

Abstract
Background
Mantle cell lymphoma (MCL) is an aggressive disease, with poor prognosis and a limited survival. However, some patients with indolent MCL can survive beyond 7~10 years. These patients remain largely asymptomatic and can be in observation for a long time without any treatment. The process of “wait and watch” leaves these patients with the potential risk of evolution to classic, aggressive MCL. On the other hand, early treatment for these patients may not impact overall survival but rather affects the quality of life. Therefore, it is essential to clearly identify this type of indolent MCL at the time of diagnosis.
Results
Reported findings of indolent presentation of MCL include: lack of B symptoms, normal serum lactic dehydrogenase (LDH) and β2-microglobulin levels (β2M), low MCL-International Prognostic Index (MIPI) score, maximum tumor diameter less than 3 cm, spleen size < 20 cm, positron emission tomography/computerized tomography with the Standard Uptake Value max <6, Ki-67 less than 30%, with some particular immunophenotype, such as CD5 and CD38 negative, markedly increased CD23 positive lymphocytes proportions, high expression of CD200, kappa light chain restriction, without C-myc, TP53 and NOTCH1/2 mutations, non-blastoid/pleomorphic histology, and no tumor growth on reevaluation every 2~3 months (followed for at least 6 months). Imaging evaluation may only be performed in the presence of disease-related symptoms or organ involvement. Meanwhile, if novel nodal or extranodal lesion is found, biopsy is mandatory to exclude lymphoma.
Common clinopathological forms of indolent presentations include monoclonal B lymphocytosis with t (11; 14); “indolent leukemic” presentation of MCL with involvement of peripheral blood, bone marrow involvement, splenomegaly, and minimal lymphadenopathies and in situ lymphoma (often found in lymph nodes removed for other reasons, and in gastrointestinal biopsies).
Conclusions
Considering these distinct indolent clinical presentations with particular features in cytology and gene mutational status, we propose to include these MCL clinical presentations under the umbrella of “Smoldering Mantle Cell Lymphoma”.
Keywords: Mantle cell lymphoma, Indolent MCL, Smoldering lymphoma
Background
Mantle cell lymphoma (MCL) is an aggressive disease, with a poor prognosis and limited survival [1]. However, up to 30% of MCL patients may have an indolent clinical course [2, 3], with survival exceeding 7~10 years [4]. These asymptomatic patients can survive despite no initial treatment using the “wait-and-watch” approach. The clear ability to differentiate between the aggressive and indolent MCL types is necessary to guide and choose which therapeutic approach should be administered. However, no established criteria are currently used to inform the treatment decision-making process for MCL patients with the indolent clinical course. Consequently, criteria for indolent MCL would help identify patients who are at risk of early progression and who are in need of immediate therapy, sparing patients from toxic treatment.
The classification and nomenclature of such indolent MCL cases remain unclear. The terms “classical MCL”, “subclinical disease”, “preclinical phase” or even “benign lymphoma” have been used previously [5]. Another report coined the term “non-nodal type of MCL” or “indolent leukemic presentation” [6]. We propose to unify all of the indolent MCL presentations under the title of “Smoldering Mantle Cell Lymphoma (SMCL)” to emphasize its initial indolent behavior and its predisposition to develop into a more clinically aggressive lymphoma. We propose that the following parameters can be used to define SMCL: lack of B symptoms, normal serum lactic dehydrogenase and β2-microglobulin levels; low MCL-International Prognostic Index (MIPI) score, maximum tumor diameter < 3 cm, spleen size <20 cm, Positron Emission Tomography/computerized tomography (PET/CT) with the Standard Uptake Value (SUV) max <6; Ki-67 < 30%; absence of c-myc, TP53 and NOTCH1/2 mutations, non-blastoid/pleomorphic histology; and no tumor growth on re-evaluation every 2~3 months (followed for at least 6 months). Imaging evaluation may only be performed in the presence of disease-related symptoms or organ involvement. If novel nodal or extranodal lesion is found, biopsy is mandatory to exclude lymphoma. Meanwhile, the full understanding of this definition will evolve as the genetics and heterogeneity underlying MCL progression are better understood and as potential biomarkers are uncovered. Furthermore, in this molecular era with the advent of big data and detailed DNA/RNA/proteomics analysis, more precise guidance regarding this classification will be available in the foreseeable future.
Proposed clinical features of SMCL (Table 1)
Table 1.
Comparison of clinical, morphology, immunophenotype and genetics features between SMCL and classic MCL
| SMCL | Classic MCL | |
|---|---|---|
| Clinical features | ||
| B symptom | without | with or without |
| Serum LDH | normal | elevated or normal |
| Serum β2-MG | normal | elevated or normal |
| MIPI | low risk | low to high risk |
| Ki-67 | < 30% | ≥30% |
| Max tumor diameter | < 3 cm | ≥3 cm |
| SUV of PET/CT | ≤ 6 | > 6 |
| evaluation every 3 mons | no tumor growth | having tumor growth |
| Morphology | ||
| Origin | germinal or post-germinal center | antigen-naïve pregerminal center |
| Cytology | non-blastoid/pleomorphic | small cell, classic, pleomorphic, or blastic |
| Immunophenotype | ||
| CD5 | low | high |
| CD38 | low | high |
| CD23 | high | low |
| CD200 | high | low |
| light chain restriction | kappa | lambda |
| Genetics | ||
| TP53 | low | high |
| NOTCH1/2 | low | high |
| C-myc | low | high |
| Cyclin D1 mRNA | low | high |
| Cell cycle | G1 or before | S |
MCL mantle cell lymphoma, LDH lactic dehydrogenase, β2-MG β2-microglobulin, MIPI mantle cell lymphoma International prognostic index, Max maximum, SUV standardized uptake value, PET/CT positron emission tomography/computerized tomography
MIPI, Ki-67 proliferation marker
In 2008, the MIPI scoring criteria were established to enable the stratification of clinically diverse MCL patients into three risk groups: low risk, intermediate risk and high risk The MIPI criteria include the following 4 independent pre-treatment prognostic factors: age, Eastern Cooperative Oncology Group performance status, pre-treatment ratio of actual/upper limits of normal for lactate dehydrogenase (LDH), and pre-treatment white blood cell (WBC) counts [7]. In this report, patients with a score of 3 or less were said to have indolent disease and could defer therapy for a median of 1 year. Moreover, once these patients began therapy, the patients showed more sensitivity to treatment, with a 5-year median survival of 60%. This risk model has been validated in other retrospective and prospective clinical publications [8, 9]. In addition to these variables, tumor proliferation is recognized as one of the strongest biological prognostic factors in MCL, and high tumor cell proliferation indicates shorter survival [10]. In order to predict MCL survival, a mathematical model was established [11]. The quantitative model combining 20 different expression levels of proliferation genes in MCL was used to determine the extent of proliferation. The proliferation signature average was inversely correlated with survival with high statistical significance not only in the training set (p = 1.92X10−5) but also in the validation set (p = 7.44 X10−5). Additionally, this signature average was correlated with the number of Ki67-positive cells (r = 0.69), which is an immunohistochemistry (IHC) marker of proliferative index. The IHC Ki-67 data is not as strong but is readily available in clinical practice and also correlated with OS [12, 13]. Hoster et al. reported that significant differences in time to treatment failure (64 months versus 19 months) and overall survival (OS) (not reached versus 45 months) were found between the Ki-67 level < 30% group versus the Ki-67 level ≥ 30% group in 543 MCL cases (p < 0.0001 each) [12]. Later, the Ki-67 index and MIPI were combined and modified to create the MIPI-c. This newer scoring criteria separated four groups of 508 patients with the following varying 5-year OS rates: 85, 72, 43, and 17% (P < .001) and was more discriminative than the MIPI criteria alone [14]. We believe that the MIPI-c scoring system should be used to diagnose SMCL, with SMCL scored as a low MIPI score ≤ 3 and a Ki-67 index <30%.
Tumor size
According to the Goldie-Coldman hypothesis, the probability that a cancer contains drug-resistant clones depends on the size of the tumor and the mutation rate. Larger tumor masses have a more heterogeneous tumor cell population, which can lead to chemotherapy resistance [15]. Additionally, decreased vascularity in the center of larger tumor masses may result in less exposure to chemotherapeutic agents. Several studies have suggested that larger tumor size acts an adverse prognostic factor [16–18], and various studies have shown tumor sizes can range from 5~10 cm. In other reports, patients with a higher tumor volume had inferior complete remission rates and higher relapse rates [19, 20]. In patients with stage 1 and 2 tumors who only received radiotherapy, one study found that patients with maximum tumor diameter < 3 cm had a local recurrence rate of 5% compared with 18% for those patients with a maximum tumor diameter ≥ 3 cm [21]. Thus, we define the threshold for tumor size at 3 cm for patients in early stage of the disease showing indolent clinical behavior in SMCL. This definition of <3 cm stems primarily from clinical intuition and over 20 years in the clinic rather than statistical data.
Spleen size
Spleen size is significantly influenced by body height and sex [22]. Splenomegaly occurs frequently in MCL patients, with a spleen measured beyond 15 cm in its longest dimension considered enlarged, and spleen size larger than 20 cm considered significant. Here, we define the upper threshold of enlargement of spleen size in SMCL as 20 cm. If spleen size is less than 20 cm, and the patient is without symptoms related to the enlarged spleen such as shortness of breath, early satiety, gastric reflux, walking problems and left upper quadrant pain, no treatment is necessary. We emphasize that an enlarged spleen may cause cytopenia, with the patient at risk for spontaneous rupture and infarction [23, 24]; therefore, we recommend that MCL patients with spleen size above 20 cm should undergo treatment.
PET/CT standard SUV
Previous data showed that low SUV observed with PET/CT correlated with an indolent clinical process [25–27]. In a retrospective study, MCL patients with a PET SUVmax <5 had better OS and FFS (87.7% vs. 34%, 45.3 m vs. 10.6 m, P < 0.01 and <0.001, respectively) [26]. Other studies have suggested that SUV combined with IPI can enhance the stratification and predict prognosis at the time of diagnosis [27]. MCL patients with IPI ≤ 2 and SUVmax ≤6 (low-risk, n = 9, 29%) were found to have the best event-free survival (EFS) compared to those with IPI > 2 or SUVmax >6 (intermediate-risk group, n = 13, 42%), IPI > 2 and SUVmax >6 (high risk, n = 9, 29%). At a median follow-up of 21 months, no relapse has been observed in the low-risk group, while the median EFS durations in the intermediate- and the high-risk groups were 37 and 22 months, respectively (p = .004) [27]. We propose, based on the latter, to include this PET value in the definition of SMCL at a SUVmax <6 with PET/CT.
Therefore, the clinical characteristics of SMCL should include the following: low MIPI scores, Ki-67 < 30%, maximum tumor diameter less than 3 cm and low SUV of PET/CT. In addition, we believe that the SMCL diagnostic factors should also include a lack of B symptoms [28], normal serum LDH [7, 29] and β2-microglobulin levels [28, 30], spleen size <20 cm and no tumor growth on reevaluation every 3 months (followed up for at least 6 months) [28].
Biologic markers
Cytology
MCL has the following 4 cytological classifications: classic, small-cell, pleomorphic, or blastic [1, 31]. Blastoid or pleomorphic variants are generally characterized by a more aggressive clinical course, higher proliferation rate and worse prognosis [32–35]. Meanwhile, the blastoid morphology is associated with TP53 mutations, c-myc gene abnormalities [36, 37], complex karyotype, and high cyclin D1 mRNA levels [38], which are all indicative of high proliferation and inferior survival [38]. The median OS for MCL patients with the blastoid variant has been reported at only 11–14.5 months [39, 40]. Additionally, the median survival time for patients whose MCL transformed from nodular or diffuse to blastoid was only 3.8 months [95% Confidence Interval (CI): 2.4–5.2 months] as compared with 26 months following the latest rebiopsy in patients without transformation (95% CI: 17–35 months, P < 0.001) [39]. The pleomorphic variant of MCL is composed of numerous large cells with irregular nuclear contours and prominent nucleoli [41], mimicking diffuse large B-cell lymphoma [42], which is also considered as an aggressive variant with c-myc gene mutations [43].
Thus, we conclude that SMCL should be the non-pleomorphic/blastic variants. Except regarding cytology, here, we would not dwell on histology because all 3 clinical presentations of SMCL have no nodes, which we can assess architecture to label the presentation as mantle zone or follicular or diffuse.
Immunophenotype
In order to explore the difference in immunophenotypic behavior between the indolent MCL and typical MCL, Espinet B, et al. measured the expression of CD38/CD200 by cytometry in non-nodal cases with cyclin D1–positive monoclonal asymptomatic lymphocytosis (MALD1) and typical MCL [44]. The B cells showed a significantly higher expression of CD38 in 24 cases of typical MCL. (median, 89%; range, 0–100%), compared to that of the 13 cases of MALD1 (median, 14%; range 0–35%). Low or absent expression of CD200 in B cells was found in 15 cases of typical MCL whereas higher expressions of CD200 positive B cells were detected in the 12 cases of MALD1. These results were also confirmed by qRT-PCR analysis. Thus, CD38 combined with CD200 could be helpful to differentiate MBL with t (11;14) from typical MCL.
High expression of CD38 in typical MCL suggest that CD38 may contribute to the survival of B cell neoplasm via adhesion molecules such as CD31 [45]. Low expression of CD38 in MALD1 may weaken the interaction between MALD1 B cells and micro vessels with CD31 expression, which result in reduced accumulation of clonal B cells. Expression of CD200 is decreased in all typical MCL, while it is highly expressed in most MALD1. CD200 binding to its receptor CD200R may produce inhibitory signals, which can cause reduced B cell proliferation. This is thought to play a crucial role of preventing overproduction of tumor cells and maintaining asymptomatic condition over a long period of time in MALD1. Conversely, with decreased expression of CD200, inhibitory signals for B cells are lost which causes uncontrolled B cell proliferation leading to the transformation of an indolent condition to an aggressive one [46].
In addition, the CD5 of a typical MCL is usually positive, however, a small subgroup of patients with MCL may have a negative CD5. The peripheral blood of such patients has atypical lymph cells, with or without lymphocytosis or lymphadenopathy, or splenomegaly, but with indolent clinical process [47].
Genetics
In the pathogenesis of MCL, CCND1 appears to be a weak oncogene. Therefore, the clinical aggressiveness of MCL is possibly associated with a secondary abnormal cytogenetic event. MCL has a highly unstable genome, which may lead to recurrent abnormalities, including loss of chromosome 1p, 8p, 9p (CDKN2A, CDKN2B), 9q, 11q (ATM), 13q14 and 17p (TP53) or addition of 3q, 8q (MYC), 10p (BMI1), 15q, and 18q. These mutations may cause damage to DNA repair [48] and contribute to hyperproliferative mutations [49, 50]. Although IGH/CCND1 rearrangement is the most crucial initial event, additional gene mutations or the addition of aberrant cytogenetic event are necessary to destabilize the indolent lymphoma. A previous study demonstrated that the genes involved in this destabilization process may be INK4a/CDK4/RB1, ARF/MDM2/p53, Cyclin D1/cdk4 (6) kinases, cyclin E/cdk2 kinase and p16INK4a, and others [11, 51, 52]. However, the mechanism is generally complicated, which needs to be further elucidated. Moreover, the time necessary for the accumulation of sufficient lesions to develop classic MCL remains unknown.
IGVH mutational status
MCL originates from antigen-naïve pre-germinal center B cells located in the mantle zone surrounding the germinal center [1, 53]. Cells from the mantle zone display high clonal diversity and express germline Ig heavy chain (IgH) V genes [54]. In contrast, in the germinal center, few B-cell clones have intraclonal diversity via somatic hypermutations in the VH region genes. MCL generally expresses VH genes, without any or minimal somatic mutations. Of particular importance, indolent MCL (70%) demonstrates significantly higher hypermutated immunoglobulin gene rearrangements compared with classical MCL (~20%) [55], suggesting that indolent MCL has germinal center or post-germinal center origin [56]. Orchard et al. found that IGVH gene mutation rates in leukemic MCL are much higher than that in nodal MCL among the 80 cases of MCL studied [57]. However, the clinical significance of IGVH gene rearrangement in MCL remains dubious. Most studies have shown no correlation with IGVH rearrangement with the outcome of the patients [58–60], in other cases, longer survival in MCL with IGVH rearrangement has been observed [61–63]. Therefore, IGVH gene mutation status is not included in the definition of SMCL.
SOX-11
In classic aggressive MCL, the neural transcription factor SOX11 gene is aberrantly expressed [56]. The prognostic role of SOX11 have shown conflicting results. SOX11 was correlated with improved survival, which was reported in two studies with cohorts of 53 and 186 MCL patients, respectively [55, 64–66]. In contrast, a negative correlation between SOX11 and better survival was reproted in two other series [55, 66]. In the recent Nordic MCL data, SOX11 was proposed to be routinely assessed with TP53 and patients with high SOX11 expression had superior OS and EFS compared to patients with low SOX11 expression [8]. However, at Lugano conference in 2017, SOX11 has no prognostic value in MCL [67]. Thus, SOX11 is not included in the definition of SMCL.
TP-53
TP53 dysfunction gives rise to mutant protein that affects the generation, development and progression of diffuse large B cell lymphoma. In essence, TP53 mutations lead to irregular B-cell phenotypes and are associated with poor overall survival [68]. TP53 has also been shown to be associated with significant independent molecular markers that are correlated with dismal outcomes [38, 69–71]. Furthermore, as demonstrated at Lugano conference in 2017, TP53 but not SOX11 immunohistochemistry has prognostic value independent of MIPI and Ki-67 [67]. In this study, MCL patient samples were sorted into four categories according to different percentage of P53 immunohistochemistry staining (0%, 1–10%, 11–50% and >50%). The results showed that TP53 deletion (0%) had no significant influence on the TTF and OS of MCL patients (p = 0.10, HR = 1.45 and p = 0.18, HR = 1.46, respectively), while TP53 mutations (>50%) are highly predictive for short time to treat failure (TTF) and poor OS (both p < 0.0001; HR 2.47 and 3.00).
Therefore, the TP53 mutational status needs to be routinely tested to define and diagnose SMCL.
NOTCH 1/2
NOTCH1/2 mutations accounted for 5~12% of MCL [72, 73]. The deregulation of NOTCH pathway is implicated in developmental disorders and oncogenesis [72]. In MCL cell lines, the inhibition of the NOTCH pathway resulted in reduced proliferation and/or increased apoptosis [72]. NOTCH1 mutations in MCL patients correlated significantly with poor OS [72]. Bea et al. found that NOTCH2 mutations are also significantly associated with poor clinical outcome using whole-genome/whole-exome analysis in 39 MCL and subsequent validation in and additional 172 cases [73]. Thus MCL with NOTCH1/2 mutations should also be rule out from SMCL.
MYC
The MYC oncogene can activate cell growth and cell cycle progression gene transcription [74, 75]. MCL with MYC mutations is associated with blastoid /pleomorphic morphology, indicating a poor prognosis [36, 76–78]. In a study of 65 patients with MCL [78], MYC mutations were higher in blastoid/pleomorphic MCL variants (mean, 19.0%) than in classic MCL (mean, 1.9%; P < 0.001). Also, high MYC mutations were significantly associated with higher expression of p53 and Ki-67 and shortened OS and PFS (all P < 0.05). Accordingly, MYC mutation is included in the definition of SMCL.
Genetic profiling
Ideally, a combination of the proliferation gene expression signature with different oncogenes related to the MCL cell cycle could provide further information regarding biological behavior of MCL and better guide its management. As early as 2003, Rosenwald et al. had reported that increased cyclin D1 mRNA expression levels combined with INK4a/ARF locus deletions correlated with increased proliferation rate and shorter survival [11]. The MKI67 gene that encodes the important proliferation marker Ki-67 was shown to be independently prognostic, even with modern therapies [79, 80]. Furthermore, in order to bypass the need for fresh tissue for pathologic analysis, a 17-gene proliferation signature based on the MKI67 gene and analyzed by nanostring in formalin-fixed paraffin-embedded (FFPE) has been reported. This assay (MCL35) assigned patients to high-risk (26%), standard-risk (29%), and low-risk (45%) groups, with median OS of 1.1, 2.6, and 8.6 years, respectively (p < .001), and this was independent of MIPI risk assessment.The analytic and clinical validity of this assay provide a reliable biomarker to support risk-adapted clinical trials [81].
Common clinopathological forms of SMCL (Fig. 1)
Fig. 1.
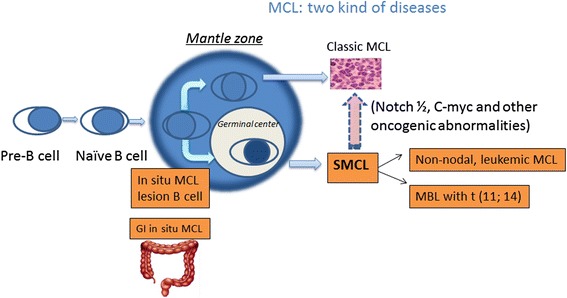
MCL actually can be divided into two kinds of disease entities: classic MCL and SMCL. SMCL includes the following hypothetical models: MBL with t (11; 14), non-nodal leukemic MCL and in situ MCL, especially GI in situ MCL. SMCL, smoldering mantle cell lymphoma; MBL, monoclonal B lymphocytosis; GI, gastrointestinal
Monoclonal B lymphocytosis (MBL) with t (11;14) (q13; q32) and cyclin D1-positive (MALD1)
With the advent of flow cytometry, monoclonal lymphocytes can be found in up to 3.5~12% of healthy population aged over 40 years old [82–88]. “Monoclonal B-lymphocytosis” (MBL) is defined as the count of B-lymphocytes in the peripheral blood less than 5000/ul [89], with lack lymph node or organ enlargement, cytopenias, or disease-related symptoms [90]. Additional features of MBL include overall kappa: lambda ratio > 3:1 or <0.3:1, or >25% B cells with absent or low expression of surface immunoglobulin or a disease-specific immunophenotype, and clinical stability over a 3-month period at follow-up. Different counts of B cells are usually related to varied clinical conditions. High-count MBL is considered as a pre-neoplastic condition, which may progress into other B cell neoplasms like chronic lymphocytic leukemia (CLL). However, a low-count state of MBL does not usually develop into leukemia, although the disease can be present for many years [91].
Asymptomatic MBL with t (11; 14) (q13; q32) and cyclin D1-positive (MALD1) is very rare, accounting for only 3% of all MCL diagnosed [44, 92]. MALD1 usually without enlargement of the lymph node and spleen, has a very indolent clinical process without treatment, with survival for up to 9 years [44, 47, 55, 87]. MALD1 has a different phenotype and gene expression profile when compared with typical MCL, with a high rate of IGVH gene mutations, lack of genomic complexity, and absence of expression of transcription factors of the high-mobility genes [55]. The gene signature of MALD1/MCL showed CD200 upregulated in MALD1 and CD38 upregulated in MCL [44]. Pathway analysis using the Ingenuity Pathway Analysis tool indicated that the expression of gene sets of the MALD1 is related to immune activation and inflammatory responses, while those of typical MCL are related to neoplastic behavior and cell proliferation [44].
Thus, we propose to classify MALD1 as SMCL. However, the SMCL like asymptomatic MBL with t (11; 14) and Cyclin D1 expression is different from typical MCL in phenotype and gene expression profile, which may have high rate of IGVH gene mutations, lack of genomic complexity, and absence of expression of transcription factors of the high-mobility genes [55].
Non-nodal, leukemic MCL (CLL-type MCL)
Elevated leukocyte counts in the MIPI of conventional MCL, as a leukemic presentation, is a feature of adverse prognosis [7]. However, mantle cell leukemia may have two different clinical courses: aggressive and indolent [55, 93]. Ondrejka et al. retrospectively analyzed 8 cases of MCL presented as leukemic forms beyond 10 years. These cases were like CLL, with mild lymphocytosis and without lymphadenopathy and splenomegaly. All cases had positive t (11:14) with considerable proportion of CD23 positive cells, and kappa light chain restriction, while typical MCL cells are generally CD23 negative and lambda light chain restricted. These patients had a long-term stable disease or the lymphocyte counts increased very slowly. After a median follow-up of 27 months, 7 patients survived, including 2 which needed some form of treatment.
Orchard et al. identified a higher incidence of mutated IGVH genes in 22 of 34 (66%) leukemic nonnodal MCL cases compared with 3 of 31 (10%) nodal MCL cases. The positive rate of CD38 in the nodal MCL group was significantly higher than that of the leukemic non-nodal group. The clinical manifestations of these leukemic patients were more like the indolent subtype than the nodal MCL patients [57].
These rare asymptomatic cases are akin to classic MCL in respect to immunohistochemistry and cytogenetics. However, these cases presented as leukemic forms, sometimes with splenomegaly, but without abnormal lymph node architecture. Such leukemic MCL cases have shown an indolent clinical course [6, 47, 52, 92], which have other features like:mutated immunoglobulin genes, low CD38 expression, lack of CD5 expression, and a low number of genomic aberrations [55, 57, 66, 92, 94]. So far, it is not clear that these asymptomatic cases are at the early stage of MCL development or a fully developed leukemic form of an MCL of indolent course. Thus, we classify non-nodal, leukemic MCL as SMCL.
In situ MCL
This new addition in the 2016 revision of the World Health Organization (WHO) classification of lymphoid neoplasms [95] is typically characterized by the presence of cyclin D1+ cells in the inner mantle zones of follicles, and is often found incidentally [96].
In situ MCL is rare and has an indolent clinical behavior [47, 94, 97–100]. Furthermore, the lymph node structure of “in situ MCL” is intact, so it can only be diagnosed by the detection of cyclin D1 with immunohistochemistry analysis [44, 91, 96, 100, 101]. Generally, “in situ MCL” cases are incidentally found by reevaluation of the previous samples of MCL patients. Racke et al. analyzed the “negative” lymph node samples 2–15 years prior to the diagnosis of 7 cases of MCL, and “in situ MCL” were found in all cases [102]. These early lesions occurred 2–86 months prior to the diagnosis of classic lymphoma, which were characterized by small groups of cyclin D1-positive lymphocytes in the mantle zone of lymph node or extra nodal tissue. After a follow-up study of “in situ MCL”, Carvajal-Cuenca A, et al. found that most of patients may not develop into classic MCL until a long period ranging from 1 to 19.5 years without any treatment [96].
“in situ MCL” is very low risk for the development of classic MCL, however, the acquired alterations in the DNA damage response pathway, such as ataxia-telangiectasia mutated (ATM), or cell cycle checkpoint kinase 2 (CHK2) inactivating mutations may facilitate the development of the tumor [53]. In addition, “in situ MCL” need to be differentiated from MCL with a mantle zone pattern and classic MCL, in that “in situ MCL” usually do not need any therapeutic intervention. Therefore, “in situ MCL” can be classified as another subtype of SMCL.
Gastrointestinal tract in situ MCL
Most patients with MCL have the gastrointestinal (GI) tract involvement, which manifest in a variety of forms, such as multiple lymphomatous polyposis (MLP) or a slight mucosal change [103, 104]. Primary GI involvement of MCL is rare, which accounts for 4 ~ 9% of GI B-cell non-Hodgkin lymphomas [105]. Some patients with primary GI tract MCL may have very indolent clinical process and good survival [106].
Neto, A. G. et al. reported a case of GI tract in situ MCL [107]. A colonoscopic biopsy following bright red blood per rectum showed benign colonic mucosa. Two years later, the patient had ileocolic intussusception related to enlarged lymph nodes and was confirmed as widespread MCL. Reevaluation of initial colonic biopsies showed cyclin D1–positive cells within small lymphoid aggregates, which were confirmed by FISH for t (11; 14). After chemotherapy, the residual disease had positive cyclin D1 staining and FISH t (11; 14) in mantle zone, which was like the initial lesions. Thus, the initial colonic lesions may be an in-situ GI MCL.
However, it is very difficult to find GI in situ lymphoma at the early onset. Histologically, the lymphoid follicular structure of colonic mucosa remains intact or only shows minimal changes due to ubiquitous lymphoid aggregates in GI tract. However, it is noteworthy that the possibility of lymphoma needs to be excluded by immunohistochemistry if the uniform size of lymph cells and nuclear irregularities are noticed [107].
Treatment strategies
The treatment approach for SMCL is profoundly influenced by the concomitant coexistence or not of an overt or classic MCL (Table 1). For patients without evidence of overt lymphoma, a “watch and wait” strategy is strongly suggested and overtreatment may be avoided [47]. Compared with other indolent lymphoma, the more aggressive behavior of overt MCL could suggest a closer follow-up. A follow-up strategy include evaluation every 3 months (at least 6 months) for MIPI scores, imaging study, morphology and pathological biopsies. However, due to the feasibility of clinical practice, imaging evaluation may only be performed in the presence of disease-related symptoms or organ involvement. Meanwhile, if novel nodal or extranodal lesion is found, biopsy is mandatory to exclude lymphoma. Generally, there are no indications to start treatment in “in situ” MCL patients, without clear evidence of concomitant or subsequent overt MCL.
However, early detection and treatment may improve the prognosis of MCL in the event of high risk mutation, such as C-myc, TP53 and NOTCH1/2 mutation, etc., and the transformation of histotype, progression of stage and localization of overt lymphoma.
Conclusions
We coined the term “SMCL” for the asymptomatic MCL cases with indolent clinical behavior. Our proposed definition of SMCL is: lack of B symptoms, normal serum LDH and b2-microglobulin levels, low MIPI score, maximum tumor diameter less than 3 cm, spleen size < 20 cm, PET/CT with the SUVmax <6, Ki-67 less than 30%, with some particular immunophenotype, such as CD5 and CD38 negative, markedly increased CD23 positive lymphocytes proportions (typical MCL usually has negative CD23), high expression of CD200, kappa light chain restriction (Typical MCL usually has lambda light chain restriction), without C-myc, TP53 and NOTCH1/2 mutation, nonblastoid/pleomorphic histology, and no tumor growth on reevaluation every 3 months, at least 6 months. The common clinical and pathological forms of SMCL may include MBL with t (11;14), nonnodal leukemic MCL and in situ lymphoma (including GI in situ lymphoma).
These clinical and pathological forms remain stable or grow very slowly over a long period of time without any symptoms or with only mild clinical symptom. It may take up to 12~15 years for SMCL progress to classic MCL. Thus, unnecessary treatment which can bring potential harm to patients can be avoided. Importantly, close observation is still needed. Some SMCL may need early intervention in order to avoid transformation to classic MCL. In addition, the mechanism of transformation from SMCL to classic MCL is not very clear, which may be partly due to additional genetic mutations which include 17p/TP53, NOTCH1/2, C-myc, or other gene mutations.
Acknowledgements
Not applicable.
Funding
This work was supported by the generous philanthropic contributions to The University of Texas MD Anderson Moon Shots Program. This work was also supported by Zhejiang Provincial Natural Science Foundation of China (LY13H080003) to Y.H.G.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Disclosure
Neither the submitted manuscript nor any similar manuscript, in whole or in part, other than an abstract, is under consideration, in press, published, or reported elsewhere.
Abbreviations
- ATM
Ataxia-telangiectasia mutated
- CHK2
Cell cycle checkpoint kinase 2
- CLL
Chronic lymphocytic leukemia
- EFS
Event-free survival
- FFPE
Formalin-fixed paraffin-embedded
- GI
Gastrointestinal
- IgH
Ig heavy chain
- LDH
Lactic dehydrogenase
- MBL
Monoclonal B-lymphocytosis
- MCL
Mantle cell lymphoma
- MIPI
Low MCL-International Prognostic Index
- MLP
Multiple lymphomatous polyposis
- OS
Overall survival
- PET/CT
Positron Emission Tomography/computerized tomography
- SMCL
Smoldering mantle cell lymphoma
- SUV
Standard Uptake Value
- WBC
White blood cell
- WHO
World Health Organization
- β2M
β2-microglobulin levels
Authors’ contributions
MW designed this review. HY and AD performed the selection of literature, drafted the manuscript, and prepared the figures. DZ collected the related references and participated in the discussion. MA and KN revised the manuscript. All authors contributed to this manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Haige Ye, Email: haigeye@gmail.com.
Aakash Desai, Email: dr.aakashdesai@gmail.com.
Dongfeng Zeng, Email: gebeidandan@sina.com.
Krystle Nomie, Email: KJNomie@mdanderson.org.
Jorge Romaguera, Email: jromague@mdanderson.org.
Makhdum Ahmed, Email: MAhmed5@mdanderson.org.
Michael L. Wang, Phone: (713) 792-2121, Email: miwang@mdanderson.org
References
- 1.Sabattini E, Bacci F, Sagramoso C, Pileri SA. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica. 2010;102(3):83–87. [PubMed] [Google Scholar]
- 2.Martin P, Chadburn A, Christos P, et al. Outcome of deferred initial therapy in mantle-cell lymphoma. J Clin Oncol. 2009;27(8):1209–1213. doi: 10.1200/JCO.2008.19.6121. [DOI] [PubMed] [Google Scholar]
- 3.Eve HE, Furtado MV, Hamon MD, Rule SA. Time to treatment does not influence overall survival in newly diagnosed mantle-cell lymphoma. J Clin Oncol. 2009;27(32):e189–e190. doi: 10.1200/JCO.2009.23.9731. [DOI] [PubMed] [Google Scholar]
- 4.Furtado M, Rule S. Indolent mantle cell lymphoma. Haematologica. 2011;96(8):1086–1088. doi: 10.3324/haematol.2011.047357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ganapathi KA, Pittaluga S, Odejide OO, Freedman AS, Jaffe ES. Early lymphoid lesions: conceptual, diagnostic and clinical challenges. Haematologica. 2014;99(9):1421–1432. doi: 10.3324/haematol.2014.107938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Royo C, Navarro A, Clot G, et al. Non-nodal type of mantle cell lymphoma is a specific biological and clinical subgroup of the disease. Leukemia. 2012;26(8):1895–1898. doi: 10.1038/leu.2012.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hoster E, Dreyling M, Klapper W, et al. A new prognostic index (MIPI) for patients with advanced-stage mantle cell lymphoma. Blood. 2008;111(2):558–565. doi: 10.1182/blood-2007-06-095331. [DOI] [PubMed] [Google Scholar]
- 8.Nordstrom L, Sernbo S, Eden P, et al. SOX11 and TP53 add prognostic information to MIPI in a homogenously treated cohort of mantle cell lymphoma--a Nordic lymphoma group study. Br J Haematol. 2014;166(1):98–108. doi: 10.1111/bjh.12854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Geisler CH, Kolstad A, Laurell A, et al. The mantle cell lymphoma international prognostic index (MIPI) is superior to the international prognostic index (IPI) in predicting survival following intensive first-line immunochemotherapy and autologous stem cell transplantation (ASCT) Blood. 2010;115(8):1530–1533. doi: 10.1182/blood-2009-08-236570. [DOI] [PubMed] [Google Scholar]
- 10.Klapper W, Hoster E, Determann O, et al. Ki-67 as a prognostic marker in mantle cell lymphoma-consensus guidelines of the pathology panel of the European MCL network. J Hematop. 2009;2(2):103–111. doi: 10.1007/s12308-009-0036-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rosenwald A, Wright G, Wiestner A, et al. The proliferation gene expression signature is a quantitative integrator of oncogenic events that predicts survival in mantle cell lymphoma. Cancer Cell. 2003;3(2):185–197. doi: 10.1016/s1535-6108(03)00028-x. [DOI] [PubMed] [Google Scholar]
- 12.Klapper W, Hoster E, Determann O, et al. Ki-67 as a prognostic marker in mantle cell lymphoma—consensus guidelines of the pathology panel of the European MCL Network. Journal of Hematopathology. 2009;2(2):103-111. doi:10.1007/s12308-009-0036-x. [DOI] [PMC free article] [PubMed]
- 13.Determann O, Hoster E, Ott G, et al. Ki-67 predicts outcome in advanced-stage mantle cell lymphoma patients treated with anti-CD20 immunochemotherapy: results from randomized trials of the European MCL network and the German low grade lymphoma study group. Blood. 2008;111(4):2385–2387. doi: 10.1182/blood-2007-10-117010. [DOI] [PubMed] [Google Scholar]
- 14.Hoster E, Rosenwald A, Berger F, et al. Prognostic value of Ki-67 index, cytology, and growth pattern in mantle-cell lymphoma: results from randomized trials of the European mantle cell lymphoma network. J Clin Oncol. 2016;34(12):1386–1394. doi: 10.1200/JCO.2015.63.8387. [DOI] [PubMed] [Google Scholar]
- 15.Goldie JH, Coldman AJ. A mathematic model for relating the drug sensitivity of tumors to their spontaneous mutation rate. Cancer Treat Rep. 1979;63(11–12):1727–1733. [PubMed] [Google Scholar]
- 16.Jagannath S, Velasquez WS, Tucker SL, et al. Tumor burden assessment and its implication for a prognostic model in advanced diffuse large-cell lymphoma. J Clin Oncol. 1986;4(6):859–865. doi: 10.1200/JCO.1986.4.6.859. [DOI] [PubMed] [Google Scholar]
- 17.Shipp MA, Harrington DP, Klatt MM, et al. Identification of major prognostic subgroups of patients with large-cell lymphoma treated with m-BACOD or M-BACOD. Ann Intern Med. 1986;104(6):757–765. doi: 10.7326/0003-4819-104-6-757. [DOI] [PubMed] [Google Scholar]
- 18.Danieu L, Wong G, Koziner B, Clarkson B. Predictive model for prognosis in advanced diffuse histiocytic lymphoma. Cancer Res. 1986;46(10):5372–5379. [PubMed] [Google Scholar]
- 19.Cabanillas F, Burke JS, Smith TL, Moon TE, Butler JJ, Rodriguez V. Factors predicting for response and survival in adults with advanced non-Hodgkin's lymphoma. Arch Intern Med. 1978;138(3):413–418. [PubMed] [Google Scholar]
- 20.Fisher RI, DeVita VT, Jr, Johnson BL, Simon R, Young RC. Prognostic factors for advanced diffuse histiocytic lymphoma following treatment with combination chemotherapy. Am J Med. 1977;63(2):177–182. doi: 10.1016/0002-9343(77)90230-3. [DOI] [PubMed] [Google Scholar]
- 21.Cox JD, Koehl RH, Turner WM, King FM. Irradiation in the local control of malignant lymphoreticular tumors (non-Hodgkin's malignant lymphoma) Radiology. 1974;112(1):179–185. doi: 10.1148/112.1.179. [DOI] [PubMed] [Google Scholar]
- 22.Chow KU, Luxembourg B, Seifried E, Bonig H. Spleen size is significantly influenced by body height and sex: establishment of normal values for spleen size at US with a cohort of 1200 healthy individuals. Radiology. 2016;279(1):306–313. doi: 10.1148/radiol.2015150887. [DOI] [PubMed] [Google Scholar]
- 23.Tan CB, Rajan D, Majeed S, Ahmed S, Freedman L, Mustacchia P. Pathologic rupture of the spleen in mantle-cell-type non-Hodgkin's lymphoma. Case Rep Med. 2012;2012:351275. doi: 10.1155/2012/351275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Boddana PV, Tomson CR, Austen B, Davies S, Francis N, White H, Rooney N. A case of lymphoma presenting as splenic infarction. BMJ Case Rep. 2009. doi:10.1136/bcr.09.2008.0849. [DOI] [PMC free article] [PubMed]
- 25.Gill S, Wolf M, Prince HM, et al. [18F]fluorodeoxyglucose positron emission tomography scanning for staging, response assessment, and disease surveillance in patients with mantle cell lymphoma. Clin Lymphoma Myeloma. 2008;8(3):159–165. doi: 10.3816/CLM.2008.n.019. [DOI] [PubMed] [Google Scholar]
- 26.Karam M, Ata A, Irish K, et al. FDG positron emission tomography/computed tomography scan may identify mantle cell lymphoma patients with unusually favorable outcome. Nucl Med Commun. 2009;30(10):770–778. doi: 10.1097/MNM.0b013e32832e0c13. [DOI] [PubMed] [Google Scholar]
- 27.Bodet-Milin C, Touzeau C, Leux C, et al. Prognostic impact of 18F-fluoro-deoxyglucose positron emission tomography in untreated mantle cell lymphoma: a retrospective study from the GOELAMS group. Eur J Nucl Med Mol Imaging. 2010;37(9):1633–1642. doi: 10.1007/s00259-010-1469-2. [DOI] [PubMed] [Google Scholar]
- 28.Cheah CY, Seymour JF, Wang ML. Mantle cell lymphoma. J Clin Oncol. 2016;34(11):1256–1269. doi: 10.1200/JCO.2015.63.5904. [DOI] [PubMed] [Google Scholar]
- 29.Vose JM. Mantle cell lymphoma: 2015 update on diagnosis, risk-stratification, and clinical management. Am J Hematol. 2015;90(8):739–745. doi: 10.1002/ajh.24094. [DOI] [PubMed] [Google Scholar]
- 30.Yoo C, Yoon DH, Kim S, et al. Serum beta-2 microglobulin as a prognostic biomarker in patients with mantle cell lymphoma. Hematol Oncol. 2016;34(1):22–27. doi: 10.1002/hon.2188. [DOI] [PubMed] [Google Scholar]
- 31.Vogt N, Klapper W. Variability in morphology and cell proliferation in sequential biopsies of mantle cell lymphoma at diagnosis and relapse: clinical correlation and insights into disease progression. Histopathology. 2013;62(2):334–342. doi: 10.1111/his.12009. [DOI] [PubMed] [Google Scholar]
- 32.Tiemann M, Schrader C, Klapper W, et al. Histopathology, cell proliferation indices and clinical outcome in 304 patients with mantle cell lymphoma (MCL): a clinicopathological study from the European MCL network. Br J Haematol. 2005;131(1):29–38. doi: 10.1111/j.1365-2141.2005.05716.x. [DOI] [PubMed] [Google Scholar]
- 33.Argatoff LH, Connors JM, Klasa RJ, Horsman DE, Gascoyne RD. Mantle cell lymphoma: a clinicopathologic study of 80 cases. Blood. 1997;89(6):2067–2078. [PubMed] [Google Scholar]
- 34.Weisenburger DD, Vose JM, Greiner TC, et al. Mantle cell lymphoma. A clinicopathologic study of 68 cases from the Nebraska lymphoma study group. Am J Hematol. 2000;64(3):190–196. doi: 10.1002/1096-8652(200007)64:3<190::aid-ajh9>3.0.co;2-b. [DOI] [PubMed] [Google Scholar]
- 35.Akyurek N, Drakos E, Giaslakiotis K, et al. Differential expression of CKS-1B in typical and blastoid variants of mantle cell lymphoma. Hum Pathol. 2010;41(10):1448–1455. doi: 10.1016/j.humpath.2010.04.001. [DOI] [PubMed] [Google Scholar]
- 36.Hao S, Sanger W, Onciu M, Lai R, Schlette EJ, Medeiros LJ. Mantle cell lymphoma with 8q24 chromosomal abnormalities: a report of 5 cases with blastoid features. Mod Pathol. 2002;15(12):1266–1272. doi: 10.1097/01.MP.0000037310.82136.99. [DOI] [PubMed] [Google Scholar]
- 37.Vincent-Fabert C, Fiancette R, Rouaud P, et al. A defect of the INK4-Cdk4 checkpoint and Myc collaborate in blastoid mantle cell lymphoma-like lymphoma formation in mice. Am J Pathol. 2012;180(4):1688–1701. doi: 10.1016/j.ajpath.2012.01.004. [DOI] [PubMed] [Google Scholar]
- 38.Slotta-Huspenina J, Koch I, de Leval L, et al. The impact of cyclin D1 mRNA isoforms, morphology and p53 in mantle cell lymphoma: p53 alterations and blastoid morphology are strong predictors of a high proliferation index. Haematologica. 2012;97(9):1422–1430. doi: 10.3324/haematol.2011.055715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Raty R, Franssila K, Jansson SE, Joensuu H, Wartiovaara-Kautto U, Elonen E. Predictive factors for blastoid transformation in the common variant of mantle cell lymphoma. Eur J Cancer. 2003;39(3):321–329. doi: 10.1016/s0959-8049(02)00456-2. [DOI] [PubMed] [Google Scholar]
- 40.Bernard M, Gressin R, Lefrere F, et al. Blastic variant of mantle cell lymphoma: a rare but highly aggressive subtype. Leukemia. 2001;15(11):1785–1791. doi: 10.1038/sj.leu.2402272. [DOI] [PubMed] [Google Scholar]
- 41.Khoury JD, Sen F, Abruzzo LV, Hayes K, Glassman A, Medeiros LJ. Cytogenetic findings in blastoid mantle cell lymphoma. Hum Pathol. 2003;34(10):1022–1029. doi: 10.1053/s0046-8177(03)00412-x. [DOI] [PubMed] [Google Scholar]
- 42.Chuang WY, Chang H, Chang GJ, et al. Pleomorphic mantle cell lymphoma morphologically mimicking diffuse large B cell lymphoma: common cyclin D1 negativity and a simple immunohistochemical algorithm to avoid the diagnostic pitfall. Histopathology. 2017;70(6):986–999. doi: 10.1111/his.13161. [DOI] [PubMed] [Google Scholar]
- 43.Molina T. Pitfalls and update in haematopathology. Case 3. Mantle cell lymphoma, aggressive variant, pleomorphic. Ann Pathol. 2012;32(5):341–345. doi: 10.1016/j.annpat.2012.07.017. [DOI] [PubMed] [Google Scholar]
- 44.Espinet B, Ferrer A, Bellosillo B, et al. Distinction between asymptomatic monoclonal B-cell lymphocytosis with cyclin D1 overexpression and mantle cell lymphoma: from molecular profiling to flow cytometry. Clin Cancer Res. 2014;20(4):1007–1019. doi: 10.1158/1078-0432.CCR-13-1077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Zucchetto A, Benedetti D, Tripodo C, et al. CD38/CD31, the CCL3 and CCL4 chemokines, and CD49d/vascular cell adhesion molecule-1 are interchained by sequential events sustaining chronic lymphocytic leukemia cell survival. Cancer Res. 2009;69(9):4001–4009. doi: 10.1158/0008-5472.CAN-08-4173. [DOI] [PubMed] [Google Scholar]
- 46.Dorfman DM, Shahsafaei A. CD200 (OX-2 membrane glycoprotein) expression in b cell-derived neoplasms. Am J Clin Pathol. 2010;134(5):726–733. doi: 10.1309/AJCP38XRRUGSQOVC. [DOI] [PubMed] [Google Scholar]
- 47.Espinet B, Sole F, Pedro C, et al. Clonal proliferation of cyclin D1-positive mantle lymphocytes in an asymptomatic patient: an early-stage event in the development or an indolent form of a mantle cell lymphoma? Hum Pathol. 2005;36(11):1232–1237. doi: 10.1016/j.humpath.2005.08.021. [DOI] [PubMed] [Google Scholar]
- 48.Ahmed M, Li L, Pinnix C, et al. ATM mutation and radiosensitivity: an opportunity in the therapy of mantle cell lymphoma. Crit Rev Oncol Hematol. 2016;107:14–19. doi: 10.1016/j.critrevonc.2016.08.008. [DOI] [PubMed] [Google Scholar]
- 49.Royo C, Salaverria I, Hartmann EM, Rosenwald A, Campo E, Bea S. The complex landscape of genetic alterations in mantle cell lymphoma. Semin Cancer Biol. 2011;21(5):322–334. doi: 10.1016/j.semcancer.2011.09.007. [DOI] [PubMed] [Google Scholar]
- 50.Chapman-Fredricks J, Sandoval-Sus J, Vega F, Lossos IS. Progressive leukemic non-nodal mantle cell lymphoma associated with deletions of TP53, ATM, and/or 13q14. Ann Diagn Pathol. 2014;18(4):214–219. doi: 10.1016/j.anndiagpath.2014.03.006. [DOI] [PubMed] [Google Scholar]
- 51.Racke F, Simpson S, Christian B, Blum K, Hasserjian R, Zhao W. Evidence of long latency periods prior to development of mantle cell lymphoma. Blood. 2010;116:2384. [Google Scholar]
- 52.Jares P, Colomer D, Campo E. Molecular pathogenesis of mantle cell lymphoma. J Clin Invest. 2012;122(10):3416–3423. doi: 10.1172/JCI61272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Jares P, Colomer D, Campo E. Genetic and molecular pathogenesis of mantle cell lymphoma: perspectives for new targeted therapeutics. Nat Rev Cancer. 2007;7(10):750–762. doi: 10.1038/nrc2230. [DOI] [PubMed] [Google Scholar]
- 54.Kuppers R, Zhao M, Hansmann ML, Rajewsky K. Tracing B cell development in human germinal centres by molecular analysis of single cells picked from histological sections. EMBO J. 1993;12(13):4955–4967. doi: 10.1002/j.1460-2075.1993.tb06189.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Fernandez V, Salamero O, Espinet B, et al. Genomic and gene expression profiling defines indolent forms of mantle cell lymphoma. Cancer Res. 2010;70(4):1408–1418. doi: 10.1158/0008-5472.CAN-09-3419. [DOI] [PubMed] [Google Scholar]
- 56.Ferrando AA. SOX11 is a mantle cell lymphoma oncogene. Blood. 2013;121(12):2169–2170. doi: 10.1182/blood-2013-02-480418. [DOI] [PubMed] [Google Scholar]
- 57.Orchard J, Garand R, Davis Z, et al. A subset of t(11;14) lymphoma with mantle cell features displays mutated IgVH genes and includes patients with good prognosis, nonnodal disease. Blood. 2003;101(12):4975–4981. doi: 10.1182/blood-2002-06-1864. [DOI] [PubMed] [Google Scholar]
- 58.Kienle D, Krober A, Katzenberger T, et al. VH mutation status and VDJ rearrangement structure in mantle cell lymphoma: correlation with genomic aberrations, clinical characteristics, and outcome. Blood. 2003;102(8):3003–3009. doi: 10.1182/blood-2003-05-1383. [DOI] [PubMed] [Google Scholar]
- 59.Camacho FI, Algara P, Rodriguez A, et al. Molecular heterogeneity in MCL defined by the use of specific VH genes and the frequency of somatic mutations. Blood. 2003;101(10):4042–4046. doi: 10.1182/blood-2002-11-3456. [DOI] [PubMed] [Google Scholar]
- 60.Schraders M, Oeschger S, Kluin PM, et al. Hypermutation in mantle cell lymphoma does not indicate a clinical or biological subentity. Mod Pathol. 2009;22(3):416–425. doi: 10.1038/modpathol.2008.199. [DOI] [PubMed] [Google Scholar]
- 61.Lai R, Lefresne SV, Franko B, et al. Immunoglobulin VH somatic hypermutation in mantle cell lymphoma: mutated genotype correlates with better clinical outcome. Mod Pathol. 2006;19(11):1498–1505. doi: 10.1038/modpathol.3800677. [DOI] [PubMed] [Google Scholar]
- 62.Bertoni F, Conconi A, Cogliatti SB, et al. Immunoglobulin heavy chain genes somatic hypermutations and chromosome 11q22-23 deletion in classic mantle cell lymphoma: a study of the Swiss Group for Clinical Cancer Research. Br J Haematol. 2004;124(3):289–298. doi: 10.1046/j.1365-2141.2003.04763.x. [DOI] [PubMed] [Google Scholar]
- 63.Cogliatti SB, Bertoni F, Zimmermann DR, et al. IgV H mutations in blastoid mantle cell lymphoma characterize a subgroup with a tendency to more favourable clinical outcome. J Pathol. 2005;206(3):320–327. doi: 10.1002/path.1781. [DOI] [PubMed] [Google Scholar]
- 64.Wang X, Asplund AC, Porwit A, et al. The subcellular Sox11 distribution pattern identifies subsets of mantle cell lymphoma: correlation to overall survival. Br J Haematol. 2008;143(2):248–252. doi: 10.1111/j.1365-2141.2008.07329.x. [DOI] [PubMed] [Google Scholar]
- 65.Nygren L, Baumgartner Wennerholm S, Klimkowska M, Christensson B, Kimby E, Sander B. Prognostic role of SOX11 in a population-based cohort of mantle cell lymphoma. Blood. 2012;119(18):4215–4223. doi: 10.1182/blood-2011-12-400580. [DOI] [PubMed] [Google Scholar]
- 66.Navarro A, Clot G, Royo C, et al. Molecular subsets of mantle cell lymphoma defined by the IGHV mutational status and SOX11 expression have distinct biologic and clinical features. Cancer Res. 2012;72(20):5307–5316. doi: 10.1158/0008-5472.CAN-12-1615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Eskelund CW, Dahl C, Hansen JW, Westman M, Kolstad A, Pedersen LB, Montano-Almendras CP, Husby S, Freiburghaus C, Ek S, Pedersen A, Niemann C, Räty R, Brown P, Geisler CH, Andersen MK, Guldberg P, Jerkeman M, Grønbæk K. TP53 mutations identify younger mantle cell lymphoma patients who do not benefit from intensive chemoimmunotherapy. 2017. doi:10.1182/blood-2017-04-779736. Accessed 06 Dec 2017. [DOI] [PubMed]
- 68.Lu TX, Young KH, Xu W, Li JY. TP53 dysfunction in diffuse large B-cell lymphoma. Crit Rev Oncol Hematol. 2016;97:47–55. doi: 10.1016/j.critrevonc.2015.08.006. [DOI] [PubMed] [Google Scholar]
- 69.Halldorsdottir AM, Lundin A, Murray F, et al. Impact of TP53 mutation and 17p deletion in mantle cell lymphoma. Leukemia. 2011;25(12):1904–1908. doi: 10.1038/leu.2011.162. [DOI] [PubMed] [Google Scholar]
- 70.Greiner TC, Moynihan MJ, Chan WC, et al. p53 mutations in mantle cell lymphoma are associated with variant cytology and predict a poor prognosis. Blood. 1996;87(10):4302–4310. [PubMed] [Google Scholar]
- 71.Hernandez L, Fest T, Cazorla M, et al. p53 gene mutations and protein overexpression are associated with aggressive variants of mantle cell lymphomas. Blood. 1996;87(8):3351–3359. [PubMed] [Google Scholar]
- 72.Kridel R, Meissner B, Rogic S, et al. Whole transcriptome sequencing reveals recurrent NOTCH1 mutations in mantle cell lymphoma. Blood. 2012;119(9):1963–1971. doi: 10.1182/blood-2011-11-391474. [DOI] [PubMed] [Google Scholar]
- 73.Bea S, Valdes-Mas R, Navarro A, et al. Landscape of somatic mutations and clonal evolution in mantle cell lymphoma. Proc Natl Acad Sci U S A. 2013;110(45):18250–18255. doi: 10.1073/pnas.1314608110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Lin CY, Loven J, Rahl PB, et al. Transcriptional amplification in tumor cells with elevated c-Myc. Cell. 2012;151(1):56–67. doi: 10.1016/j.cell.2012.08.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Klapproth K, Wirth T. Advances in the understanding of MYC-induced lymphomagenesis. Br J Haematol. 2010;149(4):484–497. doi: 10.1111/j.1365-2141.2010.08159.x. [DOI] [PubMed] [Google Scholar]
- 76.Michaux L, Wlodarska I, Theate I, et al. Coexistence of BCL1/CCND1 and CMYC aberrations in blastoid mantle cell lymphoma: a rare finding associated with very poor outcome. Ann Hematol. 2004;83(9):578–583. doi: 10.1007/s00277-004-0879-2. [DOI] [PubMed] [Google Scholar]
- 77.Aukema SM, Siebert R, Schuuring E, et al. Double-hit B-cell lymphomas. Blood. 2011;117(8):2319–2331. doi: 10.1182/blood-2010-09-297879. [DOI] [PubMed] [Google Scholar]
- 78.Choe JY, Yun JY, Na HY, et al. MYC overexpression correlates with MYC amplification or translocation, and is associated with poor prognosis in mantle cell lymphoma. Histopathology. 2016;68(3):442–449. doi: 10.1111/his.12760. [DOI] [PubMed] [Google Scholar]
- 79.Katzenberger T, Petzoldt C, Holler S, et al. The Ki67 proliferation index is a quantitative indicator of clinical risk in mantle cell lymphoma. Blood. 2006;107(8):3407. doi: 10.1182/blood-2005-10-4079. [DOI] [PubMed] [Google Scholar]
- 80.Hoster E, Rosenwald A, Berger F, et al. Tumor cell proliferation (Ki-67 index) overcomes cytology and growth pattern as prognostic factor in mantle-cell lymphoma – results from randomized trials of the European MCL network. Blood. 2014;124:abstr 2977. [Google Scholar]
- 81.Scott DW, Abrisqueta P, Wright GW, et al. New molecular assay for the proliferation signature in mantle cell lymphoma applicable to formalin-fixed paraffin-embedded biopsies. J Clin Oncol. 2017;35(15):1668–1677. doi: 10.1200/JCO.2016.70.7901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Marti GE, Shim YK, Albitar M, et al. Long-term follow-up of monoclonal B-cell lymphocytosis detected in environmental health studies. Cytometry B Clin Cytom. 2010;78(Suppl 1):S83–S90. doi: 10.1002/cyto.b.20522. [DOI] [PubMed] [Google Scholar]
- 83.Rawstron AC, Green MJ, Kuzmicki A, et al. Monoclonal B lymphocytes with the characteristics of “indolent” chronic lymphocytic leukemia are present in 3.5% of adults with normal blood counts. Blood. 2002;100(2):635–639. doi: 10.1182/blood.v100.2.635. [DOI] [PubMed] [Google Scholar]
- 84.Dagklis A, Fazi C, Sala C, et al. The immunoglobulin gene repertoire of low-count chronic lymphocytic leukemia (CLL)-like monoclonal B lymphocytosis is different from CLL: diagnostic implications for clinical monitoring. Blood. 2009;114(1):26–32. doi: 10.1182/blood-2008-09-176933. [DOI] [PubMed] [Google Scholar]
- 85.Fazi C, Scarfo L, Pecciarini L, et al. General population low-count CLL-like MBL persists over time without clinical progression, although carrying the same cytogenetic abnormalities of CLL. Blood. 2011;118(25):6618–6625. doi: 10.1182/blood-2011-05-357251. [DOI] [PubMed] [Google Scholar]
- 86.Nieto WG, Almeida J, Romero A, et al. Increased frequency (12%) of circulating chronic lymphocytic leukemia-like B-cell clones in healthy subjects using a highly sensitive multicolor flow cytometry approach. Blood. 2009;114(1):33–37. doi: 10.1182/blood-2009-01-197368. [DOI] [PubMed] [Google Scholar]
- 87.Lecluse Y, Lebailly P, Roulland S, Gac AC, Nadel B, Gauduchon P. t(11;14)-positive clones can persist over a long period of time in the peripheral blood of healthy individuals. Leukemia. 2009;23(6):1190–1193. doi: 10.1038/leu.2009.31. [DOI] [PubMed] [Google Scholar]
- 88.Hirt C, Schuler F, Dolken L, Schmidt CA, Dolken G. Low prevalence of circulating t(11;14)(q13;q32)-positive cells in the peripheral blood of healthy individuals as detected by real-time quantitative PCR. Blood. 2004;104(3):904–905. doi: 10.1182/blood-2004-02-0738. [DOI] [PubMed] [Google Scholar]
- 89.Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the international workshop on chronic lymphocytic leukemia updating the National Cancer Institute-working group 1996 guidelines. Blood. 2008;111(12):5446–5456. doi: 10.1182/blood-2007-06-093906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Marti GE, Rawstron AC, Ghia P, et al. Diagnostic criteria for monoclonal B-cell lymphocytosis. Br J Haematol. 2005;130(3):325–332. doi: 10.1111/j.1365-2141.2005.05550.x. [DOI] [PubMed] [Google Scholar]
- 91.Karube K, Scarfo L, Campo E, Ghia P. Monoclonal B cell lymphocytosis and “in situ” lymphoma. Semin Cancer Biol. 2014;24:3–14. doi: 10.1016/j.semcancer.2013.08.003. [DOI] [PubMed] [Google Scholar]
- 92.Ondrejka SL, Lai R, Smith SD, Hsi ED. Indolent mantle cell leukemia: a clinicopathological variant characterized by isolated lymphocytosis, interstitial bone marrow involvement, kappa light chain restriction, and good prognosis. Haematologica. 2011;96(8):1121–1127. doi: 10.3324/haematol.2010.036277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Vizcarra E, Martinez-Climent JA, Benet I, et al. Identification of two subgroups of mantle cell leukemia with distinct clinical and biological features. Hematol J. 2001;2(4):234–241. doi: 10.1038/sj.thj.6200111. [DOI] [PubMed] [Google Scholar]
- 94.Nodit L, Bahler DW, Jacobs SA, Locker J, Swerdlow SH. Indolent mantle cell lymphoma with nodal involvement and mutated immunoglobulin heavy chain genes. Hum Pathol. 2003;34(10):1030–1034. doi: 10.1053/s0046-8177(03)00410-6. [DOI] [PubMed] [Google Scholar]
- 95.Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375–2390. doi: 10.1182/blood-2016-01-643569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Carvajal-Cuenca A, Sua LF, Silva NM, et al. In situ mantle cell lymphoma: clinical implications of an incidental finding with indolent clinical behavior. Haematologica. 2012;97(2):270–278. doi: 10.3324/haematol.2011.052621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Richard P, Vassallo J, Valmary S, Missoury R, Delsol G, Brousset P. “In situ-like” mantle cell lymphoma: a report of two cases. J Clin Pathol. 2006;59(9):995–996. doi: 10.1136/jcp.2005.030783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Rodig SJ, Healey BM, Pinkus GS, Kuo FC, Dal Cin P, Kutok JL. Mantle cell lymphoma arising within primary nodal marginal zone lymphoma: a unique presentation of two uncommon B-cell lymphoproliferative disorders. Cancer Genet Cytogenet. 2006;171(1):44–51. doi: 10.1016/j.cancergencyto.2006.06.018. [DOI] [PubMed] [Google Scholar]
- 99.Aqel N, Barker F, Patel K, Naresh KN. In-situ mantle cell lymphoma--a report of two cases. Histopathology. 2008;52(2):256–260. doi: 10.1111/j.1365-2559.2007.02906.x. [DOI] [PubMed] [Google Scholar]
- 100.Adam P, Schiefer AI, Prill S, et al. Incidence of preclinical manifestations of mantle cell lymphoma and mantle cell lymphoma in situ in reactive lymphoid tissues. Mod Pathol. 2012;25(12):1629–1636. doi: 10.1038/modpathol.2012.117. [DOI] [PubMed] [Google Scholar]
- 101.Fend F, Cabecadas J, Gaulard P, et al. Early lesions in lymphoid neoplasia: conclusions based on the workshop of the XV. Meeting of the European Association of Hematopathology and the Society of Hematopathology, in Uppsala, Sweden. J Hematop. 2012;5(3). doi:10.1007/s12308-012-0148-6. [DOI] [PMC free article] [PubMed]
- 102.Racke F, Simpson S, Christian B, Blum KA, Hasserjian R, Zhao W. Evidence of long latency periods prior to development of mantle cell lymphoma. Blood Abstr. 2010;116:323. [Google Scholar]
- 103.Saito M, Mori A, Irie T, et al. Endoscopic follow-up of 3 cases with gastrointestinal tract involvement of mantle cell lymphoma. Intern Med. 2010;49(3):231–235. doi: 10.2169/internalmedicine.49.2766. [DOI] [PubMed] [Google Scholar]
- 104.Parente F, Cernuschi M, Orlando G, Rizzardini G, Lazzarin A, Bianchi Porro G. Kaposi's sarcoma and AIDS: frequency of gastrointestinal involvement and its effect on survival. A prospective study in a heterogeneous population. Scand J Gastroenterol. 1991;26(10):1007–1012. doi: 10.3109/00365529109003949. [DOI] [PubMed] [Google Scholar]
- 105.Ruskone-Fourmestraux A, Audouin J. Primary gastrointestinal tract mantle cell lymphoma as multiple lymphomatous polyposis. Best Pract Res Clin Gastroenterol. 2010;24(1):35–42. doi: 10.1016/j.bpg.2009.12.001. [DOI] [PubMed] [Google Scholar]
- 106.Ambinder AJ, Shenoy PJ, Nastoupil LJ, Flowers CR. Using primary site as a predictor of survival in mantle cell lymphoma. Cancer. 2013;119(8):1570–1577. doi: 10.1002/cncr.27898. [DOI] [PubMed] [Google Scholar]
- 107.Neto AG, Oroszi G, Protiva P, Rose M, Shafi N, Torres R. Colonic in situ mantle cell lymphoma. Ann Diagn Pathol. 2012;16(6):508–514. doi: 10.1016/j.anndiagpath.2011.05.001. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.