

Abstract
Introduction:
IDRS is based on four simple parameters derived from known risk factors for diabetes; two modifiable risk factors (waist circumference and physical inactivity) and two non-modifiable risk factors (age and family history of diabetes), which may be amenable to intervention. The present study has been planned as the region specific validation is important before it can be used for screening in this part of the country.
Aims:
The aim of the present study was to validate MDRF-IDRS for screening of diabetes mellitus among adult population of urban field practice area, IGMC, Shimla, Himachal Pradesh, India.
Methods:
The present community based cross sectional study was conducted among 417 adults fulfilling the eligibility criteria using a two stage sampling design.
Results:
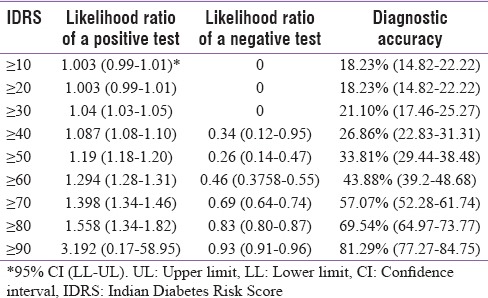
In the present study IDRS value ≥70 had an optimum sensitivity of 61.33% and specificity of 56.14% for detecting undiagnosed type 2 diabetes in the community. At an IDRS score of ≥70, the PPV was 23.47%, NPV as 86.88%, the diagnostic accuracy as 57.07%, LR for positive test as 1.398, LR for negative test as 0.69 and Youden's index as 0.17. However Youden's index was 0.19 at a cut of ≥60 i.e. higher than what was at ≥70. Higher IDRS scores increased the specificity but the sensitivity dramatically decreased. Conversely, lower IDRS values increased the sensitivity but the specificity drastically decreased. Area under the curve = 0.630 and a P value < 0.001.
Conclusions:
MDRF IDRS is user friendly screening tool but the criteria of including the parameter of physical activity for the calculation of the risk score needs to be clearly defined. In the present study the maximum sensitivity of 100% was seen at a cut off of ≥30. Hence we would recommend that all those in the medium and high risk group should be screened for type 2 Diabetes.
Keywords: Diabetes, Himachal Pradesh, Madras Diabetes Research Foundation-Indian Diabetes Risk Score, validation
INTRODUCTION
Over the past few decades, noncommunicable diseases (NCDs) have emerged as the leading causes of death globally, killing more people each year than all other causes combined.[1]
As per the International Diabetes Federation, the number of people with type 2 diabetes is increasing in every country. Currently, 387 million people are living with diabetes across the world, and it is expected to rise to a whooping figure of 592 million in 2035.[2]
Morbidity and early mortality occur as a result of inadequate health-care facilities for early detection and initiation of therapy, as well as suboptimal management of diabetes and associated morbidities. This is largely preventable by “primary prevention” of diabetes and enhancing awareness about the disease among the public and the health-care providers. The strategy for the prevention of type 2 diabetes mellitus (T2DM) is based on controlling modifiable risk factors and can be divided into two target groups; people at a high risk of developing T2DM and the entire population.
A strong argument exists in favor of screening for participants who are at increased risk for diabetes.[3] Attempts have been made to devise risk scores to screen population for diabetes both nationally and internationally.[4,5,6,7,8,9,10] The Indian Diabetes Risk Score (IDRS), a simple screening tool for prediction of undiagnosed diabetes, has been developed by Mohan et al. at the Madras Diabetes Research Foundation (MDRF), Chennai. The score referred to as MDRF-IDRS was derived from the Chennai Urban Rural Epidemiology Population Study (CURES) and was internally validated using the data from the Chennai Urban Population Study.[11] The IDRS is based on four simple parameters derived from known risk factors for diabetes; two modifiable risk factors (waist circumference and physical inactivity) and two nonmodifiable risk factors (age and family history of diabetes), which may be amenable to intervention.[12]
The score has been validated through many studies in various parts of the country,[13,14,15,16,17,18,19,20,21,22,23,24,25,26] but extensive search on PubMed reveals no study from the state of Himachal Pradesh. Keeping this in view, the present study has been planned as the region-specific validation is important before it can be used for screening in this part of the country.
Aims and objectives
The aim of the present study was to validate MDRF-IDRS for screening of T2DM among adult population of urban field practice area, Indira Gandhi Medical College (IGMC), Shimla, Himachal Pradesh, India.
MATERIALS AND METHODS
The present community-based cross-sectional study was conducted among 465 adults aged 20 years and above for a period of 1 year extending from August 2014 to July 2015 through household survey in the field practice area catered by the Urban Health Training Centre (UHTC) of Department of Community Medicine, IGMC, Shimla at Boileauganj. “Boileauganj” represents an urban population of Shimla district located within the municipal limits of Shimla city, Himachal Pradesh.
Study sample
With the target urban population of around 170,000; assuming that 50% of the screened population will be correctly diagnosed by MDRF-IDRS, 95% confidence interval, 5% margin of error, and response rate of 80%, the sample size for the present study was calculated as 384 using OpenEpi: Open Source Epidemiologic Statistics for Public Health, version 3.03a. A total of 500 participants were approached, of which 35 refused to take part in the study. Out of total 465 consenting participants, 48 were known diabetics, hence a total of 417 adults ≥20 years of age were screened for T2DM through house-to-house survey.
Study design, period, and tool
It was a cross-sectional household survey conducted for a period of 1 year from August 2014 to July 2015. IDRS[11] developed by Mohan et al. MDRF was applied as a research tool. All adults aged 20 years and above who consent to take part were included in this study.
Methodology
Boileauganj has a total population of 8205 individuals living in 2243 households as per census 2011. The study was conducted on 417 adults fulfilling the eligibility criteria for participation in the study. The study was conducted using a two-stage sampling design.
In the first stage, the households were selected by systematic random sampling. The household constituted the primary sampling unit. The whole study area was mapped, and all the main roads were identified. UHTC Boileauganj was taken as the starting point for the purpose of this study.
In the second stage, a single eligible participant was chosen from the selected household which formed the secondary sampling unit.
During each house visit, data were collected using the World Health Organization (WHO) Stepwise approach to surveillance (STEPS), which includes three steps for assessment of risk factors. The three steps are as follows:
Step 1: A predesigned, pretested pro forma was used to collect data from the study participants; this included information on sociodemographic characteristics, family history of diabetes and physical activity
-
Step 2: Anthropometric measurements were taken for all study participants. Measurements included height, weight, and waist circumference. His/her diabetes risk was assessed using MDRF-IDRS
Waist circumference was measured using a nonstretchable fiber measuring tape. The participant was asked to gather his or her shirt above the waist and to cross the arms and place the hands on opposite shoulders and stand erect in a relaxed position with both feet together. The hip area was palpated to locate the right ilium of the pelvis. A horizontal line was drawn just above the uppermost lateral border of the right ilium, and this mark was crossed at the mid-axillary line. The tape sat parallel to the floor and lied snug but did not compress the skin. The measurement was taken nearest to 1 cm
Height was measured with a tape to the nearest 1 cm. The participant was asked to stand with the heels together and toes apart. The toes should point slightly outward at approximately a 60° angle with the back of the head, shoulder blades, buttocks, and heels making contact with the wall. The participants head was placed in the Frankfort horizontal plane. The head is in the Frankfort plane when the horizontal line from the ear canal to the lower border of the orbit of the eye is parallel to the floor and perpendicular to the vertical wall
Step 3: Biochemical testing: All individuals were further evaluated for the presence of T2DM. They were asked to stay empty stomach for blood sample the next morning. After an overnight fast of 8 h, blood glucose estimation was done with a calibrated glucometer using glucose-oxidase peroxidase method (Accu-Chek® Active Meter). The patient was diagnosed with type 2 diabetes if the fasting blood glucose (FBG) values were ≥126 mg%, as per the WHO criteria. To confirm those patients for diabetes, whose FBG values were ≥126 mg%, 2 h oral glucose tolerance test (OGTT) was done. Seventy-five grams of anhydrous glucose was dissolved in 250–300 ml of water, and the participants were asked to drink it within 5 min. Exactly 2 h post 75 g of glucose, the venous blood glucose was obtained and was sent to the Biochemistry Laboratory of IGMC Shimla. Impaired glucose tolerance was labeled if the postprandial glucose values were between 140 and 199 mg/dl. Moreover, those with the glucose values ≥200 mg% were labeled as T2DM. Those who had an impaired fasting glucose (IFG) levels on glucometer, i.e., between 100 and 125 mg/dl, a repeat venous sample for FBG was taken, and only those patients who had FBG ≥126 mg% on venous sample were subjected to 2 h OGTT for the final diagnosis of DM.
The MDRF-IDRS uses a scoring system of 0–100. The risk factors used for this study are shown in Table 1.
Table 1.
Madras Diabetes Research Foundation-Indian Diabetes Risk Score
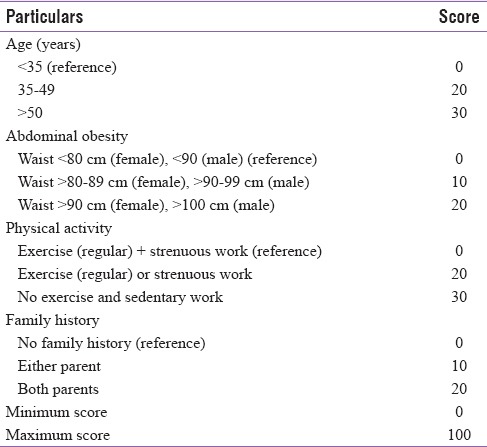
After adding up scores of all the four parameters, if the score is
≥60: The risk of having type 2 diabetes is very HIGH
30–50: MODERATE risk
<30: LOW risk.
Prior permission was taken from Institute Ethical Committee to go ahead with the study.
Statistical analysis
Statistical analysis was done using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA), OpenEpi: Open Source Epidemiologic Statistics for Public Health Version 3.03a and EpiInfo™ 7.1.5. Sensitivity, specificity, positive predictive values, negative predictive values, likelihood ratio (LR) for positive and negative tests, and diagnostic accuracy of different cutoffs were calculated for IDRS along with Youden's index. Receiver operator characteristic (ROC) curve was obtained for IDRS and area under the curve (AUC) was analyzed for the validation of the score.
RESULTS
The known diabetics (n = 48) were included for the prevalence data only (n = 465) and not for the validation of MDRF-IDRS, for which only 417 participants were included in the study. Out of these, 191 were males who constituted 45.8% of the study population. Mean age of all the 417 (screened) participants was 50.21 ± 13.78 years (51.52 ± 13.30 years in males and 49.10 ± 14.11 years in females). Age range of screened patients varied from 20 to 85 years.
Although no participant who had a low-risk score on MDRF DRS had type 2 diabetes, 33% of those had IFG levels. Majority of those who were at high risk or medium risk as per MDRF IDRS had normal blood glucose levels [Table 2].
Table 2.
Fasting blood glucose levels of the participants and their respective risk scores (n=417)
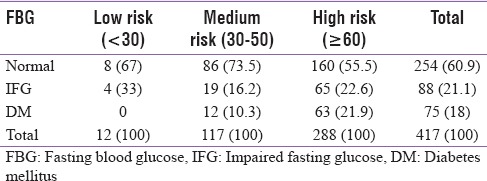
Table 3 provides the sensitivity, specificity, Youden's index, positive predictive value (PPV), and negative predictive value (NPV) of different cutoffs for IDRS.
Table 3.
Sensitivity and specificity at different cutoffs of Madras Diabetes Research Foundation Indian Diabetes Risk Score in the screened population (n=417)
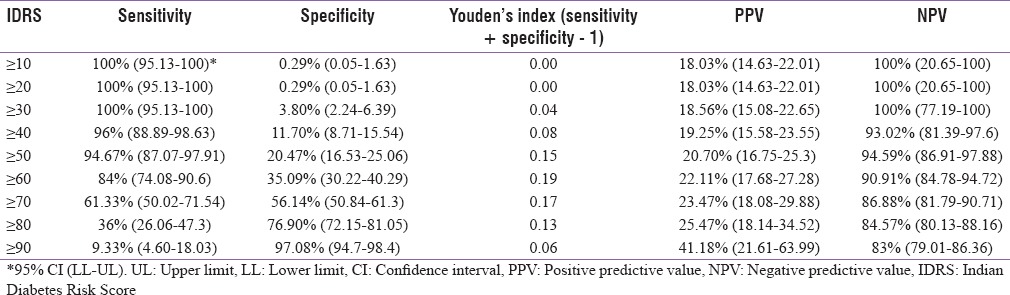
Table 4 gives the LRs for positive and negative tests as well as diagnostic accuracy for different cutoffs for IDRS.
Table 4.
Likelihood ratios of positive and negative test along with diagnostic accuracy at different cutoffs of Madras Diabetes Research Foundation Indian Diabetes Risk Score in the screened population (n=417)
In the present study, IDRS value ≥70 had an optimum sensitivity of 61.33% and specificity of 56.14% for detecting undiagnosed type 2 diabetes in the community. Higher IDRS scores increased the specificity, but the sensitivity dramatically decreased. ROC curve was obtained [Figure 1].
Figure 1.
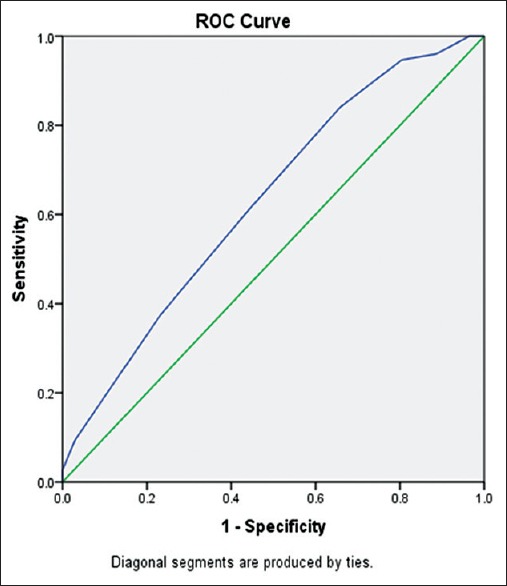
Receiver operator characteristic curve showing performance of Indian Diabetes Risk Score (n = 417) area under the curve: 0.630 (P = 0.000; 95% confidence interval: 0.564–0.697)
Our study thus confirms and validates the CURES data, and the IDRS score of ≥70 turned out to be the best cut point for identifying undiagnosed diabetes.
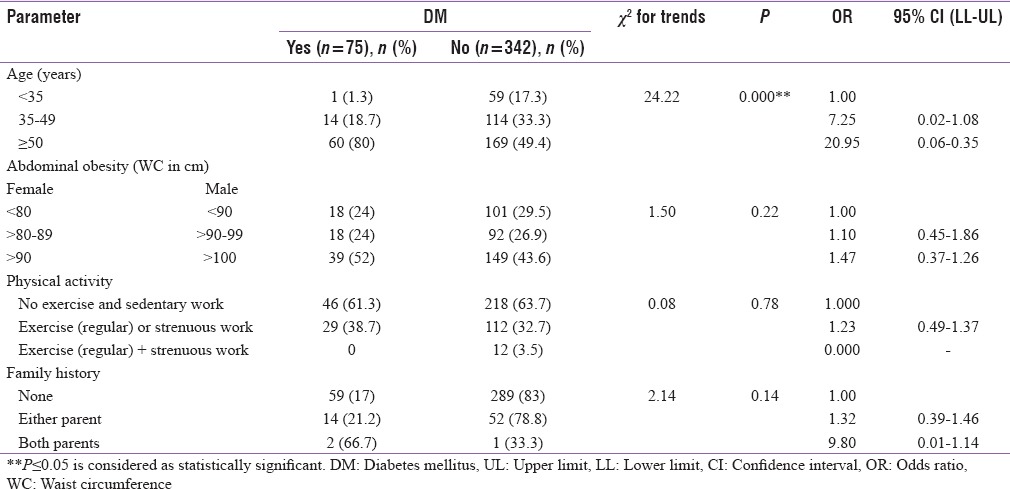
We also studied the association between T2DM and risk factors as per MDRF-IDRS among screened participants (n = 417) using Chi-square for trends [Table 5]. However, in the present study, the odds of diabetes increased with the strenuous work or regular exercise. This paradox can be due to inadvertent sampling error or the lesser sample size in the present study. Furthermore, a multiple number of factors interplay in the etiology of T2DM; it may be possible that in spite of engaging in physical activity and strenuous work, the participant might have other risk factors present such as stress which needs to be studied separately.
Table 5.
Prevalence of Type 2 diabetes mellitus and association between Type 2 diabetes mellitus and risk factors as per Madras Diabetes Research Foundation Indian Diabetes Risk Score among screened participants (n=417)
DISCUSSION AND CONCLUSION
In the present study, out of 465 consenting participants, 48 were known diabetics and rest of them (417) were screened for the presence of T2DM. As per MDRF-IDRS risk classification, maximum participants were at high risk for diabetes, i.e., 288 participants (69%), followed by medium risk - 117 participants (28%) and low risk (3%). Our study showed that an IDRS value ≥70 had an optimum sensitivity and specificity for detecting undiagnosed diabetes in the community. AUC was 0.630 and P < 0.001. Our study thus confirms and validates the CURES data, but the IDRS score of ≥70 is the best cut point for identifying undiagnosed type 2 diabetes in the present study, and at ≥70, the sensitivity remains at around 61% which reflects that there is 61% probability that MDRF-IDRS will correctly detect type 2 diabetes among the actual diseased. The specificity in the present study remains as low as around 56% which implies that there is 56% probability that the IDRS risk score will correctly detect nondiabetic among the actual nondiseased. Conversely that means that in 39% the MDRF-IDRS will give the result as a low risk even if the patient is a diabetic on biochemical tests and 44% of the times the score will give false high-risk alert even in case of actual nondiabetic adult.
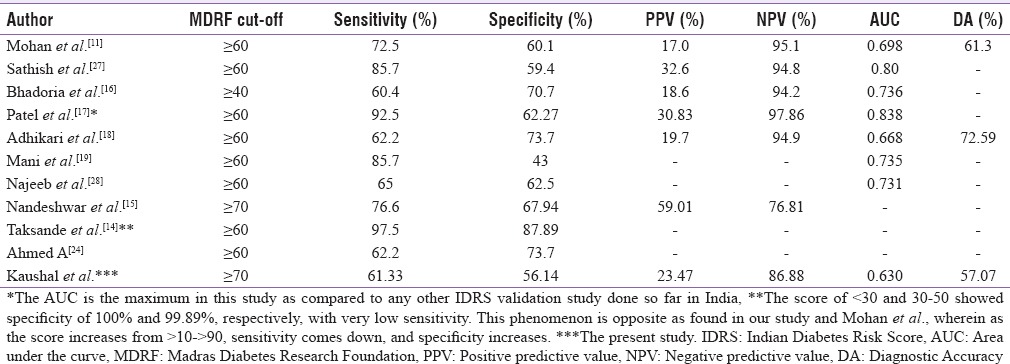
As opposed to the various studies done [Table 6] to validate the MDRF-IDRS score in various parts of the country where the cutoff for better sensitivity and specificity came at ≥60, it came to be ≥70 in the present study with the best balance between sensitivity and specificity. It is probably because of the profile of participants who were included in the study. Around 14% were <35 years of age, 31% between 35 and 49 years, and 55% above 50 years. As per MDRF-IDRS, the age group of 35–49 years gives the score of 20 directly; hence putting the participants score directly into the medium-risk category even if only one other positive parameter is there.
Table 6.
Madras Diabetes Research Foundation Indian Diabetes Risk Score validation studies from India
As per Mohan et al., all those who had a medium or high risk in the MDRF-IDRS are to be screened for diabetes (FBG and OGTT) hence putting a maximum number of participants at risk, thereby including many false positives.
After conducting this study, we came to the following conclusions regarding the use of MDRF-IDRS for screening of diabetes.
First, the criteria of including the parameter of physical activity for the calculation of the risk score need to be clearly defined. It is really subjective as to whom the interviewer may include in the sedentary/strenuous occupation or regular exercise/no exercise. For example, in the present study, we took the WHO-STEPS surveillance manual for dividing the participants into different categories of occupation or exercise levels.
Second, Mohan et al. had estimated the cost-effectiveness of MDRF-IDRS for screening as it would help in selective screening instead of universal screening. They have emphasized on screening those having the IDRS ≥60 for making it a cost cutting intervention. The results of our study demonstrated that the IDRS rarely classifies the participants in the low-risk group; as once the participant's age is ≥35 years, a score of 20 is assigned and even with another single risk factor positive, the participant gets included in the medium-risk category, thus categorizing maximum participants in either the medium-risk group (IDRS of 30–50) or high-risk group (IDRS ≥60) as found in the present study where the numbers in the high-, medium-, and low-risk group were 288, 117, and 12 respectively. Further, there were around 26% among the medium-risk group who had either IFG or diabetes and more than half of the “high-risk group” had normal blood glucose. Hence, MDRF-IDRS, though a simple and user-friendly score cannot be taken as an absolute risk estimate for type 2 diabetes at just the high-risk score. If only those with the high score would have been screened, 12 cases of type 2 diabetes would get missed and 23 participants with IFG would have missed. Although the cutoff for optimum sensitivity and specificity came at ≥70 in the present study, still the sensitivity is only around 61% and specificity as 56%. For screening purposes, we can choose a cutoff to maintain maximum sensitivity. In the present study, the maximum sensitivity of 100% was seen at a cutoff of ≥30. Hence, we would recommend that all those in the medium- and high-risk group should be screened for type 2 diabetes. Government of India has launched National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke which is envisaged to provide opportunistic screening (through opportunistic and/or camp approach) free of cost to all those above the age of 30 years at the point of primary contact with any health-care facility, be it the village, community health centre, district hospital, tertiary care hospital, etc. Commodity support for glucometer, glucostrips, and lancets have been provided to the states for screening and early detection of NCDs including type 2 diabetes at the subcenter in 100 program districts of 21 states. Hence, the overall cost of blood glucose testing has reduced dramatically.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.28
Acknowledgment
We thank the patients who enrolled in this study.
REFERENCES
- 1.Global Status Report on Non-communicable Diseases 2010. World Health Organization. 2011. [Last cited on 2014 Jun 14]. Available from: http://www.who.int/nmh/publications/ncd_report_full2010/_en/
- 2.IDF Diabetes Atlas Update Poster. 6th ed. Brussels, Belgium: International Diabetes Federation; 2014. International Diabetes Federation. [Google Scholar]
- 3.American Diabetes Association. Screening for diabetes. Diabetes Care. 2002;25:S21–4. doi: 10.2337/diacare.26.2007.s21. [DOI] [PubMed] [Google Scholar]
- 4.ADA Diabetes Risk Score. [Last cited on 2015 Nov 22]. Available from: http://www.diabetes.org/are-you-at-risk/diabetes-risk-test/
- 5.Lindström J, Tuomilehto J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care. 2003;26:725–31. doi: 10.2337/diacare.26.3.725. [DOI] [PubMed] [Google Scholar]
- 6.Schulze MB, Hoffmann K, Boeing H, Linseisen J, Rohrmann S, Möhlig M, et al. An accurate risk score based on anthropometric, dietary, and lifestyle factors to predict the development of type 2 diabetes. Diabetes Care. 2007;30:510–5. doi: 10.2337/dc06-2089. [DOI] [PubMed] [Google Scholar]
- 7.Glümer C, Carstensen B, Sandbaek A, Lauritzen T, Jørgensen T, Borch-Johnsen K. Inter Study. A Danish diabetes risk score for targeted screening: The Inter99 study. Diabetes Care. 2004;27:727–33. doi: 10.2337/diacare.27.3.727. [DOI] [PubMed] [Google Scholar]
- 8.Simmons RK, Harding AH, Wareham NJ, Griffin SJ. EPIC-Norfolk Project Team. Do simple questions about diet and physical activity help to identify those at risk of Type 2 diabetes? Diabet Med. 2007;24:830–5. doi: 10.1111/j.1464-5491.2007.02173.x. [DOI] [PubMed] [Google Scholar]
- 9.Long J, Rozo-Rivera A, Akers T, VanGeest JB, Bairan A, Fogarty KJ, et al. Validating the utility of the Spanish version of the American Diabetes Association Risk Test. Clin Nurs Res. 2006;15:107–18. doi: 10.1177/1054773805285702. [DOI] [PubMed] [Google Scholar]
- 10.Al-Lawati JA, Tuomilehto J. Diabetes risk score in Oman: A tool to identify prevalent type 2 diabetes among Arabs of the Middle East. Diabetes Res Clin Pract. 2007;77:438–44. doi: 10.1016/j.diabres.2007.01.013. [DOI] [PubMed] [Google Scholar]
- 11.Mohan V, Deepa R, Deepa M, Somannavar S, Datta M. A simplified Indian Diabetes Risk Score for screening for undiagnosed diabetic subjects. J Assoc Physicians India. 2005;53:759–63. [PubMed] [Google Scholar]
- 12.Joshi SR. Indian Diabetes Risk Score. J Assoc Physicians India. 2005;53:755–7. [PubMed] [Google Scholar]
- 13.Mohan V, Anbalagan VP. Expanding role of the Madras Diabetes Research Foundation – Indian Diabetes Risk Score in clinical practice. Indian J Endocrinol Metab. 2013;17:31–6. doi: 10.4103/2230-8210.107825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Taksande B, Ambade M, Joshi R. External validation of Indian Diabetes Risk Score in a rural community of central India. J Diabetes Mellitus. 2012;2:109–13. [Google Scholar]
- 15.Nandeshwar S, Jamra V, Pal DK. Indian Diabetes Risk Score for screening of undiagnosed diabetic subjects of Bhopal city. Natl J Community Med. 2010;1:176–7. [Google Scholar]
- 16.Bhadoria AS, Kasar PK, Toppo NA. Validation of Indian diabetic risk score in diagnosing type 2 diabetes mellitus against high fasting blood sugar levels among adult population of central India. Biomed J. 2015;38:359–60. doi: 10.4103/2319-4170.143508. [DOI] [PubMed] [Google Scholar]
- 17.Patel DN, Shah MC, Ahir GN, Amin DV, Singh MP. A study on validity of Indian Diabetes Risk Score (MDRF) for screening of diabetes mellitus among the high risk group (Policemen) of diabetes mellitus of Bhavnagar City. Innov J Med Health Sci. 2012;2:109–11. [Google Scholar]
- 18.Adhikari P, Pathak R, Kotian S. Validation of the MDRF-Indian Diabetes Risk Score (IDRS) in another south Indian population through the Boloor Diabetes Study (BDS) J Assoc Physicians India. 2010;58:434–6. [PubMed] [Google Scholar]
- 19.Mani G, Kalaivani A, Raja D. Application of Indian Diabetes Risk Score in screening of an undiagnosed rural population of Kanchipuram District, Tamil Nadu – A cross sectional survey. MRIMS J Health Sci. 2014;2:81–3. [Google Scholar]
- 20.Stanley JM, Elantamilan D, Mohanasundaram K, Kumaravel TS. Evaluation of Indian diabetic risk score for screening undiagnosed diabetes subjects in the community. Indian J Sci Technol. 2012;5:2798–9. [Google Scholar]
- 21.Rao CR, Kulkarni MM, Narayanan SS, Kamath VG, Kamath A, Ballala K, et al. Utility of Indian diabetic risk score (IDRS) in a rural area of Coastal Karnataka, India. J Evol Med Dent Sci. 2014;3:3272–7. [Google Scholar]
- 22.Chowdhury R, Mukherjee A, Saibendu KL. A study on distribution and determinants of Indian diabetic risk score (IDRS) among rural population of West Bengal. Natl J Med Res. 2012;2:282–6. [Google Scholar]
- 23.Gupta RK, Shora TN, Verma AK, Raina SK. Utility of MDRF-IDRS (Madras Diabetes Research Foundation – Indian Diabetes Risk Score) as a Tool to Assess Risk for Diabetes – A Study from North West India. 2015. [Last cited on 2015 Nov 22]. Available from: http://www.link.springer.com/article/10.1007%2Fs13410-015-0346-8 .
- 24.Ahmed A. Indian Diabetic Risk Score (IDRS), a Screening Tool for Detecting Undiagnosed Diabetes. [Last cited on 2015 Nov 22];BMR Medicine. 2015 1:1–4. Available from: http://www.bmrjournals.com/journals/Manuscript/259/Indian-diabetic-riskscore (IDRS),-Ascreening-tool-for-detcting-undiagnosed-diabetes . [Google Scholar]
- 25.Arun A, Srivastava JP, Gupta P, Sachan B, Prakash D, Zaidi ZH. Indian Diabetes Risk Score (IDRS), a strong predictor of diabetes mellitus: A cross sectional study among urban and rural population of Lucknow. Int J Appl Res. 2015;1:135–8. [Google Scholar]
- 26.Vardhan A, Adhikari P, Kotian MR, Shashidhar M, Saxena N, Gupta S, et al. The value of the Indian Diabetes Risk Score as a tool for reducing the risk of diabetes among Indian medical students. J Clin Diagn Res. 2011;5:718–20. [Google Scholar]
- 27.Sathish T, Kannan S, Sarma SP, Thankappan KR. Screening performance of diabetes risk scores among Asians and whites in rural Kerala, India. Prev Chronic Dis. 2013;10:E37. doi: 10.5888/pcd10.120131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Najeeb Q, Singh J, Pandey R, Mahajan R. A comparative study of fasting, postprandial blood glucose and glycated hemoglobin for diagnosing diabetes mellitus in staff members of MMIMSR, Mullana, Ambala. Med J DY Patil Univ. 2015;8:158–64. [Google Scholar]