

Abstract
Hexagon TB is intended for the rapid diagnostics of tuberculosis. Tuberculosis is a contagious and epidemic disease. According to the data published by WHO, 3-4 millions of patients are diagnosed with this disease annually. In 2004, 107 new cases were discovered in the area of Tuzla Municipality. Annual incidence of this disease is 62,9 per 100 000 inhabitants in Bosnia and Herzegovina; 28,9 in Slovenia; 33,2 in FYRM; 48,5 in Croatia; 41,8 in Serbia and Montenegro. Western European countries have rather low rate of the disease - 5-10 cases per 100 000 inhabitants. Efficiency of Hexagon TB examination method was tested on 100 patients. The subjects were patients with clinical symptoms of active TBC infection, persons who were in contact with TBC patients and persons earlier cured of TBC. All the subjects were tested with Hexagon TB, and the results were compared against lungs X-rays and sputum test for BK and LÖW. Hexagon TB is intended for rapid, qualitative detection of IgG, IgA, IgM antibodies against M. tuberculosis and mycobacterium in human serum, plasma or whole blood as an aid in the early diagnostics of tuberculosis infections for professional use. Hexagon TB was positive in 11 of the examined patients. 10 patients had changes suggesting TBC. 1 patient was directly positive for BK and 3 patients were positive for LÖW. Of all the examined patients, 3 were positive for all tests positive.
According to our results, Hexagon TB has significant importance in practice of rapid TBC diagnostics compared to lungs X-ray and examination of sputum for BK and LÖW
Keywords: Hexagon TB, Tuberculosis, Rapid diagnosis
INTRODUCTION
Tuberculosis is contagious granulomatosis disease caused by bacillus Mycobacterium tuberculosis. Although efficient anti-tuberculosis therapy has been available for several years, the disease is quite frequent. According to WHO data from 1998, tuberculosis represents a major health issue. Following the infection with bacillus of tuberculosis, patient may either develop the illness immediately (primary tuberculosis), or overcome the primary infection and become latent infection carrier or the illness may develop later (post primary tuberculosis) (1). Patophysiologic changes include monocytosys with intensified release of monocytes from the marrow. Monocytes are drawn towards the place of infiamma-tion where they are transformed into macrophages. Macrophages play the key role at the beginning of immune response. They phagocyte antigens and make them identified T-lymphocytes (2). Patients with serious form of illness exhibit hypergammaglobulinaemia, with primary increase in the concentration of antibodies IgM, and IgG, which remain elevated for longer period of time. IgA-antibodies collate as illness progresses (3). Diagnosis of tuberculosis is based on anamnesis, tuberculosis test, physical examination, X-ray, bacteriological and biochemical examinations. Bacteriological examinations of sputum, bronchial cough out, urine, feces, gastrolavate and other biological materials are the most relevant examination in tuberculosis diagnostics. Positive analysis for Mycobacterium tuberculosis is certain proof of illness (4). Basic limitation of the procedure is the required time, which hampers early diagnosis and timely beginning of therapy. Hexagon chromatographic immunoanalysis is particularly intended for fast, qualitative identification of IgG, IgA and IgM-antibodies of Mycobacterium tuberculosis and other mycobacteria in human serum, plasma or blood. Test is suitable for diagnosing the tuberculosis even in childhood when it is difficult to obtain caught out for illness carrier (5). The aim of this study was appraisal of Hexagon TB fast diagnosis of tuberculosis against X-ray lung examination and sputum examination for BK and LOW.
PATIENT AND METHODS
The research included 100 patients of both genders (43 male and 57 female), whose age varied between 30 and 60 years (average 41 ± 12 years). All the patients had clinical symptoms of TBC infection; they were in contact with actively infected TBC patients or with patients who were previously treated for TBC. The research lasted for 5 months (from November to March). PA snapshots of the patients’ lungs were taken in Polyclinic for lung diseases and TBC in Public Health Care in Tuzla. Their sputum was tested for the presence of acid resistant bacillus (ARB) in Microbiological Laboratory-University Clinics Centre Tuzla, along with direct BK analysis and homogenization, the same were cultivated on LOW stock. All the patients were treated with Hexagon TB in Microbiological Laboratory, at the Department for Immunology in University Clinics Centre Tuzla. The samples of sputum were taken during the period of one week; the blood sample for Hexagon TB was taken on the day the X-ray of lungs was done or the day after. With a finished enzyme immunologic test we determined the amount of antibodies class IgG (antibodies for antigen A-60) according to the micro bacterial complex of TBC in a patient’s blood (6). Hexagon TB was produced in HUMAN GMBH, from Wiesbaden in Germany. Before Hexagon TB test it is mandatory to balance the temperature of the sample with the temperature of the environment, and then label it separately for each patient. PIP has to be vertical. Place two drops of blood, than add three drops of DIL. Results are obtained after 15 minutes. Appearance of red and violet line in the upper part of the window indicates correct application of the test, and another red and violet line in the lower part of the window designates positive test result, ie. presence of TB antibodies in the specimen. Serum specimens or plasma may be stored at the temperature 2-8°C for up to 72 hours. For longer storage, specimens should be frozen at -20°C in vacuum tube. Each of the specimens should be treated as potentially infectious so caution is recommended (7).
RESULTS
Of all the examined patients 11 had positive Hexagon TB and 10 had changes in X-ray PA pulmo what is considered as a coincidence. Patients who had changes in X-ray PA pulmo were not all tested positive and vice versa. All the results were positive in three patients (Figure 1, 2). In 6 X-ray snapshots we found old specific changes that were confirmed by comparing with earlier snapshots from our film archive. In 1 X-ray snapshot we identified bronchopneumonia caused by E. coli. In 3 X-ray snapshots the identified changes suggested probable active specific changes that were subsequently proved.
FIGURE 1.
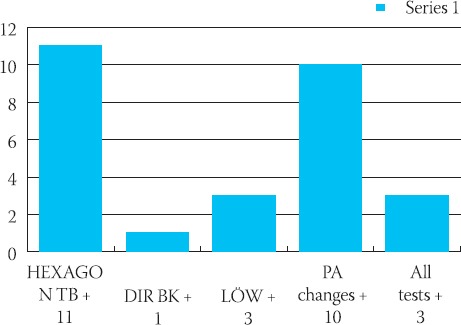
The results of Hexagon TB test in all patients
FIGURE 2.
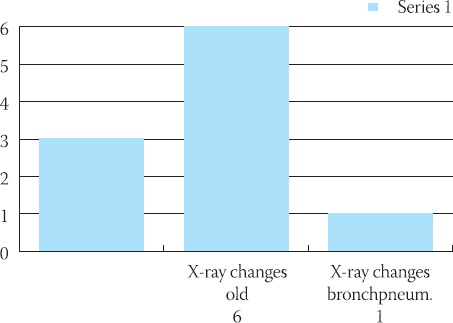
Compared X-ray changes on pulmonal parenchyme.
DISCUSSION
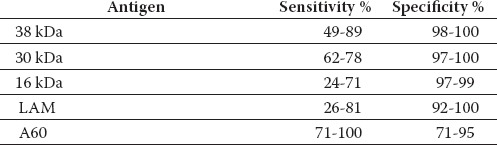
It is considered that one third of population is infected with Mycobacterium tuberculosis, and in 1995, 9 million of new tuberculosis patients were registered along approximately 3 million of deaths (8). Tuberculosis is an epidemic disease. It spreads, reaches the culmination and than gradually retreats in each affected population. Epidemic of tuberculosis in ex-Yugoslavia started in the first half of previous century, around 150 years later than in western European countries. Ever since, the spreading of infection and dying from TBC slowly decreased but war in 1992 provoked repeated increase of illness. During the period 2000-2004 approximately 125 newly tuberculosis infected people were registered in the area of Tuzla Municipality, which is extremely high number (9). Early diagnosis and timely treatment are necessary for the prevention of infection spreading (10). For the reasons above numerous commercial tests for antibodies that confirm TBC infection were developed. Sensitivity of these tests spans from 26 % to 100%, while the specificity is higher, from 71 % to 100 % (Table 1) (11). Antigen A60 is used in Hexagon TB and its sensitivity coincide with the results of our study (Table 2) (12). Hexagon TB is currently not used enough in our area.
TABLE 1.
Sensitivity and specificity of ELISA serologic Kits (using IgG antibodies)
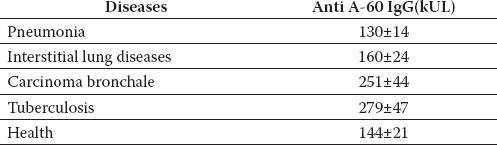
TABLE 2.
Values of antibodies IgG against antigen A60 in different lung diseases
CONCLUSION
In the frame of our study it is demonstrated that Hexagon TB has a significant role in tuberculosis diagnostics and is practical for use both in the field and in the centers. Hexagon TB is especially significant in cases where specific microbiological examination that confirms the cause is not possible or when it is difficult to obtain caught out or other biological materials for the identification of the disease carrier. It would be great contribution to early identification as well as timely treatment, which may stop progress of this contagious disease, in epidemiological sense, which still takes human lives like it used to centuries before.
LIST OF ABBREVIATIONS
WHO - World Health Organization
TBC – Tuberculosis
PA - Postero-anterior
FYRM - Former Yugoslav Republic of Macedonia
BK - Bacil Koh
Ig - Immunoglobulin
REFERENCES
- 1.Nurkić M. Mikobakterije. Tuzla: Klinički značaj i metode; 2000. [Google Scholar]
- 2.Dodig S, Čepelak I. Medicinsko-biokemiske pretrage u pul-mologiji. Zagreb: Školska knjiga; 1997. [Google Scholar]
- 3.Popovac D. Bolesti pluća. V dopunjeno izdanje Beograd. 1999 [Google Scholar]
- 4.Dizdarević Z. Nacionalni program za tuberkulozu Bosne i Hercegovine, Ministarstvo zdravlja Federacije Bosne i Hercegovine, Print M. Sarajevo. 1998:15–21. [Google Scholar]
- 5.Terr A.I. Multiple chemical sensitivities. J. Allergy Clin. Immunol. 1994;94(2):362–366. [PubMed] [Google Scholar]
- 6.Pongrac I. Bolesti pleure. Medicinsaka naklada. 1994:175. [Google Scholar]
- 7.Delacourt C, Gobin J, Gaillard J.L, de Blic J, Veron M, Schinm-mann P. Value of ELISA using Antigen-60 for the diagnosis of tuberculosis in children. Chest. 1993;104(2):393–398. doi: 10.1378/chest.104.2.393. [DOI] [PubMed] [Google Scholar]
- 8.Rotenberg S.S, Wagner J.S, Chang J.H, Fan L.L. The safety and efficacy of thoracoscopic lung biopsy for diagnosis and treatment in infant and children. J Pediatr Sugr. 1996;31(1):100–103. doi: 10.1016/s0022-3468(96)90328-0. [DOI] [PubMed] [Google Scholar]
- 9.Katola L, Brander E, Backman A. Neonatal BCG vaccination and mycobacterial cervical adenitis in childhood. Tbercle. 1987;68:291–296. doi: 10.1016/0041-3879(87)90070-5. [DOI] [PubMed] [Google Scholar]
- 10.Condos R, et al. Peripheral blood-based PCR assay to identify patients with active pulmonary tuberculosis. Lancet. 1996;347:1082–1085. doi: 10.1016/s0140-6736(96)90281-0. [DOI] [PubMed] [Google Scholar]
- 11.Mohadevan S. Serodyagnosis of tuberculosis in children. J Indian Med. Assoc. 2002;100/(2):107–112. [PubMed] [Google Scholar]
- 12.Riedel W. Nützt das Anti A-60-IgG in der Differentialdiagnose zwischen Tbc und malignen bzw. entzündlichen Lungenk-rankungen? Atemw.-Lungenkrkh. 1989;11(6):671–674. [Google Scholar]