

Abstract
Background:
Many studies have reported the association of estrogen receptor α gene (ESRα) ESRα PvuII T>C, XbaI A>G and BtgI G>A polymorphisms with Knee osteoarthritis (KOA) risk, but the results remained controversial. In order to drive a more precise estimation, the present systematic review and meta-analysis was performed to investigate the association between ESRα polymorphisms and KOA susceptibility.
Methods:
Eligible articles were identified by search of databases including PubMed, ISI Web of Knowledge and Google scholar up to March 1, 2017. Data were extracted by two independent authors and pooled odds ratio (OR) with 95% confidence interval (CI) was calculated.
Results:
A total of 22 case-control studies in eleven publications with 6,575 KOA cases and 7,459 controls were included in the meta-analysis. By pooling all the studies, either ESRα PvuII T>C and XbaI A>G polymorphisms was not associated with KOA risk in the overall population. However, ESRα BtgI G>A was significantly associated with KOA risk under all five genetic models. In the subgroup analysis by ethnicity, a significant association was observed between ESRα PvuII T>C polymorphism and KOA risk in Asians under heterozygote model. In addition, significant association was found between ESRα XbaI A>G polymorphism and KOA in Caucasians under allelic, homozygote, dominant and recessive models.
Conclusion:
The present meta-analysis suggests that ESRα BtgI G>A rather than ESRα PvuII T>C and XbaI A>G polymorphisms is associated with an increased KOA risk in overall population. Moreover, we have found that ESRα PvuII T>C and XbaI A>G polymorphisms associated with KOA susceptibility by ethnicity backgrounds.
Keywords: estrogen receptor gene, Knee, Osteoarthritis, polymorphism
Introduction
Osteoarthritis (OA) is a degenerative joint condition that affects roughly 80% of the population over 65 years of age (1). As of 2004, OA was the cause for moderate to severe disability in as many as 43.4 million people worldwide (2). The financial burden associated with posttraumatic OA was projected at $3.06 billion annually in 2006 (3). Knee Osteoarthritis (KOA) is the most prevalent type of arthritis. KOA is expected to be the fourth leading cause of disability in 2020 (4, 5). The KOA-related symptoms have a major impact on subject’s social and physical wellbeing (5). KOA normally occurs as a result of aging; however, genetics, muscle weakness around joints, malpositioning, obesity, and altered mechanical loading conditions such as repeated motions and trauma can all increase the risk of OA development (4, 6).
Rapid progress has been made in recent years to identify the locus that affect KOA risk, such as vitamin D receptor (VDR) gene, insulin-like growth factor I (IGF-I) gene, collagen type I alpha 1(COL1A1) gene and estrogen receptor α (ESRα) gene, etc. (6). Previous studies have suggested that ER-α plays an important role in the pathological process of KOA (7). Human ESRα, a member of the nuclear receptor superfamily of ligand-activated transcription factors, is one of the key mediators of hormonal response in estrogen-sensitive tissues (8, 9). The estrogen- ESRα complex is primarily responsible for regulating cellular signal pathways in vivo, as well as bone mass in skeletal systems (10). After binding to estrogen, ESRα acts as a transcriptional factor that regulates gene expression and function by interacting with the regulatory regions of target genes (11).
ESRα gene polymorphisms have been among the most intensively studied polymorphisms in genetic regulation of KOA, but, with contradictory results (11-22). This disparity can be attributed to small sample sizes, low statistical power, and/or clinical heterogeneity. In view of the uncertain association between ESRα polymorphisms and KOA risk, we sought to obtain more precise information by conducting a systematic review and meta-analysis including all the evidence produced to the date.
Materials and Methods
Literature Search Strategy
To identify the case–control studies investigating the association between ESRα PvuII T>C, XbaI A>G and BtgI G>A polymorphisms and KOA risk, we conducted a search in PubMed, Google scholar, Web of Science, and SID databases using the following keywords: ‘’osteoarthritis’’, “knee osteoarthritis”, “KOA”, ‘’estrogen receptor alpha’’, ‘’ESRα’’, “PvuII T>C”, “XbaI A>G”, “BtgI G>A”, ‘’rs2234693’’, ‘’rs9340799’’, ‘’rs2228480’’, “polymorphism”, “mutation”, “variant”, “gene”, “genotype”, “SNP”, and “allele”. The last updated search was performed on March 1, 2017. Language restriction was set to English, Chinese and Persian. Additionally, the reference list of each retrieved article was thoroughly reviewed for more original papers.
Inclusion and Exclusion Criteria
The studies were further filtered to fit in the inclusion criteria that: a) full-text published studies; b) case-control or cohort studies; c) assessment of the association between ESRα PvuII T>C, XbaI A>G and BtgI G>A polymorphisms and KOA risk; d) having available genotype frequencies in both cases and controls for estimating an odds ratio (OR) with 95% confidence interval (CI). Studies without usable data or reviews were all excluded. For more than two studies with overlapping data, the study with the most subjects or newest published data was selected; and e) written in English or Persian. The exclusion criteria were as follows: a) abstract only, short communications or case reports, letter to editor, and reviews; b) studies on other ESRα polymorphisms; c) studies with only case subjects (no healthy controls); d) studies without detailed genotype frequencies, which were unable to be calculated OR; e) studies on other osteoarthritis types; and f) duplicate data publications from the same study.
Data Extraction
Necessary information was carefully extracted from all eligible publications by two independent authors. The following data were extracted for each study: the first author’s surname, year of publication, ethnicity of the subjects, number of KOA patients and controls, genotype distribution in cases and controls, minor allele frequencies (MAFs) in control subjects, and Hardy-Weinberg equilibrium test in control subjects. In case of evaluation conflicts, the two authors carried out discussions until a consensus was reached, otherwise, a 3rd author was consulted to resolve the dispute and a final decision was made through votes.
Quality Assessment
Two independent authors assessed the study quality using the Newcastle-Ottawa quality Scale which is a star rating system. The studies were qualified based on 3 broad perspectives: selection, comparability, and exposure (case-control studies) or outcome (cohort studies). Studies scoring five or more stars were considered as moderate to high quality (23).
Statistical Analysis
The strength of association between ESRα polymorphisms and KOA was assessed by using odds ratio (OR) and 95% confidence interval (CI). The significance of the pooled OR was determined with the Z-test. The meta-analysis was performed on the association between ESRα PvuII T>C polymorphism and KOA under the allele model (C vs. T), the heterozygote model (CC vs.TT), the homozygote model (CT vs. TT), the dominant model (CC+CT vs. TT), and the recessive model (CC vs. CT+TT). For ESRα XbaI A>G polymorphism and KOA under the allele model (G vs. A), the heterozygote model (GA vs. AA), the homozygote model (GG vs. AA), the dominant model (GG+GA vs. AA), and the recessive model (GG vs. GA+AA). For ESRα BtgI G>A polymorphism and KOA under the allele model (A vs. G), the heterozygote model (AG vs. GG), the homozygote model (AA vs. GG), the dominant model (AA+AG vs. GG), and the recessive model (AA vs. GA + GG). Heterogeneity was assessed by both the Q statistic as well as I2 statistics (24, 25). The heterogeneity was considered significant if either the Q statistic had a P<0.10. An I2 value of 0% represents no heterogeneity, while values of 25%, 50%, 75%, or more represent low, moderate, high, and extreme heterogeneity, respectively. When inter-study heterogeneity existed, a random-effects model weighted by the DerSimonian–Laird method was used to calculate pooled OR (26). Otherwise, a fixed-effects model weighted by the Mantel–Haenszel method would be applied (27). Chi-Square test was used to determine the frequency distribution of genotypes in control group of each study, which were in accordance with HWE. A P>0.05 signified a departure from HWE. Subgroup analyses were performed by ethnicity and HWE status. The one-way sensitivity analyses were used to assess the stability of the results, namely, a single study in the meta-analysis was omitted each time to reflect the influence of the individual data set to the pooled OR. Additionally, sensitivity analysis was performed to evaluate the stability of the results by removing the studies not in HWE. Visual inspection of Begg’s funnel plot symmetry was performed to assess the potential publication bias. Egger’s test was also conducted to analyze the publication bias statistically (P<0.05 was considered as statistically significant) (28, 29). In the presence of a bias, the Duval and Tweedie non-parametric ‘‘trim and fill’’ methods were used to adjust for it (30). All the statistical analyses were performed by comprehensive meta-analysis (CMA) V2.0 software (Biostat, USA). All tests were two-sided, and a P<0.05 was considered statistically significant.
Results
Characteristics of Studies
Based on our search strategy, the primary screening produced 26 potentially relevant articles. Fifteen articles were excluded because they clearly did not meet the inclusion criteria or overlapping references. Finally, a total of 22 case-control studies in eleven 11 publications were included in the meta-analysis involving 6,575 KOA cases and 7,459 controls (11-22). The main characteristics of studies included in the current meta-analysis are presented in Table 1; among them, nine studies were identified for the ESRαPvuII T>C polymorphism, including a total of 3,421 cases and 4,304 controls, for the ESRαXbaI A>G polymorphism, eight studies involved a total of 2,450 cases and 2,167 controls and for the ESRαBtgI G>A polymorphism three studies were identified covering a total of 333 cases and 619 controls (11-22). All selected studies were evaluated by Newcastle-Ottawa Scale and met the high quality [Table 2]. The studies were carried out in Netherlands, China, Korea, Spain, Mexico, and Thailand. The genotype frequencies in the control group of one study on ESRαBtgI G>A polymorphism was not in agreement with HWE (P<0.05).
Table 1.
Characteristics of the studies included in the meta-analysis
| First author | Country (Ethnicity) | Case/Control | Cases | Control | MAFs | HWE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Genotypes | Alleles | Genotypes | Alleles | |||||||||||
| Pvu II T>C | CC | TC | TT | C | T | CC | TC | TT | C | T | ||||
| Bergink 2003 (12) | Netherlands (Caucasian) | 1483/687 | 434 | 737 | 312 | 1605 | 1361 | 225 | 333 | 129 | 783 | 591 | 0.430 | 0.767 |
| Jin 2004 (13) | Korea (Asian) | 151/397 | 61 | 68 | 22 | 190 | 112 | 152 | 183 | 62 | 487 | 307 | 0.386 | 0.575 |
| Xue 2004 (14) | China (Asian) | 55/176 | 17 | 23 | 15 | 57 | 53 | 57 | 87 | 32 | 201 | 151 | 0.429 | 0.905 |
| Tian 2009 (15) | China (Asian) | 38/40 | 16 | 15 | 7 | 47 | 29 | 15 | 16 | 9 | 46 | 34 | 0.425 | 0.250 |
| Yang 2009 (16) | China (Asian) | 41/40 | 14 | 17 | 10 | 45 | 37 | 12 | 23 | 5 | 47 | 33 | 0.412 | 0.238 |
| Riancho a 2010 (17) | UK (Caucasian) | 445/862 | 77 | 245 | 123 | 399 | 491 | 167 | 442 | 253 | 776 | 948 | 0.549 | 0.292 |
| Riancho b 2010 (17) | Spain (Caucasian) | 272/802 | 53 | 140 | 79 | 246 | 298 | 179 | 394 | 229 | 752 | 852 | 0.531 | 0.699 |
| Riancho c 2010 (17) | Spain (Caucasian) | 254/473 | 46 | 143 | 65 | 235 | 273 | 80 | 217 | 176 | 377 | 569 | 0.601 | 0.349 |
| Borgonio-Cuadra 2012 (18) | Mexico (Mixed) | 115/117 | 52 | 49 | 14 | 153 | 77 | 51 | 50 | 16 | 152 | 82 | 0.350 | 0.507 |
| Dai 2014 (19) | China (Asian) | 469/514 | 167 | 217 | 85 | 551 | 387 | 198 | 242 | 74 | 638 | 390 | 0.379 | 0.996 |
| Liu 2014 (20) | China (Asian) | 98/196 | 30 | 41 | 27 | 101 | 95 | 63 | 97 | 36 | 223 | 169 | 0.431 | 0.900 |
| XbaI A>G | AA | GA | GG | A | G | AA | GA | GG | A | G | ||||
| Bergink (2003) (12) | Netherlands (Caucasian) | 1483/687 | 643 | 682 | 158 | 1968 | 998 | 372 | 263 | 52 | 1007 | 367 | 0.267 | 0.560 |
| Jin 2004 (14) | Korea (Asian) | 151/397 | 98 | 49 | 4 | 245 | 57 | 256 | 126 | 15 | 638 | 156 | 0.196 | 0.917 |
| Xue 2004 (14) | China (Asian) | 55/176 | 21 | 24 | 10 | 66 | 44 | 40 | 82 | 54 | 162 | 190 | 0.539 | 0.408 |
| Tian 2009 (15) | China (Asian) | 38/40 | 18 | 16 | 4 | 52 | 24 | 6 | 21 | 13 | 33 | 47 | 0.587 | 0.598 |
| Yang 2009 (16) | China (Asian) | 41/40 | 28 | 11 | 2 | 67 | 15 | 24 | 13 | 3 | 61 | 19 | 0.237 | 0.516 |
| Borgonio-Cuadra 2012 (18) | Mexico (Mixed) | 115/117 | 70 | 41 | 4 | 181 | 49 | 62 | 47 | 8 | 171 | 63 | 0.269 | 0.821 |
| Dai 2014 (19) | China (Asian) | 469/514 | 288 | 152 | 29 | 728 | 210 | 348 | 155 | 19 | 851 | 193 | 0.184 | 0.736 |
| Liu 2014 (20) | China (Asian) | 98/196 | 36 | 43 | 19 | 115 | 81 | 49 | 92 | 55 | 190 | 202 | 0.515 | 0.398 |
| BtgI G>A | GG | AG | AA | G | A | GG | GA | AA | G | A | ||||
| Jin 2004 (13) | Korea (Asian) | 151/397 | 84 | 57 | 10 | 225 | 77 | 257 | 122 | 18 | 636 | 158 | 0.199 | 0.472 |
| Jiao 2007 (21) | China (Asian) | 76/118 | 5 | 56 | 15 | 66 | 86 | 16 | 97 | 5 | 129 | 107 | 0.453 | <0.001 |
| Tawonsawatruk 2009 (22) | Thailand (Asian) | 104/104 | 62 | 37 | 5 | 131 | 17 | 63 | 37 | 4 | 163 | 45 | 0.216 | 0.615 |
Table 2.
Quality assessment conducted according to the Newcastle-Ottawa Scale for all the included studies
| First author | Quality indicators | ||
|---|---|---|---|
| Selection | Comparability | Exposure | |
| Bergink 2003 | *** | * | ** |
| Jin 2004 | *** | * | *** |
| Xue 2004 | *** | * | *** |
| Tian 2009 | ** | * | ** |
| Yang 2009 | *** | * | ** |
| Riancho a 2010 | *** | * | ** |
| Riancho b 2010 | *** | * | ** |
| Riancho c 2010 | *** | * | *** |
| Borgonio-Cuadra 2012 | ** | * | *** |
| Dai 2014 | *** | * | ** |
| Liu 2014 | **** | * | ** |
| Jiao 2007 | ** | * | ** |
| Tawonsawatruk 2009 | *** | * | ** |
Quantitative Synthesis
ESRα PvuII T>C Polymorphism
Table 3 shows the summary ORs for the ESRα PvuII T>C polymorphism and KOA risk. The pooled results based on all included studies did not show any significant association between the ESRα PvuII T>C polymorphism and KOA risk under the allele model (C vs. T: OR = 0.958, 95% CI = 0.894-1.025, P = 212, Figure 1A), the heterozygote model (CT vs. TT: OR = 0.971, 95% CI = 0.791-1.193, P = 0.78), homozygote model (CC vs. TT, OR = 0.888, 95% CI = 0.772-1.021, P = 0.096), the dominant model (CC+CT vs. TT: OR = 0.868, 95% CI = 0.664-1.135, P = 0.300), and the recessive model (CC vs. CT+TT: OR = 0.905, 95% CI = 0.813-1.008, P = 0.070) [Table 3]. In the subgroup analyses, there was a significant association between ESRα PvuII T>C polymorphism and KOA risk under the heterozygote model (CT vs. TT: OR = 0.750, 95% CI = 0.586-0.960, P = 0.022) in the Asians, but not in Caucasian and mixed populations.
Table 3.
The meta-analysis of ESRα Pvu II T>C polymorphism and KOA risk
| Subgroup | Study Number | Genetic Model | Type of Model | Heterogeneity | Odds ratio | Publication Bias | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| I2 (%) | PH | OR | 95% CI | Ztest | POR | PBeggs | PEggers | ||||
| Overall | |||||||||||
| 11 | C vs. T | Fixed | 24.38 | 0.211 | 0.958 | 0.894-1.025 | -1.247 | 0.212 | 0.350 | 0.678 | |
| 11 | CT vs. TT | Random | 53.75 | 0.017 | 0.971 | 0.791-1.193 | -0.279 | 0.780 | 0.533 | 0.323 | |
| 11 | CC vs.TT | Fixed | 10.23 | 0.347 | 0.888 | 0.772-1.021 | -1.665 | 0.096 | 0.640 | 0.722 | |
| 11 | CC+CT vs. TT | Random | 74.93 | <0.001 | 0.868 | 0.664-1.135 | -1.036 | 0.300 | 0.533 | 0.292 | |
| 11 | CC vs. CT+TT | Fixed | 0.00 | 0.942 | 0.905 | 0.813-1.008 | -1.812 | 0.070 | 0.436 | 0.073 | |
| By Ethnicity | |||||||||||
| Caucasian | |||||||||||
| 4 | C vs. T | Random | 65.99 | 0.032 | 1.003 | 0.865-1.163 | 0.039 | 0.969 | 0.308 | 0.204 | |
| 4 | CT vs. TT | Random | 68.68 | 0.023 | 1.155 | 0.890-1.499 | 1.082 | 0.279 | 0.308 | 0.203 | |
| 4 | CC vs.TT | Fixed | 52.37 | 0.098 | 0.925 | 0.780-1.098 | -0.888 | 0.374 | 0.308 | 0.190 | |
| 4 | CC+CT vs. TT | Random | 73.23 | 0.011 | 1.103 | 0.844-1.442 | 0.720 | 0.472 | 0.308 | 0.192 | |
| 4 | CC vs. CT+TT | Fixed | 0.00 | 0.739 | 0.878 | 0.765-1.008 | -1.841 | 0.066 | 0.308 | 0.338 | |
| Asian | |||||||||||
| 6 | C vs. T | Fixed | 0.00 | 0.687 | 0.905 | 0.797-1.026 | -1.557 | 0.120 | 0.452 | 0.769 | |
| 6 | CT vs. TT | Fixed | 0.00 | 0.467 | 0.750 | 0.586-0.960 | -2.289 | 0.022 | 0.452 | 0.585 | |
| 6 | CC vs.TT | Fixed | 0.00 | 0.646 | 0.788 | 0.610-1.018 | -1.826 | 0.068 | 1.000 | 0.859 | |
| 6 | CC+CT vs. TT | Random | 73.90 | 0.002 | 0.602 | 0.349-1.038 | 0.068 | 0.068 | 0.452 | 0.509 | |
| 6 | CC vs. CT+TT | Fixed | 0.00 | 0.827 | 0.935 | 0.779-1.122 | -0.724 | 0.469 | 0.707 | 0.445 | |
| Mixed | |||||||||||
| 1 | C vs. T | Ref. | 0.00 | 1.000 | 1.072 | 0.730-1.573 | 0.355 | 0.723 | NA | NA | |
| 1 | CT vs. TT | Ref. | 0.00 | 1.000 | 1.120 | 0.494-2.539 | 0.271 | 0.786 | NA | NA | |
| 1 | CC vs.TT | Ref. | 0.00 | 1.000 | 1.165 | 0.516-2.632 | 0.368 | 0.713 | NA | NA | |
| 1 | CC+CT vs. TT | Ref. | 0.00 | 1.000 | 1.143 | 0.530-2.465 | 0.341 | 0.733 | NA | NA | |
| 1 | CC vs. CT+TT | Ref. | 0.00 | 1.000 | 1.068 | 0.636-1.793 | 0.249 | 0.803 | NA | NA | |
Figure 1.
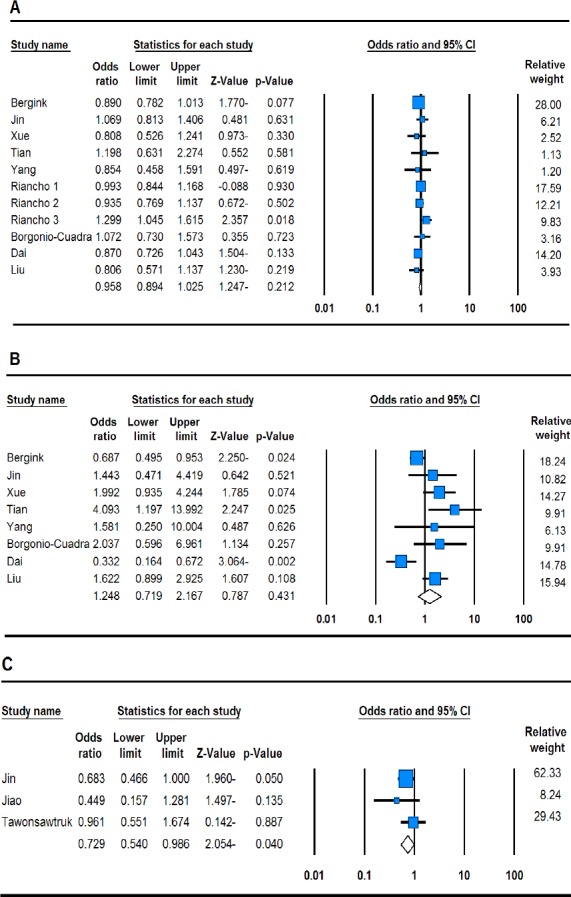
Forest plots describing the association of ESRα polymorphisms and KOA risk. A: PvuII T>C (allele model: C vs. T), B: XbaI A>G (dominant model: GG+GA vs. AA), C: BtgI G>A (recessive model: AA vs. GA+GG).
ESRα XbaI A>G Polymorphism
Table 4 shows the summary ORs for the ESRα XbaI A>G with KOA risk. Overall, this meta-analysis of included studies suggested that there was no significant association between ESRα XbaI A>G polymorphism and KOA risk under allele model (G vs. A: OR = 1.225, 95% CI = 0.896-1.675, P = 0.203), the heterozygote model (GA vs. AA: OR = 1.033, 95% CI = 0.537-1.986, P = 0.922), the homozygote model (GG vs. AA: OR = 1.572, 95% CI = 0.812-3.041, P = 0.179), the dominant model (GA+GG vs. AA: OR = 1.24, 95% CI = 0.719-2.167, p = 0.431, Figure 1B) and the recessive model (GG vs. GA+AA: OR = 1.252, 95% CI = 0.871-1.801, P = 0.225). In the subgroup analyses, there was a significant association between ESRα XbaI A>G with the KOA risk under allele model (G vs. A: OR = 0.719, 95% CI = 0.624-0.828, P <0.001), the homozygote model (GG vs. AA: OR = 0.569, 95% CI = 0.406-0.798, P = 0.001), the dominant model (GA+GG vs. AA: OR = 687, 95% CI = 0.495-0.953, P = 0.024) and the recessive model (GG vs. GA+AA: OR = 0.648, 95% CI = 0.540-0.777, P <0.001) in the Caucasians, but not in Asian and mixed populations.
Table 4.
The meta-analysis of ESRα XbaI A>G polymorphism and KOA risk
| Subgroup | Study Number | Genetic Model | Type of Model | Heterogeneity | Odds ratio | Publication Bias | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| I2 (%) | PH | OR | 95% CI | Ztest | POR | PBeggs | PEggers | ||||
| XbaI A>G | |||||||||||
| Overall | |||||||||||
| 8 | G vs. A | Random | 86.08 | <0.001 | 1.225 | 0.896-1.675 | 1.272 | 0.203 | 0.035 | 0.003 | |
| 8 | GA vs. AA | Random | 81.90 | <0.001 | 1.033 | 0.537-1.986 | 0.097 | 0.922 | 0.901 | 0.366 | |
| 8 | GG vs. AA | Random | 80.80 | <0.001 | 1.572 | 0.812-3.041 | 1.343 | 0.179 | 0.265 | 0.023 | |
| 8 | GG+GA vs. AA | Random | 73.93 | <0.001 | 1.248 | 0.719-2.167 | 0.787 | 0.431 | 0.536 | 0.148 | |
| 8 | GG vs. GA+AA | Random | 82.50 | <0.001 | 1.252 | 0.871-1.801 | 1.213 | 0.225 | 0.009 | <0.001 | |
| Caucasian | |||||||||||
| 1 | G vs. A | Ref. | 0.00 | 1.000 | 0.719 | 0.624-0.828 | -4.569 | <0.001 | NA | NA | |
| 1 | GA vs. AA | Ref. | 0.00 | 1.000 | 0.853 | 0.605-1.204 | -0.903 | 0.367 | NA | NA | |
| 1 | GG vs. AA | Ref. | 0.00 | 1.000 | 0.569 | 0.406-0.798 | -3.268 | 0.001 | NA | NA | |
| 1 | GG+GA vs. AA | Ref. | 0.00 | 1.000 | 0.687 | 0.495-0.953 | -2.250 | 0.024 | NA | NA | |
| 1 | GG vs. GA+AA | Ref. | 0.00 | 1.000 | 0.648 | 0.540-0.777 | -4.673 | <0.001 | NA | NA | |
| Asian | |||||||||||
| 6 | G vs. A | Random | 84.00 | <0.001 | 1.364 | 0.909-2.048 | 1.500 | 0.134 | 0.132 | 0.045 | |
| 6 | GA vs. AA | Random | 86.23 | <0.001 | 1.042 | 0.388-2.798 | 0.082 | 0.934 | 0.707 | 0.228 | |
| 6 | GG vs. AA | Random | 75.71 | 0.001 | 1.895 | 0.857-4.189 | 1.578 | 0.114 | 0.452 | 0.241 | |
| 6 | GG+GA vs. AA | Random | 74.31 | 0.002 | 1.380 | 0.659-2.891 | 0.853 | 0.394 | 1.000 | 0.600 | |
| 6 | GG vs. GA+AA | Random | 77.89 | <0.001 | 1.461 | 0.920-2.321 | 1.608 | 0.108 | 0.060 | 0.012 | |
| Mixed | |||||||||||
| 1 | G vs. A | Ref. | 0.00 | 1.000 | 1.361 | 0.887-2.088 | 1.412 | 0.158 | NA | NA | |
| 1 | GA vs. AA | Ref. | 0.00 | 1.000 | 1.745 | 0.489-6.220 | 0.858 | 0.391 | NA | NA | |
| 1 | GG vs. AA | Ref. | 0.00 | 1.000 | 2.258 | 0.648-7.865 | 1.279 | 0.201 | NA | NA | |
| 1 | GG+GA vs. AA | Ref. | 0.00 | 1.000 | 2.037 | 0.596-6.961 | 1.134 | 0.257 | NA | NA | |
| 1 | GG vs. GA+AA | Ref. | 0.00 | 1.000 | 1.380 | 0.819-2.325 | 1.210 | 0.226 | NA | NA | |
ESRα BtgI G>A Polymorphism
Table 5 summarizes the ORs for the ESRα BtgI G>A polymorphism with the KOA risk. Overall, this meta-analysis of included studies suggested that there was significant association between ESRα BtgI G>A polymorphism and KOA risk under the allele model (A vs. G: OR = 0.639, 95% CI = 0.515-0.793, P <0.001), the heterozygote model (AG vs. GG: OR = 0.526, 95% CI = 0.291-0.953, P = 0.034), the homozygote model (AA vs. GG: OR = 0.448, 95% CI = 0.240-0.838, P = 0.012), the dominant model (AA+AG vs. GG: OR = 0.469, 95% CI = 0.264-0.833, P = 0.010), and the recessive model (AA vs. GA + GG: OR = 0.729, 95% CI = 0.540-0.986, P = 0.040, Figure 1C). Moreover, a significant association was observed when stratified by HWE status only under the allele model (A vs. G: OR = 0.640, 95% CI = 0.496-0.825, P = 0.001).
Table 5.
The meta-analysis of ESRα BtgI G>A polymorphism and KOA risk
| Polymorphism | Study Number | Genetic Model | Type of Model | Heterogeneity | Odds ratio | Publication Bias | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| I2 (%) | PH | OR | 95% CI | Ztest | POR | PBeggs | PEggers | ||||
| BtgI G>A | |||||||||||
| 3 | A vs. G | Fixed | 32.61 | 0.227 | 0.639 | 0.515-0.793 | -4.064 | <0.001 | 0.296 | 0.294 | |
| 3 | AG vs. GG | Fixed | 59.94 | 0.082 | 0.526 | 0.291-0.953 | -2.117 | 0.034 | 1.000 | 0.865 | |
| 3 | AA vs. GG | Fixed | 60.89 | 0.078 | 0.448 | 0.240-0.838 | -2.513 | 0.012 | 0.296 | 0.651 | |
| 3 | AA+AG vs. GG | Fixed | 55.50 | 0.106 | 0.469 | 0.264-0.833 | -2.583 | 0.010 | 1.000 | 0.894 | |
| 3 | AA vs. GA+GG | Fixed | 0.00 | 0.390 | 0.729 | 0.540-0.986 | -2.054 | 0.040 | 1.000 | 0.790 | |
| By HWE | |||||||||||
| 2 | A vs. G | Fixed | 66.30 | 0.085 | 0.640 | 0.496-0.825 | -3.444 | 0.001 | NA | NA | |
| 2 | AG vs. GG | Fixed | 0.00 | 0.952 | 0.830 | 0.406-1.698 | -0.510 | 0.610 | NA | NA | |
| 2 | AA vs. GG | Fixed | 0.00 | 0.719 | 0.635 | 0.316-1.275 | -1.277 | 0.202 | NA | NA | |
| 2 | AA+AG vs. GG | Fixed | 0.00 | 0.833 | 0.700 | 0.352-1.388 | -1.022 | 0.307 | NA | NA | |
| 2 | AA vs. GA+GG | Fixed | 0.00 | 0.321 | 0.762 | 0.556-1.043 | -1.695 | 0.090 | NA | NA | |
Sensitivity Analyses
Sensitivity analyses were performed to assess the influence of each individual study on the pooled OR by sequential removal of individual studies. However, the results suggested that no individual study significantly affected the pooled OR, thus suggesting that the results of this meta-analysis are stable (data not shown). Additionally, sensitivity analysis was performed by excluding HWE-violating studies for ESRα BtgI G>A polymorphism and the corresponding pooled ORs were materially altered, indicating that the results are statistically affected by HWE status [Table 5].
Publication bias
Begg’s funnel plot and Egger’s test were performed to access the small study effects of the literatures. The funnel plot revealed no obvious publication bias for ESRα PvuII T>C and BtgI G>A polymorphisms, and this was confirmed by Begg’s test and Egger’s test [Figure 2A]. However, the shapes of the funnel plots revealed obvious asymmetry for ESRα XbaI A>G in the allele model [Figure 2B], homozygote model and recessive model [Figure 2C], suggesting that there were obvious publication biases in these two genetic models. Moreover, the results of Egger’s regression test also provided sufficient evidence for publication bias (allele model: PBegg’s = 0.035, PEgger’s = 0.003; the homozygote model: PBegg’s = 0.265, PEgger’s = 0.023; and the recessive model: PBegg’s = 0.009, PEgger’s <0.001). However, adjusting the models by the trim and fill method was not materially altered.
Figure 2.
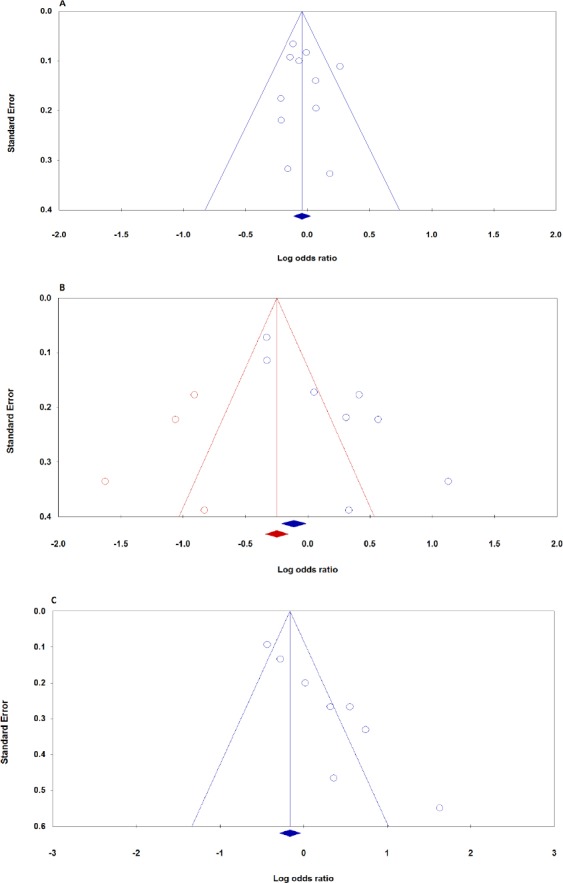
Begg’s funnel plots of the ESRα polymorphisms and KOA risk for publication bias test. A: Pvu II T>C (allele model: C vs. T), B: XbaI A>G (allele model: G vs. A, with trim and fill test), C: XbaI A>G (recessive model: GG vs. GA+AA).
Discussion
Despite the fact that ESRα gene is one of the most studied genes in OA, to the best of our knowledge this is the most comprehensive meta-analysis that focused on the association between ESRα PvuII T>C, XbaI A>G and BtgI G>A polymorphisms and susceptibility of KOA (31). In the present study, neither ESRα PvuII T>C and XbaI A>G polymorphisms had a statistically significant association with the risk of KOA in the overall population. Moreover, we have found a significant association between the ESRα PvuII T>C polymorphism and KOA in Asians under the heterozygote model, but not in Caucasian and mixed populations, and that the ESRα XbaI A>G polymorphism was significantly associated with KOA in Caucasian, but not Asian mixed populations. In a more recent meta-analysis by Ren et al. they have suggested that ERα PvuII polymorphism was not associated with OA in either population. However, they have observed that the ERα XbaI polymorphism associated with OA in Europeans but not Asians. In addition, we have found that ESRα BtgI G>A polymorphism significantly associated with KOA risk under all five genetic models.
Compared with the previous meta-analyses, in this meta-analysis we have focused only on association between ESRα gene polymorphisms and risk of KOA (32-36). Our meta-analysis results were different from a previous meta-analysis, which revealed no significant association between BtgI G>A polymorphism and risk of KOA risk. Several reasons may explain this difference (36-38). It seems the inclusion and exclusion criteria were different. However, Ma et al. suggested that XbaI A>G and BtgI G>A rather than Pvu II T>C polymorphisms are associated with OA risk (37). In another meta-analysis, Yin et al. found a significant associations between the XbaI A>G polymorphism and the OA risk in Europeans and Asians (34). Ren et al, suggested that there may be a significant association between the ERα XbaI polymorphism and OA by ethnicity (33).
The preset meta-analysis results are consistent with the study performed by Ge et al, who failed to detect any association between the ESRα PvuII polymorphism and fracture risk in postmenopausal women (39). However Sun et al., in a different meta-analysis, reported that ESRα PvuII polymorphism may be the risk factor for different cancers such as hepatocellular carcinoma, prostate cancer and gallbladder cancer (40). Luo et al. reported that ESRα PvuII and XbaI polymorphisms were significantly associated with precocious puberty susceptibility (41). In another meta-analysis, He et al. observed that ESRα PvuII polymorphism was significantly associated with risk of premature ovarian failure, while ESRα XbaI polymorphism was not associated with the condition risk (42). Therefore, these findings indicate that the ESRα polymorphisms exert different effect on various conditions. So, it is necessary to get a better understanding of ESRα polymorphisms on KOA susceptibility, especially when inclusive and controversial findings still exist.
Between-study heterogeneity is a common problem in meta-analysis for genetic association studies (43). In the current meta-analysis, we have used fixed-effects or random-effects models based on heterogeneity results. A significant heterogeneity was seen in association of ESRα polymorphisms for ESRα XbaI A>G under all genetic models and ESRα Pvu II T>C polymorphism under two heterozygote and dominant models with KOA risk. A number of characteristics that vary among studies could be the sources of heterogeneity between-study such as ethnicity, gender, sample selection, source of controls, age, sample size, environmental exposures etc. (43-45). As so, we used meta-regression and sensitivity analysis by ethnicity, which aim to reduce heterogeneity; however, the results indicated that ethnicity was not the source of heterogeneity in the study.
Publication bias is a known threat to the validity of meta-analysis, which occurs when studies with statistically significant or clinically favorable results are more likely to be published than studies with non-significant or unfavorable results. Consistent with the results of Yin et al., there were obvious publication biases in the XbaI A>G under the allele and recessive genetic models in this study. However, adjusting the models by the trim and fill method was not materially altered.
We conducted the largest and most comprehensive quantitative meta-analysis of the relationship between ESRα PvuII T>C, XbaI A>G and BtgI G>A polymorphisms and susceptibility of KOA. However, the results of the present meta-analysis should also be interpreted within the context of its limitations. The number of studies and the number of subjects in the studies included in the current meta-analysis were small or medium and had insufficient statistical power to detect the association. Therefore, more studies with larger sample size and providing more detailed information are needed. Secondly, the subjects in this meta-analysis were from mostly Asian descent populations; hence, our results are only applicable to this ethnic population. Therefore, more studies containing the full range of possible ethnic differences are required to avoid selection bias. Also, due to limited individual data, we did not conduct a more precise analysis on other covariates such as age, gender, and environmental factors. Moreover, in this meta-analysis publication bias existed for some genetic models. Only full-text articles published in English were included in this meta-analysis, missing some eligible studies which were unpublished or reported in other languages. This may bias the present results. Therefore, the results should be interpreted with caution. Finally, several genes were identified to significantly mutate in KOA. The possible gene–gene and gene–environment interactions may play central roles in the KOA susceptibility and need further confirmation in future studies.
In conclusion, our meta-analysis suggested that ESRα BtgI G>A rather than ESRα PvuII T>C and XbaI A>G polymorphisms is associated with an increased KOA risk in overall population. However, we have found that ESRα PvuII T>C and XbaI A>G polymorphisms are associated with KOA susceptibility by ethnicity backgrounds. Moreover, due to the limited sample size, more large-scale and multi-racial association studies are required to further clarify the genetic association between various ESRα polymorphisms and risk of KOA.
No specific funding was obtained to support the conduct of this study.
The authors declare that they have no competing interests.
Acknowledgment
Not applicable.
References
- 1.Loeser R. Age-related changes in the musculoskeletal system and the development of osteoarthritis. Clin Geriatr Med. 2010;26(3):371–86. doi: 10.1016/j.cger.2010.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jesus C, Jesus I, Agius M. Treatment of depression in patients with osteoarthritis: the importance of an early diagnosis and the role of Duloxetine. Psychiatr Danub. 2016;28(Suppl-1):149–53. [PubMed] [Google Scholar]
- 3.Brown TD, Johnston RC, Saltzman CL, Marsh JL, Buckwalter JA. Posttraumatic osteoarthritis: a first estimate of incidence, prevalence, and burden of disease. J Orthop Trauma. 2006;20(10):739–44. doi: 10.1097/01.bot.0000246468.80635.ef. [DOI] [PubMed] [Google Scholar]
- 4.Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis Cartilage. 2013;21(9):1145–53. doi: 10.1016/j.joca.2013.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sobhan MR, Mehdinejad M, Jamaladini MH, Mazaheri M, Zare-Shehneh M, Neamatzadeh H. Association between aspartic acid repeat polymorphism of the asporin gene and risk of knee osteoarthritis: a systematic review and meta-analysis. Acta Orthop Traumatol Turc. 2017 doi: 10.1016/j.aott.2017.08.001. S1017-995X(17):30278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: part I. Caspian J Intern Med. 2011;2(2):205–12. [PMC free article] [PubMed] [Google Scholar]
- 7.Roman-Blas JA, Castañeda S, Largo R, Herrero-Beaumont G. Osteoarthritis associated with estrogen deficiency. Arthritis Res Ther. 2009;11(5):241. doi: 10.1186/ar2791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alcazar L, Arakaki P, Godoy-Santos A, Santos M. Estrogen receptor polymorphism and its relationship to pathological process. Am J Med Sci. 2010;340(2):128–32. doi: 10.1097/MAJ.0b013e3181d4eb5d. [DOI] [PubMed] [Google Scholar]
- 9.Anousha N, Hossein-Nezhad A, Biramijamal F, Rahmani A, Maghbooli Z, Aghababaei E, et al. Association study of estrogen receptor alpha gene polymorphisms with spontaneous abortion: is this a possible reason for unexplained spontaneous abortion? Biomed Res Int. 2013;2013:256470. doi: 10.1155/2013/256470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tang L, Cheng GL, Xu ZH. Association between estrogen receptor αgene (ESR1) PvuII (C/T) and XbaI (A/G) polymorphisms and hip fracture risk: evidence from a meta-analysis. PLoS One. 2013;8(12):e82806. doi: 10.1371/journal.pone.0082806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Welboren WJ, Stunnenberg HG, Sweep FC, Span PN. Identifying estrogen receptor target genes. Mol Oncol. 2007;1(2):138–43. doi: 10.1016/j.molonc.2007.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bergink AP, van Meurs JB, Loughlin J, Arp PP, Fang Y, Hofman A, et al. Estrogen receptor alpha gene haplotype is associated with radiographic osteoarthritis of the knee in elderly men and women. Arthritis Rheum. 2003;48(7):1913–22. doi: 10.1002/art.11046. [DOI] [PubMed] [Google Scholar]
- 13.Jin SY, Hong SJ, Yang HI, Yoo MC, Lee HJ, Hong MS, et al. Estrogen receptor-alpha gene haplotype is associated with primary knee osteoarthritis in Korean population. Arthritis Res Ther. 2004;6(5):R415–21. doi: 10.1186/ar1207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Xue Y, Li D, Yao L, Zhou Y, Xiao D, Guo SQ. Relationship between estrogen receptor gene polymorphism and osteoarthritis in Han women. Chin J Rheumatol. 2004;8(2):583–6. [Google Scholar]
- 15.Tian Z, Guo X, Zhou F, Huang CX, Su M, Long XL. Study on relationship between polymorphisms of estrogen alpha receptor gene and primary knee osteoarthritis among women in human. Pract Prevent Med. 2009;16(1):1724–7. [Google Scholar]
- 16.Yang JX, Fu SJ, Xiao FS. Case-control study between estrogen receptor gene polymorphisms and osteoarthritis in southern Sichuan high fluoride areas. West China Med J. 2009;24(1):826–9. [Google Scholar]
- 17.Riancho JA, Garcia-Ibarbia C, Gravani A, Raine EV, Rodriguez-Fontenla C, Soto-Hermida A, et al. Common variations in estrogen-related genes are associated with severe large-joint osteoarthritis: a multicenter genetic and functional study. Osteoarthritis Cartilage. 2010;18(7):927–33. doi: 10.1016/j.joca.2010.04.002. [DOI] [PubMed] [Google Scholar]
- 18.Borgonio-Cuadra VM, Gonzalez-Huerta C, Duarte-Salazar C, de Los Angeles Soria-Bastida M, Cortes-Gonzalez S, Miranda-Duarte A. Analysis of estrogen receptor alpha gene haplotype in Mexican mestizo patients with primary osteoarthritis of the knee. Rheumatol Int. 2012;32(5):1425–30. doi: 10.1007/s00296-011-1890-2. [DOI] [PubMed] [Google Scholar]
- 19.Dai X, Wang C, Dai J, Shi D, Xu Z, Chen D, et al. Association of single nucleotide polymorphisms in estrogen receptor alpha gene with susceptibility to knee osteoarthritis: a case-control study in a Chinese Han population. Biomed Res Int. 2014;2014:151457. doi: 10.1155/2014/151457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Liu W, Shao FM, Yan L, Cao HX, Qiu D. Polymorphisms in the gene encoding estrogen receptor alpha are associated with osteoarthritis in Han Chinese women. Int J Clin Exp Med. 2014;7(12):5772–7. [PMC free article] [PubMed] [Google Scholar]
- 21.Jiao B. Single nucleotide polymorphisms of osteoarthritis-related susceptibility genes. Beijing: Capital Institute of Physical Education; 2007. [Google Scholar]
- 22.Tawonsawatruk T, Trachoo O, Channoom T, Sura T, Eu-ahsunthornwattana J, Woratanarat P, et al. Association of estrogen receptor-alpha single-nucleotide polymorphism (codon 594 G-->A) and Thai patients affected by knee osteoarthritis. J Med Assoc Thai. 2009;92(Suppl 6):S45–50. [PubMed] [Google Scholar]
- 23.Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. The Ottawa Hospital. 2014 Available at: URL: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp;
- 24.Cochran WG. The combination of estimates from different experiments. Biometrics. 1954;10(1):101–29. [Google Scholar]
- 25.Khoram-Abadi KM, Forat-Yazdi M, Kheirandish S, Saeidi N, Zarezade Z, Mehrabi N, et al. DNMT3B -149 C>T and -579 G>T polymorphisms and risk of gastric and colorectal cancer: a Meta-analysis. Asian Pac J Cancer Prev. 2016;17(6):3015–20. [PubMed] [Google Scholar]
- 26.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 27.Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–48. [PubMed] [Google Scholar]
- 28.Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101. [PubMed] [Google Scholar]
- 29.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- 31.Chapman K, Valdes AM. Genetic factors in OA pathogenesis. Bone. 2012;51(2):258–64. doi: 10.1016/j.bone.2011.11.026. [DOI] [PubMed] [Google Scholar]
- 32.Wang Q, Yan XB, Sun QQ, Hu AM, Liu HL, Yin YW. Genetic polymorphism of the estrogen receptor alpha gene and susceptibility to osteoarthritis: evidence based on 15,022 subjects. Curr Med Res Opin. 2015;31(6):1047–55. doi: 10.1185/03007995.2015.1037727. [DOI] [PubMed] [Google Scholar]
- 33.Ren Y, Tan B, Yan P, You Y, Wu Y, Wang Y. Association between polymorphisms in the estrogen receptor alpha gene and osteoarthritis susceptibility: a meta-analysis. BMC Musculoskelet Disord. 2015;16(1):44. doi: 10.1186/s12891-015-0506-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Yin YW, Sun QQ, Hu AM, Wang Q, Liu HL. Association of rs9340799 polymorphism in estrogen receptor alpha gene with the risk of osteoarthritis: evidence based on 8,792 subjects. Med Genet Genomics. 2014;290(2):513–20. doi: 10.1007/s00438-014-0940-3. [DOI] [PubMed] [Google Scholar]
- 35.Kerkhof HJ, Meulenbelt I, Carr A, Gonzalez A, Hart D, Hofman A, et al. Common genetic variation in the Estrogen Receptor Beta (ESR2) gene and osteoarthritis: results of a meta-analysis. BMC Med Genet. 2010;11(1):164. doi: 10.1186/1471-2350-11-164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wise BL, Demissie S, Cupples LA, Felson DT, Yang M, Shearman AM, et al. The relationship of estrogen receptor and genes with osteoarthritis of the hand. J Rheumatol. 2009;36(12):2772–9. doi: 10.3899/jrheum.081208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ma H, Wu W, Yang X, Liu J, Gong Y. Genetic effects of common polymorphisms in estrogen receptor alpha gene on osteoarthritis: a meta-analysis. Int J Clin Exp Med. 2015;8(8):13446–54. [PMC free article] [PubMed] [Google Scholar]
- 38.Lee YH. Meta-analysis of genetic association studies. Ann Lab Med. 2015;35(3):283–7. doi: 10.3343/alm.2015.35.3.283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ge YZ, Xu LW, Jia RP, Xu Z, Li WC, Wu R, et al. Association of polymorphisms in estrogen receptors (ESR1 and ESR2) with male infertility: a meta-analysis and systematic review. J Assist Reprod Genet. 2014;31(5):601–11. doi: 10.1007/s10815-014-0212-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Sun H, Hou J, Shi W, Zhang L. Estrogen Receptor 1 (ESR1) genetic variations in cancer risk: a systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2015;39(1):127–35. doi: 10.1016/j.clinre.2014.07.016. [DOI] [PubMed] [Google Scholar]
- 41.Luo Y, Liu Q, Lei X, Wen Y, Yang YL, Zhang R, et al. Association of estrogen receptor gene polymorphisms with human precocious puberty: a systematic review and meta-analysis. Gynecol Endocrinol. 2015;31(7):516–21. doi: 10.3109/09513590.2015.1031102. [DOI] [PubMed] [Google Scholar]
- 42.He M, Shu J, Huang X, Tang H. Association between estrogen receptora gene (ESR1) PvuII (T/C) and XbaI (A/G) polymorphisms and premature ovarian failure risk: evidence from a meta-analysis. J Assist Reprod Genet. 2014;32(2):297–304. doi: 10.1007/s10815-014-0393-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sobhan MR, Forat-Yazdi M, Mazaheri M, Zare-Shehneh M, Neamatzadeh H. Association between the DNA repair gene XRCC3 rs↧39 polymorphism and risk of osteosarcoma: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2017;18(2):549–55. doi: 10.22034/APJCP.2017.18.2.549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Jafari-Nedooshan J, Forat-Yazdi M, Neamatzadeh H, Zare-Shehneh M, Kargar S, Seddighi N. Genetic Association of XRCC1 gene rs1799782, rs25487 and rs25489 polymorphisms with risk of thyroid cancer: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2017;18(1):263–70. doi: 10.22034/APJCP.2017.18.1.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Mehdinejad M, Sobhan MR, Mazaheri M, Zare-Shehneh M, Neamatzadeh H, Kalantar SM. Genetic association between ERCC2, NBN, RAD51 gene variants and osteosarcoma risk: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2017;18(5):1315–21. doi: 10.22034/APJCP.2017.18.5.1315. [DOI] [PMC free article] [PubMed] [Google Scholar]