

Abstract
Background
An inguinoscrotal hernia is defined as “giant” if descending below the midpoint of the inner thigh of a patient in upright position. In developed countries this is a rare entity. In the literature different surgical techniques have been reported so far to achieve a successful treatment.
Case presentation
We present the case of a 63 year-old man suffering from a giant inguinoscrotal hernia, whom we treated using a combined open transabdominal and inguinal approach following an unsuccessful laparoscopic attempt. Meshes were placed in a premuscular position (Lichtenstein’s procedure) and in a preperitoneal position. In addition, a reconstruction of the abdominal wall by modified components separation technique was performed. During the early postoperative period no complications were registered. Intensive care treatment was not necessary. The patient was discharged on postoperative day 8 in an excellent condition. Six months after surgery a scrotal hematocele was diagnosed and operatively removed. After a follow-up of 1.5 years neither hernia recurrence, nor chronic groin pain were recorded. The patient reported to be sexually active. His quality of life improved notably.
Additionally, a Medline and PubMed database research was performed to create an overall picture of the existing surgical treatment strategies. Included were patients with diagnosis of primary giant inguinoscrotal hernia according to the given definition. Emergency interventions and cases without details of the surgical approach were excluded.
Conclusions
Firstly, this report describes a novel, successful surgical treatment of a giant inguinoscrotal hernia without administering preoperative progressive pneumoperitoneum therapy or visceral resection. Secondly, we summarize cases previously reported as a practical guide for possible surgical therapy approaches.
Keywords: Hernia, Inguinal hernia, Hernia repair, Components separation
Background
To be classified a giant inguinoscrotal hernia, the entity described has to extend below the level of the midpoint of the patient’s inner thigh in upright position [1] or should display an anteroposterior diameter of at least 30 cm or a laterolateral diameter of about 50 cm with non-reducibility for more than 10 years [2].
The prevalence of giant inguinoscrotal hernias in developed countries is very low and often associated with mental neglect for many years. If persisting for decades, a so-called loss of domain can occur, which illustrates that reintegration of the hernia’s content into the abdominal cavity is associated with severe problems related to the prevailing lack of space. The sudden elevation of the intraabdominal pressure can gravely impair the patient’s respiratory function. Moreover, an abdominal compartment syndrome can emerge, bringing along insufficient perfusion of the viscera [3].
In order to avoid the development of an abdominal compartment syndrome, the preoperative administration of a progressive pneumoperitoneum was suggested [4]. Studies show that this preoperative treatment can be useful, as the enlargement of the abdominal capacity can facilitate bowel reintegration as well as lung adaption to the postoperative situation in cases of a loss of domain [5, 6].
To avoid the development of a dangerously elevated intraabdominal pressure, also the reduction of the hernia’s content is possible. However, bowel resection is associated with the risk of anastomotic insufficiency. Another method to achieve tension-reduced abdominal occlusion, is the enlargement of the surface of the abdominal wall. For this purpose, components separation of the abdominal wall was already described in 1990 [7]. Also, direct midline laparotomy extension using mesh graft was successfully applied to surgically treat giant inguinoscrotal hernias [8].
Case presentation
A 63 year-old Caucasian patient who suffered from a giant inguinoscrotal hernia descending to his knees presented to our clinic. The entity had become more and more severe over the preceding decade. A computed tomography revealed that two-thirds of the small bowel and part of the ascending and transverse colon were included in the enormous herniation (Fig. 1). No incarceration was registered, nor did the patient suffer from groin pain or digestion irregularities. His waist circumference was 108.5 cm. No additional health problems other than arterial hypertension were registered. His laboratory parameters at presentation were normal (Hemoglobin: 0.009 mmol/L (normal range: 0.008-0.011 mmol/L); Leucocyte count: 7.5 × 109/L (normal range: 3.5–10 × 109/L), C-reactive protein: 19.05 nmol/L (normal range: <47,62 nmol/L)). An operation was suggested, since the giant inguinoscrotal hernia impaired his quality of life. The patient was married and was employed as freight worker when developing his medical condition. The entity notably limited his sexual activity. After a detailed explanation of possible risks including bowel resection and orchiectomy, the patient signed an informed consent for operative treatment. Although the possibility of preoperative administration of progressive pneumoperitoneum therapy was discussed, the patient refused this approach.
Fig. 1.
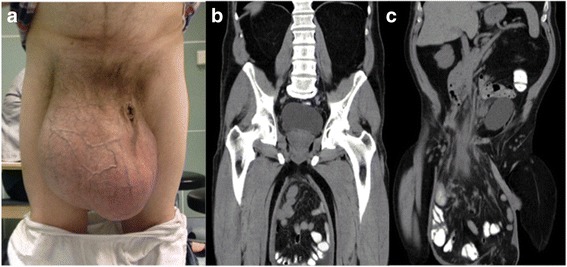
Frontal view of the giant inguinoscrotal hernia descending to the level of the knees (a). Computed tomography of the entity displaying subtotal evisceration of small bowel and ascending and transverse colon with intact vascularization (b/c)
A laparoscopic reduction of the hernia content was unsuccessful. Therefore, an open transabdominal approach by midline laparotomy was chosen. The small intestine was replaced, but the right hemicolon remained fixed in the hernial sac. An additional right-sided inguinal incision to isolate the peritoneal sac was performed. By omental resection, we sufficiently gained space to mobilize the protruded colon back into the abdominal cavity. Complete resection of the hernial sac required the removal of the vascularization of the right testicle. Therefore, ipsilateral orchiectomy was performed. Subsequently, we used Lichtenstein’s technique in order to reinforce the abdominal occlusion using an UltraPro Mesh (10 × 15 cm, Ethicon, Johnson and Johnson, Norderstedt, Germany).
Via the midline laparotomy, we additionally placed a ProGrip Mesh (10 × 15 cm, Covidien, Dublin, Ireland) into a preperitoneal position, to thoroughly cover the instable area. Since the former content of the herniation was too voluminous to allow direct tension-free suturing of the lower part of the laparotomy wound, we subsequently performed modified components separation completed by mesh insertion. Therefore a subcutaneous tissue flap was released to the sides until anterior axillar line, followed by separation of the external oblique muscle from the internal oblique muscle and relaxing incisions of the internal oblique/transversus abdominis muscle. Bilateral access to the rectus sheath allowed the preparation of a retromuscular plane. After suturing of the posterior lamina (Vicryl), the reconstruction was completed by retromuscular mesh insertion (UltraPro Mesh 30 × 15 cm, Ethicon, Johnson and Johnson Norderstedt, Germany). The created overlap of the meshes (retromuscular and preperitoneal mesh) was 3 cm in the distal part. Suction drainages were placed subcutaneous plane. During the early postoperative period no complications occurred. Intensive care treatment was not necessary. No impairment of respiration or oxygenation was registered. We discharged the patient on postoperative day 8 in an excellent condition.
Six months after the operation, a hematocele in localization of the former right testicle was diagnosed. The operative removal of the hematoma and adjacent tissue was performed. After having removed the hematoma, the patient was fully satisfied with the overall postoperative result. Plastic surgery, in order to reduce the size of the scrotal skin surface, was not performed at any time. We successfully relied on the skin’s capacity to retract after removing the continuous tension caused by the giant hernia.
In a follow-up visit, 18 months after hernioplasty, no impairment of digestion was reported. Clinically and sonographically no hernia recurrence was registered. An acceptable cosmetic result prevailed (Fig. 2). Furthermore, the patient reported to be sexually active again. His quality of life had improved notably after the restoration of the giant inguinoscrotal hernia.
Fig. 2.

Clinical result following surgical treatment of giant inguinoscrotal hernia at 1.5 year postoperative follow-up
Discussion and conclusion
Giant inguinoscrotal hernias represent a rare entity in developed countries. Different approaches are possible. Open abdominal and inguinal approaches are commonly used, if necessary in combination. According to the outer circumstances, ranging from high-end surgery in developed countries to surgery with limited resources in less developed countries, the surgical therapy has to be adapted to achieve the optimal result for the individual patient.
It is necessary to treat inguinoscrotal hernias, since organ perforation can occur, potentially causing peritonitis and sepsis [9, 10]. It is proved that early elective operations are associated with less fatal complications than emergency interventions [11]. Early elective surgical treatment helps to avoid visceral resection, which may bring along the risk of anastomotic leakage and potential prosthetic infection [12, 13].
In order to avoid the development of an abdominal compartment syndrome, resulting from a sudden elevation of the intraabdominal pressure following organ reposition, the preoperative administration of progressive pneumoperitoneum therapy was suggested [4]. Intraperitoneal gas insufflation can be performed continuously or fractionally. Atmospheric air should be preferred to O2 or CO2, since these gasses are absorbed rapidly [5]. Furthermore, one should consider that the application of this method requires a prolonged stay in hospital [14]. The insufflated gas can also spread into the hernial sac and, instead of widening the abdominal space, provoke an enlargement of the hernia itself [8]. After comprehensively informing our patient about this procedure and the associated risks, he refused this approach.
Another method to achieve tension-reduced abdominal occlusion is the enlargement of the abdominal space. This can be achieved by components separation of the abdominal wall, as reported by Ramirez et al. in 1990 [7]. For this technique, the rectus muscle is released from the posterior rectus sheath by separation of the external oblique muscle from the internal oblique muscle in an avascular plane, avoiding the need of mesh insertion. For reconstruction of the abdominal wall, in cases of giant inguinoscrotal hernias, also the direct extension of a midline laparotomy defect using mesh insertion was reported [8]. In the present case, we partly combined these techniques and additionally inserted a premuscular mesh in Lichtenstein’s position.
To avoid the development of a dangerously elevated intraabdominal pressure, reduction of the hernia’s content is another possible solution, e.g. by bowel resection. This, however, is associated with the risk of insufficiency of the anastomosis created, possibly leading to peritonitis, sepsis and even death. Anastomotic insufficiency can also cause infection of the mesh grafts inserted, potentially endangering the reconstruction of the abdominal cavity. In the case we presented, omental resection was performed, whereas bowel resection was avoided.
A laparoscopic approach, via transabdominal preperitoneal hernia repair (TAPP) or totally extraperitoneal (TEP) inguinal hernia repair, can be attempted to make use of the advantages of minimally invasive surgery [15]. If a laparoscopic approach is aimed for, it is recommendable to reduce the volume of the herniated organs prior to the operation, to facilitate the reposition manoeuvre. The application of Macrogol, (polyethylene glycol)-based laxatives, has been reported to be helpful in this regard, as it promotes the emptying of the intestine to be replaced [16].
Often, orchiectomy becomes necessary when removing the hernial sac because of adhesions, which are frequently observed in patients with a longer history of a giant inguinoscrotal hernia. Another reason for orchiectomy is the possible development of orchitis after an extended dissection of the spermatic cord. Additionally, orchiectomy was reported to facilitate an adequate closure of the hernial defect [14].
A follow-up analysis of cases of surgically treated giant inguinoscrotal hernias (from 1 to 96 months postoperatively) did not show recurrence, even though different approaches were performed (Table 1). The most infrequent approach is the singularly laparoscopic one (TAPP), reported by Momiyama et al. in 2016, who applied Stoppa’s method of placing a mesh in a pre-peritoneal position.
Table 1.
Comparison of different surgical approaches to giant inguinoscrotal hernias
| Bowel preparation | Pneumoperitoneum | Laparoscopic approach | Open abdominal approach | (Extended) inguinal approach | Omentectomy | Bowel resection | Orchiectomy | Scrotum resection | Components separation | Mesh in premuscular position | Mesh in preperitoneal postition | Mesh between internal and external oblique | Appendectomy | Postoperative intensive care | Postoperative discharge day | Hematocele/seroma development | Recurrence | Last follow-up (postoperative month) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| – | – | + | + | + | + | – | + | – | + | + | + | + | – | – | 8 | + | – | 18 | Present Case Report |
| – | + | – | – | + | – | – | – | – | – | + | – | – | – | n/a | n/a | – | n/a | n/a | Baca-Prieto et al. 2017 [19] |
| – | – | – | – | + | 7× | – | 1 | – | – | + | – | – | 2× | n/a | 6.3* | 10× | – | 48 | Bierca et al. 2013 [20] (15 cases) |
| + | – | – | + | + | – | + | + | + | – | – | + | – | – | + | 9 | – | – | 18–96 | Cavalli et al. 2015 [2] |
| + | – | – | + | + | – | + | + | + | – | – | + | – | – | + | 8 | – | – | Cavalli et al. 2015 [2] | |
| + | – | – | – | + | – | – | + | + | – | – | + | – | – | + | 7 | – | – | Cavalli et al. 2015 [2] | |
| + | – | – | – | + | – | – | + | + | – | – | + | – | – | + | 6 | – | – | Cavalli et al. 2015 [2] (2 cases) | |
| – | – | – | – | + | + | – | – | – | – | + | – | – | – | – | 4 | + | – | 3 | Dinesh et al. 2014 [21] |
| + | – | – | + | + | – | + | + | – | – | – | – | – | – | – | 28 | – | – | 8 | Fadiran et al. 1992 [22] |
| – | – | – | – | + | – | – | – | – | – | + | – | – | – | n/a | n/a | – | – | 12 | Gillellamudi et al. 2010 [23] |
| – | – | – | + | – | – | – | – | – | – | – | + | – | – | – | 5 | – | n/a | n/a | Goonetilleke et al. 2010 [24] |
| + | – | – | + | – | – | – | – | – | + | – | – | + | – | – | 13 | + | – | 2 | Hamad et al. 2013 [25] |
| – | – | – | – | + | + | – | + | + | – | + | – | – | – | – | n/a | – | – | 36 | Karthikeyan et al. 2014 [26] |
| – | + | – | – | + | – | – | + | – | – | – | + | – | – | + | 7 | – | – | 36 | Kovachev et al. 2010 [14] |
| – | – | – | + | + | – | – | + | – | – | – | + | – | – | – | 7 | – | – | 24 | Kovachev et al. 2010 [14] |
| – | – | – | – | + | + | + | – | + | – | + | – | – | – | + | 8 | – | n/a | n/a | Kumar et al. 2016 [27] |
| – | – | – | – | + | + | – | – | – | – | – | – | – | – | + | 6 | – | – | n/a | Mohamad et al. 2017 [28] |
| + | – | + | – | – | – | – | – | – | – | – | + | – | – | – | 12 | – | – | 12 | Momiyama et al. 2016 [16] |
| – | – | – | + | + | + | + | – | – | – | – | + | – | – | + | n/a | – | – | 6 | Monestiroli et al. 2007 [12] |
| – | – | – | + | + | + | + | + | + | – | – | + | – | – | + | n/a | – | – | 12 | Patsas et al. 2010 [29] |
| – | + | – | + | – | – | – | – | – | – | – | + | – | + | – | 14 | – | – | 11 | Piskin et al. 2010 [30] |
| – | + | – | – | + | – | – | – | – | – | – | + | – | + | – | 13 | – | – | 9 | Piskin et al. 2010 [30] |
| – | – | – | + | + | – | – | + | – | – | + | – | – | – | + | 10 | – | – | 6 | Sahsamanis et al. 2016 [31] |
| – | – | – | – | + | – | – | – | – | – | – | – | – | – | – | 1 | 1× | – | 1 | Savoie et al. 2014 [18] {25 cases} |
| – | – | – | + | + | + | – | + | – | – | + | – | – | – | n/a | n/a | – | – | 1 | Singh et al. 2015 [32] |
| + | – | – | – | + | – | – | + | 2× | – | – | 4× | – | – | – | 3 | – | – | 12 | Sturniolo et al. 1999 [33] (5 cases) |
| – | – | – | – | + | + | – | – | – | – | + | – | – | – | – | 7 | + | – | 48 | Trakarnsagna et al. 2014 [34] |
| – | – | – | – | + | – | – | – | + | – | + | – | – | + | + | 6 | – | – | 3 | Turner et al. 2010 [35] |
| – | – | – | – | + | + | – | – | – | – | + | – | – | – | + | 6 | – | – | 6 | Tarchouli et al. 2015 [36] |
n/a = not assessed, * = “on average” in cited source
In the literature, reduction of the scrotal skin is described as helpful to achieve a cosmetically acceptable result [2]. We successfully relied on the skin’s ability to recover after the removal of continuous tension caused by the giant hernia. Scrotal skin was not resected at any time. On the other hand, it was described as useful to preserve the redundant scrotal skin, in order to keep a safety net, which can allow the temporary replacement of hernial contents back into the scrotum. This may be necessary in the early postoperative period, after a failed hernia repair, or in case of respiratory compromise [17]. However, scrotal skin reduction seems to be protective with regard to the postoperative development of hematocele/seroma (Table 1). According to Savoie et al., who contributed a case series to the current literature, in which 25 men from the Ivory Coast underwent Bassini’s hernia repair, the abandonment of the distal hernial sac in the scrotum can be proposed to selected patients, in order to prevent bleeding and cutaneous complications [18].
In the present case, we successfully used a novel combination of the existing techniques avoiding bowel resection and preoperative progressive pneumoperitoneum.
Acknowledgements
There is nothing to be acknowledged.
Funding
For this study no funding exists.
Availability of data and materials
The data supporting our thesis is completely available in this article. Articles referred to can be found in the reference list.
Abbreviations
- TAPP
Transabdominal preperitoneal hernia repair
- TEP
Totally extraperitoneal hernia repair
Authors’ contributions
JIS and DWK analyzed the existing data concerning the treatment of the patient regarded, wrote the manuscript and designed the tables by analyzing the existing literature on the issue. PG treated the patient regarded, read and approved the manuscript. HL and DWK critically revised the manuscript. All authors read and approved the final version of the manuscript.
Authors’ information
Not applicable.
Ethics approval and consent to participate
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
This case report study was carried out respecting the Declaration of Helsinki in its current version. Ethical approval: not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Julia Isabelle Staubitz, Email: julia.staubitz@unimedizin-mainz.de.
Peter Gassmann, Email: peter.gassmann@unimedizin-mainz.de.
Daniel Wilhelm Kauff, Phone: 00496131/17 7291, Email: daniel.kauff@unimedizin-mainz.de.
Hauke Lang, Email: hauke.lang@unimedizin-mainz.de.
References
- 1.Hodgkinson DJ, McIlrath DC. Scrotal reconstruction for giant inguinal hernias. Surg Clin N Am. 1984;64:301–313. doi: 10.1016/S0039-6109(16)43287-1. [DOI] [PubMed] [Google Scholar]
- 2.Cavalli M, Biondi A, Bruni PG, Campanelle G. Giant inguinal hernia: the challenging hug technique. Hernia. 2015;19:775–783. doi: 10.1007/s10029-014-1324-7. [DOI] [PubMed] [Google Scholar]
- 3.Lardiére-Deguelte S, Appéré F, Goi AV, Marcus C, Flament JB, Delattre JF, Palot JP. Efficacité du pneumopéritoine progressif préoperatoire dans le traitment des grandes éventrations: evaluation volumetrique par tomodensitometrie. e – memoires de l’Académie Nationale de Chirurgie. 1984;9:103–106. [Google Scholar]
- 4.Moreno IG. Chronic eventrations and large hernias; preoperative treatment by progressive pneumoperitoneum; original procedure. Surgery. 1947;22:945–953. [PubMed] [Google Scholar]
- 5.Oprea V, Matei O, Gheorghescu D, Leuca D, Buia F, Rosianu M, Dinca M. Progressive preoperative pneumoperitoneum (PPP) as an adjunct for surgery of hernias with loss of domain. Chirurgia (Bucur) 2014;109:664–669. [PubMed] [Google Scholar]
- 6.Sabbagh C, Dumont F, Fuks D, Yzet T, Verhaeghe P, Regimbeau JM. Progressive preoperative pneumoperitoneum preparation (the Goni Moreno protocol) prior to large incisional hernia surgery: volumetric, respiratory and clinical impacts. A prospective study. Hernia. 2012;16:33–40. doi: 10.1007/s10029-011-0849-2. [DOI] [PubMed] [Google Scholar]
- 7.Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990;86:519–526. doi: 10.1097/00006534-199009000-00023. [DOI] [PubMed] [Google Scholar]
- 8.Merrett ND, Waterworth MW, Green MF. Repair of giant inguinoscrotal inguinal hernia using marlex mesh and scrotal skin flaps. Aust N Z J Surg. 1994;64:380–383. doi: 10.1111/j.1445-2197.1994.tb02231.x. [DOI] [PubMed] [Google Scholar]
- 9.Lajevardi SS, Gundara JS, Collins SA, Samra JS. Acute gastric rupture in a giant inguinoscrotal hernia. J Gastrointest Surg. 2015;19:2283–2285. doi: 10.1007/s11605-015-2916-y. [DOI] [PubMed] [Google Scholar]
- 10.Gaedecke J, Schuler J. Brinker, Quintel M, Ghadimi M. Emergency repair of giant inguinoscrotal hernia in a septic patient. J Gastrointest Surg. 2013;17:837–839. doi: 10.1007/s11605-012-2136-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Primatesta P, Goldacre MJ. Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol. 1996;25:835–8359. doi: 10.1093/ije/25.4.835. [DOI] [PubMed] [Google Scholar]
- 12.Monestiroli UM, Bondurri A, Gandini F, Lenna G, Vellini S, Danelli P. Giant inguinoscrotal hernia. Tech Coloproctol. 2007;11:283–285. doi: 10.1007/s10151-007-0368-4. [DOI] [PubMed] [Google Scholar]
- 13.Weiss CL, Brauckhoff M, Steuber J. Emergency management of a monstrous inguinal hernia. Zentralbl Chir. 1997;122:931–933. [PubMed] [Google Scholar]
- 14.Kovachev LS, Paul AP, Chowdhary P, Choudhary P, Filipov ET. Regarding extremely large inguinal hernias with a contribution of two cases. Hernia. 2010;14:193–197. doi: 10.1007/s10029-009-0517-y. [DOI] [PubMed] [Google Scholar]
- 15.Kulacoglu H. Current options in inguinal hernia repair in adult patients. Hippokratia. 2011;15:223–231. [PMC free article] [PubMed] [Google Scholar]
- 16.Momiyama M, Mizutani F, Yamamoto T, Aoyama Y, Hasegawa H, Yamamoto H. Treatment of a giant inguinal hernia using transabdominal pre-peritoneal repair. J Surg Case Rep. 2016;9:1–3. doi: 10.1093/jscr/rjw159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mehendale FV, Taams KO, Kingsworth AN. Repair of a giant inguinoscrotal hernia. Br J Plast Surg. 2000;53:525–529. doi: 10.1054/bjps.2000.3383. [DOI] [PubMed] [Google Scholar]
- 18.Savoie PH, Abdalla S, Bordes J, Laroche J, Fournier R, Pons F, Bonnet S. Surgical repair of giant inguinoscrotal hernias in an austere environment: leaving the distal sac limits early complications. Hernia. 2014;18:113–118. doi: 10.1007/s10029-013-1049-z. [DOI] [PubMed] [Google Scholar]
- 19.Baca-Prieto JE, Dominquez-Carrillo LG. Hernia Gigante inguino-escrotal. Revista de gastroenterologia de México. 2017;82:89–91. doi: 10.1016/j.rgmx.2016.06.003. [DOI] [PubMed] [Google Scholar]
- 20.Bierca J, Kosim A, Kołodziejczak M, Zmora J, Kultys E. Effectiveness of Lichtenstein repairs in planned treatment of giant inguinal hernia - own experience. Wideochir Inne Tech Maloinwazyjne. 2013;8:36–42. doi: 10.5114/wiitm.2011.30971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dinesh HN, Jagadish Kumar CD, Shreyas N. Giant inguinoscrotal hernia repaired by Lichtensteins technique without loss of domain - a case report. J Clin Diagn Res. 2014;8:ND07–ND08. doi: 10.7860/JCDR/2014/9662.4882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Fadiran OA, Lawal OO, Jeje J, Bankole O, Oyero T. Giant inguino scrotal hernia: a case report. Cent Afr J Med. 1992;38:127–130. [PubMed] [Google Scholar]
- 23.Gillellamudi SB. Hanging giant inguinoscrotal hernia. NJIRM. 2010;1:47–48. [Google Scholar]
- 24.Goonetilleke K, McIlroy B. Giant inguinoscrotal hernia presenting with acute renal failure: a case report and review of literature. Ann R Coll Surg Engl. 2010;92:W21–W23. doi: 10.1308/147870810X12659688852158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hamad A, Marimuthu K, Mothe B, Hanafy M. Repair of massive inguinal hernia with loss of abdominal domain using laparoscopic component separation technique. J Surg Case Rep. 2013;3:rjt008. doi: 10.1093/jscr/rjt008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Karthikeyan VS, Sistla SC, Ram D, Ali SM, Rajkumar N. Giant inguinoscrotal hernia- report of a rare case with literature review. Int Surg. 2014;99:560–564. doi: 10.9738/INTSURG-D-13-00083.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kumar A, Choudhary PR, Gandhi A, Jalthania M, Gothwal S. Giant inguinal hernia- a great escape from second abdomen: a report of a case and review of different surgical techniques. SAS J Surg. 2016;2:26–30. [Google Scholar]
- 28.Mohamad IS, Chuan CY, Balasubbiah N, Zakaria Z, Hassan S. Giant Inguinoscrotal hernia: the challenging surgical repair and postoperative management. Int J Dual Diagn. 2017;2:18–21. [Google Scholar]
- 29.Patsas A, Tsiaousis P, Papaziogas B, Koutelidakis I, Goula C, Atmatzidis K. Repair of a giant inguinoscrotal hernia. Hernia. 2010;14:305–307. doi: 10.1007/s10029-009-0533-y. [DOI] [PubMed] [Google Scholar]
- 30.Piskin T, Aydin C, Barut B, Dirican A, Kayaalp C. Preoperative progressive pneumoperitoneum for giant inguinal hernias. Ann Saudi Med. 2010;30:317–320. doi: 10.4103/0256-4947.65268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sahsamanis G, Samaras S, Dimitrakopoulos G. Treatment of a half century year old giant inguinoscrotal hernia. A case report. Int J Surg Case Rep. 2016;25:51–54. doi: 10.1016/j.ijscr.2016.05.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Singh G, Jadhav DS, Nongmaithem M, Ali I. Giant inguinal hernia. A challenge to surgeons. J Dent Med Sci. 2015;14:24–27. [Google Scholar]
- 33.Sturniolo G, Tonante A, Gagliano E, Taranto F, Lo Schiavo MG, D'Alia C. Surgical treatment of the giant inguinal hernia. Hernia. 1999;3:27–30. doi: 10.1007/BF01576738. [DOI] [Google Scholar]
- 34.Trakarnsagna A, Chinswangwatanakul V, Methasate A, Swangsri J, Phalanusitthepha C, Parakonthun T, Taweerutchana V, Akaraviputh T. Giant inguinal hernia: report of a case and reviews of surgical techniques. Int J Surg Case Rep. 2014;5:868–872. doi: 10.1016/j.ijscr.2014.10.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Turner EJ, Malhas A, Christi I, Oke T. Management of a giant inguinoscrotal hernia with an ulcerated base in a patient with cardiac disease. J Surg Case Rep. 2010;8:9. doi: 10.1093/jscr/2010.8.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Tarchouli M, Ratbi MB, Bouzroud M, Ait-Ali A, Bounaim A, Sair K. Giant inguinoscrotal hernia containing intestinal segments and urinary bladder successfully repaired by simple hernioplasty technique: a case report. J Med Case Reports. 2015;9:276. doi: 10.1186/s13256-015-0759-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data supporting our thesis is completely available in this article. Articles referred to can be found in the reference list.