SD group model building and the resulting capacitation of a community coalition to think systemically. The problems that contribute to system dysfunction vary for different stakeholders, and few mechanisms in the community facilitate an understanding of the whole picture and its structural characteristics and flaws. Despite disparate perspectives of stakeholders regarding the problem, their goals are the same—to eliminate the epidemic by preventing transmission and effectively treating all who are infected. This provides the potential for development of meaningful solutions when co-constructed by those stakeholders through a facilitated process of systems critique and evaluation.
Acknowledgments
We wish to thank the members of the Greater Hartford HIV CVL System Dynamics Modeling Task Force who contributed their time, ideas, expertise, and experiences to this effort, including Merry Bajana, Christina Cipriani, Angelique Croasdale-Mills, Ricardo Cruz, Robin Deutsch, Linda Estabrook, Alice Ferguson, Nilda Fernandez, Seja Jackson, Heidi Jenkins, Jennifer Krebsbach, Clifford Lumpkin, John Merz, Mauricio Montezuma, Fernando Morales, Tung Nguyen, Bill Petrosky, Janette Rodriguez, Romario Roper, Ashley Rosario, Carol Steinke, LaToya Tyson, Yolanda Velez, and Danielle Warren-Dias. Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Numbers R01MH103176 and R21MH110335. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Glossary
List of Abbreviations
- AIDS
acquired immune deficiency syndrome
- CBOs
community-based organizations
- CDC
Centers for Disease Control and Prevention
- CLD
causal loop diagram
- CVL
community viral load
- GMB
group model building
- HIV
human immunodeficiency virus
- LGBT
lesbian/gay/bisexual/transgender
- PLWHIV
people living with HIV
- PrEP
pre-exposure prophylaxis [pills]
- SD
system dynamics
- STIs
sexually transmitted infections
- T&T
[HIV] testing and treatment
Contributor Information
Margaret R. Weeks, Institute for Community Research, 2 Hartford Sq. W., Ste. 100, Hartford, CT 06106, 860-278-2044.
Jianghong Li, Institute for Community Research.
David Lounsbury, Albert Einstein College of Medicine, Montefiore Medical Center, 3300 Kossuth Avenue, Bronx, NY 10467.
Helena Danielle Green, Institute for Community Research.
Maryann Abbott, Institute for Community Research.
Marcie Berman, Institute for Community Research.
Lucy Rohena, Institute for Community Research.
Rosely Gonzalez, Institute for Community Research.
Shawn Lang, AIDS Connecticut.
Heather Mosher, Institute for Community Research.
References
- Andersen D, Richardson G. Scripts for group model building. System Dynamics Review. 1997;13(2):107–129. [Google Scholar]
- Arquitt S, Johnstone R. A scoping and consensus building model of a toxic blue-green algae bloom. System Dynamics Review. 2004;20(2):179–198. [Google Scholar]
- Attia S, Egger M, Muller M, Zwahlen M, Low N. Sexual transmission of HIV according to viral load and antiretroviral therapy: systematic review and meta-analysis. AIDS. 2009;23(11):1397–1404. doi: 10.1097/QAD.0b013e32832b7dca. [DOI] [PubMed] [Google Scholar]
- Barlas Y. Formal aspects of model validity and validation in system dynamics. System Dynamics Review. 1996;12:183–210. [Google Scholar]
- Batchelder A, Gonzalez JS, Palma A, Schoenbaum E, Lounsbury DW. A Social Ecological Model of Syndemic Risk affecting Women with and At‐Risk for HIV in Impoverished Urban Communities. Am J Community Psychol. 2015;56(3–4):229–240. doi: 10.1007/s10464-015-9750-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Batchelder A, Lounsbury DW. Simulating Syndemic Risk: Using System Dynamics Modeling to Understand Psycho-Social Challenges Facing Women Living with and At-Risk for HIV. In: Neal Z, editor. Handbook of Applied System Science. London: Routledge Press (Taylor & Francis Group); 2016. [Google Scholar]
- Best A, Trochim WM, Haggerty J, Moor G, Norman C. Systems thinking for knowledge integration: New models for policy-research collaboration. In: Ferlie E, Hyde P, McKee L, editors. Organizing and Reorganizing: Power and Change in Health Care Organizations. London: Routledge; 2008. [Google Scholar]
- CDC. HIV Surveillance Report. 2015;27 Retrieved from http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. [Google Scholar]
- Dodd PJ, Garnett GP, Hallett TB. Examining the promise of HIV elimination by ‘test and treat’ in hyperendemic settings. AIDS. 2010;24(5):729–U128. doi: 10.1097/QAD.0b013e32833433fe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster-Fishman PG, Behrens TR. Systems change reborn: rethinking our theories, methods, and efforts in human services reform and community-based change. Am J Community Psychol. 2007;39(3–4):191–196. doi: 10.1007/s10464-007-9104-5. [DOI] [PubMed] [Google Scholar]
- Foster-Fishman PG, Berkowitz SL, Lounsbury DW, Jacobson S, Allen NA. Building collaborative capacity in community coalitions: A review and integrative framework. Am J Community Psychol. 2001;29(2):241–261. doi: 10.1023/A:1010378613583. [DOI] [PubMed] [Google Scholar]
- Foster-Fishman PG, Nowell B, Yang H. Putting the system back into systems change: a framework for understanding and changing organizational and community systems. Am J Community Psychol. 2007;39(3–4):197–215. doi: 10.1007/s10464-007-9109-0. [DOI] [PubMed] [Google Scholar]
- Gillen EM, Hassmiller Lich K, Yeatts KB, Hernandez ML, Smith TW, Lewis MA. Social ecology of asthma: engaging stakeholders in integrating health behavior theories and practice-based evidence through systems mapping. Health Education & Behavior. 2014;41(1):63–77. doi: 10.1177/1090198113486804. [DOI] [PubMed] [Google Scholar]
- Granich RM, Crowley S, Vitoria M, Smyth C, Kahn JG, Bennett R, Williams B. Highly active antiretroviral treatment as prevention of HIV transmission: review of scientific evidence and update. Curr Opin HIV AIDS. 2010;5(4):298–304. doi: 10.1097/COH.0b013e32833a6c32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373(9657):48–57. doi: 10.1016/S0140-6736(08)61697-9. [DOI] [PubMed] [Google Scholar]
- Haghdoost A, Karamouzian M. Zero new HIV infections, zero discrimination, and zero AIDS-related deaths: feasible goals or ambitious visions on the occasion of the world AIDS day. Int J Prev Med. 2012;3(12):819–823. doi: 10.4103/2008-7802.104850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch G, Homer J, Evans E, Zielinski A. A System Dynamics Model for Planning Cardiovascular Disease Interventions. Am J Public Health. 2010;100(4):616–622. doi: 10.2105/AJPH.2009.159434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch G, Levine R, Miller RL. Using system dynamics modeling to understand the impact of social change initiatives. Am J Community Psychol. 2007;39(3–4):239–253. doi: 10.1007/s10464-007-9114-3. [DOI] [PubMed] [Google Scholar]
- Hoard M, Homer J, Manley W, Furbee P, Haque A, Helmkamp J. Systems modeling in support of evidence-based disaster planning for rural areas. International Journal of Hygiene and Environmental Health. 2005;208(1–2):117–125. doi: 10.1016/j.ijheh.2005.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Homer JB, Hirsch GB. System dynamics modeling for public health: background and opportunities. Am J Public Health. 2006;96(3):452–458. doi: 10.2105/AJPH.2005.062059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hovmand PS. Community Based System Dynamics. New York: Springer; 2014. [Google Scholar]
- Hovmand PS, Andersen DF, Rouwette E, Richardson GP, Rux K, Calhoun A. Group model-building ‘scripts’ as a collaborative planning tool. Systems Research and Behavioral Science. 2012;29:179–193. [Google Scholar]
- Hovmand PS, Ford DN. Sequence and timing of three community interventions to domestic violence. Am J Community Psychol. 2009;44(3–4):261–272. doi: 10.1007/s10464-009-9264-6. [DOI] [PubMed] [Google Scholar]
- Hovmand PS, Rouwette E, Andersen D. Scriptapedia 3.04 2011 [Google Scholar]
- Hull MW, Wu ZY, Montaner JSG. Optimizing the engagement of care cascade: a critical step to maximize the impact of HIV treatment as prevention. Curr Opin HIV AIDS. 2012;7(6):579–586. doi: 10.1097/COH.0b013e3283590617. [DOI] [PubMed] [Google Scholar]
- Joint UN Programme on HIV/AIDS. Getting to Zero: 2011–2015 strategy. UNAIDS; Geneva: 2010. [Google Scholar]
- Joint UN Programme on HIV/AIDS. 90-90-90: An ambitious treatment target to help end the AIDS epidemic. Geneva: UNAIDS; 2014. [Google Scholar]
- Leischow SJ, Milstein B. Systems thinking and modeling for public health practice. Am J Public Health. 2006;96(3):403–405. doi: 10.2105/AJPH.2005.082842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lounsbury DW, Hirsch GB, Vega C, Schwartz CE. Understanding social forces involved in diabetes outcomes: a systems science approach to quality-of-life research. Qual Life Res. 2014;23(3):959–969. doi: 10.1007/s11136-013-0532-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lounsbury DW, Schwartz B, Palma A, Blank A. Simulating patterns of patient engagement, treatment adherence, and viral suppression: A system dynamics approach to evaluating HIV care management. AIDS patient care and STDs. 2015;29(S1):S55–S63. doi: 10.1089/apc.2014.0276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin EG, MacDonald RH, Smith LC, Gordon DE, Tesoriero JM, Laufer FN, O’Connell DA. Mandating the offer of HIV testing in New York: simulating the epidemic impact and resource needs. J Acquir Immune Defic Syndr. 2015;68(Suppl 1):S59–67. doi: 10.1097/QAI.0000000000000395. [DOI] [PubMed] [Google Scholar]
- Martinez-Moyano IJ, Richardson GP. Best practices in system dynamics modeling. System Dynamics Review. 2013;29(2):102–123. [Google Scholar]
- Montaner JSG, Hogg R, Wood E, Kerr T, Tyndall M, Levy AR, Harrigan PR. The case for expanding access to highly active antiretroviral therapy to curb the growth of the HIV epidemic. Lancet. 2006;368(9534):531–536. doi: 10.1016/S0140-6736(06)69162-9. [DOI] [PubMed] [Google Scholar]
- Palma A, Lounsbury DW. Complexity: The Evolution Toward 21st-Century Science. In: El-Sayed A, Galea S, editors. Systems Science and Population Health. London: Oxford University Press; 2017. pp. 37–47. [Google Scholar]
- Pesce JE, Kpaduwa CS, Danis M. Deliberation to enhance awareness of and prioritize socioeconomic interventions for health. Social Science & Medicine. 2011;72(5):789–797. doi: 10.1016/j.socscimed.2011.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phillips AN, Staszewski S, Weber R, Kirk O, Francioli P, Miller V, Ledergerber B. HIV viral load response to antiretroviral therapy according to the baseline CD4 cell count and viral load. JAMA. 2001;286(20):2560–2567. doi: 10.1001/jama.286.20.2560. [DOI] [PubMed] [Google Scholar]
- Richardson GP. Feedback thought in social science and systems theory. Pegasus Communications, Inc; 1999. [Google Scholar]
- Richardson GP. Reflections on the foundations of system dynamics. System Dynamics Review. 2011;27(3):219–243. [Google Scholar]
- Richardson GP, Andersen DF. Teamwork in Group Model Building. System Dynamics Review. 1995;11:1–14. [Google Scholar]
- Roberts N, Anderson D, Deal R, Garet M, Shaffer W. Introducation to computer simulation: A system dynamics modeling approach. Reading, Massachusetts: Addison-Wiley Publishing Company; 1983. [Google Scholar]
- Roussos ST, Fawcett SB. A review of collaborative partnerships as a strategy for improving community health. Annual Review of Public Health. 2000;21:369–402. doi: 10.1146/annurev.publhealth.21.1.369. [DOI] [PubMed] [Google Scholar]
- Rouwette EAJA, Vennix JAM, van Mullekom T. Group model building effectiveness: a review of assessment studies. System Dynamics Review. 2002;18(1):5–45. [Google Scholar]
- Stave KA. Using system dynamics to improve public participation in environmental decisions. System Dynamics Review. 2002;18(2):139–167. [Google Scholar]
- Stave KA. Participatory system dynamics modeling for sustainable environmental management: Observations from four cases. Sustainability. 2010;2:2762–2784. [Google Scholar]
- Sterman JD. Business dynamics: systems thinking and modeling for a complex world. Vol. 19. Irwin/McGraw-Hill; Boston: 2000. [Google Scholar]
- Stith S, Pruitt I, Dees J, Fronce M, Green N, Som A, Linkh D. Implementing community-based prevention programming: A review of the literature. Journal of Primary Prevention. 2006;27(6):599–617. doi: 10.1007/s10935-006-0062-8. [DOI] [PubMed] [Google Scholar]
- Trochim WM, Cabrera DA, Milstein B, Gallagher RS, Leischow SJ. Practical challenges of systems thinking and modeling in public health. Am J Public Health. 2006;96(3):538–546. doi: 10.2105/AJPH.2005.066001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van den Belt M. Mediated modeling: a system dynamics approach to environmental consensus building. Washington, DC: Island press; 2004. [Google Scholar]
- Ventana Systems, I. Vensim 6.4 2015 [Google Scholar]
- Weeks MR, Abbott M, Hilario H, Radda K, Medina Z, Prince M, Kaplan C. Structural issues affecting creation of a community action and advocacy board. Health Education Research. 2013;28(3):375–391. doi: 10.1093/her/cyt051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimmerman L, Lounsbury DW, Rosen CS, Kimerling R, Trafton JA, Lindley SE. Participatory System Dynamics Modeling: Increasing Stakeholder Engagement and Precision to Improve Implementation Planning in Systems. Adm Policy Ment Health. 2016;43(6):834–849. doi: 10.1007/s10488-016-0754-1. [DOI] [PMC free article] [PubMed] [Google Scholar]