

Abstract
Purpose The aim of the study was to evaluate the “over the top” (OTT) nonanatomical technique for revision of anterior cruciate ligament (ACL) reconstruction.
Methods Twenty-four patients with a mean age of 31.9 ± 11.2 years underwent revision of ACL reconstruction using OTT technique. International Knee Documentation Committee (IKDC) score, Knee Injury and Osteoarthritis Outcome Score (KOOS), Lysholm score, Tegner score, Subjective Patient Outcome for Return to Sport (SPORTS) score, Anterior Cruciate Ligament-Return to Sport After Injury (ACL-RSI) scale, and KT-1000 evaluation were recorded at a mean follow-up of 30.7 ± 18.9 months.
Results Postoperatively, the IKDC objective total score significantly improved ( p = 0.0046). The KOOS, Lysholm, and Tegner scores also improved, but the results were not statistically significant (62.4 vs. 72.6, 6.5 vs. 75.8, and 4.1 vs. 6.0, respectively). The subjective IKDC evaluation score improved from an average of 51.1 points to 63.7 points at the last follow-up ( p = 0.0027). The RTP prevalence was 81.8%, with 44.4% of the patients returning to the same preinjury level. According to the SPORTS score, 16.6% of patients played sport without limitations in activity and performance. The average ACL-RSI score was 52.1 ± 27.0. No major complications were reported. A total of 21.5% of patients underwent surgical removal of staples. The failure prevalence was 14.3% and the cumulative survivorship, calculated using the Kaplan–Meier method, was equal to 70% at 60 months of follow-up.
Conclusion The OTT technique in the revision ACL reconstruction provided improvement in objective and subjective scores, good RTP prevalence, and acceptable rate of complication and failure. One of the advantages was the possibility to avoid the femoral tunnel.
Level of Evidence Level IV, therapeutic case series.
Keywords: anterior cruciate ligament, over the top, revision
Introduction
Anterior cruciate ligament (ACL) lesion is a very common injury during sport and daily activities. The purposes of an ACL arthroscopic reconstruction are to recover normal joint laxity, prevent further trauma, allow the return to patients' previous activity level (sport and work), and possibly avoid the early osteoarthritic changes observed in unstable knees. 1 2 It has been estimated that the number of ACL reconstructions (ACL-Rs) in the United States increased from 32.9/100,000 person-years in 1994 to 43.5/10,000 person-years in 2006. 2
Patients treated for revision ACL-R are particularly interesting because risk factors that increase the likelihood of multiple failures have not yet been determined. 3 Younger age, early return to pivoting sports, family history of ACL injury, 4 5 6 and the use of allografts 7 have been shown to be risk factors for primary ACL-R failure.
Although surgical techniques have improved over the decades, the failure prevalence of ACL-R in the literature is reported to range from 3 to 29.5%. 3 7 A recent meta-analysis reported failure prevalence to range from 4.3 to 12.7% 8 due to several reasons, including young age, high level of sports activity, prior meniscectomy, and surgical errors. 4 Consequently, the number of revision ACL-R has increased in recent years. 9
Revision ACL-R may be a demanding procedure with the aim to restore normal joint laxity and knee function in a multiple injured joint with altered anatomy. Therefore, clinical results of revisions are generally considered inferior compared with primary ACL-R. 10
The “over the top” (OTT) technique is a combined arthroscopic intra- and extra-articular procedure, which combines an anatomic tibial tunnel and placement of the graft behind the femoral condyle in an “over the top position” with or without an extra-articular augmentation. Normally, the length of the graft allows the addition of a lateral tenodesis. 11 12 The main advantage of this technique, in the case of revision surgery, is the possibility to avoid the problem of femoral tunnel management (malposition, enlargement, or deficit of posterior femoral wall) and control the lateral instability, which is often associated with rerupture. 13 14 This technique can be performed using either autograft or allograft.
The objective of this retrospective study was to evaluate the results of revision ACL-R performed using the OTT technique. We hypothesize that OTT technique is effective in revision ACL-R in terms of clinical outcomes, patient satisfaction, return-to-sport, and rate of complications and failures.
Methods
Study Design
The Institutional Review Board (IRB) at the authors' institution defined this study as an exempt from IRB approval (retrospective study on a well-established surgical procedure).
Participants
All the patients who underwent a revision of ACL-R using the OTT technique at our institution by the senior authors between January 2008 and July 2015 were enrolled. Preoperative evaluation included a complete history, physical and radiographic examinations, and magnetic resonance (MR) to confirm the presence of an ACL rerupture and rule out possible associated lesions. The cause of failure was identified and recorded. Patients' data from surgery, sports participation, and rehabilitation were collected ( Table 1 ). Furthermore, data regarding complications, such as fever, wound problems or thrombotic events, and revision surgeries, were recorded.
Table 1. Collected data, including associated lesions and surgery, preoperative sports, physioterapy, and failures.
| Surgery | |
|---|---|
| Associated lesions | |
| Meniscal tears | |
| Medial | 7 (5 longitudinal lesions of the posterior horn, 2 bucket-handle lesions) |
| Lateral | 3 (2 longitudinal lesions of posterior horn, 1 bucket-handle lesion) |
| Ligaments tears | 1 (MCL laxity) |
| Other | 2 (tibial plateau fracture) |
| Additional surgical procedures | |
| Meniscectomy | 6 |
| Meniscal suture | 2 |
| Other | 2 (1 chondral debridement, 1 high tibial osteotomy) |
| Postoperative complications | – |
| Staples pain | |
| Femoral | 4 |
| Tibial | 1 |
| Both | 3 |
| Staples removal | 3 |
| Traumatic rupture of the graft | 1 |
| Recurrent instability after surgery | 2 |
| Revision ACL surgery | 1 |
| Waiting for revision surgery | – |
| Other surgery | 1 (meniscectomy) |
| Sport | |
| Preinjury sport ( n ) | 22 |
| Contact sports | 14 |
| Noncontact sport | 8 |
| Preinjury level sport practice | |
| Recreational | 7 |
| Competitive | 15 |
| ACL injury during sports | 17 |
| Physiotherapy | 24 |
| Start after surgery | |
| < 1 mo | 12 |
| > 1 mo | 12 |
| Duration | |
| Mean ± SD | 4.3 ± 2.1 |
| < 3 mo | 5 |
| > 3 mo | 19 |
| Sessions per week, mean ± SD | 3.5 ± 1 |
| Failures | 4 |
| Further injury | 1 |
| Recurrent instability | 3 |
Abbreviations: ACL, anterior cruciate ligament; MCL; SD, standard deviation.
In this study, traumatic rerupture of the operated ligament, subjective instability, and objective instability (positive Lachman test with difference greater than 5 mm compared with the contralateral, rotational laxity with clunk or gross clunk at the Pivot shift test) were considered as failure.
Surgical Technique
The patient was placed in the supine position, and a pneumatic tourniquet was placed around the proximal part of the tight. During preliminary arthroscopic evaluation performed by anterolateral and anteromedial portals, meniscectomy or chondroplasty was performed when necessary. ACL remnant was carefully debrided, and the tibial insertion area of the ruptured ACL graft and the intercondylar notch was prepared. Through a 3 to 4 cm oblique incision in the proximal medial metaphysis of the tibia, the gracilis and semitendinosus (G-ST) tendons were isolated and harvested carefully with a tendon stripper. The maximum possible portion of the tendon was obtained while preserving the tibial insertion. The harvested tendons were sutured together. When allograft was used, it was fixed at the proximal part of the tibia.
Tibial tunnel was drilled with a guidewire under arthroscopic control, trying to reproduce the posteromedial part of ACL tibial insertion. The intra-articular emergence was placed at the center of the native footprint. A messenger wire was passed into the joint through the tibial tunnel and taken through the anteromedial portal. The lateral femoral condyle (LFC) was then exposed through a 3 to 5 mm lateral incision, and the ileotibial band was divided in its posterior third and retracted anteriorly. A second messenger wire was passed into the OTT position through the superolateral portion of the intercondylar groove and taken outside the tibial tunnel using the previous messenger wire. The graft was passed through the tibial tunnel and into the OTT position. The graft was manually tensioned and fixed with two titanium staples with the knee in 90 degrees of flexion, external rotation of the foot, and a posterior drawer applied. The remaining part of the graft was then passed deep into the ileotibial band and over the lateral collateral ligament, as a lateral plasty, and fixed with one titanium staple below Gerdy's tubercle.
In our study, we used 8 autografts (G-ST) and 16 allografts (10 Achilles tendons and 6 posterior tibial tendons).
The patients were advised to undergo a rehabilitation program. When a meniscal suture or cartilage procedure was performed (41.6% of patients), the postoperative protocol included a restriction of weight bearing depending on the associated procedures, for at least 4 weeks. Otherwise, patients were allowed for immediate full weight-bearing and range of motion (ROM). Return to full sport participation was allowed, depending on the type of sport and level, between 6 and 9 months postoperatively. The criterion used to allow RTP was related to clinical knee stability, without pain or effusion and satisfying functional testing (isokinetic test at least 85% compared with the contralateral and single-limb hop test greater than 90% compared with the contralateral) as described in the literature. 15
Outcome Measures
International Knee Documentation Committee (IKDC) subjective and objective scores, Knee Injury and Osteoarthritis Outcome Score (KOOS), Tegner score, and Lysholm score were recorded pre-operatively and at the last follow-up.
Patients were asked to assess their satisfaction through two different questions: whether they would have the procedure performed again and what was the rate of knee function (from 0 to 100% compared with preinjury level) at the time of the visit. The Subjective Patient Outcome for Return to Sport (SPORTS) score was recorded to evaluate the return to sport, and the Anterior Cruciate Ligament-Return to Sport After Injury (ACL-RSI) scale was recorded to assess the psychological and emotional component in return to sport.
Statistical Analysis
Descriptive statistics was used for all demographic, subjective outcomes, sports participation, and rehabilitation data. Continuous variables were presented with average and standard deviation (SD). Categorical variables were presented as frequency and percentages. To analyze the differences between preoperative and postoperative scores or data, t -test was applied to normally distributed continuous outcomes, while chi-square test was used for categorical outcomes. For all tests, a p- value less than 0.05 was considered statistically significant. All statistical analyses were performed using Microsoft Excel.
Results
The average follow-up was 30.7 ± 18.9 months. Twenty-eight patients (28 knees) were enrolled in the study. Patients were contacted by phone and asked to participate in the study. Two patients were untraceable and two patients refused to participate in the study, leaving 24 patients (85.8%) in the study. The average age was 31.9 ± 11.2 years. There were 19 men (79.2%) and 5 women (20.8%). Eighteen patients were available for a clinical evaluation, while six patients (25%) could not be clinically evaluated because they were unable to come for the visit. Consequently, these patients were excluded from the objective evaluation and underwent a telephone questionnaire evaluating subjective outcomes and RTP.
Twenty-one patients had chronic lesions (duration greater than 3 months). Furthermore, thirteen patients had associated lesions. Additional surgical procedures were performed in 10 patients. All patients underwent postoperative rehabilitation. Patients underwent physical therapy for an average period of 4.3 ± 2.1 months, with an average of 3.5 ± 1.0 sessions per week. Twelve patients started the rehabilitation before the month after surgery, and 19 patients performed the rehabilitation for more than 3 months. All data are shown in Table 1 .
Objective evaluation was available for 18 patients. The overall IKDC objective score showed significant differences between preoperative and postoperative period ( p = 0.0046), with 72.2% patients graded as normal or nearly normal at the last follow-up compared with 0% in the preoperative setting ( Fig. 1 ). The results of manual knee evaluations significantly improved in the postoperative period. Particularly, only two patients showed a positive Lachman test +++ . Furthermore, one of them showed a gross clunk at Pivot shift test. The results are reported in Table 2 . At the KT-1000 evaluation, the average side-to-side difference in the postoperative period was 3.1 mm ± 2.42 (four patients presented a side-to-side difference ≥ 5 mm).
Fig. 1.
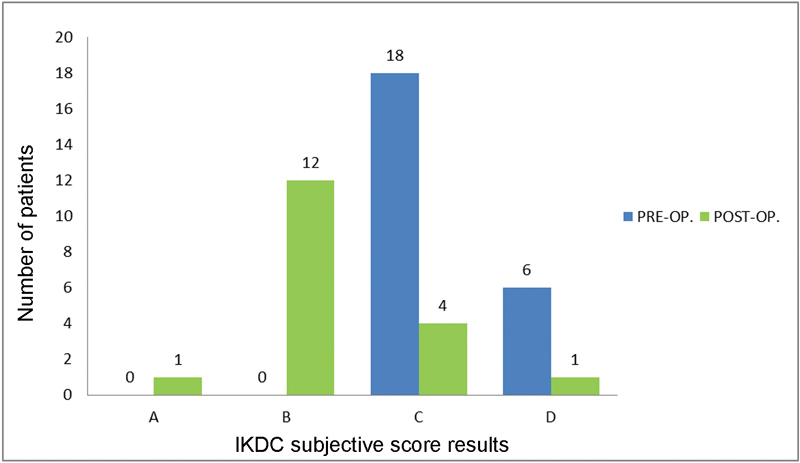
International Knee Documentation Committee (IKDC) score.
Table 2. Number and percentage of patients after manual tests (Lachman test, anterior drawer test, Pivot shift test, and KT-1000 arthrometer score).
| Preoperative ( n = 24) | Postoperative ( n = 18) | p -Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Normal | 1+ | 2+ | 3+ | Normal | 1+ | 2+ | 3+ | ||
| Lachman | 0 | 1 | 18 | 5 | 4 | 12 | 2 | 0 | 0.0001 |
| Anterior drawer test | 1 | 4 | 15 | 4 | 8 | 8 | 2 | 0 | 0.0123 |
| Pivot shift | 5 | 1 | 14 | 4 | 7 | 10 | 0 | 1 | 0.0018 |
| Lachman > 5 mm | |||||||||
| Preoperative | 23 (95.8%) | ||||||||
| Postoperative | 2 (11.1%) | ||||||||
| Pivot shift clunk or gross clunk | |||||||||
| Preoperative | 18 (75%) | ||||||||
| Postoperative | 1 (5.6%) | ||||||||
| KT-1000 arthrometer scores (mm) in postoperative period ( n = 18) | |||||||||
| Injured knee average (±SD) | 6.7 ± 2.5 | ||||||||
| Healty knee average (±SD) | 3.6 ± 1.8 | ||||||||
| Difference average (±SD) | 3.1 ± 2.42 | ||||||||
| p -Value | 0.0001 | ||||||||
Abbreviations: SD, standard deviation.
The KOOS, Lysholm, and Tegner scores improved in the postoperative period, but the differences were not significant. At subjective IKDC form evaluation, the mean scores of pre- and postoperative period were 51.1 versus 63.7 points, respectively ( p = 0.0027), with a statistically significant improvement. The results are summarized in Table 3 . Twenty patients (83.3%) stated that they would have the surgery performed again. Furthermore, the average “satisfaction” score was 69.0 ± 17.4%.
Table 3. Subjective scores: Lysholm score, Tegner score, KOOS, and subjective IKDC (mean ± SD, n = 24) .
| Preoperative | Postoperative | p -Value | |
|---|---|---|---|
| Lysholm | 64.5 ± 25.1 | 75.8 ± 26.4 | 0.1324 |
| Tegner | 4.1 ± 2.5 | 6.0 ± 2.3 | 0.1220 |
| KOOS | |||
| Pain | 74.8 ± 24.5 | 80.0 ± 19.3 | 0.4306 |
| Symptoms | 66.4 ± 21.1 | 71.6 ± 20.8 | 0.3760 |
| Activity daily living | 78.9 ± 28.7 | 86.7 ± 20.7 | 0.7157 |
| Sport | 47.9 ± 34.5 | 58.1 ± 33.9 | 0.3062 |
| Quality of life | 44.0 ± 28.0 | 56.8 ± 31.3 | 0.2905 |
| Subjective IKDC | 51.1 ± 14.0 | 63.7 ± 13.7 | 0.0027 |
Abbreviations: IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; SD, standard deviation.
Twenty-two patients (91.6%) were involved in some sports before injury, and 63.6% of them were involved in contact sports ( Table 1 ). The average prevalence of return to sport was 81.8%, with 44.4% of patients returning to the same preinjury level. Reasons for nonreturning to sport or returning to a lower level are shown in Fig. 2 . Fear of reinjury during sports was detected in three cases (12.5%). At the ACL-RSI score, the average score was 52.1%. The subjects who did not return to sport obtained a lower score (cutoff = 60) at ACL-RSI scale ( p = 0.0168).
Fig. 2.
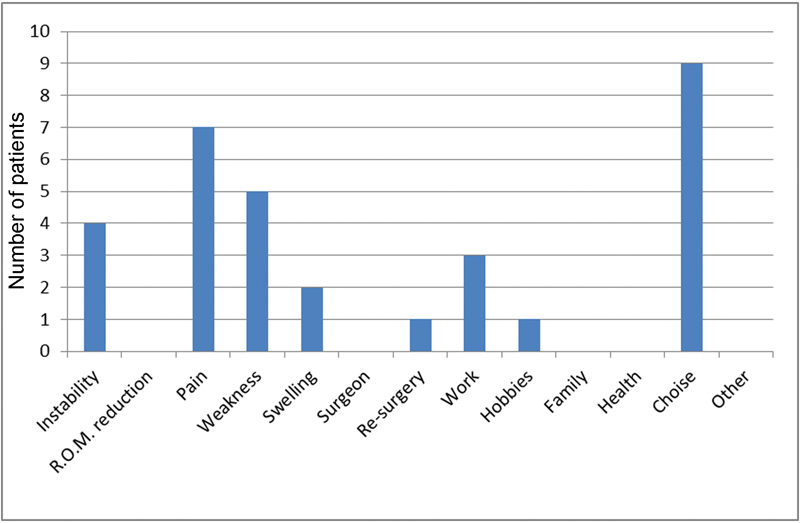
Reasons for nonreturn to sport or return to sport at a lower level than the preinjury period.
At the last follow-up, nine patients (37.5%) reported a SPORTS score of 9 or 10, meaning being able to play sports without limitations and with or without slight pain ( Fig. 3 ). Table 4 shows patient data related to the return to sport.
Fig. 3.
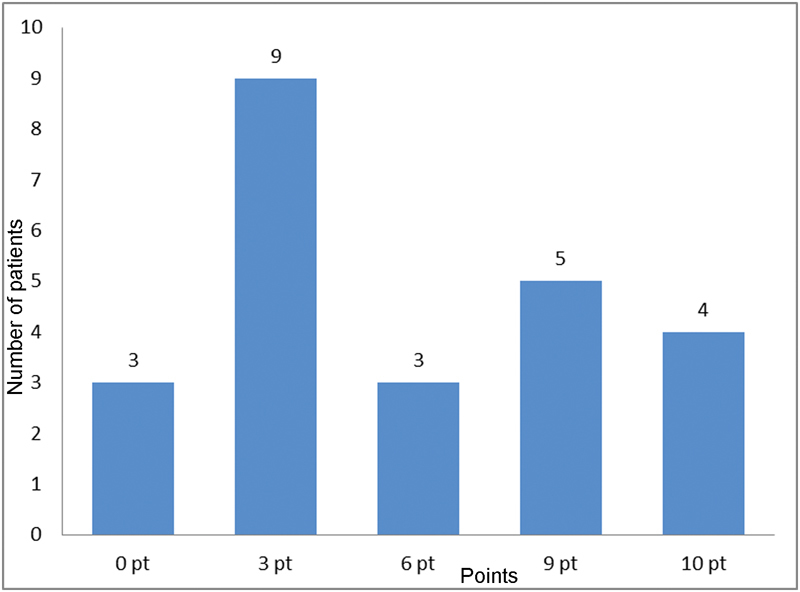
Distribution of SPORTS score.
Table 4. Patient data related to return to sport (number of patients, time after surgery, level of sport, ACL-RSI score; n = 24) .
| Return to sport ( n ) | 18 |
| Average time after surgery | 8.0 ± 4.6 months |
| After surgery level sport practice | |
| Same | 8 |
| Lower | 10 |
| ACL-RSI average score | 52.1 ± 27.1 |
| Patients returned to sport | 18 |
| ACL-RSI < 60 | 8 |
| ACL-RSI > 60 | 10 |
| Patients nonreturned to sport | 6 |
| ACL-RSI < 60 | 6 |
| ACL-RSI > 60 | 0 |
| p -Value | 0.0168 |
Abbreviation: ACL-RSI, Anterior Cruciate Ligament-Return to Sport After Reinjury.
No postoperative complications were observed, such as infection or deep venous thrombosis. Eight patients (33.3%) reported pain related to the presence of the staples used to fix the graft. Three of these patients required removal of the staples. One patient only required further arthroscopy for subtotal meniscectomy at 2.5 years of follow-up. Out of the 24 patients, 1 had traumatic graft rupture at 19 months of follow-up, but the patient rejected any further surgery. One patient showed instability at Lachman and Pivot shift tests. Furthermore, the two patients who refused to participate in the study were not satisfied with the outcome of the surgery. They reported recurrent instability that led them to undergo further revision surgery in other orthopaedic centers. Therefore, these patients have been considered as failures, with a total prevalence of 14.3%. All data are shown in Table 1 .
Considering these four failures, the cumulative survivorship, calculated using the Kaplan–Meier method was equal to 70% at 60 months of follow-up ( Fig. 4 ).
Fig. 4.
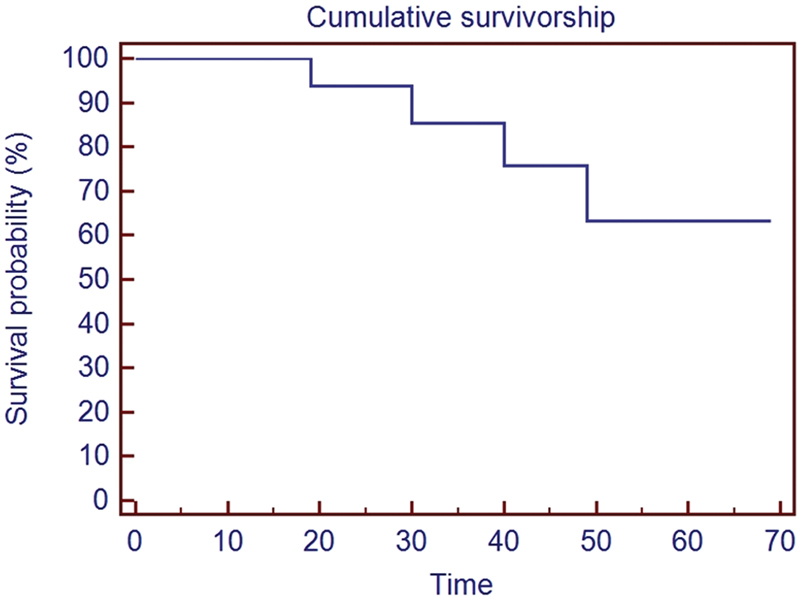
Survivorship calculated using the Kaplan–Meier method.
Discussion
Revision ACL-R represents a challenge for the orthopaedic surgeon, because graft choice options and positioning of bone tunnels are more limited than with primary ACL-R, sometimes requiring staged procedures to restore normal joint laxity and bone stock. 16
The OTT technique performed in this study was first described in 1992 by Marcacci et al. 12 This technique may have different advantages compared with anatomic revision ACL-R, particularly regarding the femoral tunnel management. During revision surgery, when the posterior femoral wall is found to be deficient, the OTT technique may be a valid option, also to overcome the problem of femoral tunnel malpositioning. 13 14 It is, therefore, a simple solution for revision cases, eliminating the issues of management of femoral tunnel malposition, presence of intra-articular hardware, and tunnel enlargement. 17 It must be considered that this nonanatomical fixation of the graft may lead to a partial loss of knee stability, which could be less evident in anatomical reconstruction of ACL. Nevertheless, in this study, the rate of chronic instability was not superior to the use of other anatomical techniques. Furthermore, our patients were not elite athletes; so, the possible instability resulting from the surgery might not have interfered with ordinary daily life activities.
In this study, 72% of patients had a high objective IKDC score in postoperative period, similarl to that reported by Buda et al 18 with OTT procedures and Hwan Ahn et al 19 using anatomical techniques.
KT-1000 testing revealed that the average side-to-side difference after surgery was 3.1 mm. This result is in line with the result reported by Buda et al 18 for revisions using OTT technique, but higher than the mean values obtained by Wegrzyn et al 20 and Salmon et al 21 using anatomical techniques. Regarding subjective evaluation, the mean IKDC subjective score, KOOS score, Lysholm score, and Tegner score were lower than the results of current literature regarding revision surgery, both with OTT technique 18 and anatomical procedures. 19 Despite all the scores displaying improvement at the last follow-up, only the IKDC subjective score demonstrated a statistically significant improvement ( p = 0.0027), probably due to the fact that patients had minimal symptoms even before surgery. Similarly, a statistically significant improvement in the subjective IKDC score was reported by Griffith et al 22 ( p < 0.001).
Some studies 23 24 reported superior results using anatomical fixation technique combined with lateral plasty. Although this technique can potentially provide superior stability, it is certainly more invasive and demanding. Furthermore, anatomical techniques may not be applicable in selected cases of revision surgery (e.g., bone loss of femoral condyle due to wrong placement of previous tunnel or encumbrance due to the presence of previous fixation devices). These reasons are again in support of this less anatomical, less invasive, and less demanding technique. Furthermore, it is important to emphasize that in our study, the best results were obtained on the subjective perception of the patient, which may affect the quality of life.
Several studies reported poor patient-reported outcomes with revision ACL-R compared with primary ACL-R. 22 25 In this study, patients were asked to rate their knee compared with the controlateral, and the average rating was almost 70%. This result is closer to that reported by Andriolo et al 26 in their meta-analysis, with 73% of patients describing their knee as normal or nearly normal.
As most of the patients who suffered failed ACL surgery were young and active subjects, 2 and one of the main indications for surgery was the patient's desire to return to sport, it was important to evaluate the prevalence of return to sports after ACL-R and revision ACL-R. Many studies have described the prevalence of return to sport after ACL-R or revision ACL-R in professional or semiprofessional athletes. 27 Indeed, our study population practiced sports at a lower level. In this study, more than 80% of patients returned to sport with more than 40% returning to the same preinjury level. In very recent studies, Lefevre et al 25 and Anand et al 28 described similar results, with prevalence of return to sport greater than 70% and almost 40% of patients returning to the same preinjury level. These results were also confirmed by a recent meta-analysis, 26 with 75% of patients returning to sport and 43% of them returning to the same preinjury level.
Several factors influence the return to sport, especially after revision surgery. Older age was assumed to be a risk factor for the lower prevalence of return to sport. 29 In this study, the mean patients' age at revision surgery was more compared with the age of primary ACL-R reported in the literature. 30 This fact may influence prevalence of return to sport. Younger patients were more likely to return to the preinjury level of activity compared with older patients. 29
One of the main causes for not returning to sport was the fear of reinjury (kinesiophobia). 31 However, in this study, only 12.5% reported fear of reinjury as the primary cause for not returning to sport, while the most cited cause was the presence of knee symptoms.
In recent years, the psychological and emotional components in returning to sport became considerably important. 32 In this study, the psychological readiness of athletes to return to sport was evaluated using the ACL-RSI scale. Subjects who returned to sports demonstrated better scores than those who did not return to sports ( p = 0.0168). These results were comparable with those in the study by Lefevre et al, 25 where the ACL-RSI score was significantly better in patients who returned to their usual sport at 6 months (54.7 ± 21.1) compared with those who returned after 1 year (49.5 ± 24.8).
No major complications were reported in this study, albeit 21.5% of patients underwent surgical removal of staples. Removal was performed at least 1 year postoperatively, with no effect on final clinical outcome. A total of 4.1% of patients underwent subtotal meniscectomy after revision ACL reconstruction. If we consider the two patients who refused to participate in the study because of unsatisfactory results and persistence of instability, there were four failures in this population, with failure prevalence equal to 14.3%. The cumulative survivorship, calculated using the Kaplan–Meier method was equal to 81.3% at 60 months of follow-up. This result is in line with that reported in the literature, with a failure rate ranging from 24 to 36%. 33 34 Recent studies 35 36 reported lower failure rates, ranging from 1.7 to 7.7%. Lastly, the prevalence of subsequent operations on the same knee in our study is in line with the prevalence referred by a recent meta-analysis, 36 which reported 3.7% of subsequent interventions.
This study had several limitations. First, it was a retrospective study without a control group. Furthermore, the sample size was small and some patients were lost to follow-up. In addition, the study lacked a radiographic evaluation of the operated knees aimed to evaluate the onset of arthritic changes at the last follow-up. In conclusion, the main advantage of the nonanatomical ACL reconstruction using the OTT technique was the absence of femoral tunnels. This made the femoral fixation easier, especially in the case of wide tunnels or wrong placement of the previous tunnel, while the possible loss of strength appeared nonsignificant in this series. According to our data, the results are not inferior to those reported with other techniques, in terms of objective and subjective clinical outcomes, patients' satisfaction, return to sport, and complications and failures.
References
- 1.Spindler K P, Wright R W. Clinical practice. Anterior cruciate ligament tear. N Engl J Med. 2008;359(20):2135–2142. doi: 10.1056/NEJMcp0804745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mall N A, Chalmers P N, Moric M et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42(10):2363–2370. doi: 10.1177/0363546514542796. [DOI] [PubMed] [Google Scholar]
- 3.Wright R W, Dunn W R, Amendola A et al. Risk of tearing the intact anterior cruciate ligament in the contralateral knee and rupturing the anterior cruciate ligament graft during the first 2 years after anterior cruciate ligament reconstruction: a prospective MOON cohort study. Am J Sports Med. 2007;35(07):1131–1134. doi: 10.1177/0363546507301318. [DOI] [PubMed] [Google Scholar]
- 4.Barber-Westin S D, Noyes F R. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy. 2011;27(12):1697–1705. doi: 10.1016/j.arthro.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 5.Irrgang J J, Anderson A F, Boland A L et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med. 2001;29(05):600–613. doi: 10.1177/03635465010290051301. [DOI] [PubMed] [Google Scholar]
- 6.Collins N J, Misra D, Felson D T, Crossley K M, Roos E M. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS) Arthritis Care Res (Hoboken) 2011;63 11:S208–S228. doi: 10.1002/acr.20632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Leys T, Salmon L, Waller A, Linklater J, Pinczewski L. Clinical results and risk factors for reinjury 15 years after anterior cruciate ligament reconstruction: a prospective study of hamstring and patellar tendon grafts. Am J Sports Med. 2012;40(03):595–605. doi: 10.1177/0363546511430375. [DOI] [PubMed] [Google Scholar]
- 8.Kraeutler M J, Bravman J T, McCarty E C. Bone-patellar tendon-bone autograft versus allograft in outcomes of anterior cruciate ligament reconstruction: a meta-analysis of 5182 patients. Am J Sports Med. 2013;41(10):2439–2448. doi: 10.1177/0363546513484127. [DOI] [PubMed] [Google Scholar]
- 9.Grossman M G, ElAttrache N S, Shields C L, Glousman R E. Revision anterior cruciate ligament reconstruction: three- to nine-year follow-up. Arthroscopy. 2005;21(04):418–423. doi: 10.1016/j.arthro.2004.12.009. [DOI] [PubMed] [Google Scholar]
- 10.Wiggins A J, Grandhi R K, Schneider D K, Stanfield D, Webster K E, Myer G D. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2016;44(07):1861–1876. doi: 10.1177/0363546515621554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marcacci M, Zaffagnini S, Marcheggiani Muccioli G M et al. Arthroscopic intra- and extra-articular anterior cruciate ligament reconstruction with gracilis and semitendinosus tendons: a review. Curr Rev Musculoskelet Med. 2011;4(02):73–77. doi: 10.1007/s12178-011-9075-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Marcacci M, Zaffagnini S, Iacono F, Neri M P, Loreti I, Petitto A. Arthroscopic intra- and extra-articular anterior cruciate ligament reconstruction with gracilis and semitendinosus tendons. Knee Surg Sports Traumatol Arthrosc. 1998;6(02):68–75. doi: 10.1007/s001670050075. [DOI] [PubMed] [Google Scholar]
- 13.Golish S R, Baumfeld J A, Schoderbek R J, Miller M D. The effect of femoral tunnel starting position on tunnel length in anterior cruciate ligament reconstruction: a cadaveric study. Arthroscopy. 2007;23(11):1187–1192. doi: 10.1016/j.arthro.2007.06.013. [DOI] [PubMed] [Google Scholar]
- 14.Yiannakopoulos C K, Fules P J, Korres D S, Mowbray M AS. Revision anterior cruciate ligament surgery using the over-the-top femoral route. Arthroscopy. 2005;21(02):243–247. doi: 10.1016/j.arthro.2004.09.026. [DOI] [PubMed] [Google Scholar]
- 15.Xergia S A, Pappas E, Georgoulis A D. Association of the single-limb hop test with isokinetic, kinematic, and kinetic asymmetries in patients after anterior cruciate ligament reconstruction. Sports Health. 2015;7(03):217–223. doi: 10.1177/1941738114529532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Coats A C, Johnson D L. Two-stage revision anterior cruciate ligament reconstruction: indications, review, and technique demonstration. Orthopedics. 2012;35(11):958–960. doi: 10.3928/01477447-20121023-08. [DOI] [PubMed] [Google Scholar]
- 17.Marcacci M, Zaffagnini S, Giordano G, Iacono F, Presti M L. Anterior cruciate ligament reconstruction associated with extra-articular tenodesis: a prospective clinical and radiographic evaluation with 10- to 13-year follow-up. Am J Sports Med. 2009;37(04):707–714. doi: 10.1177/0363546508328114. [DOI] [PubMed] [Google Scholar]
- 18.Buda R, Ruffilli A, Di Caprio F et al. Allograft salvage procedure in multiple-revision anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(02):402–410. doi: 10.1177/0363546512471025. [DOI] [PubMed] [Google Scholar]
- 19.Ahn J H, Lee Y S, Ha H C. Comparison of revision surgery with primary anterior cruciate ligament reconstruction and outcome of revision surgery between different graft materials. Am J Sports Med. 2008;36(10):1889–1895. doi: 10.1177/0363546508317124. [DOI] [PubMed] [Google Scholar]
- 20.Wegrzyn J, Chouteau J, Philippot R, Fessy M H, Moyen B. Repeat revision of anterior cruciate ligament reconstruction: a retrospective review of management and outcome of 10 patients with an average 3-year follow-up. Am J Sports Med. 2009;37(04):776–785. doi: 10.1177/0363546508330141. [DOI] [PubMed] [Google Scholar]
- 21.Salmon L J, Pinczewski L A, Russell V J, Refshauge K. Revision anterior cruciate ligament reconstruction with hamstring tendon autograft: 5- to 9-year follow-up. Am J Sports Med. 2006;34(10):1604–1614. doi: 10.1177/0363546506288015. [DOI] [PubMed] [Google Scholar]
- 22.Griffith T B, Allen B J, Levy B A, Stuart M J, Dahm D L. Outcomes of repeat revision anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(06):1296–1301. doi: 10.1177/0363546513482568. [DOI] [PubMed] [Google Scholar]
- 23.Guzzini M, Mazza D, Fabbri M et al. Extra-articular tenodesis combined with an anterior cruciate ligament reconstruction in acute anterior cruciate ligament tear in elite female football players. Int Orthop. 2016;40(10):2091–2096. doi: 10.1007/s00264-016-3261-9. [DOI] [PubMed] [Google Scholar]
- 24.Ferretti A, Monaco E, Ponzo A et al. Combined intra-articular and extra-articular reconstruction in anterior cruciate ligament-deficient knee: 25 years later. Arthroscopy. 2016;32(10):2039–2047. doi: 10.1016/j.arthro.2016.02.006. [DOI] [PubMed] [Google Scholar]
- 25.Lefevre N, Klouche S, Mirous G, Herman S, Gerometta A, Bohu Y. Return to sport after primary and revision anterior cruciate ligament reconstruction: a prospective comparative study of 552 patients from the FAST cohort. Am J Sports Med. 2017;45(01):34–41. doi: 10.1177/0363546516660075. [DOI] [PubMed] [Google Scholar]
- 26.Andriolo L, Filardo G, Kon E et al. Revision anterior cruciate ligament reconstruction: clinical outcome and evidence for return to sport. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):2825–2845. doi: 10.1007/s00167-015-3702-9. [DOI] [PubMed] [Google Scholar]
- 27.Paterno M V, Rauh M J, Schmitt L C, Ford K R, Hewett T E. Incidence of second ACL injuries 2 years after primary acl reconstruction and return to sport. Am J Sports Med. 2014;42(07):1567–1573. doi: 10.1177/0363546514530088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Anand B S, Feller J A, Richmond A K, Webster K E. Return-to-sport outcomes after revision anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2016;44(03):580–584. doi: 10.1177/0363546515618381. [DOI] [PubMed] [Google Scholar]
- 29.Shelbourne K D, Benner R W, Gray T. Return to sports and subsequent injury rates after revision anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2014;42(06):1395–1400. doi: 10.1177/0363546514524921. [DOI] [PubMed] [Google Scholar]
- 30.Kvist J, Kartus J, Karlsson J, Forssblad M. Results from the Swedish national anterior cruciate ligament register. Arthroscopy. 2014;30(07):803–810. doi: 10.1016/j.arthro.2014.02.036. [DOI] [PubMed] [Google Scholar]
- 31.Cozzi A L, Dunn K L, Harding J L, Valovich McLeod T C, Welch Bacon C E. Kinesiophobia after anterior cruciate ligament reconstruction in physically active individuals. J Sport Rehabil. 2015;24(04):434–439. doi: 10.1123/jsr.2014-0196. [DOI] [PubMed] [Google Scholar]
- 32.Christino M A, Fantry A J, Vopat B G. Psychological aspects of recovery following anterior cruciate ligament reconstruction. J Am Acad Orthop Surg. 2015;23(08):501–509. doi: 10.5435/JAAOS-D-14-00173. [DOI] [PubMed] [Google Scholar]
- 33.Safran M R, Harner C D. Technical considerations of revision anterior cruciate ligament surgery. Clin Orthop Relat Res. 1996;(325):50–64. doi: 10.1097/00003086-199604000-00007. [DOI] [PubMed] [Google Scholar]
- 34.Noyes F R, Barber-Westin S D. Revision anterior cruciate surgery with use of bone-patellar tendon-bone autogenous grafts. J Bone Joint Surg Am. 2001;83-A(08):1131–1143. doi: 10.2106/00004623-200108000-00001. [DOI] [PubMed] [Google Scholar]
- 35.Hettrich C M, Dunn W R, Reinke E K, Spindler K P; MOON Group.The rate of subsequent surgery and predictors after anterior cruciate ligament reconstruction: two- and 6-year follow-up results from a multicenter cohort Am J Sports Med 201341071534–1540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Maletis G B, Inacio M CS, Funahashi T T. Analysis of 16,192 anterior cruciate ligament reconstructions from a community-based registry. Am J Sports Med. 2013;41(09):2090–2098. doi: 10.1177/0363546513493589. [DOI] [PubMed] [Google Scholar]