

Abstract
Child Anxiety Tales, an online web-based cognitive-behavioral parent-training program for parents of youth with anxiety, was developed and evaluated. Parents (N = 73; 59 females; 52.1% Caucasian, 42.5% African American, 4.1% Hispanic) who reported concerns about anxiety in their child (aged 7–14 yrs; Mean=10.1 ±1.6) were randomly assigned to (a) parent-training provided through Child Anxiety Tales (CAT), (b) parent-training provided via bibliotherapy (BIB), or (c) a waitlist control (WLC). Measures of parent knowledge, the acceptability of training, and child symptomatology were completed at pre- and post-parent-training and at 3-month follow-up. Findings support the feasibility, acceptability, and beneficial effects on knowledge of Child Anxiety Tales for parents of youth with impairment from anxiety.
Progress has been made in the identification and treatment of anxiety disorders in children and adolescents and cognitive behavioral therapy (CBT), having met the criteria used for evaluation, has been deemed an empirically-supported treatment (Hollon & Beck, 2013). Despite these advances, with over 13% of youth requiring services for anxiety (as many as 14 million youth; Costello et al., 2005; US Census Report 2012) and the limited supply of mental health professionals trained in providing evidence based treatments, something is needed to close the gap. Such prevalence numbers are conservative estimates of the true need, given that many youth experience distressing anxiety that, though below diagnostic threshold, is nevertheless associated with dysfunction and impairment. To move closer to meeting the need there is a growing emphasis on broadening the array of treatment delivery formats to include online and computer-based efforts (Kendall, Carper, Khanna & Harris, 2014).
CBT, typically provided face-to-face, is the first-line treatment of choice for childhood anxiety disorders, with evidence supporting its efficacy and durability (e.g., Kendall et al., 2008; Walkup et al., 2008). CBT is empirically-supported and recommended, but a variety of barriers prevent many of those in need from receiving such service. These barriers include a lack of access to facilities and practitioners and matters of finance (cost or insufficient insurance coverage; Diala et al. 2000; Kataoka et al. 2003; Mechanic et al. 2002; Pumariega et al. 1998). Additional delivery formats are urgently needed.
A growing literature supports internet-based interventions for mental health conditions (for review see Anderrson, 2010; Myers & Turvey, 2013). Unlike individual face-to-face therapy, technology capitalizes on the ability to reach a large proportion of the population in need of services and offers opportunities for paraprofessionals to oversee the administration of the interventions (Kazdin, 2015; Kazdin & Blaze, 2011). An effective intervention that can be delivered by paraprofessionals (or parents in their own home) would overcome barriers and reach many youth.
Parents/guardians who are concerned about their child’s difficulties related to excessive anxiety and stress are in a valuable position to serve as change-agents for their children. Parent-based interventions have been found to be effective in reducing impairment in youth (e.g., Parent Effectiveness Training, see Cedar & Levant, 1990; parent-training videos for managing conduct problems; Webster-Stratton et al., 1989), and parents have administered interventions that have benefited other parents (Hoagwood et al., 2010). Parents often turn to self-help printed materials (bibliotherapy) to guide how they try to help their children (Elgar & McGrath, 2003). However, bibliotherapy has shortcomings. First, many resources are of questionable quality, and most lack empirical support (Scogin, 2003; Redding, Herber, Forman, & Gaudiano, 2007). Second, Bibliotherapy (BIB) lacks step-by-step audio/visual guides and/or interactive learning experiences that can increase both the engagement in and the effectiveness of the program. Lastly, the content cannot be easily/quickly updated (Marks, et al., 2007).
Computer-based parent-training programs offer an accessible, private, convenient, and engaging resource for parents who would like to learn how to manage their child’s difficulties…such as how to help their child better manage anxiety (Spence, Holmes, March, & Lipp, 2006). Giving concerned parents access to web-based information may also promote awareness of and/or initiation of empirically supported treatments for youth who are in need (Kenardy, McCafferty & Rosa, 2003). A web-based format is transportable between work and home settings, and has 24-hour access and confidentiality (Bogels & Phares, 2007). The multimedia content provides active engagement and multiple forms of learning (auditory, visual), which may allow for better processing and understanding. These positive factors may increase the likelihood that parents will be involved (e.g., both parents, under-served populations (Elgar & McGrath, 2003), will be more informed about child anxiety and evidence-based strategies for anxiety management, and will be able to implement the strategies effectively with their child. For those youth who may require more intensive treatment, the training may set the stage and encourage parents to seek access to evidence-based treatments (Kenardy, McCafferty & Rosa, 2003). From both an individual and public health perspective, there is substantial potential in self-guided parent-training interventions to improve the mental health of children and families (Scogin, 2003).
The present project developed and evaluated an online parent-training program for parents of youth (7–17 years of age) with anxiety. We worked with parents of anxious youth (from both clinical and non-clinical samples) and with CBT experts using an iterative process to develop and beta-test the resulting modules to ensure ease of use, clarity, utility, and treatment integrity. It was hypothesized that parents would report higher rates of acceptability for the Child Anxiety Tales program than for either bibliotherapy (BIB) or waitlist (WLC), and that both Child Anxiety Tales and BIB would produce significant beneficial change in parent knowledge from pre- to post-training, with the gains being significantly better than those for WLC participants. It was expected that the changes seen following training would remain at 3-month follow-up. In addition, using parent-report of anxiety symptoms in youth at post-training and 3-month follow-up, we examined the effectiveness of Child Anxiety Tales compared to BIB and WLC, and we explored factors (e.g., youth age; parent age) that may be related to outcomes.
Methods
Participants
Parents (N=73, 59 females) of youth who reported being concerned regarding their child’s anxiety and distress were participants. A 20-minute semi-scripted telephone screening procedure was followed to elicit preliminary inclusion/exclusion information and to provide additional information to potential participants. Parents were included if they were English speaking, able to read/understand an English-language newspaper, had access to a computer with a DVD Rom drive and/or internet access, and who expressed sufficient concern about anxiety in their child (CBCL-A T score ≥60). Parents were not eligible if (a) their child was receiving alternate treatments (e.g., medications, CBT) for anxiety or mood problems, or reported symptoms that demanded immediate attention (e.g., suicidal risk, psychotic symptoms). If a child diagnosis of an anxiety disorder was suspected (≥70 on CBCL-A/D), referrals were also provided for a complete diagnostic evaluation.
Measures
Parent Knowledge Questionnaire
Parents were asked about child anxiety and about factors that can maintain anxiety in youth. This questionnaire was based on the items from the competency test for CBT therapists used in the CAMS trial (Walkup et al, 2008), with adaptations to assess “parents’” knowledge about anxiety and how to parent an anxious child. Parents completed the measure at pre- and post-training and at 3-month follow-up.
Client Satisfaction Questionnaire (CSQ; Larsen et al., 1979)
The CSQ-8 is a widely used 8-item measure of client satisfaction (Godley et al., 1998; Lehrman-Waterman & Ladany, 2001) that has shown strong retest reliability, internal consistency (Ladany & Lehrman-Waterman et al., 1999), and sensitivity to treatment (Nguyen et al., 1983). Nguyen et al. (1983) reported that the CSQ-8 discriminated groups and did not suffer from the “ceiling effects.” At post-training, parents rated satisfaction with their randomly-assigned training condition.
Computer Experience Questionnaire (CEQ)
The CEQ assesses the parent/user’s experience with and comfort using computers. The CEQ is a 4-item (5-point) scale that parents completed pre-training.
Child Anxiety Tales Feedback Forms
Feedback forms have been developed to collect specific feedback on each user’s experience with the Child Anxiety Tales program. The measure appeared at the end of each of the web-based modules to rate their experience. The form included items assessing participant self-reported ease of use and navigation, clarity, utility, pace, appeal, likelihood of remembering the content, likelihood of recommending to others, and an open-ended section to provide recommendations or comments. These data informed the final version of the program. Only parents randomized to WPT completed this measure.
Child Behavior Checklist-Anxiety Subscale (CBCL-A; Achenbach, 1991; Kendall et al., 2007)
The 18-item CBCL-A was used as a parent measure of child anxiety symptomotology. The CBCL-A is a scale developed from CBCL items (Achenbach, 1991) to assess anxious symptomatology. Items are rated 0 to 2 depending on the degree to which the particular statement characterizes the child. CBCL-A scores significantly discriminated AD children from NAD children and correlated significantly with other measures of child anxiety and was sensitive to treatment changes (Kendall et al., 2007).
Spence Children’s Anxiety Scale – Parent Version (SCASp; Spence, 1999)
The 38-item SCASp asks parents about their child’s anxiety symptoms. Scores (0 to 114) have good internal consistency (.89), and distinguish diagnosed anxious youth from nonclinical children (Spence et al., 2003; Nauta et al., 2004).
Procedures
Parent(s) were recruited via FocusPointe, a company that supports recruitment from general population for research purposes. Potential participants completed a brief telephone screening before being invited for further assessment. Parents signed informed consent prior to the assessment with the understanding that there would be random assignment to 1 of 3 conditions (i.e., Child Anxiety Tales, BIB, WLC). Participants completed pre-training measures and then completed the training (or wait period) on their own over the next 10 weeks. Participants returned to complete post-training assessment at the end of 10 weeks, and again to complete the 3-month follow-up. At follow-up, parents completed the measure of their satisfaction, and again completed measures of knowledge and child symptoms. Parents in the Child Anxiety Tales condition completed feedback forms regarding their experience with the Child Anxiety Tales program specific to each module. Those in the WLC, at the end of the wait period and after their WL assessment, were offered their choice of either parent-training modality.
Conditions
“Child Anxiety Tales:” A web-based parent-training program (Kendall & Khanna, 2014; see Figure 1. Sample Screens)
Figure 1.

Sample Screens
Parents randomized to Child Anxiety Tales received link access to the Child Anxiety Tales program for 10 weeks. Parents were instructed to watch and interact with the Child Anxiety Tales program and apply the strategies described to help their child develop skills to cope with anxiety. Parents could work at their own pace, but were expected to complete the program within 10 weeks. Reminders regarding the timeline and the upcoming post-training assessment were sent at the end of weeks 8 and 9.
Child Anxiety Tales was designed and developed by a multidisciplinary team of researchers, programmers, parents, and therapists. The development process included (a) script drafts, (b) expert panel review, (c) storyboard development, (d) beta development, and (e) beta testing. The program script was based on cognitive-behavioral principles of anxiety (Kendall & Hedtke, 2006) and effective parent-training strategies found to benefit anxious youth (Khanna & Kendall, 2010). Focus groups were held with (a) parents of anxious youth and (b) therapists working with anxious youth and their parents. Feedback was incorporated into the final script that was sent to expert CBT therapists for review. Feedback was again incorporated, with the final draft including recommendations for the audio, video inserts, animation (flash and static), and interactive learning activities.
The resulting Child Anxiety Tales program consists of 10 modules to educate and empower parents to help their child better manage anxiety (see Table 1). Based on information provided by the parent during completion of the screener, users are provided with some modules that contain the same content for all parents (e.g., Modules 1, 2) and other modules that are specific to the description they provided of their child. Within these personalized modules, users view and interact with the tale of a child with anxiety problems akin to those of their own child, and are provided with opportunities to make choices and see how such choices would likely impact the child. Child Anxiety Tales is housed within a website: www.CopingCatParents.com. The website provides a symptom checker, information and resources on anxiety and its treatment, a library of audio/video illustrations, and references including parent testimonials and treatment strategy samples. All are provided to help empower parents to help them help their children struggling with anxiety.
Table 1.
Child Anxiety Tales module descriptions
| Title | Content | |
|---|---|---|
| 1 | Symptoms of Anxiety | Psychoeducation about the nature of anxiety, the physiological symptoms of anxiety, when anxiety is normal, and ways that the symptoms may be seen in real situations. |
| 2 | CBT for Anxiety | An illustrated presentation of the guiding principles and components of CBT (e.g., affective education, relaxation training, changing self-talk, problem-solving, exposure tasks). |
| 3 | Myth busters | An interactivity that addresses common misconceptions about anxiety and what maintains anxiety |
| 4 | Relaxation Training | Training in breathing and relaxation strategies for parents to use and teach to their child. |
| 5 | the FEAR plan | An overview of “the steps” to managing anxiety. |
| 6 | Challenging Anxious Thoughts | Instructions on helping their child develop coping strategies to challenge anxious self-talk. |
| 7 | Problem-Solving | The process of problem-solving, as well as how parents can both teach their child problem-solving skills and provide opportunities for them to practice. |
| 8 | Rewards and Consequence | An overview of contingency management, and tips for consistent praise and rewarding for effort. |
| 9 | Exposure tasks | Principles and illustrative examples describing approach vs. avoidance and strategies for encouraging approach and step-by-step instructions on planning opportunities for real-world practice. |
| 10 | Preventing Relapse | A summary/review of the program, along with tips and strategies to help maintain gains. |
Bibliotherapy (BIB)
Each parent randomized to BIB was provided with “Helping Your Anxious Child: A Step-by-Step Guide (Rapee, Spence, Cobham, & Wignall, 2000).” This book was chosen because it is the best available–its efficacy was evaluated in research and supported (compared to waitlist and to standard group treatment). Rapee et al (2006) reported that children whose parents received bibliotherapy with no therapist contact benefited more than children of WL parents. In the present study, parents were instructed to read the chapters and apply the strategies described in them to help their child develop skills to cope with anxiety. Parents were able to work at their own pace, but were asked to complete the reading within 10 weeks. Reminders regarding the timeline and the upcoming post-training assessment were sent at the end of weeks 8 and 9.
Waitlist Control (WLC)
Parents assigned to WLC were assessed at pre- and post-, separated by 10 weeks. After parents completed the post-training assessment, they were offered their choice of either Child Anxiety Tales or BIB.
Data Analysis
Power
Sample size was determined by conducting power analyses for the primary aims of the study. Based on the effect sizes reported from a meta-analysis (Den Boer, et al., 2004; moderate to large effects between bibliotherapy and treatment as usual), the current project required a sample of 18 participants per condition to achieve a power of .80 to detect significant differences (p < .05) between WPT, BIB and WLC (Faul, Erdfelder, Lang, & Buchner, 2007). A sample size of 20 participants per condition provides power greater than .80 to detect differences among conditions at posttraining. Analyses for the secondary aims were exploratory. For these analyses we report significant results after correcting for multiple tests and giving careful consideration of their relationship with other findings.
Pretraining comparisons
To examine differences across conditions (on pretraining variables), ANOVA tests were used. These and subsequent analyses using ANOVA were followed (when appropriate) by Scheffe tests. Using χ2 tests for categorical variables and one-way analyses of variance (ANOVAs) for continuous variables, comparisons of group differences were conducted on pretraining measures (e.g., baseline knowledge, computer experience, child symptoms). Analyses were conducted to examine relationships with subject characteristics (e.g., age). Tests were also conducted to examine differences between completers and noncompleters (e.g., not participating at follow-up) on demographic and pretraining measures.
Dependent Variables
Differences/changes on measures of satisfaction, knowledge, and child anxious symptoms, from pre- to post-training for all conditions were evaluated using 3 (condition, between subjects) × 2 (time, within subjects) repeated measures mixed factorial ANOVAs. Outcome variables were evaluated using the intent-to-treat sample (i.e., all cases included at randomization).
Although there are no specific hypotheses regarding the potential role of computer experience, gender and/or ethnicity, we explored outcomes with regard to these variables.
Follow-up
Participants were assessed at 3-months post-training. Given that WLC participants had received Child Anxiety Tales or BIB after the wait period, they were not included in follow-up analyses. Two (condition, between subjects) × 2 (time, within subjects) repeated measures mixed factorial ANOVAs were used to examine changes from pretraining to follow-up. Note: we did not test that posttraining and follow-up scores will not differ significantly (that would be testing the null hypothesis), but rather tested for significant differences between pretraining and follow-up. It was hypothesized that both training conditions will produce significant change in the dependent variables, and that improvement will be greater for the Child Anxiety Tales than the BIB condition.
Results
Participants and Demographic Information
A total of 110 potential participants were recruited and eligible for participation. Of the 110 eligible participants, 73 signed consent forms, completed the baseline evaluation, and were randomly assigned to Child Anxiety Tales (n = 25), BIB (n = 24), or WLC (n = 24). Eleven participants (15.1%) did not attend the post-training evaluation and 26 participants (35.6%) did not attend the follow-up evaluation. A CONSORT diagram is presented as Figure 2.
Figure 2.
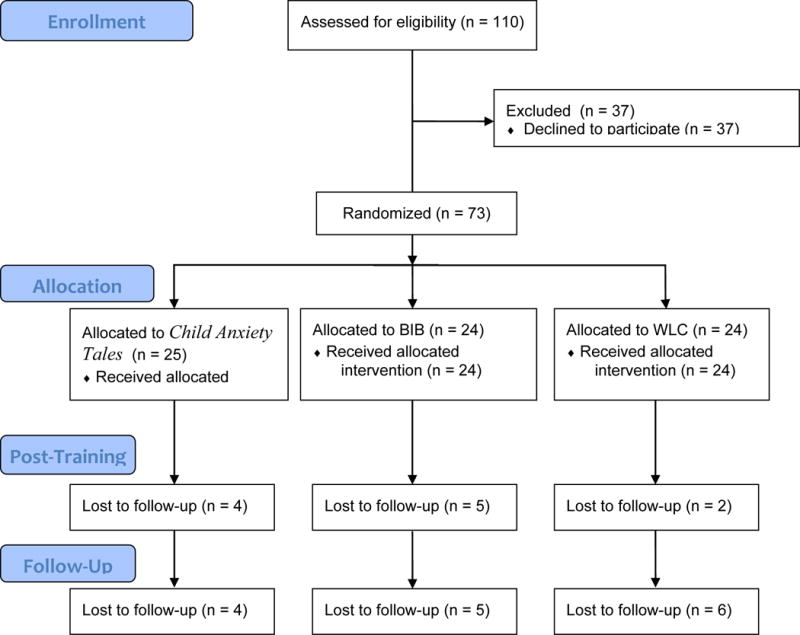
CONSORT diagram of participant flow
There were no significant differences in participants across conditions on demographic variables. The mean age of parents was 43.25 years (SD = 7.53 years). The sample included comparable numbers of African American (42.5%) and Caucasian (52.1%) participants. Roughly 80% of participants attended a professional or trade school, college, or graduate school. The majority of participants were married (58.9%) and the mean age of the child whose anxiety participants were concerned about was 12.64 years (SD = 3.16 years). Further demographic characteristics of participants, including comparisons across conditions, are presented in Table 2.
Table 2.
Baseline characteristics of study participants by training condition.
| Variable | Child Anxiety Tales (n=25) | BPT (n = 24) | WLC (n=24) | Total (n=73) | p |
|---|---|---|---|---|---|
| Demographic Characteristics | |||||
| Age – M (SD) | 45.24 (7.65) | 42.08 (7.37) | 42.33 (7.64) | 43.25 (7.53) | 0.27 |
| Female – n (%) | 20 (80.0) | 21 (87.5) | 18 (75.0) | 59 (80.8) | 0.54 |
| Race – n (%) | 0.50 | ||||
| - White | 11 (44.0) | 14 (58.3) | 13 (54.2) | 38 (52.1) | |
| - African American/Black | 13 (52.0) | 9 (37.5) | 9 (37.5) | 31 (42.5) | |
| - Multiracial | 0 (0) | 1 (4.2) | 2 (8.3) | 3 (4.1) | |
| - Other | 1 (4.0) | 0 (0) | 0 (0) | 1 (1.4) | |
| Hispanic or Latino/a – n (%) | 2 (8.0) | 1 (4.2) | 0 (0) | 3 (4.1) | |
| Education – n (%) | 0.48 | ||||
| - High school or less | 7 (28.0) | 2 (8.3) | 6 (25.0) | 15 (20.5) | |
| - College | 15 (60.0) | 18 (75.0) | 14 (58.3) | 47 (64.4) | |
| - Graduate school | 3 (12.0) | 4 (16.7) | 4 (16.7) | 11 (15.1) | |
| Household Income – n (%) | 0.10 | ||||
| - Less than $50,000 | 16 (64.0) | 8 (33.3) | 11 (45.8) | 35 (47.9) | |
| - $50,001 to $100,000 | 7 (28.0) | 13 (54.2) | 7 (29.2) | 27 (37.0) | |
| - Greater than $100,000 | 2 (8.0) | 3 (12.5) | 6 (25.0) | 11 (15.1) | |
|
| |||||
| Clinical Characteristics | |||||
| CBCL-A – M (SD) | 14.96 (5.59) | 16.38 (5.56) | 16.96 (4.45) | 16.08 (5.23) | 0.39 |
| CEQ – M (SD) | 24.68 (0.90) | 23.71 (1.94) | 24.17 (2.35) | 24.19 (1.85) | 0.18 |
| PKT – M (SD) | 5.78 (2.74) | 5.40 (2.17) | 5.94 (2.53) | 5.71 (2.47) | 0.74 |
Note: CBCL-A = Child Behavior Checklist – Anxiety subscale; CEQ = Computer Experience Questionnaire; PKT = Parent Knowledge Test.
Data Screening
Analyses for skewness and kurtosis revealed that study variables were approximately normally distributed and reflected an adequate range. Variables were examined for missingness, and analyses indicated that participants who did not attend the post-training and/or follow-up evaluation did not differ from those who did (all p’s > 0.05). Analyses were performed in two ways: using the last observation carried forward (LOCF) and using multiple imputation assuming missingness at random (MAR). Results were similar for the two missing-data methods. We report the results using the conservative LOCF. Means and standard deviations of dependent variables at each time point for each study condition are presented in Table 3.
Table 3.
Means and standard deviations of dependent variables at each time point by study condition.
| Pretraining | Posttraining | 3-Month Follow Up | |||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Child Anxiety Tales | BPT | WLC | Child Anxiety Tales | BPT | WLC | Child Anxiety Tales | BPT | WLC | |
| Knowledge Test | 5.78 (2.74) |
5.40 (2.17) |
5.94 (2.53) |
9.44 (5.05) |
7.56 (2.94) |
6.04 (3.10) |
9.00 (5.35) |
8.17 (2.91) |
– |
| CBCL-A | 14.96 (5.59) |
16.38 (5.56) |
16.96 (4.45) |
10.88 (4.94) |
11.67 (6.42) |
13.46 (5.53) |
9.84 (5.15) |
11.29 (6.27) |
– |
| SCAS-P | 12.06 (10.37) |
9.12 (7.03) |
11.05 (8.12) |
20.71 (14.64) |
20.00 (13.67) |
25.30 (14.41) |
17.21 (9.17) |
20.19 (14.97) |
– |
| CSQ-8 | – | – | – | 27.24 (2.88) |
25.47 (3.34) |
17.91 (3.10) |
27.71 (3.41) |
24.47 (3.79) |
– |
Note: Means and standard deviations presented at posttraining and follow-up are from the intent-to-treat sample. CBCL-A = Child Behavior Checklist – Anxiety Subscale; SCAS-P = Spence Children’s Anxiety Scale – Parent Version; CSQ-8 = Client Evaluation of Services – 8-item.
Post-training Outcomes
Regarding knowledge of CBT principles, a significant Training Condition × Time interaction was found, F(2,70) = 10.12, p < 0.001, ω2 = 0.22. Simple effects were calculated for each condition and for condition at time. There was a significant effect of time for Child Anxiety Tales participants (t = 6.59, p < 0.001) and for BIB participants (t = 3.82, p < 0.001). No significant differences in knowledge from pre- to post-training were found for those participants in the WLC condition, t = 0.18, p = 0.86.
Evaluating child anxiety using the CBCL-A scores, there was a significant main effect of time, F(1, 70) = 44.53, p < 0.001, ω2 = 0.39. The simple effects of time were significant for participants in all conditions: Child Anxiety Tales (t = −3.89, p < 0.001); BIB (t = −4.40, p < 0.001), and WLC (t = −3.27, p < 0.01).
Regarding SCAS-P scores, there was a significant main effect of time, F(1, 50) = 98.03, p < 0.001, ω2 = 0.66, and a marginally significant Training Condition × Time interaction, F(2, 50) = 2.97, p = 0.059, ω2 = 0.11. The simple effects of time were significant for participants across conditions: Child Anxiety Tales (t = 5.24, p < 0.001), BIB (t = 4.16, p < 0.001), WLC (t = 7.87, p < 0.001), such that there were significant SCAS-P increases for participants in all conditions.
Maintenance at Follow-Up
Regarding knowledge of CBT principles, there was a significant main effect of time, F(1, 47) = 32.07, p < 0.001, ω2 = 0.41. Participants in the Child Anxiety Tales (t = 5.35, p < 0.001) and BIB (t = 3.67, p ≤ 0.001) conditions evidenced increased knowledge from pre-training to 3-month follow-up. Regarding CBCL-A scores, there was a significant main effect of time, F(1, 47) = 37.67, p < 0.001, ω2 = 0.45. Participants in the Child Anxiety Tales (t = −4.40, p < 0.001) and BIB (t = −4.28, p < 0.001) conditions evidenced decreased CBCL-A scores from pre-training to 3-month follow-up. Similarly, regarding SCAS-P scores, there was a significant main effect of time, F(1, 32) = 16.36, p < 0.001, ω2 = 0.34. Scores on the SCAS-P increased for participants in the Child Anxiety Tales (t = 2.21, p < 0.05) and BIB (t = 3.51, p ≤ 0.001) conditions from pre-training to follow-up.
Satisfaction Outcomes
A one-way ANOVA compared participant satisfaction at post-training across conditions. Significant differences emerged, F(2, 59) = 54.72, p < 0.001. Satisfaction with Child Anxiety Tales (M = 27.24, SD = 2.88) was significantly higher than the WLC condition (M = 17.91, SD = 3.10), t = 9.85, p < 0.001. Similarly, satisfaction with the BIB program (M = 25.47, SD = 3.34) was significantly higher than the WLC condition, t = 7.78, p < 0.001. At posttraining, the satisfaction with Child Anxiety Tales training, compared to BIB, approached significance, t = 1.80, p = 0.08. An independent-samples t-test was evaluated differences in participant satisfaction between Child Anxiety Tales and BIB at 3-month follow-up. Results indicated that participants who received Child Anxiety Tales (M = 27.71, SD = 3.41) were significantly more satisfied at follow-up than participants who received the BIB training (M = 24.47, SD = 3.79), t = 2.85, p < 0.01.
Feedback Form
Participants in the WPT group were asked to provide feedback following completion of each training module. The rate of completion for all 10 modules was predictably low given the repetitiveness of answering the same questions weekly and without study personnel oversight or additional support. Almost all, 97% (n=36, including those n=12 who elected the WPT program following waitlist), completed the online Feedback Form for Module 1, and 29% (n=11) completing the Module 10 Feedback Form. Ratings were high for ease of use and navigation, clarity, utility, pace, appeal, likelihood of remembering the content, likelihood of recommending to others as well as an open-ended section to provide recommendations or comments (See Table 2).
Discussion
Parents are often searching for ways to better understand their child’s distress, to address their needs, and to support their progress. Despite advances in parent training for externalizing problems in youth (Maughan, Christiansen, Jenson & Clark, 2005), few resources exist for parents of youth with internalizing problems. The development of an empirically supported web-based parent training program addresses an unmet need and helps parents gain access to empirically based practice.
The Child Anxiety Tales program was found to be a feasible and acceptable parent-training program for improving knowledge about anxiety and CBT for anxiety in parents of youth struggling with anxiety. Knowledge, the essential first step in empowering parents to be able to help their children manage interfering anxiety and distress, was improved following training in CBT for child anxiety. Indeed, parent knowledge about how to manage youth with anxiety improved significantly after BIB and Child Anxiety Tales, and both parent-training approaches were significantly better than WLC. Importantly, these gains were maintained at 3-month follow-up. Akin to the empirical support that was found for the Rapee book (2000; Rapee et al., 2006), the present findings support the educational benefits of both BIB and Child Anxiety Tales.
Web-based parent-training and bibliotherapy have several shared benefits. Both offer self-paced learning, 24/7 access, and affordability. In our study, both protocols were based on empirically-supported cognitive-behavioral principals for anxiety in youth. Both were equally effective in communicating evidence-based content. These similarities, along with the relatively small and non-clinical sample, may account for why the hypothesized benefits of an evidence-based and engaging web-based program over bibliotherapy could not be detected.
Client preference for learning method and different learning styles may have played a key role in both knowledge and satisfaction results. Interestingly, of the 24 participants in the WLC condition, 12 selected access to the web-based program, 9 selected book and the remaining 3 declined access to either training method. In this small sample we see that parents were fairly evenly split in their learning-method preference before trying either approach. Parents may have strong beliefs and have different learning styles – those who prefer print and those who prefer audio/visual content – that would impact their scores on knowledge tests and satisfaction ratings. Thus, making available evidence based content in both print and media for the general population given diverse learning styles and preferences may be ideal.
Parent-report of child anxiety ratings on the CBCL-A improved for all three groups over time. It may be that due to a relatively small, non-clinical sample, and only parent-report of child anxiety symptoms, differences could not be detected. The SCAS scores increased over time in all three conditions. The measure being more categorical compared to the dimensional CBCL may explain why results were not consistent in this subclinical population. A larger trial with multi-method assessment of child symptoms including child-, teacher-reports, and clinical interview, as well as an additional assessment of parent behavior change (e.g., parent-child interaction tasks) to more thoroughly measure learning, and child and family functioning is needed to evaluate the effectiveness of the training program.
A goal for Child Anxiety Tales was to make available an online parent-training program that provides parents with an accessible, confidential, convenient, and reliable resource from which to learn about child anxiety as well as learn valuable empirically-supported strategies that encourages choosing approach over avoidance and utilizing coping skills. Though further study of the program is needed to evaluate effectiveness in improving child symptoms, our results are promising. Parents of youth struggling with anxiety found the program easy to use and useful. We were pleased to hear the overwhelmingly positive responses to the open ended comments section including, “I was surprised to find it so helpful,” and “very clear and informative.” Child Anxiety Tales provides accessible, stand-alone, evidence-based, parent-training that may help many youth struggling with anxiety who may have otherwise faced barriers to access EBP.
Table 4.
WPT Feedback Form Means and Standard Deviations
| Item | Mean Score (n=36) |
|---|---|
| 1. The module was easy to navigate. | 4.68 |
| 2. The information was presented clearly. | 4.68 |
| 3. The information presented was useful. | 4.68 |
| 4. The pace of the program was good. | 4.51 |
| 5. I liked the interactivity. | 3.91 |
| 6. The module was engaging. | 4.13 |
| 7. I feel more confident in my ability to help my child after this module. | 4.21 |
| 8. I think I will remember the material covered in this module. | 4.23 |
| 9. I would recommend this program to a friend after having finished this module. | 4.39 |
| 10. I plan to continue to the next module. | 4.86 |
Note: Likert Scale: 1=Not at all; 3=Somewhat; 5=Very Much
Acknowledgments
Funding
Research on Child Anxiety Tales was supported by NIMH SBIR MH084321.
Footnotes
Parts of this article were previously presented at the Association for Cognitive and Behavioral Therapies Child Anxiety Special Interest Group Meeting, Philadelphia, November 2014.
Conflict of interest
The authors (Khanna, Kendall) receive royalties as authors of the Child Anxiety Tales program.
ORCID
Matthew M. Carper http://orcid.org/0000-0001-7125-9851
References
- Achenbach TM. Manual for the Child Behavior Checklist, Parent Report Form and 1991 Profile. Burlington: University of Vermont, Department of Psychiatry; 1991. [Google Scholar]
- Andersson G. The promise and pitfalls of the Internet for cognitive behavioural therapy. BMC Medicine. 2010;8:82. doi: 10.1186/1741-7015-8-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bogels S, Phares V. Fathers’ role in the etiology, prevention and treatment of child anxiety: A review and new model. Clinical Psychology Review. 2007 doi: 10.1016/j.cpr.2007.07.011. [DOI] [PubMed] [Google Scholar]
- Cedar B, Levant RF. A meta-analysis of the effects of parent effectiveness training. American Journal of Family Therapy. 1990;18:373–384. [Google Scholar]
- Elgar FJ, McGrath PJ. Self-administered psychosocial treatments for children and families. Journal of Clinical Psychology. 2003;59:321–339. doi: 10.1002/jclp.10132. [DOI] [PubMed] [Google Scholar]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods. 2007;39:175–191. doi: 10.3758/bf03193146. [DOI] [PubMed] [Google Scholar]
- Hollon S, Beck AT. Cognitive and cognitive-behavioral therapies. In: Lambert M, editor. Handbook of Psychotherapy and Behavior Change. New York: Wiley; 2013. pp. 393–442. [Google Scholar]
- Kazdin AE. Technology-Based Interventions and Reducing the Burdens of Mental Illness Perspectives and Comments on the Special Series. Cognitive and Behavioral Practice. 2015;22:359–366. [Google Scholar]
- Kazdin AE, Blase SL. Rebooting psychotherapy research and practice to reduce the burden of mental illness. Perspectives on Psychological Science. 2011;6:21–37. doi: 10.1177/1745691610393527. [DOI] [PubMed] [Google Scholar]
- Kenardy J, Mccafferty K, Rosa V. Internet-delivered indicated prevention for anxiety disorders: a randomized controlled trial. Behavioral and Cognitive Psychotherapy. 2003;31:279–289. [Google Scholar]
- Kendall PC, Hedtke K. Cognitive-behavioral therapy for anxious children: Therapist manual. 3rd. Ardmore, PA: Workbook Publishing; 2006. [Google Scholar]
- Kendall PC, Carper MM, Khanna MS, Harris MS. Computer technology and children’s mental health. In: Scott R, Kosslyn S, editors. Emerging Trends in the Social and Behavioral Sciences. Hoboken, NJ: John Wiley and Sons; 2014. [Google Scholar]
- Kendall PC, Hudson J, Gosch E, Flannery-Schroeder E, Suveg C. Cognitive-behavioral therapy for anxiety disordered youth: A randomized clinical trial evaluating child and family modalities. Journal of Consulting and Clinical Psychology. 2008;76:282–297. doi: 10.1037/0022-006X.76.2.282. [DOI] [PubMed] [Google Scholar]
- Kendall PC, Khanna M. Child Anxiety Tales: A web-based parent-training program. Ardmore, PA: Workbook Publishing, Inc; 2014. [Google Scholar]
- Kendall PC, Puliafico A, Barmish A, Choudhury M, Henin A, Treadwell K. Assessing anxiety with the Child Behavior Checklist and Teacher Report Form (CBCL-A and TRF-A) Journal of Anxiety Disorders. 2007;21:1004–1015. doi: 10.1016/j.janxdis.2006.10.012. [DOI] [PubMed] [Google Scholar]
- Ladany N, Lehrman-Waterman D, Molinaro M, Wolgast B. Psychotherapy supervisor ethical practices: Adherence to guidelines, the supervisory working alliance, and supervisee satisfaction. Counseling Psychologist. 1999;27(3):443–475. [Google Scholar]
- Larsen DL, Attkisson CC, Hargreaves WA, Nguyen TD. Assessment of client/patient satisfaction: Development of a general scale. Evaluation and Program Planning. 1979;4:197–207. doi: 10.1016/0149-7189(79)90094-6. [DOI] [PubMed] [Google Scholar]
- Lehrman-Waterman D, Ladany N. Development and validation of the Evaluation Process Within Supervision Inventory. Journal of Counseling Psychology. 2001;48:168–177. [Google Scholar]
- Marks IM, Cavanagh K, Gega L. Hands-on-help: Computer-aided psychotherapy. New York: Psychology Press; 2007. [Google Scholar]
- Maughan D, Christiansen E, Jenson W, Clark E. Behavioral parent training as a treatment for externalizing behavior and disruptive behavior disorders: A meta-analysis. School Psychology Review. 34:267–286. [Google Scholar]
- Nauta MH, Scholing A, Rapee RM, Abbott M, Spence SH. Development of a parent report measure of children’s anxiety: Psychometric properties and comparison with child report in a clinic and normal sample. Behaviour Research and Therapy. 2004;42:813–839. doi: 10.1016/S0005-7967(03)00200-6. [DOI] [PubMed] [Google Scholar]
- Ngyuen TD, Attkisson CC, Stegner B. Assessment of patient satisfaction: Development and refinement of a service evaluation questionnaire. Evaluation and Program Planning. 1983;6:299–314. doi: 10.1016/0149-7189(83)90010-1. [DOI] [PubMed] [Google Scholar]
- Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: A randomized controlled trial. Journal of Consulting and Clinical Psychology. 2006;74:436–444. doi: 10.1037/0022-006X.74.3.436. [DOI] [PubMed] [Google Scholar]
- Rapee RM, Spence SH, Cobham VE, Wignall A. Helping your anxious child: A step-by-step guide for parents. Oakland, CA: New Harbinger; 2000. [Google Scholar]
- Redding RE, Herbert JD, Forman EM, Gaudiano BA. Popular self-help books for anxiety, depression, and trauma: How scientifically grounded and useful are they? Professional Psychology: Research and Practice 2007 [Google Scholar]
- Scogin FR. Introduction: The status of self-administered treatments. Journal of Clinical Psychology. 2003;59(3):247–249. doi: 10.1002/jclp.10129. [DOI] [PubMed] [Google Scholar]
- Spence SH. Spence Children’s Anxiety Scale (Parent Version) Brisbane, Queensland, Australia: University of Queensland; 1999. [Google Scholar]
- Spence SH, Barrett PM, Turner CM. Psychometric properties of the Spence Children’s Anxiety Scale with young adolescents. Journal of Anxiety Disorders. 2003;17:605–625. doi: 10.1016/S0887-6185(02)00236-0. [DOI] [PubMed] [Google Scholar]
- Spence SH, Holmes JM, March S, Lipp OV. The feasibility and outcome of clinic plus internet delivery of cognitive-behavior therapy for childhood anxiety. Journal of Consulting and Clinical Psychology. 2006;74(3):614–621. doi: 10.1037/0022-006X.74.3.614. [DOI] [PubMed] [Google Scholar]
- Walkup J, Albano AM, Piacentini J, Birmaher B, Compton S, Sherrill J, Ginsburg G, Rynn M, McCracken J, Waslick B, Iyengar S, March J, Kendall PC. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. New England Journal of Medicine. 2008;359:2753–2766. doi: 10.1056/NEJMoa0804633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webster-Stratton C, Kolpacoff M, Hollinswork T. Self-administered videotape therapy for families with conduct-problem children: Comparison with two cost effective treatments and a control group. Journal of Consulting and Clinical Psychology. 1989;57:550–553. doi: 10.1037//0022-006x.56.4.558. [DOI] [PubMed] [Google Scholar]