

Abstract
The marijuana amotivational syndrome posits that cannabis use fosters apathy through the depletion of motivation-based constructs such as self-efficacy. The current study pursued a two-round design to rule out concomitant risk factors responsible for the connection from marijuana intake to lower general self-efficacy. College students (N = 505) completed measures of marijuana use, demographics (age, gender, and race), personality (extraversion, agreeableness, conscientiousness, openness, and neuroticism), other substance use (alcohol and tobacco), and general self-efficacy (initiative, effort, and persistence) in two assessments separated by a month. Hierarchical regression models found that marijuana use forecasted lower initiative and persistence, even after statistically ruling out 13 pertinent baseline covariates including demographics, personality traits, alcohol use, tobacco use, and self-efficacy subscales. A cross-lagged panel model involving initiative, effort, persistence, alcohol use, cigarette use, and marijuana use sought to unravel the temporal precedence of processes. Results showed that only marijuana (but not alcohol or tobacco) intake significantly and longitudinally prompted lower initiative and persistence. Furthermore, in the same model, the opposite temporal direction of events from lower general self-efficacy subscales to marijuana use were untenable. Findings provide partail support for the marijuana amotivational syndrome, underscore marijuana as a risk factor in decreased general self-efficacy, and offer implications and insights for marijuana prevention and future research.
Keywords: marijuana, amotivational syndrome, general self-efficacy, cross-lagged panel modeling, longitudinal
Marijuana is the most widely used illicit drug in the United States. Approximately 1 in 5 college students (20.8%) have consumed marijuana in the past 30 days (Johnston, O’Malley, Bachman, Schulenberg, & Miech, 2015). Cannabis intake could lead to adverse consequences (Volkow, Baler, Compton, & Weiss, 2014), including impaired cognition (Conroy, Kurth, Brower, Strong, & Stein, 2015), car crash injury (Blows et al., 2005), diminished educational attainment (Fleming, White, Haggerty, Abbott, & Catalano, 2012), school dropout (McCaffrey, Liccardo Pacula, Han, & Ellickson, 2010), and poorer life satisfaction (Swain, Gibb, Horwood, & Fergusson, 2012). Studies tracking first-year college students for up to six years after college reveal that trajectory groups characterized by chronic and later-increase in marijuana use fare poorly on multiple physical and mental health outcomes, such as functional impairment and psychological distress (Arria, Caldeira, Bugbee, Vincent, & O’Grady, 2016; Caldeira, O’Grady, Vincent, & Arria, 2012). Given national trends in decreasing perceived marijuana risk (Pacek, Mauro, & Martins, 2015) and increasing marijuana use (Hasin et al., 2015) in young adults, the study of cannabis intake is very timely in the context of marijuana legalization and policy changes in the United States and underscores the need to identify risks and consequences to inform prevention campaigns and interventions targeting college students.
The current study seeks to clarify and understand the temporal directionality of marijuana use and general self-efficacy. Research examining general self-efficacy is important as it plays a central role in the study of prevention science topics focused on curtailing undesirable behavioral outcomes and improving human functioning including better self-regulation, reduced negative affect, lower vulnerability to anxiety and depression, greater happiness, positive mental health, and better quality of life (Andersson, Moore, Hensing, Krantz, & Staland-Nyman, 2014; Kvarme, Haraldstad, Helseth, Sørum, & Natvig, 2009; Luszczynska, Gutiérez-Doña, & Schwarzer, 2005, Natvig, Albrektsen, & Qvarnstrøm, 2003). Furthermore, compromised general self-efficacy serves as a risk factor that could “spill over” and translate into lower domain specific self-efficacy (Chen, Gully & Eden, 2001), a pivotal construct commonly applied and scrutinized in prevention research frameworks including the Theory of Planned Behavior (Ajzen, 1991) and the Health Belief Model (Rosenstock, Strecher, & Becker, 1988). If cannabis use is revealed to be an antecedent of lower general self-efficacy, information about the risk pathway could be targeted in marijuana prevention programs to curtail use and reduce its deleterious effects on initiative, effort, and persistence.
Marijuana Use and Reductions in Motivation
Despite decades of research, the marijuana use and motivational reduction connection remains controversial (Volkow et al., 2016). The term “amotivational syndrome” was first coined by Smith (1968) to denote the diminished desire to work or to compete among young people who consumed marijuana frequently. Early reports documenting the connection between cannabis intake and lack of motivation were primarily premised on clinical observations (McGlothlin & West, 1968; Smith, 1968). Subsequent analyses based on the Colorado Rocky Mountain longitudinal study revealed significant associations involving marijuana use and constructs in the motivation-instigation structure (Jessor, Jessor, & Finney, 1973; Jessor, 1976). Specifically, greater achievement expectations and values were hypothesized to reflect motivation toward conventional goals, whereas greater independence values were proposed to reflect motivation toward nonconventional activities such as marijuana use. Results found that emphasis placed on independence compared to achievement values emerged as one of the strongest predictors of marijuana use in both high school and college students. Other studies, however, revealed that marijuana use was not significantly related to amotivation (Duncan, 1987) or that the connection was instead accounted for by confounds such as personality traits (Kupfer, Detre, Koral, & Fajans, 1973; Mellinger, Somers, Davidson, & Manheimer, 1976).
Later investigations that tested the marijuana amotivational syndrome focused on the connections of marijuana use and motivation-related constructs in the context of the school or workplace. A narrative literature review of the topic proposed that the marijuana amotivational syndrome serves as an underlying mechanism by which early marijuana use is related to subsequently lower educational attainment (Lynskey and Hall, 2000). Research has documented that college students who frequently used cannabis reported less energy, compromised productivity, increased procrastination, and greater school and work absences compared to classmates who rarely or never used (Buckner, Ecker, & Cohen, 2010). Momentary ecological assessments sampling the marijuana experiences of college student users several times per day found that greater cravings and the number of minutes smoking marijuana forecasted poorer academic motivation and achievement (Phillips, Phillips, Lalonde, & Tormohlen, 2015). Research also shows that increases in marijuana use anticipated decreases in grade point average and a longer time to graduate from college (Arria et al., 2015). Furthermore, college students with a history of frequent marijuana use were likely have plans to delay graduation or drop out of college entirely (Suerken et al., 2016).
In addition to the aforementioned correlational research, experimental investigations support the impact of marijuana use on motivation-related constructs. The receipt of inhaled dosages of marijuana in a controlled laboratory setting diminishes motivation to perform a task (Cherek, Lane, & Dougherty, 2002). Using a two-option (work vs. non-work) experimental task that varied in reinforcement contingencies, adolescents with marijuana in their bodies (detected in urine samples) switched from the work to non-work option more quickly than the control group of nonusers (Lane, Cherek, Pietras, and Steinberg, 2005), suggesting that cannabis consumers are not as persistent. The performance detriment in users held even after statistically controlling for gender, cognitive aptitude, and diagnoses of conduct problems.
General Self-Efficacy as a Motivation-Related Construct
The concept of self-efficacy was first proposed by Bandura (1977) as part of his unified theory of behavioral change. Self-efficacy is the belief in one’s own ability to pursue, organize, and implement goal-directed behaviors (Bandura, 1994). Bandura (1977) distinguished between efficacy and outcome expectations, with the former linking person to behavior and the latter linking behavior to outcome. In this framework, a person’s own efficacy expectations reflect motivation in initiating and persisting in a behavior. Although early research focused on self-efficacy specific to behaviors, tasks, and situations, later work led to the development of a global self-efficacy measure that was not context dependent (Sherer et al., 1982). Factor analysis of the general self-efficacy scale yielded three underlying dimensions (Bosscher & Smit, 1998): initiative (confidence in starting a new behavior), effort (willingness to put in hard work and complete a behavior), and persistence (perseverance and tenacity to perform a behavior in face of uncertainty). These three independent, yet correlated, subscales capture motivational belief components in the overall capability to perform behaviors.
The literature reveals only two studies that have investigated the association between general motivation or self-efficacy and marijuana use. Barnwell, Earleywine, and Wilcox (2006) found that daily marijuana users did not differ in their level of global motivation compared to abstainers of marijuana use. Grevenstein, Bluemke, and Kroeninger-Jungaberle (2016) found that lower general self-efficacy longitudinally predicted higher marijuana use, but the study did not evaluate the reverse temporal direction of the two variables or report analyses disaggregated by self-efficacy subscales.
Current Study
The present investigation tests the amotivational syndrome by examining the connections of marijuana use and general self-efficacy subscales (initiative, effort, and persistence) in a sample of young adults measured in two rounds separated by a month. The study addresses several limitations of prior research. First, marijuana use associations with each of the three general self-efficacy subscales have not been tested previously. A nuanced possibility is that using this psychoactive substance might be related to lower levels for some, but not all, of the general self-efficacy subscales. Only the general self-efficacy subscales identified to be significant should be meaningfully targeted in prevention and risk-reduction campaigns and interventions.
Second, pertinent covariates were incorporated into analyses. The marijuana use and amotivation pathway could be attenuated by personality traits (Kupfer et al., 1973; Mellinger et al., 1976), especially high agreeableness and low conscientiousness (Fridberg, Vollmer, O’Donnell, & Skosnik, 2011; Terracciano, Löckenhoff, Crum, Bienvenu, & Costa, 2008), so statistically eliminating these factors as rival explanations of general self-efficacy is ideal. Alcohol and tobacco use (Keith, Hart, McNeil, Silver, & Goodwin, 2015; Suerken et al., 2014) might co-occur with marijuana use and therefore these other substances should be statistically controlled as competing predictors of general self-efficacy. Third, the current research pursues a longitudinal design (Lac, 2016; Lac & Crano, 2016) to address the methodological limitation of cross-sectional research unable to evaluate cannabis intake as a temporal antecedent of self-efficacy reductions. Even in previous experimental and longitudinal research, only a single directional process (marijuana use to motivation-related construct) is tested and the reverse process of events (motivation-related construct to marijuana use) is rarely empirically tested and scrutinized as a competing process (Cherek et al., 2002; Grevenstein et al. 2016; Jessor et al., 1973; Lane et al., 2005). A central tenet of the amotivational syndrome is that cannabis intake leads to amotivation (not the other way around). Thus, a cross-lagged panel design to scrutinize the directionality of marijuana and general self-efficacy would address this gap in the literature.
Two sets of analyses were pursued. In hierarchical regression models, baseline marijuana usage was specified to longitudinally predict each general self-efficacy subscale (initiative, effort, and persistence). The covariates incorporated and ruled out as confounds included baseline demographics (age, gender, and race), personality (extraversion, agreeableness, conscientiousness, openness, and neuroticism), other substances (alcohol and tobacco), and self-efficacy (initiative, effort, and persistence). In the cross-lagged panel model, initiative, effort, and persistence, alcohol use, cigarette use, and marijuana use were specified in both rounds to estimate the temporal precedence of events. Considering that the amotivational syndrome is typically ascribed to the properties of cannabis (not other substances), marijuana use was hypothesized to longitudinally predict reduced general self-efficacy (might depend on the subscale), but alcohol and tobacco use were expected to be unrelated to general self-efficacy.
Method
Participants
The sample of 505 undergraduate students averaged 19.06 (SD = 1.32) years of age. Gender distribution consisted of 69.9% female and 30.1% male. Racial classification included 62.8% White, 14.9% Latino, 5.0% Black, and 17.4% Asian.
Procedure
Students were compensated with subject pool or extra credit in psychology courses for participation. After enrolling in the study, each participant received an email that contained a confidential and secure link to the web-based questionnaire (T1). The electronic consent form was followed by assurances of confidentiality and the questionnaire items. Participants completed the follow-up questionnaire one month later (T2). During each administration, participants received up to two reminders via email to complete the study. The final sample for analyses consisted of 505 (out of 575) participants who provided complete responses in both periods. Completers and noncompleters did not significantly (p > .05) differ on age, gender, and race. A University IRB approved this study.
Measures
Marijuana Use
The marijuana intake question (“On how many days in the past 30 days did you use marijuana?”) required an open-ended quantitative response from 0 to 30.
Other Substance Use
Alcohol (“On how many days in the past 30 days did you use alcohol?”) and cigarette (“On how many days in the past 30 days did you use cigarettes?”) use were measured. Participants entered open-ended quantitative responses from 0 to 30.
General self-efficacy
The General Self-Efficacy Scale (Sherer et al., 1982) is based on three factors (Bosscher & Smit, 1988). The subscales were initiative (e.g., “If something looks too complicated I will not even bother to try it”; 3 items; T1 α = .90; T2 α = .90), effort (e.g., “If I can’t do a job the first time, I keep trying until I can”; 5 items; T1 α = .83; T2 α = .87) and persistence (e.g., “When unexpected problems occur, I don’t handle them very well”; 4 items; T1 α = .84; T2 α = .88). Response anchors ranged from 1 (strongly disagree) to 7 (strongly agree). Responses to the negatively phrased items were reverse scored. Higher subscale mean scores represented higher self-efficacy.
Exploratory factor analysis applying common factor (principal axis factoring) extraction and oblique (oblimin) rotation was performed on the Time 1 items of the General Self-Efficacy Scale. The eigenvalue greater > 1 criterion (Kaiser, 1960), scree plot, (Cattell, 1966) and simple structure in interpretability of factor loadings (Gorsuch, 1983) all supported a three-factor solution. Item loadings (pattern matrix) ranged from .64 to .87 for initiative, .54 to .82 for effort, and .58 to .87 for persistence. The interfactor correlations were .45 for initiative and effort, .44 for initiative and persistence, and .52 for effort and persistence. Exploratory factor analysis on the Time 2 items corroborated the three-factor solution.
Personality
The Big Five personality taxonomy (Costa & McCrae, 1995) was captured with the 44-item version (John, 1990; John & Srivastava, 1999). The subscales included extraversion (e.g., “Is outgoing, sociable”; 8 items; α = .88), agreeableness (e.g., “Is considerate and kind to almost everyone”; 9 items; α = .79), conscientiousness (e.g. “Makes plans and follows through with them”; 9 items; α = .79), openness (e.g., “Is inventive”; α = .77; 10 items), and neuroticism (e.g. “Can be moody”; α =.81; 8 items). Options ranged from 1 (strongly disagree) to 5 (strongly agree). Responses to negatively phrased items were reverse scored. Higher subscale mean scores represented greater levels of the traits.
Analytic Plan
The substance use variables of marijuana, alcohol, and cigarette possessed nonnormal distributional properties (Tabachnick & Fidell, 2012): Skewness ranged from 1.27 to 4.30 and kurtosis from 2.18 to 19.15. The medians and interquartile ranges were as follows: T1 alcohol (4; 1 to 8) T1 cigarette (0; 0 to 0), T1 marijuana (0; 0 to 1), T2 alcohol (4; 1 to 7), T2 cigarette (0; 0 to 0), and T2 marijuana (0; 0 to 1). Thus, each substance use variable was binary transformed (0 = nonuse, 1 = use).
The hierarchical (sequential) multiple regression analyses (Tabachnick & Fidell, 2012; Warner, 2013) served to statistically control for covariates potentially responsible for the longitudinal connection from marijuana use to lower general self-efficacy (Crano & Lac, 2012). The T2 outcomes of initiative, effort, and persistence were estimated in three separate hierarchal regression models predicted by T1 measures. In each model, the simple contribution of marijuana status (0 = nonuser, 1 = user) was entered in Step 1. Step 2 accounted for the demographics characteristics of age, gender (0 = male, 1 = female), and race (0 = racial minority, 1 = Caucasian). The personality traits of extraversion, agreeableness, conscientious, openness, and neuroticism were entered into Step 3. Step 4 evaluated the contribution of other substances including alcohol (0 = nonuser, 1= user) and cigarette (0 = nonuser, 1 = user). Finally, the baseline self-efficacy subscales of initiative, effort, and persistence were entered in Step 5. The highest variance inflation factor (VIF) value of 1.91 indicated no multicolinearity problems (Tabachnick & Fidell, 2012).
The cross-lagged panel analysis involving initiative, effort, persisetence, alcohol use, cigarette use, and marijuana use was comprehensively estimated in a hybrid model combining linear multiple regression and binary logistic regression. Accordingly, path coefficients to quantiative outcomes (T2 initiative, effort, and persistence) represent multiple regression beta weights, whereas coeffficients to binary outcomes (T2 alcohol, cigarette, and marijuana) represent adjusted odds ratios. The testing of both types of statistical techniques in a single hybrid model was possible using Mplus software (Muthén & Muthén, 2010) and maximum-likelihood estimation. The program does not permit the specification of error term correlations involving binary and quantiative outcomes in the integrative model (Muthén & Muthén, 2010)
Cross-lagged panel models are pursued for the purpose of making inferences regarding the temporal precedence of a set of constructs in nonexperimental research (Kenny, 1975; Shadish, Cook & Campbell, 2002). Cross-lagged panel models contain three types of statistical relations (Lac, 2016; Locascio, 1982; Shadish et al., 2002). Synchronnous correlations represent the nondirectional associations of different variables asessed in the same round (e.g., T1 initaitive and T1 marijuana use). Autoregressive paths indicate the magnitude of a variable assessed in a prior round predicting its subsequent measurement (e.g., T1 initiative to T2 initiative), while statistically controlling for all other lagged antecedent measures. These test-retest relations, reflecting temporal stability coefficients, almost always emerge as the strongest coefficients in the model. The cross-lagged paths of a variable from an earlier round predicting a different variable at a later round are most relevant in testing the temporal precedeence of constructs (e.g,. T1 marijuana use to T2 initiative). Directionality is evidenced if a cross-lagged path attains significance after controlling for all paths and antecedent measures in the model.
Results
Hierarchical Multiple Regression Models
The sample consisted of 27.5% marijuana users (72.5% nonusers), 76.1% alcohol users (23.8% nonusers), and 16.0% cigarette users (84.0% nonusers). Hierarchical regression analyses controlling for covariates of the T1 marijuana use to T2 self-efficacy connection are presented in Table 1. Model 1 shows the T1 variables in predicting T2 initiative. Marijuana use (compared to nonuse) longitudinally predicted lower initiative (Step 1). The final model (Step 5) involving the simultaneous entry of all predictors reveals that marijuana use (vs. nonuse), lower initiative, lower effort, and lower persistence forecasted lower T2 initiative.
Table 1.
Hierarchial Multiple Regression of T1 Measures Predicting T2 Initiative, Effort, and Persistence
| Model 1: T2 Initiative
|
Model 2: T2 Effort
|
Model 3: T2 Peristence
|
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Step 1 | Step 2 | Step 3 | Step 4 | Step 5 | Step 1 | Step 2 | Step 3 | Step 4 | Step 5 | Step 1 | Step 2 | Step 3 | Step 4 | Step 5 | ||
| Step 1 | Marijuana use | −.13** | −.13** | −.10* | −.09* | −.08* | −15*** | −.14** | −.10* | −.08 | −.02 | −.14** | −.13** | −.12* | −.11* | −.09* |
| Step 2 | Age | .04 | .06 | .06 | .05 | −.07 | −.05 | −.04 | −.07 | .01 | .06 | .06 | .04 | |||
| Gender | .02 | −.01 | −.01 | .04 | .06 | −.05 | −.04 | −.02 | .04 | .01 | .01 | .03 | ||||
| Race | .10* | .05 | .05 | .04 | .07 | −.01 | −.01 | .00 | .11* | .04 | .04 | .05 | ||||
| Step 3 | Extroversion | .00 | .00 | −.07 | .12** | .13** | .06 | .08 | .08 | .04 | ||||||
| Agreeableness | .05 | .04 | .03 | .10* | .10* | .05 | .07 | .07 | .04 | |||||||
| Conscientiousness | 29*** | 29*** | .04 | .41*** | .41*** | .13** | .25*** | 25*** | .06 | |||||||
| Openness | 14** | 14** | .02 | .10* | .10* | .03 | .06 | .06 | .03 | |||||||
| Neuroticism | −.12** | −.12** | −.01 | .04 | .02 | .07 | − 27*** | − 27*** | −.11* | |||||||
| Step 4 | Alcohol use | .03 | .04 | −.01 | −.03 | .02 | .01 | |||||||||
| Tobacco use | −.05 | −.03 | −.05 | −.03 | −.05 | .−.05 | ||||||||||
| Step 5 | Initiative | .51*** | .03 | .07 | ||||||||||||
| Effort | 13*** | .50*** | .03 | |||||||||||||
| Persistence | .13* | .08 | 43*** | |||||||||||||
| Model R2 | .02** | .03** | 19*** | 19*** | .45*** | .02*** | .04** | .29*** | .30*** | .46*** | .02** | .03** | .26*** | .27***. | 41*** | |
p < .05.
p < .01.
p < .001.
Coefficients are β weights.
Model 2 as presented in Table 1 shows the T1 variables in predicting T2 effort. Marijuana use (vs. nonuse) entered as the only predictor contributed to T2 compromised effort (Step 1). After concurrently accounting for demographics and personality (Step 3), the marijuana use (vs. nonuse) variable remained predictive of lower T2 effort. However, after additionally controlling for alcohol and tobacco use (Step 4), the marijuana status to effort pathway was attenuated and no longer significant. In the final model (Step 5), only conscientiousness and effort uniquely contributed to T2 effort.
Model 3 as presented in Table 1 shows the T1 variables in predicting T2 persistence. Marijuana use (vs. nonuse) entered by itself contributed to lower T2 persistence (Step 1). In the final model controlling for all covariates (Step 5), the variables of marijuana use (vs. nonuse), higher neuroticism, and lower persistence (Step 5) forecasted lower T2 persistence.
Figure 1 shows the mean scores for the general self-efficacy subscales tracked across both measurement rounds as a function of T1 marijuana status. The mean scores presented in this figure adjusted for the regression analysis covariates in Table 1.
Figure 1.
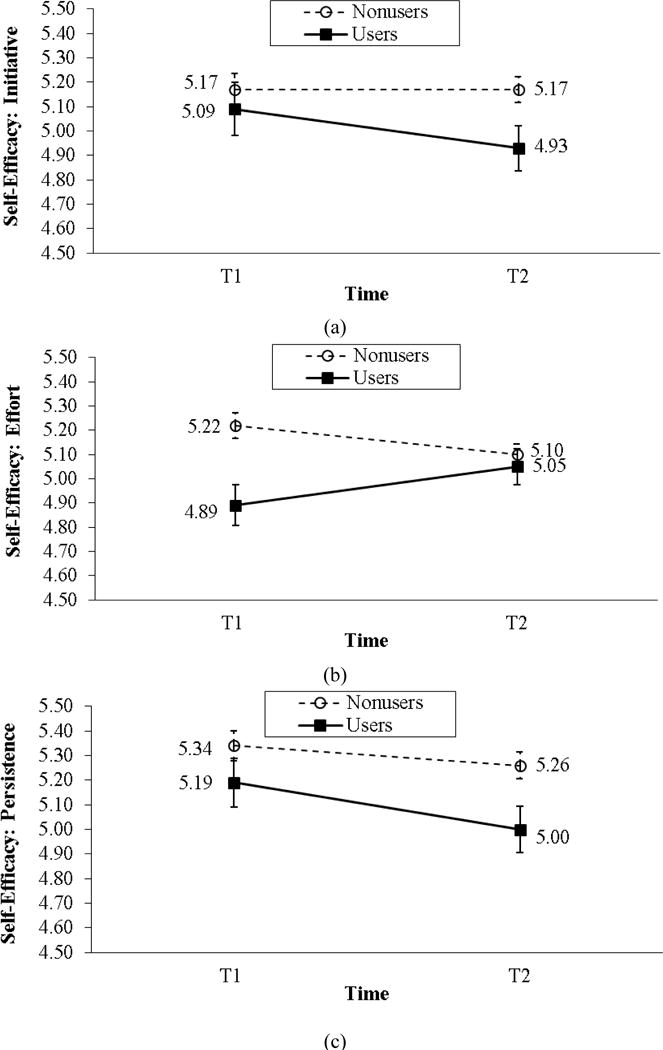
Self-efficacy subscales as a function of T1 marijuana status (adjusted means and standard errors controlling for the same covariates in Table 1).
Cross-Lagged Panel Model
The cross-lagged panel model tested initiative, effort, persistence, alcohol use, cigarette use, and marijuana use in both rounds. All possible saturated combinations of synchronous correlations in T1, autoregressive paths from T1 to T2, and cross-lagged paths from T1 to T2 were estimated. All paths were retained and controlled for regardless of whether coefficients attained significance, with only the significant paths of the model diagrammed in Figure 2. In examining the T1 synchronous correlations, the three general self-efficacy subscales were significantly associated, and the three substance use measures were significantly associated. Furthermore, T1 marijuana use (vs. nonuse) was significantly correlated with T1 lower effort. As expected, every possible autoregressive path of the same variable assessed in different rounds (e.g., T1 initiative to T2 initiative; T1 marijuana use to T2 marijuana use) emerged as significant.
Figure 2.
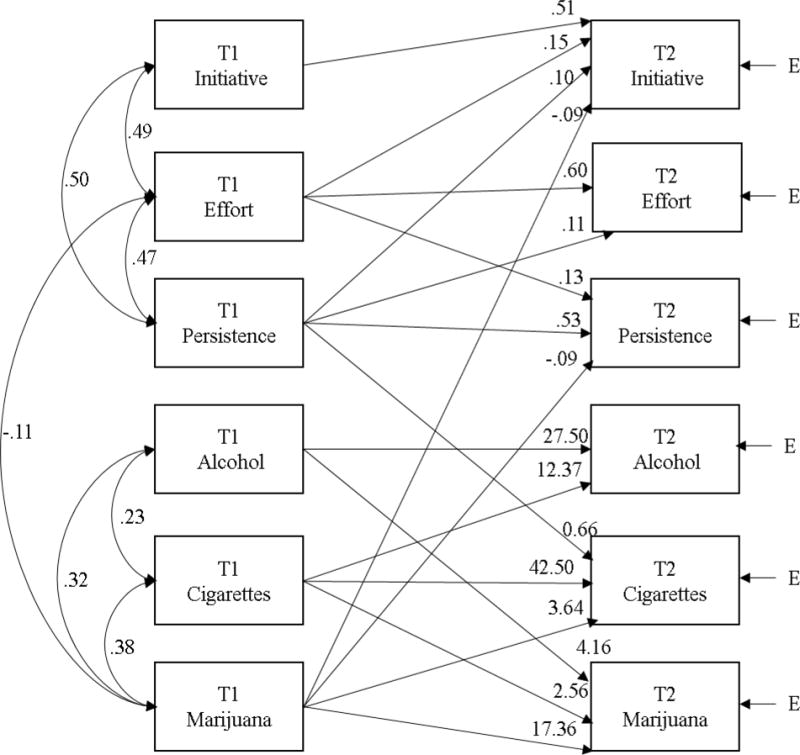
Cross-lagged panel model. All possible combinations of correlations involving T1 measures, as well as test-retest and cross-lagged paths from T1 to T2, are controlled in the model. For diagrammatic clarity, only significant (p < .05) coefficients are displayed. Coefficients to T2 initiative, effort, and persistence represent (adjusted) beta weights. Coefficients to T2 alcohol, cigarettes, and marijuana represented (adjusted) odds ratios. E = predictive error.
Next, the cross-lagged paths were evaluated (Figure 2). The general self-efficacy subscales as outcomes were interpreted first. Lower T2 initiative was longitudinally predicted by lower effort, lower persistence, and marijuana use (vs. nonuse). T2 effort was predicted by persistence. Antecedents of lower T2 persistence were lower effort and marijuana use (vs. nonuse). The substance use outcomes were interpreted next. T2 alcohol use was preceded by cigarette use; T2 cigarette use was predicted by lower persistence and marijuana intake; and T2 marijuana use was anticipated by alcohol and cigarette use. Results, taken together, reveal that the temporal precedence of events is that marijuana use promotes subsequently lower scores on two general self-efficacy subscales, but the opposite processes from reduced self-efficacy subscales to marijuana use were untenable.
Discussion
The marijuana amotivational syndrome postulates that marijuana users are more likely than nonusers to experience apathy and passivity, which may lead to loss in productivity and aversion of goal-oriented behaviors. Although past research has documented that marijuana use is related to poorer academic outcomes in adolescents and young adults (Arria et al., 2015; Phillips et al., 2015; Suerken et al., 2016), it is not entirely clear whether these connections are specific to academic domains or can be generalized to wider motivation-based constructs such as general self-efficacy. The current study applied a longitudinal design to elucidate the possibility of reciprocal relations involving marijuana use and general confidence (as represented by three self-efficacy subscales). Contrary to a recent investigation showing that general self-efficacy is longitudinally related to lower marijuana intake but did not test the process in the opposite direction (Grevenstein et al., 2016), we found that the risk pathways from marijuana use to initiative and persistence emerged as significant. Moreover, these effects remained robust even after controlling for a variety of covariates. The prediction of marijuana use on the lower effort subscale was significant without controlling for covariates, and remained significant after controlling for demographics and personality factors, but became attenuated upon inclusion of other substances. Overall, the pattern of results is mostly consistent with the amotivational syndrome and supports hypotheses positing marijuana as an antecedent of compromised general self-efficacy.
Cannabis use was a significant predictor of lower initiative and persistence over a one-month period in the study. In contrast to early investigations utilizing lifetime measures of marijuana use (e.g., Duncan, 1987; McGlothlin & West, 1968), the current investigation focused on the more recent period of past month usage. The findings from our study are similar to results applying a recent measurement interval of intake. One investigation, for example, demonstrated that a brief and immediate exposure to marijuana ingested in the laboratory curtailed motivation in performance tasks (e.g., Cherek et al., 2002; Lane et al., 2005). In the broader context of mixed findings in the literature, our investigation emphasizes the importance of specifying a suitable time frame to assess the relation between cannabis use and motivation-related outcomes. Possibly, past year or lifetime measures of cannabis intake may be less sensitive in detecting the recent psychoactive effects of the substance on the motivation to pursue, accomplish, and sustain behaviors. As such, the link from cannabis use to lower motivation-based constructs may emerge only when the investigation focuses on usage during a reasonably recent period, such as within the past day, week, or month. Future research should measure past usage of different intervals to refine the methodological understanding of the cannabis consumption to self-efficacy link based on the recency of intake.
Marijuana users reported lower levels of effort than nonusers in T1 (users also would score lower than nonusers in T2 if covariates were not incorporated). The connection between marijuana use and lower effort could preexist prior to the start of this investigation especially among chronic and long-term marijuana users. The start of this study was not based on a particular transitional or developmental period that marks the initiation or progression of marijuana use. Although speculative, the identified past month marijuana users in the current research may have been longer-term users, so that the baseline measurement of the effort subscale exhibited a significant difference between users and nonusers. In the hierarchial regression analysis, the marijuana use to effort connection was no longer significant after controlling for alcohol and tobacco use, suggesting these other substances in combination may serve as rival explanations of the temporal reduction in this self-efficacy factor.
This study possesses two notable strengths to enable stronger statistical inferences, including the application of a longitudinal design and statistically ruling out of pertinent covariates. Given that the current research provides support for the temporal link from marijuana use to general self-efficacy, findings could inform the construction of educational materials for mass media campaigns and interventions. Perceived risk of marijuana use is strongly associated with marijuana use (Merrill, 2015), so current findings showing associations of marijuana use and lower scores on two self-efficacy subscales could be applied to the design of informational messages to correct misperceptions of marijuana use risk. In motivational interviewing (Miller, & Rollnick, 2012), college counselors could draw on the current findings as a conversational centerpiece regarding the advantages and disadvantages of cannabis in the context of motivation, self-efficacy, pursuit of personal goals, and behavioral change ambivalence in student users (Walker, Stephens, Rowland, & Roffman, 2011). Finally, the findings provide informational insights for clinicians to share with clients who use marijuana and encounter motivational problems.
Findings should be interpreted in the context of limitations. First, all study variables were measured using self-reports, a data collection method that might be susceptible to report and recall bias. Second, although marijuana use is normative in college students (Fleming et al., 2012), the sample of undergraduate students enrolled in psychology courses may limit the generalizability of findings. Future research should replicate and extend the findings using noncollege attending youth and high risk adults. Third, marijuana use was treated a binary variable due to the predominance of nonusers, so the research does not provide information about the dose-response effect of marijuana use on general self-efficacy subscales. The pursuit of such an investigation would be most appropriate with a clinical sample that uses frequently. Fourth, general self-efficacy is conceptualized as a broad and encompassing efficacy construct not specific to a target behavior. Future research could examine domain specific self-efficacy as potential outcomes. Finally, although many relevant covariates were accounted for in the analyses, this listing is not exhaustive. Other important constructs such as social rejection, deviant peer affiliation, internalizing symptoms, and decreased enthusiasm for participation in conventional activities should be considered in future studies to evaluate additional mechanistic pathways (Jessor et al., 1973; Jessor, 1976; Kupfer, 1973).
In summary, despite the pivotal role of the general self-efficacy in multiple domains of human functioning (Luszczynska et al., 2005), research has neglected to examine reciprocal associations involving cannabis use and general self-efficacy subscales. The study was the first to utilize cross-lagged panel modeling to elucidate the directionality of these measures. Results found that marijuana use longitudinally predicted lower initiative and persistence, whereas the reversed directional processes were unsupported. The investigation also advances the research by documenting the unique contributions of marijuana use on general self-efficacy factors, with results varying depending on the subscale scrutinized. Future prevention research should examine possible risk and mechanistic pathways from marijuana use to other negative consequences that might ensue due to general self-efficacy reductions.
Acknowledgments
Funding. Manuscript preparation by 1st author was supported by the NIH/NIAAA Loan Repayment Program (L30 AA024314-01; PI: Lac). Manuscript preparation by the 2nd author was supported by the Institutional National Research Service Award (T32 AA013525; PI: Riley) and the Intramural Research Program of the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Footnotes
Compliance with Ethnical Standards
Disclosure of potential conflicts of interest. The authors declare that they have no conflict of interest.
Ethical approval. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent. Informed consent was obtained from all individual participants included in the study.
References
- Andersson L, Moore C, Hensing G, Krantz G, Staland-Nyman C. General self-efficacy and its relationship to self-reported mental illness and barriers to care: A general population study. Community Mental Health Journal. 2014;50(6):721–728. doi: 10.1007/s10597-014-9722-y. [DOI] [PubMed] [Google Scholar]
- Ajzen I. The theory of planned behavior. Organizational behavior and human decision processes. 1991;50(2):179–211. [Google Scholar]
- Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O’Grady KE. The academic consequences of marijuana use during college. Psychology of Addictive Behaviors. 2015;29(3):564. doi: 10.1037/adb0000108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O’Grady KE. Marijuana use trajectories during college predict health outcomes nine years postmatriculation. Drug & Alcohol Dependence. 2016;159:158–165. doi: 10.1016/j.drugalcdep.2015.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977;84(2):191–215. doi: 10.1037//0033-295x.84.2.191. [DOI] [PubMed] [Google Scholar]
- Bandura A. Self-efficacy. John Wiley & Sons; 1994. [Google Scholar]
- Barnwell SS, Earleywine M, Wilcox R. Cannabis, motivation, and life satisfaction in an internet sample. Substance Abuse Treatment, Prevention, and Policy. 2006;1:2. doi: 10.1186/1747-597X-1-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blows S, Ivers RQ, Connor J, Ameratunga S, Woodward M, Norton R. Marijuana use and car crash injury. Addiction. 2005;100(5):605–611. doi: 10.1111/j.1360-0443.2005.01100.x. [DOI] [PubMed] [Google Scholar]
- Bosscher RJ, Smit JH. Confirmatory factor analysis of the general self-efficacy scale. Behaviour Research and Therapy. 1988;36:330–343. doi: 10.1016/s0005-7967(98)00025-4. [DOI] [PubMed] [Google Scholar]
- Buckner JD, Ecker AH, Cohen AS. Mental health problems and interest in marijuana treatment among marijuana-using college students. Addictive Behaviors. 2010;35(9):826–833. doi: 10.1016/j.addbeh.2010.04.001. [DOI] [PubMed] [Google Scholar]
- Caldeira KM, O’Grady KE, Vincent KB, Arria AM. Marijuana use trajectories during the post-college transition: Health outcomes in young adulthood. Drug & Alcohol Dependence. 2012;125(3):267–275. doi: 10.1016/j.drugalcdep.2012.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cattell RB. The scree test for the number of factors. Multivariate Behaviorial Research. 1966;1:245–276. doi: 10.1207/s15327906mbr0102_10. [DOI] [PubMed] [Google Scholar]
- Chen G, Gully SM, Eden D. Validation of a new general self-efficacy scale. Organizational Research Methods. 2001;4(1):62–83. [Google Scholar]
- Cherek DR, Lane SD, Dougherty DM. Possible amotivational effects following marijuana smoking under laboratory conditions. Experimental and Clinical Psychopharmacology. 2002;10(1):26–38. doi: 10.1037//1064-1297.10.1.26. [DOI] [PubMed] [Google Scholar]
- Conroy DA, Kurth ME, Brower KJ, Strong DR, Stein MD. Impact of marijuana use on self-rated cognition in young adult men and women. The American Journal on Addictions. 2015;24(2):160–165. doi: 10.1111/ajad.12157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa PT, McCrae RR. Domains and facets: Hierarchical personality assessment using the revised neo personality inventory. Journal of Personality Assessment. 1995;64:21–50. doi: 10.1207/s15327752jpa6401_2. [DOI] [PubMed] [Google Scholar]
- Crano WD, Brewer MB, Lac A. Principles and methods of social research. 3rd. New York: Routledge; 2015. [Google Scholar]
- Crano WD, Lac A. The evolution of research methodologies in social psychology: A historical analysis. In: Kruglanski AW, Stroebe W, editors. Handbook of the history of social psychology. New York: Psychology Press; 2012. pp. 159–174. [Google Scholar]
- Duncan DF. Lifetime prevalence of “amotivational syndrome” among users and nonusers of hashish. Psychology of Addictive Behaviors. 1987;1(2):114–119. [Google Scholar]
- Fleming CB, White HR, Haggerty KP, Abbott RD, Catalano RF. Educational paths and substance use from adolescence into early adulthood. Journal of Drug Issues. 2012;42(2):104–126. doi: 10.1177/0022042612446590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fridberg DJ, Vollmer JM, O’Donnell BF, Skosnik PD. Cannabis users differ from non-users on measures of personality and schizotypy. Psychiatry Research. 2011;186(1):46–52. doi: 10.1016/j.psychres.2010.07.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorsuch R. Factor analysis. Hillsdale, NJ: Lawrence Erlbaum Associates; 1983. [Google Scholar]
- Grevenstein D, Bluemke M, Kroeninger-Jungaberle H. Incremental validity of sense of coherence, neuroticism, extraversion, and general self-efficacy: Longitudinal prediction of substance use frequency and mental health. Health & Quality of Life Outcomes. 2016;14:9. doi: 10.1186/s12955-016-0412-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasin DS, Saha TD, Kerridge BT, Goldstein RB, Chou SP, Zhang H, Huang B. Prevalence of marijuana use disorders in the United States between 2001–2002 and 2012–2013. JAMA Psychiatry. 2015;72(12):1235–1242. doi: 10.1001/jamapsychiatry.2015.1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor R, Jessor SL, Finney J. A social psychology of marijuana use: Longitudinal studies of high school and college youth. Journal of Personality and Social Psychology. 1973;26(1):1–15. doi: 10.1037/h0034214. [DOI] [PubMed] [Google Scholar]
- Jessor R. Predicting time of onset of marijuana use: A developmental study of high school youth. Journal of Consulting and Clinical Psychology. 1976;44(1):125–134. doi: 10.1037//0022-006x.44.1.125. [DOI] [PubMed] [Google Scholar]
- John OP. The ‘big five’ factor taxonomy: Dimensions of personality in the natural language and in questionnaires. In: Pervin LA, editor. Handbook of personality: Theory and research. New York, NY, US: Guilford Press; 1990. pp. 66–100. [Google Scholar]
- John OP, Srivastava S. The big five trait taxonomy: History, measurement, and theoretical perspectives. In: Pervin LA, John OP, editors. Handbook of personality: Theory and research. 2nd. New York, NY, US: Guilford Press; 1999. pp. 102–138. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Miech RA. Monitoring the Future national survey results on drug use, 1975–2014: Volume 2, College students and adults ages 19–55. Ann Arbor: Institute for Social Research, The University of Michigan; 2015. [Google Scholar]
- Kaiser HF. The application of electronic computers to factor analysis. Educational and Psychological Measurement. 1960;20:141–151. [Google Scholar]
- Keith DR, Hart CL, McNeil MP, Silver R, Goodwin RD. Frequent marijuana use, binge drinking and mental health problems among undergraduates. American Journal on Addictions. 2015;24(6):499–506. doi: 10.1111/ajad.12201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenny DA. Cross-lagged panel correlation – test for spuriousness. Psychological Bulletin. 1975;82:887–903. [Google Scholar]
- Kupfer DJ, Detre T, Koral J, Fajans P. A comment on the “amotivational syndrome” in marijuana smokers. American Journal of Psychiatry. 1973;130(12):1319–1322. doi: 10.1176/ajp.130.12.1319. [DOI] [PubMed] [Google Scholar]
- Kvarme LG, Haraldstad K, Helseth S, Sørum R, Natvig GK. Associations between general self-efficacy and health-related quality of life among 12–13-year-old school children: A cross-sectional survey. Health and Quality of Life Outcomes. 2009;7:85. doi: 10.1186/1477-7525-7-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lac A. Longitudinal Designs. In: Levesque RJR, editor. Encyclopedia of adolescence. Switzerland: Springer International; 2016. pp. 1–6. [Google Scholar]
- Lac A, Crano WD. Marijuana use. In: Levesque RJR, editor. Encyclopedia of Adolescence. 2nd. Switzerland: Springer International; 2016. pp. 1–8. [Google Scholar]
- Lane SD, Cherek DR, Pietras CJ, Steinberg JL. Performance of heavy marijuana-smoking adolescents on a laboratory measure of motivation. Addictive Behaviors. 2005;30(4):815–828. doi: 10.1016/j.addbeh.2004.08.026. [DOI] [PubMed] [Google Scholar]
- Locascio JJ. The cross-lagged correlation technique: Reconsideration in terms of exploaratory utilility, assumption specification and robustness. Educational and Psychological Measurement. 1982;42:1023–1036. [Google Scholar]
- Luszczynska A, Gutiérez-Doña B, Schwarzer R. General self-efficacy in various domains of human functioning: Evidence from five countries. International Journal of Psychology. 2005;40(2):80–89. doi: 10.1080/00207590444000041. [DOI] [Google Scholar]
- Lynskey M, Hall W. The effects of adolescent cannabis use on educational attainment: A review. Addiction. 2000;95(11):1621–1630. doi: 10.1046/j.1360-0443.2000.951116213.x. [DOI] [PubMed] [Google Scholar]
- McCaffrey DF, Liccardo Pacula R, Han B, Ellickson P. Marijuana use and high school dropout: The influence of unobservables. Health Economics. 2010;19(11):1281–1299. doi: 10.1002/hec.1561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGlothlin WH, West LJ. The marihuana problem: An overview. American Journal of Psychiatry. 1968;125(3):370–378. [PubMed] [Google Scholar]
- Mellinger GD, Somers RH, Davidson ST, Manheimer DI. The amotivational syndrome and the college student. Annals of the New York Academy of Sciences. 1976;282(1):37–55. doi: 10.1111/j.1749-6632.1976.tb49883.x. [DOI] [PubMed] [Google Scholar]
- Merrill RM. Use of marijuana and changing risk perceptions. American Journal of Health Behavior. 2015;39(3):308–317. doi: 10.5993/AJHB.39.3.3. [DOI] [PubMed] [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Helping people change. Guilford press; 2012. [Google Scholar]
- Muthén L, Muthén B. Mplus user’s guide. 6th. Los Angeles, CA: Muthén & Muthén; 2010. [Google Scholar]
- Natvig GK, Albrektsen G, Qvarnstrém U. Associations between psychosocial factors and happiness among school adolescents. International Journal of Nursing Practice. 2003;9(3):166–175. doi: 10.1046/j.1440-172X.2003.00419.x. [DOI] [PubMed] [Google Scholar]
- Pacek LR, Mauro PM, Martins SS. Perceived risk of regular cannabis use in the United States from 2002 to 2012: Differences by sex, age, and race/ethnicity. Drug and Alcohol Dependence. 2015;149:232–244. doi: 10.1016/j.drugalcdep.2015.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phillips KT, Phillips MM, Lalonde TL, Tormohlen KN. Marijuana use, craving, and academic motivation and performance among college students: An in-the-moment study. Addictive Behaviors. 2015;47:42–47. doi: 10.1016/j.addbeh.2015.03.020. [DOI] [PubMed] [Google Scholar]
- Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Education & Behavior. 1988;15(2):175–183. doi: 10.1177/109019818801500203. [DOI] [PubMed] [Google Scholar]
- Shadish WR, Cook TD, Campbel DT. Experimental and quasi-experiemtal designs for generalized causal inference. Boston, MA: Houghton, Mifflin and Company; 2002. [Google Scholar]
- Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers RW. The self-efficacy scale: Construction and validation. Psychological Reports. 1982;51:663–671. [Google Scholar]
- Smith DE. Acute and chronic toxicity of marijuana. Journal of Psychoactive Drugs. 1968;2(1):37–48. [Google Scholar]
- Suerken CK, Reboussin BA, Sutfin EL, Wagoner KG, Spangler J, Wolfson M. Prevalence of marijuana use at college entry and risk factors for initiation during freshman year. Addictive Behaviors. 2014;39(1):302–307. doi: 10.1016/j.addbeh.2013.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suerken CK, Reboussin BA, Egan KL, Sutfin EL, Wagoner KG, Spangler J, Wolfson M. Marijuana use trajectories and academic outcomes among college students. Drug and Alcohol Dependence. 2016;162:137–145. doi: 10.1016/j.drugalcdep.2016.02.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swain NR, Gibb SJ, Horwood L, Fergusson DM. Alcohol and cannabis abuse/dependence symptoms and life satisfaction in young adulthood. Drug and Alcohol Review. 2012;31(3):327–333. doi: 10.1111/j.1465-3362.2011.00339.x. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. Upper Saddle River, N.J.: Pearson Education; 2012. [Google Scholar]
- Terracciano A, Löckenhoff CE, Crum RM, Bienvenu OJ, Costa PT. Five-Factor Model personality profiles of drug users. BMC Psychiatry. 2008;8(1):22. doi: 10.1186/1471-244X-8-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volkow ND, Baler RD, Compton WM, Weiss SB. Adverse health effects of marijuana use. New England Journal Of Medicine. 2014;370(23):2219–2227. doi: 10.1056/NEJMral402309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volkow ND, Swanson JM, Evins AE, DeLisi LE, Meier MH, Gonzalez R, Baler R. Effects of cannabis use on human behavior, including cognition, motivation, and psychosis: A review. JAMA psychiatry. 2016;73(3):292–297. doi: 10.1001/jamapsychiatry.2015.3278. [DOI] [PubMed] [Google Scholar]
- Walker D, Stephens R, Rowland J, Roffman R. The influence of client behavior during motivational interviewing on marijuana treatment outcome. Addictive Behaviors. 2011;36(6):669–673. doi: 10.1016/j.addbeh.2011.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warner RM. Applied statistics: From bivariate through multivariate techniques. 2nd. Thousand Oaks, CA, US: Sage Publications, Inc; 2013. [Google Scholar]