

Abstract
Although a growing body of research has examined Purging Disorder (PD), there remains a lack of conclusive evidence regarding the diagnostic validity of PD. This meta-analysis compared PD to DSM–5 eating disorders (i.e., Anorexia Nervosa [AN], Bulimia Nervosa [BN], and Binge Eating Disorder [BED]) and controls. A comprehensive literature search identified 38 eligible studies. Group differences on indicators of course of illness and both general and eating psychopathology were assessed using standardized effect sizes. Results supported the conceptualization of PD as a clinically significant eating disorder, but findings were less clear regarding its distinctiveness from other eating disorder diagnoses. More specifically, PD significantly differed from BN and BED in natural course of illness (g = .40–.54), and PD significantly differed from AN in treatment outcome (g = .27), with PD characterized by a better prognosis. Overall, PD was more similar to AN and BED on many dimensional measures of general and eating-related psychopathology, though PD was less severe than BN in most of these domains. PD, BN, and BED groups also evidenced similar frequencies of subjective binge episodes (SBEs), yet PD evidenced less frequent SBEs than AN. There is a clear need for future studies of PD to assess validators that have not been reported comprehensively in the literature, such as mortality, medical morbidity, and course of illness. Additionally, empirical classification studies are needed to inform future classifications of PD, particularly with regard to categorical differences between PD and other eating disorders.
Keywords: eating disorders, eating disorder not otherwise specified, meta-analysis, other specified feeding or eating disorder, purging disorder
With the publication of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–5; (American Psychiatric Association, 2013), there have been changes to the diagnostic criteria for Anorexia Nervosa (AN), Bulimia Nervosa (BN), and Binge Eating Disorder (BED), in part to address the concerning finding that most individuals presenting for eating disorder (ED) treatment did not meet diagnostic criteria for one of the primary EDs in the DSM–IV (American Psychiatric Association, 2000; Fairburn & Bohn, 2005). Previously such individuals would have received a diagnosis of Eating Disorder Not Otherwise Specified (EDNOS), whereas the DSM–5 includes the categories of Other Specified Feeding or Eating Disorder (OSFED) and Unspecified Feeding and Eating Disorder (UFED) to account for individuals with clinically significant ED symptoms who do not meet criteria for a full-threshold ED. OSFED in particular identifies a number of specific ED symptom constellations, several of which are consistent with primary DSM–5 EDs, with certain exceptions such as limited duration (e.g., symptoms occurring for less than three months), low frequency (e.g., binge eating or purging occurring less than once per week), or atypical presentation (e.g., AN symptoms with significant weight loss, but current weight in the normal range).
One notable change to the DSM–5 was the inclusion of Purging Disorder (PD) as one specified type within OSFED. PD is characterized by recurrent purging behavior (i.e., self-induced vomiting, laxative, and/or diuretic abuse) to influence shape or weight in the absence of objective binge eating episodes (OBEs; i.e., eating an unusually large amount of food and experiencing a concurrent sense of loss of control; Keel, Haedt, & Edler, 2005). Purging behavior is a particularly concerning clinical phenomenon in EDs, as it is associated with medical problems across body systems, including metabolic disturbances, electrolyte imbalances, edema, dental problems, esophageal tears and oral bleeding, swollen salivary glands, and musculoskeletal and gastrointestinal problems (Fairburn, 1985; Keel, 2005). Although earlier research documented symptoms consistent with PD among individuals with eating psychopathology (Mitchell, Pyle, Hatsukami, & Eckert, 1986), only since its formal introduction by Keel and colleagues (Keel, Mayer, & Harnden-Fischer, 2001; Keel et al., 2005) has the syndrome been the subject of more focused empirical research. The point prevalence of PD varies depending on the definition used (Crowther, Armey, Luce, Dalton, & Leahey, 2008; Haedt & Keel, 2010), though lifetime prevalence estimates have ranged from 1.1% (Favaro, Ferrara, & Santonastaso, 2003) to 5.3% (Wade, Bergin, Tiggemann, Bulik, & Fairburn, 2006).
To date, existing findings have generally supported the clinical significance of PD. For instance, compared with individuals without PD, those with PD exhibit higher levels of general psychopathology, distress, eating pathology, and personality disorders (Keel, Wolfe, Gravener, & Jimerson, 2008; Keel et al., 2005). However, research has yielded mixed findings regarding how PD compares to other EDs, particularly BN. For example, some studies have demonstrated that women with PD do not significantly differ from those with BN on measures of symptom severity, impairment, body dissatisfaction, or dietary restraint (Binford & Le Grange, 2005; Keel, Mayer, & Harnden-Fischer, 2001; Keel et al., 2005). In contrast, other literature suggests that, compared with individuals with PD, individuals with BN generally report greater eating psychopathology (Binford & Le Grange, 2005), lower self-esteem (Binford & Le Grange, 2005), and higher levels of general psychopathology, including mood disorders (Keel et al., 2008; Keel et al., 2005) and anxiety (Fink, Smith, Gordon, Holm-Denoma, & Joiner, 2009). Regarding mortality, one study reported the crude mortality ratio of PD (5.0%) to be higher than both those of BN and AN purging subtypes, and the standard mortality ratio of 3.90 (95% confidence interval: 2.05, 7.21) suggested the elevated mortality risk in PD (compared with the general population) was not attributable to chance; however, it is unclear if this is a consistent finding in PD (Koch, Quadflieg, & Fitchter, 2013, 2014).1 Further, empirical classification studies have yielded mixed findings regarding the distinctiveness of PD, with some identifying a latent class resembling PD (Striegel-Moore et al., 2005; Sullivan, Bulik, & Kendler, 1998), and others not consistently supporting this finding (Bulik, Sullivan, & Kendler, 2000; Keel et al., 2004; Wade, Crosby, & Martin, 2006). Notably, there remains a dearth of information on the course, outcome, or treatment response of PD (Keel & Striegel-Moore, 2009), as well as limited data regarding medcal morbidity in PD and the degree to which purging behavior may indirectly contribute to mortality in EDs (Forney, Haedt-Matt, & Keel, 2014; Keel et al., 2008).
To date, only one meta-analysis (Thomas, Vartanian, & Brownell, 2009) has systematically compared EDNOS (now OSFED) to other ED diagnoses. Previous literature characterized EDNOS as comprising relatively heterogeneous subgroups, with the proportion of EDNOS cases resembling PD ranging from 11% (Eddy, Doyle, Hoste, Herzog, & Le Grange, 2008) to 43% (Binford & Le Grange, 2005). However, there were few studies specifying PD as an EDNOS subtype in Thomas et al.’s (2009) analyses (k = 5), and comparisons were only made between PD and BN on a limited number of outcomes. Although nosological changes reflected in the DSM–5 may have addressed some of the diagnostic issues raised by Thomas et al.’s (2009) analyses (e.g., by reducing the frequency criterion for BN and including PD as an OSFED type), the extent to which PD represents a substantial proportion of those with clinically significant ED psychopathology remains unclear and thus warrants further investigation.
Current Conceptualization for Evaluating the Validity of PD
Taken together, the mixed nature of the aforementioned evidence raises a broader issue of the diagnostic validity of PD, particularly with regard to distinctiveness from other EDs. As such, to inform future classification systems and provide a conceptualization that has clinical utility, the present investigation sought to evaluate the clinical significance and diagnostic validity of PD using a hierarchical approach and meta-analytic methodology. First, we aimed to assess the clinical significance of PD by comparing PD samples with non-ED samples on general measures of severity (i.e., mortality, medical and psychiatric morbidity, impairment, quality of life,). Second, we sought to examine the validity of categorizing PD as an ED by comparing PD to non-ED samples on measures of body dissatisfaction, restraint, and eating psychopathology. Third, we evaluated the validity of PD as a distinct ED diagnosis by making comparisons between PD and established DSM–5 diagnoses (i.e., AN, BN, BED) on measures of general and ED-related psychopathology.
The latter comparisons (i.e., between PD and other EDs) included multiple levels of evaluation. In the absence of alternative analytic approaches (e.g., taxometric or factor mixture analyses), the presence of purging and the lack of OBEs inherent in the definition of PD limits the degree to which the validity of these characteristics can be assessed as meaningful boundaries with other EDs that are defined by different symptom topographies (i.e., AN which is associated with low weight; AN-restricting type [AN-r], which is not associated with recurrent OBEs; BN, which is associated with recurrent OBEs; and BED, which is associated with recurrent OBEs without regular purging or other compensatory behavior). However, comparing PD with other EDs on indicators of concurrent and predictive validity may provide empirical evidence to inform future classification systems2 (Kendell, 1989). Moreover, there is evidence to suggest that EDs are more accurately categorized based upon both qualitative differences and the degree of underlying severity (Keel, Crosby, Hildebrandt, Haedt-Matt, & Gravener, 2013).
Thus, when evaluating the validity of a diagnostic category such as PD it is important to consider both categorical differences in symptom topography and dimensional differences in severity. With the understanding that there are some qualitative differences in the topography of symptoms between PD and other EDs, we aimed to compare PD with other EDs on dimensions of severity and theoretically salient constructs to assess whether (a) PD evidences distinct course of illness compared with other EDs (i.e., predictive validity); and (b) if the level of general psychopathology and ED-related psychopathology in PD is similar to or different from full-threshold DSM–5 EDs (i.e., concurrent validity).
Predictive validity was evaluated by comparing PD with other EDs on variables related to course of illness, including mortality, age of onset, duration of illness, natural course outcome, treatment outcome, and treatment history. Consistent group differences in predictive validity would suggest that individuals PD exhibit a different trajectory of illness compared with other EDs, which may support distinctions between PD and other EDs in classification systems.
Concurrent validity was assessed by clinical features that were both non-ED and ED-related. Consistent with previous research (Keel et al., 2013), we used non-ED indicators (i.e., medical and psychiatric morbidity, general psychopathology, suicidality, impairment, quality of life) to compare groups along a continuum of severity that may underlie all EDs but differ in degree. Indicators of psychiatric morbidity and general psychopathology included depression, anxiety, substance use, impulsivity, perfectionism, and self-esteem. Similarly, we compared PD with other EDs on dimensional measures of ED-related psychopathology (i.e., restraint, body dissatisfaction, eating psychopathology, SBE and purging frequencies) to inform how PD compares to other groups in ED symptomatology. Similarities in general and ED-related validators would suggest PD is comparable with full-threshold diagnoses in overall severity, whereas differences may indicate PD represents a distinct syndrome differing in severity.
Method
Study Selection
To obtain a comprehensive list of studies for inclusion in this meta-analysis, a literature search was conducted using the Psy-cINFO, PubMed, Medline, and CINAHL electronic databases. To identify potential studies, the search parameters “purging disorder,” “subjective bulimia nervosa,” “compensatory eating disorder,” or “EDNOS-P” were entered adjacent to the terms “anorexi*”3 or “bulimi,*” “binge eating disorder,” or “controls” to capture the full range of terminology used to refer to AN, BN, BED, PD, and controls. To avoid potential publication biases, the Dissertation Abstracts International electronic database was also included in the search.
The resulting list of articles was separately cross-referenced with the following search parameters: “mortality,” “morbidity,” “comorbid*,” “psychiatric,” “medical,” “suicid*,” psychopathology,” “impairment,” “quality of life,” “symptom,*” “body dissatisfaction” or “body satisfaction,” “depression,” “anxiety,” “self-esteem,” “impuls*,” “perfectionism,” “treatment,” “history,” “outcome,” “course,” “age of onset,” “duration,” and “eating psychopathology” (or “eating disturbance”). References of the identified studies were searched to further identify studies for inclusion.
Eligibility Criteria
The following inclusion criteria were applied:
Only empirical studies were included so as to allow for the calculation of the standardized mean difference (i.e., effect size) of dependent variables among the subgroups.
Only studies that compared AN, BN, BED, or non-ED control groups with PD on the dependent variables of interest were included. Comparison groups (AN, BN, BED) that included subclinical forms were not included given that the present study aimed to examine PD in relation to full-threshold EDs as defined in DSM–5 (American Psychiatric Association, 2013).
Only studies written in English were included, although the country in which the data were collected was not restricted.
We contacted all authors to inquire about possible additional data that were not reported in the manuscript, when there was insufficient data to calculate necessary effect sizes, and when studies appeared to have overlapping samples; we also inquired about possible additional data that was not reported in the manuscript. Six authors provided additional data, some of which were not reported in publications. Six studies (Brown, Haedt-Matt, & Keel, 2011; Edler, Haedt, & Keel, 2007; Keel, Wolfe, Liddle, De Young, & Jimerson, 2007; Keel, Holm-Denoma, & Crosby, 2011; Stice, Marti, Shaw, & Jaconis, 2009; Wade, Fairweather-Schmidt, Zhu, & Martin, 2015) were excluded because they used the same sample as other studies that were identified (Keel et al., 2008; Keel et al., 2005; Stice, Marti, & Rohde, 2013; Wade, Bergin, Tiggemann, Bulik, & Fairburn, 2006; Wade, 2007). Thus, 38 studies were identified for inclusion, one of which was an unpublished dissertation. Figure 1 depicts a flow diagram of the study selection process.
Figure 1.
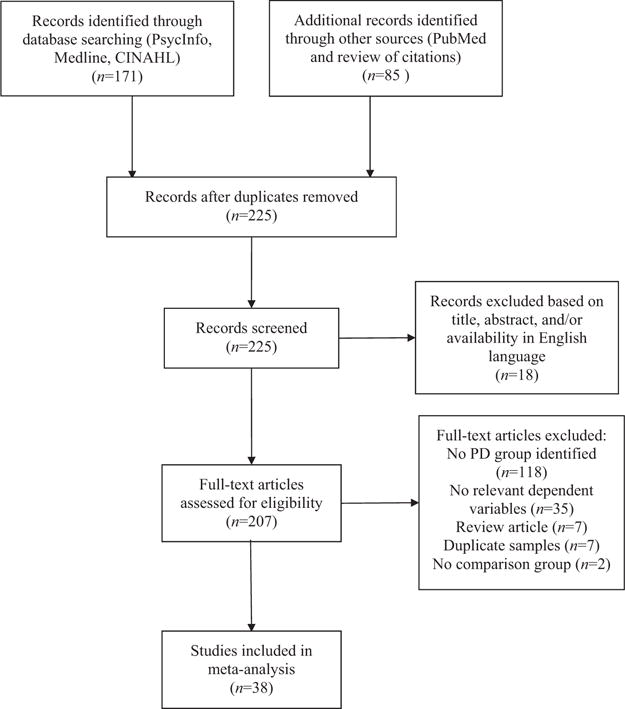
PRISMA flow diagram of study selection.
Data Collection
A coding form was developed to extract descriptive and quantitative information from each study (e.g., means, standard deviations, and subsample sizes; means, and exact/categorical p values; (Lipsey & Wilson, 2001). Table 1 describes all coded comparisons, dependent variables, and moderators.
Table 1.
Summary of Comparisons, Dependent Variables, and Moderators Coded
| Comparison groups | Dependent variables | Moderators | Moderator levels coded |
|---|---|---|---|
| Purging Disorder (PD) Bulimia Nervosa (BN) Anorexia Nervosa (AN) Binge Eating Disorder (BED) Non-eating disorder controls |
Mortality (Standard or crude mortality rate) Medical morbidity (% with co-occurring medical diagnosis) Quality of life (dimensional measure) Functional impairment (dimensional measure) Suicidality (% with lifetime attempt or current ideation, or degree of ideation) Age of onset (years) Duration of illness (months) Natural course of illness (% remitted) Treatment outcome (% remitted) Treatment history (Number of episodes of care, duration of treatment) Depression (dimensional measure or % with mood disorder diagnosis) Anxiety (dimensional measure or % with anxiety disorder diagnosis) Substance use (dimensional measure or % with substance use disorder diagnosis) Impulsivity (dimensional measure or % with impulse control disorder diagnosis) Perfectionism (dimensional measure) Self-esteem (dimensional measure) Eating psychopathology (dimensional measure) Dietary restraint (dimensional measure) Body dissatisfaction (dimensional measure) Subjective binge frequency (weekly) Purging frequency (weekly) |
Type of purging specified for PD diagnosis | Exclusively purging behavior (i.e., self-induced vomiting, laxatives, and/or diuretic abuse) was required for PD diagnosis Not exclusively purging behavior (i.e., non-purging compensatory behaviors such as exercise or fasting were included in PD diagnosis or was unspecified) |
|
| |||
| Purging frequency criterion for PD diagnosis | At least once weekly At least twice weekly Not specified |
||
|
| |||
| Inclusion of over-evaluation of shape and weight in PD diagnosis | Described Not described |
||
|
| |||
| Inclusion of subjective binge episodes in PD diagnosis | Allowed Excluded Not specified |
||
|
| |||
| Subtype of Anorexia Nervosa (AN) | Restricting subtype (AN-r) Binge-purge subtype (AN-bp) Mixed/Not specified |
||
|
| |||
| Sample demographic | Non-treatment sample General psychiatric outpatient Specialized eating disorder treatment center Mixed Not specified |
||
|
| |||
| Sample age group | Adolescent/child (age 18 and under) Adult (including college/university samples) Mixed ages Not specified |
||
|
| |||
| Method of eating disorder diagnosis | Self-report Structured interview/clinician ratings |
||
The first author screened, identified, and coded all studies, and the second author recoded all published studies. Acceptable agreement was found between the two coders on categorical variables (κ = .90), and the percent exact agreement on quantitative variables was 95.3%. Coders resolved disagreements by discussion. To compare group means on dependent variables, effect sizes were calculated as standardized mean differences, Hedge’s g, which is appropriate for use with small sample sizes (Hedges, 1981). The values of g were interpreted such that magnitudes of 0.2, 0.5, and 0.8 represented small, medium, and large effects, respectively (Hedges, 1981).
Because meta-analysis requires independence for each study in analyses, each study could only contribute one effect size per comparison (Lipsey & Wilson, 2001). Thus, to adjust for dependencies among effect sizes, when studies reported data on multiple measures of the same construct (e.g., two measures of body dissatisfaction), the measures were averaged to create a composite measure that was used in effect size calculations.
Statistical Analyses
To determine the values and significance of mean effect sizes for each comparison, a random effects model was applied. A random effects model assumes that the variability is attributable to both within-study sampling error as well as random, between-study variance, that is,τ2 (Hedges & Pigott, 2004; Lipsey & Wilson, 2001). The random effects model is often preferred because it takes into account possible variations in study procedures and settings, and the resulting findings are considered to be more generalizable (Lipsey & Wilson, 2001; Rosenthal, 1995). However, for comparisons consisting of five or fewer studies, a fixed effect model was applied (Borenstein, personal communication during workshop, 2013). To balance the importance of reaching conclusions with the issues of statistical power (Valentine, Pigott, & Rothstein, 2010), only comparisons that were comprised of at least three effect sizes were interpreted, though all comparisons were coded and reported in tables.
The present study used both the Q statistic and the I2 statistic to assess the heterogeneity of effect size distributions. The Q statistic has poor power to detect true heterogeneity when the meta-analysis includes a small number of studies, whereas the I2 statistic is not dependent on the number of studies in the meta-analysis (Higgins & Thompson, 2002). While the Q statistic assesses the statistical significance of heterogeneity, the I2 statistic indicates the proportion of total variability in a set of effect sizes that is attributable to true between-study differences (Huedo-Medina, Sánchez-Meca, Marín-Martínez, & Botella, 2006). It has been suggested that the I2 statistic be interpreted such that percentages of 25, 50, and 75 represent low, medium, and high degrees of between-study variability, respectively. Furthermore, Fu and colleagues (2011) have advised requiring a minimum of four studies at each level to pursue analyses with categorical moderators.
Therefore, if the Q and I2 statistics together suggested substantial heterogeneity in the observed effect size distribution (as indicated by a significant Q value and I2 statistic ≥75%), and there were at least four studies at each moderator level for which there was available data, follow-up moderator analyses were conducted to model between-study variance. That is, moderation analyses assessed whether categorical study descriptors accounted for a statistically significant proportion of the effect size variability (Lipsey & Wilson, 2001). In the moderator analyses, the difference between effect sizes across different levels of the moderator was assessed by computing the between-groups homogeneity statistic, QB. Comprehensive Meta-Analysis Version 3.0 (Borenstein, Hedges, Higgins, & Rothstein, 2014) and SPSS version 24.0 were used to conduct statistical analyses.
Publication Bias
To minimize publication bias (i.e., the file drawer problem) we included both published articles and unpublished dissertations in our search process. After completing analyses, the presence of publication bias was assessed to determine whether it was likely that the publication of only significant results accounted for the observed effects. This was done by calculating the fail-safe N, which is the number of studies with a g of 0 that would bring the overall effect size to a nonsignificant level (Rosenthal, 1979).
Results
The 38 studies ranged in year of publication from 1997 to 2016. Sample sizes ranged from 56 to 13,035 (Md = 433.50, M = 1,147.89, SD = 2,171.21). On average, participants were 23.50 years old (SD = 7.03) and had a BMI of 24.54 (SD = 4.58). Samples were predominately female (M = 95.6% female, SD = 9.51), and mostly Caucasian (M = 74.17% Caucasian, SD = 14.95). Table 2 summarizes descriptive information and coded moderators. Table 3 displays overall effect sizes, heterogeneity statistics, and fail-safe Ns; Table 4 summarizes significant moderation analyses; and Table 5 contains individual effect sizes for each study.
Table 2.
Summary of Studies and Coded Moderators
| Study name | Method of diagnosis | Sample demographic | Age group | Participant sex | N | Age
|
BMI
|
AN subtype | PD diagnostic criteria
|
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Type of purging behavior | Purging frequency criterion | Body image disturbance | SBEs included | |||||||
| Allen, Byrne, Oddy, and Crosby (2013a) | Self-report | Non-treatment | Adolescent | Male and female | 1,383 | 14.01 | .19 | n.s. | Purging | ≥1×/wk | Described | n.s. | ||
| Allen, Byrne, Oddy, and Crosby (2013b) | Self-report | Non-treatment | Adolescent | Male and female | 1,383 | 14.01 | .19 | n.s. | Purging | ≥1×/wk | Described | n.s. | ||
| Binford and Le Grange (2005) | Structured interview | Specialized ED treatment | Adolescent | Male and female | 56 | 16.55 | 1.36 | Purging | ≥1×/wk | Described | n.s. | |||
| Darcy et al. (2015) | Structured interview | Specialized ED treatment | Adolescent | Female only | 114 | Not exclusive to purging | n.s. | Described | n.s. | |||||
| Davis, Holland, and Keel (2014) | Structured interview | Non-treatment | Adult | Female only | 60 | 21.12 | 5.15 | 21.82 | 2.20 | Not exclusive to purging | ≥2×/wk | Described | Allowed | |
| Eddy, Doyle, Hoste, Herzog, and Le Grange (2008) | Structured interview | Specialized ED treatment | Adolescent | Male and female | 281 | 16.00 | 2.00 | Purging | ≥2×/wk | n.s. | Allowed | |||
| Ekeroth, Clinton, Norring, and Birgegard (2013) | Structured interview | Specialized ED treatment | Adult | Female only | 2,233 | 25.70 | 7.84 | Both | Purging | n.s. | Described | Allowed | ||
| Favaro, Ferrara, and Santonastaso (2003) | Structured interview | Non-treatment | Adult | Female only | 934 | 20.9 | 2.60 | n.s. | Purging | ≥2×/wk | Described | n.s. | ||
| Fink, Smith, Gordon, Holm-Denoma, and Joiner (2009) | Structured interview | Non-treatment | Adult | Female only | 294 | 18.87 | 2.58 | n.s. | Purging | ≥2×/wk | n.s. | n.s. | ||
| Flament et al. (2015) | Self-report | Non-treatment | Adolescent | Male and female | 3,043 | 14.19 | 1.61 | n.s. | Purging | ≥1×/wk | Described | n.s. | ||
| García, Planell, Estragués, i Escursell, and Carracedo (2010) | Structured interview | Specialized ED treatment | Mixed | Female only | 73 | Not exclusive to purging | n.s. | n.s. | n.s. | |||||
| Goldschmidt et al. (2016) | Structured interview | Specialized ED treatment | Adolescent | Male and female | 245 | 16.20 | 1.50 | AN-bp | Purging | ≥1×/wk | Described | Allowed | ||
| Haedt and Keel (2010) | Self-report | Non-treatment | Adult | Male and female | 2,491 | 20.00 | 1.70 | 22.07 | 2.90 | Purging | ≥1×/wk | Described | Excluded | |
| Helverskov et al. (2011) | Structured interview | Specialized ED treatment | Mixed | Male and female | 965 | 22.00 | 6.20 | n.s. | Not exclusive to purging | n.s. | Described | n.s. | ||
| Keel, Haedt, and Edler (2005) | Structured interview | Non-treatment | Adult | Female only | 111 | 25.10 | 6.00 | 21.70 | 1.60 | Purging | ≥2×/wk | Described | Allowed | |
| Keel, Mayer, and Harnden-Fischer (2001) | Structured interview | Non-treatment | Mixed | Female only | 54 | Purging | ≥2×/wk. | Described | Allowed | |||||
| Keel, Wolfe, Gravener, and Jimerson (2008) | Structured interview | Non-treatment | Adult | Female only | 119 | Purging | ≥2×/wk | Described | Allowed | |||||
| Knoph et al. (2013) | Self-report | Non-treatment | Adult | Female only | 3,534 | 30.00 | 4.70 | n.s. | Not exclusive to purging | ≥1×/wk | n.s. | n.s. | ||
| Koch, Quadflieg, and Fichter (2013) | Self-report | Specialized ED treatment | Adult | Male and female | 1,484 | AN-bp | Purging | ≥1×/wk | Described | n.s. | ||||
| Le Grange et al. (2006) | Structured interview | Mixed | Adult | Female only | 204 | 25.70 | 8.90 | Not exclusive to purging | n.s. | n.s. | Allowed | |||
| MacDonald, Trottier, McFarlane, and Olmsted (2015) | Structured interview | Specialized ED treatment | Adolescent | Male and female | 158 | 27.10 | 8.80 | 23.20 | 4.40 | Not exclusive to purging | ≥1×/wk | n.s. | Allowed | |
| Marino (2011) | Structured interview | Specialized ED treatment | Mixed | Male and female | 1,033 | AN-bp | Purging | ≥2×/wk | n.s. | n.s. | ||||
| Metzler-Brody et al. (2011) | Self-report | General psychiatric | Adult | Female only | 158 | 30.20 | 5.90 | n.s. | Not exclusive to purging | n.s. | n.s. | n.s. | ||
| Nakai, Fukushima, Taniguchi, Nin, and Teramukai (2013) | Structured interview | Specialized ED treatment | Mixed | Female only | 1,029 | n.s. | Not exclusive to purging | n.s. | n.s. | n.s. | ||||
| Pisetsky, Thornton, Lichtenstein, Pedersen, and Bulik (2013) | Self-report | Non-treatment | Adult | Female only | 13,035 | Both | Purging | ≥1×/wk | Described | n.s. | ||||
| Roberto, Grilo, Masheb, and White (2010) | Self-report | Non-treatment | n.s. | Female only | 234 | 34.10 | 10.20 | Not exclusive to purging | ≥1×/wk | n.s. | n.s. | |||
| Roberto, Haynos, Schwartz, Brownell, and White (2013) | Self-report | Non-treatment | Adult | Male and female | 371 | 33.20 | 12.10 | 28.82 | 8.97 | Purging | ≥1×/wk | n.s. | n.s. | |
| Rockert, Kaplan, and Olmsted (2007) | Structured interview | Specialized ED treatment | Mixed | Male and female | 1,449 | 28.49 | 8.90 | Both | Purging | ≥1×/wk | n.s. | n.s. | ||
| Smith and Crowther (2013) | Self-report | Non-treatment | Adult | Female only | 94 | 19.77 | 4.22 | 23.70 | 4.98 | Purging | ≥1×/wk | Described | Allowed | |
| Solmi, Hotopf, Hatch, Treasure, and Micali (2016) | Structured interview | Non-treatment | Mixed | Male and female | 145 | Purging | ≥2×/wk | n.s. | n.s. | |||||
| Stice, Marti, and Rohde (2013) | Structured interview | Non-treatment | Adolescent | Female only | 496 | 13.00 | n.s. | Purging | ≥1×/wk | Described | n.s. | |||
| Støving et al. (2012) | Structured interview | Specialized ED treatment | Mixed | Female only | 605 | n.s. | Purging | ≥1×/wk | n.s. | n.s. | ||||
| Tasca et al. (2012) | Structured interview | Specialized ED treatment | Adult | Female only | 1,831 | Both | Purging | ≥1×/wk | Described | n.s. | ||||
| Tobin, Griffing, and Griffing (1997) | Structured interview | Specialized ED treatment | Mixed | Male and female | 267 | AN-bp | Not exclusive to | ≥2×/wk | n.s. | n.s. | ||||
| Wade (2007) | Structured interview | Non-treatment | Mixed | Female only | 759 | 35.00 | 2.11 | Purging | ≥2×/wk | n.s. | Allowed | |||
| Wade, Bergin, Tiggemann, Bulik, and Fairburn (2006) | Structured interview | Non-treatment | Adult | Female only | 1,002 | 34.97 | 2.11 | Both | Purging | ≥2×/wk | n.s. | Allowed | ||
| Watson et al. (2013) | Self-report | Non-treatment | Adult | Female only | 1,876 | 29.90 | 4.60 | Purging | ≥1×/wk | n.s. | n.s. | |||
| Wolfe, Jimerson, Smith, and Keel (2011) | Structured interview | Non-treatment | Adult | Female only | 72 | Purging | ≥2×/wk | n.s. | n.s. | |||||
Note. ED = eating disorder; BMI = Body Mass Index; AN = Anorexia Nervosa; AN-r = AN restricting subtype; AN-bp = AN binge-purge subtype; Both = both AN-r and AN-bp subtypes included. n.s. = Not specified. Purging behavior was defined as self-induced vomiting, laxative, and/or diuretic use; non-purging behavior included other compensatory behaviors (i.e., exercise and fasting). Empty cells indicate values were not specified by the study.
Table 3.
Summary of Overall Effect Sizes, Heterogeneity Statistics, and Fail-Safe N for Comparisons of PD With AN, BN, BED, and Control Groups
| Comparison | Dependent variable | Studies (n) |
g | SE | p | Heterogeneity
|
Fail-safe N | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Q | df | p | I2 | |||||||
| PD vs. Control | Mortality | 0 | — | — | — | — | — | — | — | — |
| Medical morbidity | 1 | .68 | .46 | .142 | — | — | — | — | — | |
| Suicidality | 6 | 1.94 | .99 | .050 | 433.59 | 5 | <.001 | 98.85 | 583 | |
| Quality of life | 2 | −.95 | .01 | <.001 | 111.58 | 1 | <.001 | 99.10 | ||
| Functional impairment | 1 | .43 | .25 | .086 | — | — | — | — | — | |
| Depression | 7 | 1.13 | .25 | <.001 | 70.78 | 6 | <.001 | 91.52 | 1,131 | |
| Anxiety | 8 | 1.42 | .37 | <.001 | 60.61 | 7 | <.001 | 88.45 | 192 | |
| Impulsivity | 5 | 1.25 | .12 | <.001 | 12.04 | 4 | <.017 | 66.78 | 102 | |
| Substance use | 5 | .13 | .01 | <.001 | 44.22 | 4 | <.001 | 90.95 | 195 | |
| Body dissatisfaction | 8 | 2.16 | .46 | <.001 | 136.69 | 7 | <.001 | 94.88 | 623 | |
| Dietary restraint | 7 | 1.78 | .44 | <.001 | 130.32 | 6 | <.001 | 95.40 | 439 | |
| Eating psychopathology | 10 | 1.71 | .43 | <.001 | 260.96 | 9 | <.001 | 96.55 | 672 | |
|
| ||||||||||
| PD vs. AN | Mortality | 1 | .17 | .22 | .422 | — | — | — | — | — |
| Medical morbidity | 0 | — | — | — | — | — | — | — | — | |
| Suicidality | 7 | .10 | .12 | .415 | 24.34 | 6 | <.001 | 75.35 | — | |
| Quality of life | 0 | — | — | — | — | — | — | — | — | |
| Functional impairment | 2 | −.29 | .07 | <.001 | .48 | 1 | .488 | <.001 | * | |
| Depression | 9 | .20 | .14 | .162 | 58.39 | 8 | <.001 | 86.30 | — | |
| Anxiety | 5 | .10 | .05 | .054 | 2.00 | 4 | .736 | <.001 | — | |
| Impulsivity | 0 | — | — | — | — | — | — | — | — | |
| Substance use | 4 | .23 | .06 | <.001 | 7.53 | 3 | .057 | 60.18 | 5 | |
| Age of onset (years) | 6 | .44 | .15 | .003 | 21.16 | 5 | .001 | 76.37 | 43 | |
| Duration of illness (months) | 7 | .10 | .07 | .177 | 13.07 | 6 | .042 | 54.08 | — | |
| Natural course (% remitted) | 2 | .10 | .32 | .759 | 1.07 | 1 | .301 | 6.69 | — | |
| Treatment outcome (% remitted) | 4 | .27 | .05 | <.001 | 3.58 | 3 | .311 | 16.18 | 18 | |
| Treatment history | 4 | −.30 | .08 | <.001 | 10.89 | 3 | .012 | 72.45 | 23 | |
| SBE frequency | 3 | −.17 | .06 | .004 | 5.67 | 2 | .059 | 64.74 | * | |
| Purging frequency | 4 | .48 | .06 | <.001 | 11.32 | 3 | .010 | 73.49 | 59 | |
| Self-esteem | 3 | .58 | .12 | <.001 | 62.59 | 2 | <.001 | 96.80 | * | |
| Perfectionism | 3 | −.08 | .08 | .346 | 2.75 | 2 | .253 | 27.34 | — | |
| Eating psychopathology | 9 | −.16 | .27 | .552 | 252.59 | 8 | <.001 | 96.83 | — | |
| Body dissatisfaction | 8 | .14 | .20 | .494 | 121.75 | 7 | <.001 | 94.25 | — | |
| Restraint | 5 | .14 | .06 | .017 | 16.43 | 4 | .002 | 75.65 | 4 | |
|
| ||||||||||
| PD vs. BN | Mortality | 1 | .86 | .26 | .001 | — | — | — | — | * |
| Medical morbidity | 0 | — | — | — | — | — | — | — | — | |
| Suicidality | 9 | −.57 | .34 | .093 | 113.77 | 8 | <.001 | 92.97 | — | |
| Quality of life | 1 | −2.97 | .34 | <.001 | — | — | — | — | — | |
| Functional impairment | 2 | −.22 | .08 | .005 | .00 | 1 | .983 | <.001 | * | |
| Depression | 20 | −.22 | .11 | .042 | 130.51 | 19 | <.001 | 85.44 | 50 | |
| Anxiety | 13 | −.24 | .14 | .087 | 77.91 | 12 | <.001 | 84.60 | — | |
| Impulsivity | 6 | −.51 | .20 | .013 | 16.36 | 5 | .006 | 69.43 | 25 | |
| Substance use | 10 | −.06 | .06 | .339 | 7.77 | 9 | .558 | .00 | — | |
| Age of onset (years) | 9 | .26 | .11 | .012 | 21.53 | 8 | .006 | 62.84 | 25 | |
| Duration of illness (months) | 15 | −.12 | .07 | .103 | 32.55 | 14 | .003 | 56.99 | — | |
| Natural course (% remitted) | 6 | .54 | .14 | <.001 | 5.04 | 5 | .412 | .70 | 10 | |
| Treatment outcome (% remitted) | 5 | −.06 | .06 | .335 | 10.36 | 4 | .035 | 61.40 | — | |
| Treatment history | 6 | −.33 | .18 | .069 | 10.98 | 5 | .05 | 54.44 | — | |
| SBE frequency | 10 | −.27 | .15 | .073 | 45.35 | 9 | <.001 | 80.15 | — | |
| Purging frequency | 12 | −.25 | .08 | .003 | 21.62 | 11 | .027 | 49.12 | 44 | |
| Self-esteem | 8 | .45 | .21 | .036 | 68.70 | 7 | <.001 | 89.81 | 42 | |
| Perfectionism | 8 | −.42 | .21 | .044 | 80.86 | 7 | <.001 | 91.34 | 33 | |
| Eating psychopathology | 25 | −.94 | .21 | <.001 | 763.92 | 24 | <.001 | 96.86 | 3,585 | |
| Body dissatisfaction | 21 | −.33 | .07 | <.001 | 67.86 | 20 | <.001 | 70.53 | 266 | |
| Restraint | 16 | −.15 | .09 | .115 | 45.98 | 15 | <.001 | 67.38 | — | |
|
| ||||||||||
| PD vs. BED | Mortality | 0 | — | — | — | — | — | — | — | — |
| Medical morbidity | 0 | — | — | — | — | — | — | — | — | |
| Suicidality | 5 | .16 | .09 | .085 | 3.69 | 4 | .449 | <.001 | — | |
| Quality of life | 0 | — | — | — | — | — | — | — | — | |
| Functional impairment | 2 | −.19 | .11 | .081 | 1.37 | 1 | .241 | 27.23 | — | |
| Depression | 7 | .02 | .19 | .920 | 24.26 | 6 | <.001 | 75.27 | — | |
| Anxiety | 6 | .10 | .17 | .550 | 9.87 | 5 | .079 | 49.35 | — | |
| Impulsivity | 1 | .28 | .46 | .536 | — | — | — | — | — | |
| Substance use | 4 | .03 | .14 | .827 | 11.33 | 3 | .010 | 73.52 | — | |
| Age of onset (years) | 3 | .05 | .12 | .666 | .97 | 2 | .615 | .00 | — | |
| Duration of illness (months) | 6 | −.45 | .15 | .002 | 8.72 | 5 | .121 | 42.68 | 23 | |
| Natural course (% remitted) | 5 | .40 | .13 | .002 | 7.65 | 4 | .105 | 47.73 | 11 | |
| Treatment outcome (% remitted) | 2 | .26 | .13 | .051 | .95 | 1 | .330 | <.001 | — | |
| Treatment history | 2 | −.40 | .33 | .222 | .86 | 1 | .353 | <.001 | — | |
| SBE frequency | 3 | −.18 | .10 | .062 | .02 | 2 | .988 | <.001 | — | |
| Purging frequency | 2 | .89 | .11 | <.001 | 6.93 | 1 | .008 | 85.57 | — | |
| Self-esteem | 1 | .45 | .22 | .040 | — | — | — | — | * | |
| Perfectionism | 3 | .10 | .17 | .546 | 2.18 | 2 | .336 | 8.40 | — | |
| Eating psychopathology | 9 | −.28 | .22 | .218 | 58.87 | 8 | <.001 | 86.41 | — | |
| Body dissatisfaction | 7 | −.16 | .12 | .174 | 10.62 | 6 | .101 | 43.50 | — | |
| Restraint | 5 | .65 | .09 | <.001 | 54.41 | 4 | <.001 | 92.65 | — | |
Note. PD = Purging Disorder; AN = Anorexia Nervosa; BN = Bulimia Nervosa; BED = Binge Eating Disorder. Positive g values indicate higher means in the PD group. The fail-safe N was calculated for statistically significant effect sizes (p < .05).
Indicates the fail-safe N was not possible to be calculated if fewer than 3 studies were included in the comparison, or if fixed effects model was used with a limited number of studies.
Table 4.
Summary Statistics for Moderation Analyses
| Comparison groups | Dependent variable | Moderator | Q | df | p | Moderator levels | Number of studies | g | SE | p |
|---|---|---|---|---|---|---|---|---|---|---|
| PD/AN | Eating psychopathology | Inclusion of SBEs in PD diagnosis | 4.42 | 1 | .036 | Allowed | 4 | .32 | .18 | .084 |
| Not specified | 5 | −.39 | .42 | .352 | ||||||
|
|
||||||||||
| Body dissatisfaction | Inclusion of SBEs in PD diagnosis | 4.17 | 1 | .041 | Allowed | 4 | .48 | .14 | <.001 | |
| Not specified | 4 | −.21 | .31 | .489 | ||||||
Note. PD = Purging Disorder; AN = Anorexia Nervosa; BN = Bulimia Nervosa; BED = Binge Eating Disorder; SBE = Subjective binge episode. No studies were available at the “Excluded” level of the moderator.
Table 5.
Summary of Individual Effect Sizes
| Study name | AN subtype | Comparison | Outcome | Measure | g | SE | p |
|---|---|---|---|---|---|---|---|
| Allen, Byrne, Oddy, and Crosby (2013a) | PD vs. BED | Depression | Beck Depression Inventory for Youth | −.07 | .35 | .836 | |
| PD vs. BED | Eating psychopathology | Global index of eating disorder symptoms (derived from EDE-Q) | .38 | .35 | .278 | ||
| PD vs. BN | Depression | Beck Depression Inventory for Youth | .08 | .32 | .789 | ||
| PD vs. BN | Eating psychopathology | Global index of eating disorder symptoms (derived from EDE-Q) | −.48 | .32 | .135 | ||
| PD vs. Control | Depression | Beck Depression Inventory for Youth | 1.03 | .23 | <.001 | ||
| PD vs. Control | Eating psychopathology | Global index of eating disorder symptoms (derived from EDE-Q) | 2.90 | .25 | <.001 | ||
| n.s. | PD vs. AN | Depression | Beck Depression Inventory for Youth | .18 | .71 | .797 | |
| n.s. | PD vs. AN | Eating psychopathology | Global index of eating disorder symptoms (derived from EDE-Q) | .26 | .71 | .714 | |
| Allen, Byrne, Oddy, and Crosby (2013b) | PD vs. BED | Natural course | % remitted | .00 | .33 | .989 | |
| PD vs. BN | Natural course | % remitted | .20 | .33 | .549 | ||
| Binford and Le Grange (2005) | PD vs. BN | Anxiety | Anxiety disorder | .14 | .34 | .686 | |
| PD vs. BN | Body dissatisfaction | EDE-shape concern | −.69 | .28 | .015 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern | −.94 | .29 | .001 | ||
| PD vs. BN | Depression | BDI | −.21 | .28 | .439 | ||
| PD vs. BN | Depression | Depression diagnosis | −.14 | .30 | .651 | ||
| PD vs. BN | Duration of illness | Months | −.10 | .28 | .710 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern | −1.26 | .30 | <.001 | ||
| PD vs. BN | Purging frequency | −.29 | .28 | .290 | |||
| PD vs. BN | Restraint | EDE-restraint | .16 | .28 | .566 | ||
| PD vs. BN | SBE frequency | .02 | .28 | .937 | |||
| PD vs. BN | Self-esteem | RSE | −.56 | .28 | .044 | ||
| PD vs. BN | Substance use | Substance use disorder | −.03 | .31 | .924 | ||
| Darcy et al. (2015) | PD vs. BN | Body dissatisfaction | EDE-shape concern | −.06 | .21 | .768 | |
| PD vs. BN | Body dissatisfaction | EDE-weight concern | −.14 | .21 | .516 | ||
| PD vs. BN | Depression | Depression diagnosis | .37 | .25 | .135 | ||
| PD vs. BN | Duration of illness | Months | .01 | .21 | .974 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concerns | −.26 | .21 | .214 | ||
| PD vs. BN | Purging frequency | −.24 | .21 | .265 | |||
| PD vs. BN | Restraint | EDE-restraint | .00 | .21 | 1.000 | ||
| PD vs. BN | SBE frequency | .36 | .21 | .086 | |||
| Davis, Holland, and Keel (2014) | PD vs. BN | Age of onset | (unpublished data) | −.09 | .31 | .780 | |
| PD vs. BN | Anxiety | STAI-trait | −.51 | .32 | .108 | ||
| PD vs. BN | Body dissatisfaction | BSQ | −.96 | .33 | .003 | ||
| PD vs. BN | Duration of illness | Months (unpublished data) | −.05 | .31 | .876 | ||
| PD vs. BN | Eating psychopathology | EAT | −.96 | .33 | .003 | ||
| PD vs. BN | Perfectionism | EDI-perfectionism | .03 | .31 | .922 | ||
| PD vs. Control | Anxiety | STAI-trait | 1.67 | .36 | <.001 | ||
| PD vs. Control | Body dissatisfaction | BSQ | 2.23 | .40 | <.001 | ||
| PD vs. Control | Eating psychopathology | EAT | 1.55 | .36 | <.001 | ||
| PD vs. Control | Perfectionism | EDI-perfectionism | .76 | .32 | .018 | ||
| Eddy, Doyle, Hoste, Herzog, and Le Grange (2008)a | PD vs. BN | Body dissatisfaction | EDE-shape concern | −.50 | .20 | .012 | |
| PD vs. BN | Body dissatisfaction | EDE-weight concern | −.50 | .20 | .012 | ||
| PD vs. BN | Depression | BDI | −.08 | .20 | .681 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern | −1.04 | .21 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDE-global | −.61 | .20 | .002 | ||
| PD vs. BN | Purging frequency | −.55 | .20 | .006 | |||
| PD vs. BN | Restraint | EDE-restraint | −.13 | .20 | .498 | ||
| PD vs. BN | SBE frequency | −.12 | .20 | .530 | |||
| PD vs. BN | Self-esteem | RSE | .33 | .20 | .091 | ||
| n.s. | PD vs. AN | Body dissatisfaction | EDE-shape concern | .95 | .21 | <.001 | |
| n.s. | PD vs. AN | Body dissatisfaction | EDE-weight concern | .92 | .21 | <.001 | |
| n.s. | PD vs. AN | Depression | BDI | .61 | .20 | .003 | |
| n.s. | PD vs. AN | Eating psychopathology | EDE-eating concern | .69 | .20 | .001 | |
| n.s. | PD vs. AN | Eating psychopathology | EDE-global | .94 | .21 | <.001 | |
| n.s. | PD vs. AN | Purging frequency | 1.14 | .21 | <.001 | ||
| n.s. | PD vs. AN | Restraint | EDE-restraint | .65 | .20 | .001 | |
| n.s. | PD vs. AN | SBE frequency | .26 | .20 | .182 | ||
| n.s. | PD vs. AN | Self-esteem | RSE | −.54 | .20 | .007 | |
| Ekeroth, Clinton, Norring, and Birgegard (2013) | AN-bp | PD vs. AN | Age of onset | (unpublished data) | .15 | .15 | .330 |
| AN-bp | PD vs. AN | Anxiety | Anxiety disorder | .04 | .13 | .783 | |
| AN-bp | PD vs. AN | Body dissatisfaction | EDE-shape concern (unpublished data) | .23 | .11 | .029 | |
| AN-bp | PD vs. AN | Depression | Mood disorder | −.25 | .11 | .018 | |
| AN-bp | PD vs. AN | Duration of illness | Months (unpublished data) | .21 | .15 | .156 | |
| AN-bp | PD vs. AN | Eating psychopathology | EDE-Q global | −.08 | .09 | .386 | |
| AN-bp | PD vs. AN | Impairment | CIA | −.53 | .10 | <.001 | |
| AN-bp | PD vs. AN | Purging frequency | −.46 | .09 | <.001 | ||
| AN-bp | PD vs. AN | Restraint | EDE-restraint (unpublished data) | −.27 | .11 | .012 | |
| AN-bp | PD vs. AN | SBE frequency | −.28 | .09 | .003 | ||
| AN-bp | PD vs. AN | Substance use | Substance use disorder | .00 | .17 | 1.000 | |
| AN-bp | PD vs. AN | Suicidality | % classified as “high risk” (unpublished data) | .13 | .29 | .644 | |
| AN-bp | PD vs. AN | Suicidality | CPRS-S-A item 19 (unpublished data) | −.27 | .11 | .011 | |
| AN-bp | PD vs. AN | Treatment outcome | % with no diagnosis | .39 | .11 | <.001 | |
| AN-r | PD vs. AN | Age of onset | (unpublished data) | −.04 | .14 | .794 | |
| AN-r | PD vs. AN | Anxiety | Anxiety disorder | .25 | .13 | .065 | |
| AN-r | PD vs. AN | Body dissatisfaction | EDE-shape concern (unpublished data) | .69 | .09 | .000 | |
| AN-r | PD vs. AN | Depression | Mood disorder | .18 | .11 | .096 | |
| AN-r | PD vs. AN | Duration of illness | Months (unpublished data) | .30 | .14 | .031 | |
| AN-r | PD vs. AN | Eating psychopathology | EDE-Q global | .57 | .09 | .000 | |
| AN-r | PD vs. AN | Impairment | CIA | −.06 | .09 | .499 | |
| AN-r | PD vs. AN | Purging frequency | 1.37 | .10 | <.001 | ||
| AN-r | PD vs. AN | Restraint | EDE-restraint (unpublished data) | .38 | .09 | <.001 | |
| AN-r | PD vs. AN | SBE frequency | −.18 | .09 | .048 | ||
| AN-r | PD vs. AN | Substance use | Substance use disorder | .60 | .20 | .002 | |
| AN-r | PD vs. AN | Suicidality | % classified as “high risk” (unpublished data) | 1.08 | .44 | .014 | |
| AN-r | PD vs. AN | Suicidality | CPRS-S-A item 19 (unpublished data) | .15 | .09 | .114 | |
| AN-r | PD vs. AN | Treatment outcome | % with no diagnosis | .26 | .10 | .012 | |
| PD vs. BED | Age of onset | (unpublished data) | .02 | .15 | .918 | ||
| PD vs. BED | Anxiety | Anxiety disorder | .07 | .17 | .656 | ||
| PD vs. BED | Body dissatisfaction | EDE-shape concern (unpublished data) | .07 | .11 | .522 | ||
| PD vs. BED | Depression | Mood disorder | −.47 | .13 | <.001 | ||
| PD vs. BED | Duration of illness | Months (unpublished data) | −.50 | .15 | .001 | ||
| PD vs. BED | Eating psychopathology | EDE-Q global | .41 | .12 | <.001 | ||
| PD vs. BED | Impairment | CIA | −.15 | .12 | .196 | ||
| PD vs. BED | Purging frequency | 1.03 | .12 | <.001 | |||
| PD vs. BED | Restraint | EDE-restraint (unpublished data) | 1.24 | .12 | <.001 | ||
| PD vs. BED | SBE frequency | −.19 | .12 | .107 | |||
| PD vs. BED | Substance use | Substance use disorder | −.20 | .19 | .301 | ||
| PD vs. BED | Suicidality | % classified as “high risk” (unpublished data) | .39 | .37 | .285 | ||
| PD vs. BED | Suicidality | CPRS-S-A item 19 (unpublished data) | .15 | .11 | .190 | ||
| PD vs. BED | Treatment outcome | % with no diagnosis | .28 | .13 | .035 | ||
| PD vs. BN | Age of onset | (unpublished data) | .12 | .10 | .234 | ||
| PD vs. BN | Anxiety | Anxiety disorder | .11 | .12 | .320 | ||
| PD vs. BN | Body dissatisfaction | EDE-shape concern (unpublished data) | −.08 | .08 | .327 | ||
| PD vs. BN | Depression | Mood disorder | −.27 | .09 | .003 | ||
| PD vs. BN | Duration of illness | Months (unpublished data) | −.13 | .10 | .200 | ||
| PD vs. BN | Eating psychopathology | EDE-Q global | −.12 | .08 | .155 | ||
| PD vs. BN | Impairment | CIA | −.22 | .08 | .006 | ||
| PD vs. BN | Purging frequency | −.30 | .08 | <.001 | |||
| PD vs. BN | Restraint | EDE-restraint (unpublished data) | .20 | .08 | .009 | ||
| PD vs. BN | SBE frequency | −.14 | .08 | .082 | |||
| PD vs. BN | Substance use | Substance use disorder | −.15 | .14 | .280 | ||
| PD vs. BN | Suicidality | % classified as “high risk” (unpublished data) | .09 | .20 | .651 | ||
| PD vs. BN | Suicidality | CPRS-S-A item 19 (unpublished data) | .03 | .08 | .662 | ||
| PD vs. BN | Treatment outcome | % with no diagnosis | .04 | .09 | .618 | ||
| Favaro, Ferrara, and Santonastaso (2003) | PD vs. BED | Age of onset | .53 | .50 | .291 | ||
| PD vs. BED | Duration of illness | Months | −.71 | .50 | .161 | ||
| PD vs. BED | Treatment history | % with any type of treatment | .38 | .90 | .674 | ||
| PD vs. BED | Treatment outcome | % remitted | −.38 | .67 | .566 | ||
| PD vs. BN | Age of onset | .96 | .36 | .007 | |||
| PD vs. BN | Duration of illness | Months | −.80 | .35 | .024 | ||
| PD vs. BN | Treatment history | % with any type of treatment | −.81 | .60 | .177 | ||
| PD vs. BN | Treatment outcome | % remitted | .59 | .41 | .150 | ||
| n.s. | PD vs. AN | Age of onset | .69 | .39 | .075 | ||
| n.s. | PD vs. AN | Duration of illness | Months | −.41 | .38 | .282 | |
| n.s. | PD vs. AN | Treatment history | % with any type of treatment | −1.24 | .62 | .044 | |
| n.s. | PD vs. AN | Treatment outcome | % remitted | .39 | .44 | .380 | |
| Fink et al. (2009)b | PD vs. Control | Anxiety | BAI | .09 | .41 | .833 | |
| PD vs. Control | Body dissatisfaction | EDI-body dissatisfaction | 1.61 | .42 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDI-drive for thinness | 1.57 | .42 | <.001 | ||
| PD vs. Control | Depression | BDI | .40 | .01 | <.001 | ||
| PD vs. Control | Eating psychopathology | EDI-bulimia | −.09 | .41 | .826 | ||
| PD vs. Control | Impulsivity | IBS | 1.02 | .41 | .014 | ||
| PD vs. Control | Perfectionism | EDI-perfectionism | 1.65 | .42 | <.001 | ||
| PD vs. Control | Self-esteem | RSE | .34 | .41 | .411 | ||
| Flament et al. (2015) | PD vs. BED | Anxiety | MASC-10 | −.33 | .28 | .233 | |
| PD vs. BED | Depression | CDI | .12 | .27 | .669 | ||
| PD vs. BED | Eating psychopathology | DEBQ emotional eating | −1.52 | .31 | <.001 | ||
| PD vs. BED | Restraint | DEBQ restrained eating | .26 | .27 | .346 | ||
| PD vs. BED | Substance use | Substance use | .70 | .32 | .027 | ||
| PD vs. BED | Suicidality | Suicidality | .27 | .33 | .407 | ||
| PD vs. BN | Anxiety | MASC-10 | −.38 | .20 | .060 | ||
| PD vs. BN | Depression | CDI | −.48 | .20 | .019 | ||
| PD vs. BN | Eating psychopathology | DEBQ emotional eating | −1.22 | .22 | <.001 | ||
| PD vs. BN | Restraint | DEBQ restrained eating | −.29 | .20 | .152 | ||
| PD vs. BN | Substance use | Substance use | .10 | .23 | .677 | ||
| PD vs. BN | Suicidality | Suicidality | −.25 | .23 | .274 | ||
| PD vs. Control | Anxiety | MASC-10 | .66 | .16 | <.001 | ||
| PD vs. Control | Depression | CDI | .87 | .16 | <.001 | ||
| PD vs. Control | Eating psychopathology | DEBQ emotional eating | .14 | .16 | .364 | ||
| − | PD vs. Control | Restraint | DEBQ restrained eating | 1.41 | .16 | <.001 | |
| PD vs. Control | Substance use | Substance use | .86 | .19 | <.001 | ||
| PD vs. Control | Suicidality | Suicidality | .88 | .18 | <.001 | ||
| García, Planell, Estragués, i Escursell, and Carracedo (2010) | PD vs. BED | Body dissatisfaction | BSQ | .54 | .46 | .241 | |
| PD vs. BED | Body dissatisfaction | EDI-body dissatisfaction | −.55 | .46 | .235 | ||
| PD vs. BED | Body dissatisfaction | EDI-drive for thinness | .04 | .46 | .922 | ||
| PD vs. BED | Duration of illness | Months | −.74 | .47 | .114 | ||
| PD vs. BED | Eating psychopathology | BITE Severity Scale | .04 | .46 | .938 | ||
| PD vs. BED | Eating psychopathology | BITE Symptoms Scale | −.63 | .47 | .177 | ||
| PD vs. BED | Eating psychopathology | EDI-bulimia | −.25 | .46 | .582 | ||
| PD vs. BED | Impulsivity | EDI-impulsiveness | .28 | .46 | .536 | ||
| PD vs. BED | Perfectionism | EDI-perfectionism | .23 | .46 | .613 | ||
| PD vs. BN | Body dissatisfaction | BSQ | −.50 | .30 | .099 | ||
| PD vs. BN | Body dissatisfaction | EDI-body dissatisfaction | −.66 | .31 | .031 | ||
| PD vs. BN | Body dissatisfaction | EDI-drive for thinness | 1.02 | .32 | .001 | ||
| PD vs. BN | Duration of illness | Months | −.27 | .30 | .363 | ||
| PD vs. BN | Eating psychopathology | BITE Severity Scale | −1.21 | .33 | <.001 | ||
| PD vs. BN | Eating psychopathology | BITE Symptoms Scale | −1.57 | .34 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDI-bulimia | −2.86 | .42 | .000 | ||
| PD vs. BN | Impulsivity | EDI-impulsiveness | −.71 | .31 | .022 | ||
| PD vs. BN | Perfectionism | EDI-perfectionism | −.28 | .30 | .358 | ||
| Goldschmidt et al. (2016)c | AN-bp | PD vs. AN | Body dissatisfaction | EDE-shape concern PD LOC | .26 | .26 | .313 |
| AN-bp | PD vs. AN | Body dissatisfaction | EDE-shape concern PD NO LOC | .28 | .21 | .185 | |
| AN-bp | PD vs. AN | Body dissatisfaction | EDE-weight concern PD LOC | .35 | .26 | .188 | |
| AN-bp | PD vs. AN | Body dissatisfaction | EDE-weight concern PD NO LOC | .36 | .21 | .088 | |
| AN-bp | PD vs. AN | Depression | BDI (PD LOC) | .04 | .26 | .869 | |
| AN-bp | PD vs. AN | Depression | BDI (PD NO LOC) | .04 | .21 | .835 | |
| AN-bp | PD vs. AN | Eating psychopathology | EDE-eating concern (PD LOC) | .15 | .26 | .567 | |
| AN-bp | PD vs. AN | Eating psychopathology | EDE-eating concern (PD NO LOC) | .14 | .21 | .493 | |
| AN-bp | PD vs. AN | Restraint | EDE-restraint (PD LOC) | −.50 | .26 | .059 | |
| AN-bp | PD vs. AN | Restraint | EDE-restraint (PD NO LOC) | −.49 | .21 | .021 | |
| AN-bp | PD vs. AN | Self-esteem | RSE (PD LOC) | 1.64 | .30 | <.001 | |
| AN-bp | PD vs. AN | Self-esteem | RSE (PD NO LOC) | 1.61 | .24 | <.001 | |
| PD vs. BN | Body dissatisfaction | EDE-shape concern PD LOC | −.41 | .23 | .073 | ||
| PD vs. BN | Body dissatisfaction | EDE-shape concern PD NO LOC | −.27 | .16 | .091 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern PD LOC | −.32 | .23 | .158 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern PD NO LOC | −.13 | .16 | .419 | ||
| PD vs. BN | Depression | BDI (PD LOC) | −.25 | .23 | .275 | ||
| PD vs. BN | Depression | BDI (PD NO LOC) | −.24 | .16 | .132 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern (PD LOC) | −.63 | .23 | .006 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern (PD NO LOC) | −.68 | .16 | <.001 | ||
| PD vs. BN | Restraint | EDE-restraint (PD LOC) | −.43 | .23 | .057 | ||
| PD vs. BN | Restraint | EDE-restraint (PD NO LOC) | .06 | .16 | .686 | ||
| PD vs. BN | Self-esteem | RSE (PD LOC) | 1.13 | .23 | <.001 | ||
| PD vs. BN | Self-esteem | RSE (PD NO LOC) | −.27 | .16 | .094 | ||
| Haedt and Keel (2010) | PD vs. Control | Anxiety | Checklist (unpublished data) | 1.83 | .49 | <.001 | |
| PD vs. Control | Body dissatisfaction | EDI-drive for thinness (unpublished data) | 1.45 | .24 | <.001 | ||
| PD vs. Control | Depression | Checklist (unpublished data) | .43 | .46 | .349 | ||
| PD vs. Control | Eating psychopathology | EDI-bulimia (unpublished data) | .94 | .24 | <.001 | ||
| PD vs. Control | Medical morbidity | History of cancer, high blood pressure, diabetes, or migraines (unpublished data) | .68 | .46 | .142 | ||
| PD vs. Control | Perfectionism | EDI-perfectionism | .98 | .01 | <.001 | ||
| PD vs. Control | Purging frequency | (unpublished data) | 6.12 | .39 | <.001 | ||
| PD vs. Control | Quality of life/psychosocial functioning | Satisfaction with relationships | −1.40 | .01 | <.001 | ||
| PD vs. Control | Quality of life/psychosocial functioning | Satisfaction with school | −.50 | .01 | <.001 | ||
| PD vs. Control | Restraint | Restraint Scale items (unpublished data) | 1.58 | .38 | <.001 | ||
| PD vs. Control | Substance use | Frequency of alcohol use | .04 | .01 | <.001 | ||
| PD vs. Control | Substance use | Frequency of cigarette use | .22 | .01 | <.001 | ||
| PD vs. Control | Treatment history | Lifetime eating disorder treatment (unpublished data) | .92 | .64 | .154 | ||
| Helverskov et al. (2011) | PD vs. BN | Eating psychopathology | EDE-global | −.40 | .14 | .006 | |
| PD vs. BN | Eating psychopathology | EDI-total | −.19 | .14 | .184 | ||
| PD vs. BN | Purging frequency | .01 | .14 | .957 | |||
| n.s. | PD vs. AN | Purging frequency | .50 | .15 | .001 | ||
| Keel, Haedt, and Edler (2005) | PD vs. BN | Age of onset | (unpublished data) | .25 | .25 | .317 | |
| PD vs. BN | Anxiety | Lifetime anxiety disorder | .34 | .26 | .189 | ||
| PD vs. BN | Anxiety | STAI-trait | −.62 | .23 | .007 | ||
| PD vs. BN | Body dissatisfaction | BSQ | −.37 | .23 | .104 | ||
| PD vs. BN | Body dissatisfaction | EDE-shape concern | −.36 | .23 | .116 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern | .08 | .23 | .734 | ||
| PD vs. BN | Depression | BDI | −.59 | .23 | .011 | ||
| PD vs. BN | Depression | Lifetime mood disorder | −.20 | .31 | .522 | ||
| PD vs. BN | Duration of illness | (unpublished data) | −.47 | .25 | .061 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern | −.69 | .23 | .003 | ||
| PD vs. BN | Eating psychopathology | EDE-global | −.22 | .23 | .334 | ||
| PD vs. BN | Impulsivity | BIS-11 | −.01 | .23 | .972 | ||
| PD vs. BN | Impulsivity | Lifetime impulse control disorder | −.22 | .27 | .411 | ||
| PD vs. BN | Natural course (%remitted) | % remitted at follow-up; i.e., no symptoms within last 12 weeks | .42 | .68 | .533 | ||
| PD vs. BN | Purging frequency | −.53 | .23 | .022 | |||
| PD vs. BN | Restraint | EDE-restraint | .00 | .23 | 1.000 | ||
| PD vs. BN | Restraint | TFEQ | −1.05 | .24 | <.001 | ||
| PD vs. BN | Substance use | Lifetime substance use disorder | .35 | .25 | .165 | ||
| PD vs. BN | Suicidality | Current suicidal ideation (unpublished data) | −.53 | .86 | .534 | ||
| PD vs. BN | Treatment history | Current treatment(unpublished data) | −.25 | .26 | .328 | ||
| PD vs. BN | Treatment history | Lifetime treatment(unpublished data) | −.27 | .51 | .603 | ||
| PD vs. Control | Anxiety | Lifetime anxiety disorder | 1.63 | .46 | <.001 | ||
| PD vs. Control | Anxiety | STAI-trait | 1.25 | .26 | <.001 | ||
| PD vs. Control | Body dissatisfaction | BSQ | 3.68 | .39 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE-shape concern | 4.01 | .41 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE-weight concern | 4.71 | .46 | <.001 | ||
| PD vs. Control | Depression | BDI | 1.44 | .26 | <.001 | ||
| PD vs. Control | Depression | Lifetime mood disorder | 1.96 | .40 | <.001 | ||
| PD vs. Control | Eating psychopathology | EDE-eating concern | 2.84 | .33 | <.001 | ||
| PD vs. Control | Eating psychopathology | EDE-global | 5.10 | .49 | <.001 | ||
| PD vs. Control | Impulsivity | BIS-11 | .82 | .24 | .001 | ||
| PD vs. Control | Impulsivity | Lifetime impulse control disorder | 1.88 | .80 | .019 | ||
| PD vs. Control | Restraint | EDE-restraint | 3.98 | .41 | <.001 | ||
| PD vs. Control | Restraint | TFEQ | 3.37 | .37 | <.001 | ||
| PD vs. Control | Substance use | Lifetime substance use disorder | 1.65 | .43 | <.001 | ||
| PD vs. Control | Treatment history | Current treatment (unpublished data) | 1.61 | .58 | .006 | ||
| PD vs. Control | Treatment history | Lifetime treatment (unpublished data) | 1.99 | .40 | <.001 | ||
| Keel, Mayer, and Harnden-Fischer (2001)d | PD vs. BN | Anxiety | STAI-state | .18 | .27 | .500 | |
| PD vs. BN | Anxiety | STAI-trait | .14 | .27 | .595 | ||
| PD vs. BN | Depression | BDI | −.02 | .27 | .938 | ||
| PD vs. BN | Eating psychopathology | Bulimia Test-Revised | −.89 | .28 | .002 | ||
| PD vs. BN | Impulsivity | BIS-11 | −.78 | .28 | .005 | ||
| PD vs. BN | Purging frequency | −.79 | .28 | .005 | |||
| PD vs. BN | Restraint | Revised Restraint Scale | −.43 | .27 | .119 | ||
| PD vs. BN | Restraint | TFEQ-cognitive | .36 | .27 | .187 | ||
| PD vs. BN | Restraint | TFEQ-disinhibition | −.51 | .27 | .064 | ||
| PD vs. BN | Restraint | TFEQ-hunger | −.28 | .27 | .303 | ||
| PD vs. BN | SBE frequency | Loss of control frequency | −.82 | .28 | .004 | ||
| PD vs. BN | Substance abuse | DAST | −.40 | .27 | .143 | ||
| PD vs. BN | Substance abuse | MAST | −.47 | .27 | .085 | ||
| PD vs. BN | Treatment history | % with lifetime history of treatment | −.92 | .33 | .005 | ||
| Keel, Wolfe, Gravener, and Jimerson (2008) | PD vs. BN | Anxiety | Lifetime anxiety disorder | .13 | .27 | .622 | |
| PD vs. BN | Anxiety | STAI-trait | −7.35 | .63 | <.001 | ||
| PD vs. BN | Body dissatisfaction | BSQ (unpublished data) | −.51 | .22 | .023 | ||
| PD vs. BN | Body dissatisfaction | EDE weight and shape concerns (unpublished data) | −.35 | .22 | .113 | ||
| PD vs. BN | Depression | BDI | −5.43 | .49 | .000 | ||
| PD vs. BN | Depression | Lifetime mood disorder | −.74 | .29 | .011 | ||
| PD vs. BN | Eating psychopathology | EDE-global (unpublished data) | −.41 | .22 | .064 | ||
| PD vs. BN | Restraint | EDE-restraint (unpublished data) | −.14 | .22 | .512 | ||
| PD vs. BN | Restraint | TFEQ-CR (unpublished data) | .20 | .22 | .362 | ||
| PD vs. BN | Impulsivity | BIS-11 | −2.13 | .29 | <.001 | ||
| PD vs. BN | Impulsivity | Lifetime impulse control disorder | −.38 | .30 | .202 | ||
| PD vs. BN | Purging frequency | −.30 | .24 | .220 | |||
| PD vs. BN | Quality of life/psychosocial functioning | SAS-SR | −2.97 | .34 | <.001 | ||
| PD vs. BN | SBE frequency | (unpublished data) | .49 | .22 | .028 | ||
| PD vs. BN | Substance use | Lifetime substance use disorder | −.15 | .27 | .564 | ||
| PD vs. BN | Age of onset | (unpublished data) | .14 | .24 | .538 | ||
| PD vs. BN | Duration of illness | Months (unpublished data) | −.23 | .24 | .333 | ||
| PD vs. BN | Suicidality | Current suicidal ideation (unpublished data) | −.06 | .91 | .949 | ||
| PD vs. BN | Suicidality | Lifetime attempt (unpublished data) | .44 | .47 | .351 | ||
| PD vs. BN | Treatment history | Current treatment (unpublished data) | .02 | .35 | .958 | ||
| PD vs. BN | Treatment history | Lifetime treatment (unpublished data) | −.11 | .27 | .677 | ||
| PD vs. Control | Suicidality | Lifetime attempt (unpublished data) | .69 | .65 | .291 | ||
| PD vs. Control | Treatment history | Current treatment (unpublished data) | .75 | .49 | .128 | ||
| PD vs. Control | Treatment history | Lifetime treatment (unpublished data) | .86 | .27 | .002 | ||
| PD vs. Control | Anxiety | Lifetime anxiety disorder | .91 | .32 | .004 | ||
| PD vs. Control | Anxiety | STAI-trait | 6.52 | .64 | <.001 | ||
| PD vs. Control | Body dissatisfaction | BSQ (unpublished data) | 4.73 | .44 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE weight and shape concerns (unpublished data) | 5.20 | .47 | <.001 | ||
| PD vs. Control | Depression | BDI | 5.30 | .54 | <.001 | ||
| PD vs. Control | Depression | Lifetime mood disorder | .91 | .32 | .004 | ||
| PD vs. Control | Eating psychopathology | EDE-global (unpublished data) | 5.46 | .49 | <.001 | ||
| PD vs. Control | Restraint | EDE-restraint (unpublished data) | 3.95 | .39 | <.001 | ||
| PD vs. Control | Restraint | TFEQ-CR (unpublished data) | 4.55 | .43 | <.001 | ||
| PD vs. Control | Impulsivity | BIS-11 | 3.16 | .38 | <.001 | ||
| PD vs. Control | Impulsivity | Lifetime impulse control disorder | .54 | .38 | .157 | ||
| PD vs. Control | Quality of life/psychosocial functioning | SAS-SR | 2.96 | .37 | <.001 | ||
| PD vs. Control | SBE frequency | (unpublished data) | 1.61 | .26 | <.001 | ||
| PD vs. Control | Substance use | Lifetime substance use disorder | .83 | .32 | .010 | ||
| Knoph et al. (2013) | PD vs. BED | Natural course (%remitted) | % with no ED diagnosis at follow-up | .33 | .24 | .157 | |
| PD vs. BN | Natural course (%remitted) | % with no ED diagnosis at follow-up | .62 | .25 | .013 | ||
| n.s. | PD vs. AN | Natural course (%remitted) | % with no ED diagnosis at follow-up | −.04 | .35 | .899 | |
| Koch, Quadflieg, and Fichter (2013) | AN-bp | PD vs. AN | Age of onset | Age of onset | .29 | .08 | <.001 |
| AN-bp | PD vs. AN | Anxiety | Anxiety disorder | .18 | .11 | .104 | |
| AN-bp | PD vs. AN | Body dissatisfaction | SIAB-S body image | −.49 | .08 | <.001 | |
| AN-bp | PD vs. AN | Depression | BDI | −.33 | .08 | <.001 | |
| AN-bp | PD vs. AN | Depression | Mood disorder | .00 | .10 | .980 | |
| AN-bp | PD vs. AN | Duration of illness | Months | .20 | .08 | .013 | |
| AN-bp | PD vs. AN | Eating psychopathology | EDI-bulimia | −.91 | .08 | <.001 | |
| AN-bp | PD vs. AN | Eating psychopathology | SIAB-S bulimic symptoms | −1.46 | .09 | <.001 | |
| AN-bp | PD vs. AN | Mortality | Crude mortality rate | .17 | .22 | .422 | |
| AN-bp | PD vs. AN | Substance use | Substance-related disorder | −.17 | .19 | .356 | |
| AN-bp | PD vs. AN | Treatment history | Total length of treatment in years | −.21 | .08 | .010 | |
| AN-bp | PD vs. AN | Treatment outcome | % with no diagnosis | .08 | .11 | .469 | |
| PD vs. BN | Age of onset | −.02 | .08 | .839 | |||
| PD vs. BN | Anxiety | Anxiety disorder | .16 | .10 | .095 | ||
| PD vs. BN | Body dissatisfaction | SIAB-S body image | .08 | .08 | .293 | ||
| PD vs. BN | Depression | BDI | −.04 | .08 | .613 | ||
| PD vs. BN | Depression | Mood disorder | .04 | .09 | .692 | ||
| PD vs. BN | Duration of illness | Months | .16 | .08 | .030 | ||
| PD vs. BN | Eating psychopathology | EDI bulimia | −2.10 | .09 | <.001 | ||
| PD vs. BN | Eating psychopathology | SIAB-S bulimic symptoms | −5.22 | .14 | <.001 | ||
| PD vs. BN | Mortality | Crude mortality rate | .86 | .26 | .001 | ||
| PD vs. BN | Substance use | Substance-related disorder | −.06 | .17 | .713 | ||
| PD vs. BN | Treatment history | Total length of treatment in years | .00 | .08 | .975 | ||
| PD vs. BN | Treatment outcome | % with no diagnosis | −.22 | .10 | .034 | ||
| Le Grange et al. (2006) | PD vs. BN | Body dissatisfaction | EDE-shape concern | .20 | .22 | .375 | |
| PD vs. BN | Body dissatisfaction | EDE-weight concern | .11 | .22 | .626 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern | −.21 | .22 | .341 | ||
| PD vs. BN | Restraint | EDE-restraint | .26 | .22 | .254 | ||
| MacDonald, Trottier, McFarlane, and Olmsted (2015) | PD vs. BN | Age of onset | (unpublished data|) | .45 | .24 | .064 | |
| PD vs. BN | Body dissatisfaction | EDE-shape concern (unpublished data) | −.09 | .26 | .728 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern (unpublished data) | .14 | .25 | .583 | ||
| PD vs. BN | Depression | BDI-II (unpublished data|) | −.28 | .25 | .258 | ||
| PD vs. BN | Duration of illness | Months (unpublished data|) | −.25 | .24 | .313 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern (unpublished data) | −.64 | .25 | .012 | ||
| PD vs. BN | Purging frequency | (unpublished data) | −.30 | .24 | .215 | ||
| PD vs. BN | Restraint | EDE-restraint (unpublished data) | .16 | .25 | .528 | ||
| PD vs. BN | SBE frequency | (unpublished data) | −.16 | .24 | .524 | ||
| PD vs. BN | Self-esteem | RSE (unpublished data|) | .42 | .25 | .084 | ||
| PD vs. BN | Treatment outcome | % remitted (defined as 1 binge eating and/or vomiting episode in the last two weeks of treatment and 1 episode in the first month after treatment ended) | .47 | .30 | .119 | ||
| Marino (2011) | AN-bp | PD vs. AN | Body dissatisfaction | EDE-shape concern | −.54 | .28 | .059 |
| AN-bp | PD vs. AN | Body dissatisfaction | EDE-weight concern | −.54 | .28 | .059 | |
| AN-bp | PD vs. AN | Depression | IDS-SR | −.62 | .30 | .039 | |
| AN-bp | PD vs. AN | Eating psychopathology | EDE-eating concern | −1.37 | .31 | <.001 | |
| AN-bp | PD vs. AN | Restraint | EDE-restraint | .54 | .28 | .059 | |
| PD vs. BN | Body dissatisfaction | EDE-shape concern | −.45 | .24 | .060 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern | −.45 | .24 | .060 | ||
| PD vs. BN | Depression | IDS-SR | −.44 | .23 | .060 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern | −1.08 | .24 | <.001 | ||
| PD vs. BN | Restraint | EDE-restraint | .45 | .24 | .060 | ||
| Metzler-Brody et al. (2011) | PD vs. BED | Anxiety | STAI-trait | −.06 | .38 | .870 | |
| PD vs. BED | Depression | Edinburgh Postnatal Depression Scale | .42 | .38 | .270 | ||
| PD vs. BED | Depression | PHQ severity | .71 | .39 | .069 | ||
| PD vs. BN | Anxiety | STAI-trait | −.46 | .35 | .184 | ||
| PD vs. BN | Depression | Edinburgh Postnatal Depression Scale | −.26 | .35 | .453 | ||
| PD vs. BN | Depression | PHQ severity | .15 | .35 | .656 | ||
| PD vs. Control | Anxiety | STAI-trait | .13 | .27 | .636 | ||
| PD vs. Control | Depression | Edinburgh Postnatal Depression Scale | .69 | .27 | .011 | ||
| PD vs. Control | Depression | PHQ severity | 1.05 | .28 | .000 | ||
| n.s. | PD vs. AN | Anxiety | STAI-trait | −.08 | .34 | .811 | |
| n.s. | PD vs. AN | Depression | Edinburgh Postnatal Depression Scale | .75 | .36 | .037 | |
| n.s. | PD vs. AN | Depression | PHQ severity | .97 | .37 | .008 | |
| Nakai, Fukushima, Taniguchi, Nin, and Teramukai (2013)e | PD vs. BED | Body dissatisfaction | EDI-body dissatisfaction | −1.08 | .28 | <.001 | |
| PD vs. BED | Body dissatisfaction | EDI-drive for thinness | −.50 | .27 | .066 | ||
| PD vs. BED | Duration of illness | Months | −.48 | .27 | .075 | ||
| PD vs. BED | Eating psychopathology | EAT | .14 | .27 | .614 | ||
| PD vs. BED | Eating psychopathology | EDI-bulimia | −1.13 | .28 | <.001 | ||
| PD vs. BED | Eating psychopathology | EDI-total | −.73 | .27 | .008 | ||
| PD vs. BED | Perfectionism | EDE-perfectionism | −.20 | .27 | .454 | ||
| PD vs. BN | Age of onset | .94 | .26 | <.001 | |||
| PD vs. BN | Body dissatisfaction | EDI-body dissatisfaction | −1.00 | .26 | <.001 | ||
| PD vs. BN | Body dissatisfaction | EDI-drive for thinness | −1.00 | .26 | <.001 | ||
| PD vs. BN | Duration of illness | Months | −.43 | .25 | .090 | ||
| PD vs. BN | Eating psychopathology | EAT | −.66 | .26 | .010 | ||
| PD vs. BN | Eating psychopathology | EDI-bulimia | −1.90 | .26 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDI-total | −1.16 | .26 | <.001 | ||
| PD vs. BN | Perfectionism | EDE-perfectionism | −.30 | .25 | .240 | ||
| n.s. | PD vs. AN | Age of onset | .99 | .26 | <.001 | ||
| n.s. | PD vs. AN | Body dissatisfaction | EDI-body dissatisfaction | −.12 | .26 | .634 | |
| n.s. | PD vs. AN | Body dissatisfaction | EDI-drive for thinness | −.54 | .26 | .036 | |
| n.s. | PD vs. AN | Duration of illness | Months | −.32 | .26 | .209 | |
| n.s. | PD vs. AN | Eating psychopathology | EAT | −.86 | .26 | .001 | |
| n.s. | PD vs. AN | Eating psychopathology | EDI-bulimia | −.68 | .26 | .009 | |
| n.s. | PD vs. AN | Eating psychopathology | EDI-total | −.59 | .26 | .022 | |
| n.s. | PD vs. AN | Perfectionism | EDI-perfectionism | −.07 | .26 | .798 | |
| Pisetsky, Thornton, Lichtenstein, Pedersen, and Bulik (2013) | AN-bp | PD vs. AN | Anxiety | Lifetime anxiety disorder | −.16 | .18 | .374 |
| AN-bp | PD vs. AN | Depression | Lifetime depression | .81 | .24 | .001 | |
| AN-bp | PD vs. AN | Substance use | Lifetime alcohol abuse/dependence | −.17 | .24 | .477 | |
| AN-bp | PD vs. AN | Substance use | Lifetime substance use (other than alcohol) | .20 | .24 | .416 | |
| AN-bp | PD vs. AN | Suicidality | % with lifetime attempt | −.13 | .27 | .631 | |
| AN-r | PD vs. AN | Anxiety | Lifetime anxiety disorder | .13 | .19 | .489 | |
| AN-r | PD vs. AN | Depression | Lifetime depression | 1.24 | .24 | <.001 | |
| AN-r | PD vs. AN | Substance use | Lifetime alcohol abuse/dependence | .03 | .26 | .916 | |
| AN-r | PD vs. AN | Substance use | Lifetime substance use (other than alcohol) | .25 | .26 | .340 | |
| AN-r | PD vs. AN | Suicidality | % with lifetime attempt | .21 | .32 | .518 | |
| PD vs. BED | Anxiety | Lifetime anxiety disorder | −.10 | .26 | .705 | ||
| PD vs. BED | Depression | Lifetime depression | .74 | .32 | .020 | ||
| PD vs. BED | Substance use | Lifetime alcohol abuse/dependence | −.30 | .33 | .354 | ||
| PD vs. BED | Substance use | Lifetime substance use (other than alcohol) | −.16 | .32 | .621 | ||
| PD vs. BED | Suicidality | % with lifetime attempt | −.14 | .39 | .714 | ||
| PD vs. BN | Anxiety | Lifetime anxiety disorder | −.34 | .16 | .030 | ||
| PD vs. BN | Depression | Lifetime depression | .83 | .22 | <.001 | ||
| PD vs. BN | Substance use | Lifetime alcohol abuse/dependence | −.44 | .20 | .030 | ||
| PD vs. BN | Substance use | Lifetime substance use (other than alcohol) | .08 | .21 | .715 | ||
| PD vs. BN | Suicidality | % with lifetime attempt | −.11 | .24 | .656 | ||
| PD vs. Control | Suicidality | % with lifetime attempt | 1.06 | .20 | <.001 | ||
| Roberto, Grilo, Masheb, and White (2010) | PD vs. BED | Body dissatisfaction | EDE-Q shape concern | −.28 | .22 | .198 | |
| PD vs. BED | Body dissatisfaction | EDE-Q weight concern | −.34 | .22 | .126 | ||
| PD vs. BED | Depression | BDI | −.59 | .22 | .007 | ||
| PD vs. BED | Eating psychopathology | EDE-Q eating concern | −.38 | .22 | .084 | ||
| PD vs. BED | Eating psychopathology | EDE-Q global | −.05 | .22 | .809 | ||
| PD vs. BED | Restraint | EDE-Q restraint | .70 | .22 | .002 | ||
| PD vs. BED | Restraint | TFEQ-disinhibition | −1.10 | .23 | <.001 | ||
| PD vs. BED | Restraint | TFEQ-hunger | −.41 | .22 | .063 | ||
| PD vs. BED | Restraint | TFEQ-restraint | 1.19 | .23 | .000 | ||
| PD vs. BED | SBE frequency | −.17 | .22 | .438 | |||
| PD vs. BED | Self-esteem | RSE | .45 | .22 | .040 | ||
| PD vs. BN | Body dissatisfaction | EDE-Q shape concern | −1.06 | .25 | <.001 | ||
| PD vs. BN | Body dissatisfaction | EDE-Q weight concern | −1.00 | .25 | <.001 | ||
| PD vs. BN | Depression | BDI | −1.21 | .26 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDE-Q eating concern | −1.18 | .26 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDE-Q global | −.99 | .25 | <.001 | ||
| PD vs. BN | Restraint | EDE-Q restraint | −.20 | .24 | .414 | ||
| PD vs. BN | Restraint | TFEQ-disinhibition | −1.50 | .27 | <.001 | ||
| PD vs. BN | Restraint | TFEQ-hunger | −.65 | .25 | .009 | ||
| PD vs. BN | Restraint | TFEQ-restraint | .48 | .24 | .047 | ||
| PD vs. BN | SBE frequency | −.46 | .24 | .058 | |||
| PD vs. BN | Self-esteem | RSE | .87 | .25 | .001 | ||
| Roberto, Haynos, Schwartz, Brownell, and White (2013) | PD vs. BED | Body dissatisfaction | EDE-Q shape concern | −.03 | .28 | .911 | |
| PD vs. BED | Body dissatisfaction | EDE-Q weight concern | .07 | .28 | .810 | ||
| PD vs. BED | Eating psychopathology | EDE-Q eating concern | .48 | .28 | .083 | ||
| PD vs. BED | Restraint | EDE-Q restraint | .46 | .28 | .099 | ||
| PD vs. BN | Body dissatisfaction | EDE-Q shape concern | −.65 | .32 | .039 | ||
| PD vs. BN | Body dissatisfaction | EDE-Q weight concern | −.78 | .32 | .015 | ||
| PD vs. BN | Eating psychopathology | EDE-Q eating concern | −.88 | .32 | .006 | ||
| PD vs. BN | Restraint | EDE-Q restraint | −.76 | .32 | .017 | ||
| PD vs. Control | Body dissatisfaction | EDE-Q shape concern | .57 | .25 | .022 | ||
| PD vs. Control | Body dissatisfaction | EDE-Q weight concern | .84 | .25 | .001 | ||
| PD vs. Control | Eating psychopathology | EDE-Q eating concern | 1.09 | .25 | <.001 | ||
| PD vs. Control | Restraint | EDE-Q restraint | .71 | .25 | .005 | ||
| Rockert, Kaplan, and Olmsted (2007) | AN-bp | PD vs. AN | Duration of illness | Months | .06 | .11 | .600 |
| AN-r | PD vs. AN | Duration of illness | Months | .00 | .12 | .971 | |
| PD vs. BED | Duration of illness | Months | −.67 | .18 | <.001 | ||
| PD vs. BN | Body dissatisfaction | EDI-body dissatisfaction (BN-p) | −.18 | .10 | .060 | ||
| PD vs. BN | Body dissatisfaction | EDI-drive for thinness (BN-p) | −.18 | .10 | .060 | ||
| PD vs. BN | Depression | BDI (BN-p) | .26 | .10 | .008 | ||
| PD vs. BN | Duration of illness | Months (BN-p) | −.24 | .10 | .013 | ||
| PD vs. BN | Eating psychopathology | EDI-bulimia (BN-p) | −.38 | .10 | <.001 | ||
| PD vs. BN | Perfectionism | EDI-perfectionism (BN-p) | −.18 | .10 | .060 | ||
| PD vs. BN | Self-esteem | RSE (BN-p) | −.18 | .10 | .060 | ||
| Smith and Crowther (2013) | PD vs. BN | Body dissatisfaction | BSQ | −.93 | .29 | .001 | |
| PD vs. BN | Body dissatisfaction | EDE-Q-shape concern | −.98 | .29 | .001 | ||
| PD vs. BN | Body dissatisfaction | EDE-Q-weight concern | −1.01 | .29 | .001 | ||
| PD vs. BN | Body dissatisfaction | SATAQ-internalization | −.42 | .28 | .133 | ||
| PD vs. BN | Eating psychopathology | EDDS composite | −1.44 | .31 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDE-Q-eating concern | −.70 | .28 | .014 | ||
| PD vs. BN | Impulsivity | BEQ-impulse strength | .46 | .28 | .097 | ||
| PD vs. BN | Impulsivity | BIS-11 | −.12 | .28 | .664 | ||
| PD vs. BN | Perfectionism | MPS-concern over mistakes | −.20 | .28 | .470 | ||
| PD vs. BN | Perfectionism | MPS-doubts about actions | −.43 | .28 | .122 | ||
| PD vs. BN | Perfectionism | MPS-personal standards | .03 | .28 | .917 | ||
| PD vs. BN | Purging frequency | −.24 | .28 | .382 | |||
| PD vs. BN | Restraint | TFEQ-disinhibition | −1.74 | .32 | <.001 | ||
| PD vs. BN | Restraint | TFEQ-hunger | −1.31 | .30 | <.001 | ||
| PD vs. BN | Restraint | TFEQ-restraint | .10 | .28 | .722 | ||
| PD vs. BN | SBE frequency | −.73 | .28 | .011 | |||
| PD vs. BN | Self-esteem | RSE | .90 | .29 | .002 | ||
| PD vs. Control | Body dissatisfaction | BSQ | 1.77 | .36 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE-Q-shape concern | 2.01 | .38 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE-Q-weight concern | 1.83 | .37 | <.001 | ||
| PD vs. Control | Body dissatisfaction | SATAQ-internalization | 1.55 | .35 | <.001 | ||
| PD vs. Control | Eating psychopathology | EDDS composite | 1.84 | .37 | <.001 | ||
| PD vs. Control | Eating psychopathology | EDE-Q-eating concern | .64 | .31 | .041 | ||
| PD vs. Control | Impulsivity | BEQ-impulse strength | .42 | .31 | .180 | ||
| PD vs. Control | Impulsivity | BIS-11 | .30 | .31 | .327 | ||
| PD vs. Control | Perfectionism | MPS-concern over mistakes | .95 | .32 | .003 | ||
| PD vs. Control | Perfectionism | MPS-doubts about actions | .59 | .31 | .060 | ||
| PD vs. Control | Perfectionism | MPS-personal standards | .53 | .31 | .091 | ||
| PD vs. Control | Restraint | TFEQ-disinhibition | .65 | .31 | .040 | ||
| PD vs. Control | Restraint | TFEQ-hunger | −.08 | .31 | .793 | ||
| PD vs. Control | Restraint | TFEQ-restraint | 1.44 | .35 | <.001 | ||
| PD vs. Control | Self-esteem | RSE | −.67 | .32 | .032 | ||
| Solmi, Hotopf, Hatch, Treasure, and Micali (2016) | PD vs. BED | Anxiety | PTSD | 1.68 | .97 | .084 | |
| PD vs. BED | Substance abuse | AUDIT (Hazardous drinking) | 2.25 | 1.01 | .027 | ||
| PD vs. BED | Suicidality | History of ideation or attempt | 1.32 | .72 | .067 | ||
| PD vs. BN | Anxiety | PTSD | .00 | .64 | 1.000 | ||
| PD vs. BN | Substance abuse | AUDIT (Hazardous drinking) | .89 | .72 | .214 | ||
| PD vs. BN | Suicidality | History of ideation or attempt | .55 | .70 | .437 | ||
| PD vs. Control | Anxiety | PTSD | 2.71 | .82 | .001 | ||
| PD vs. Control | Substance abuse | AUDIT (Hazardous drinking) | 2.54 | .71 | <.001 | ||
| PD vs. Control | Suicidality | History of ideation or attempt | 1.50 | .65 | .021 | ||
| Stice, Marti, and Rohde (2013) | PD vs. BED | Duration of illness | Months | .46 | .35 | .193 | |
| PD vs. BED | Impairment | Functional impairment (Social Adjustment Scale-Self Report for Youth) | −.59 | .35 | .097 | ||
| PD vs. BED | Natural course | % remitted | .09 | .77 | .909 | ||
| PD vs. BED | Suicidality | Suicidality | −.05 | .35 | .886 | ||
| PD vs. BED | Treatment history | Number of visits to mental health providers | −.52 | .35 | .140 | ||
| PD vs. BN | Duration of illness | Months | .87 | .38 | .021 | ||
| PD vs. BN | Impairment | Functional impairment (Social Adjustment Scale-Self Report for Youth) | −.22 | .36 | .546 | ||
| PD vs. BN | Natural course | % remitted | −.49 | .90 | .585 | ||
| PD vs. BN | Suicidality | Suicidality | .04 | .36 | .908 | ||
| PD vs. BN | Treatment history | Number of visits to mental health providers | −.56 | .37 | .127 | ||
| PD vs. Control | Impairment | Functional impairment | .43 | .25 | .086 | ||
| PD vs. Control | Suicidality | Suicidality | 1.36 | .25 | <.001 | ||
| PD vs. Control | Treatment history | Number of visits to mental health providers | .38 | .25 | .130 | ||
| n.s. | PD vs. AN | Duration of illness | Months | −.90 | .55 | .103 | |
| n.s. | PD vs. AN | Impairment | Functional impairment (Social Adjustment Scale-Self Report for Youth) | −.66 | .54 | .222 | |
| n.s. | PD vs. AN | Natural course | % remitted | .87 | .82 | .284 | |
| n.s. | PD vs. AN | Suicidality | Suicidality | .70 | .54 | .200 | |
| n.s. | PD vs. AN | Treatment history | Number of visits to mental health providers | −1.22 | .57 | .031 | |
| Støving et al. (2012) | n.s. | PD vs. AN | Age of onset | (PD group: vomiting and laxatives) | .09 | .25 | .721 |
| n.s. | PD vs. AN | Treatment history | (PD group: vomiting and laxatives) | −.83 | .25 | .001 | |
| Tasca et al. (2012) | AN-bp | PD vs. AN | Anxiety | PAI-anxiety | −.17 | .12 | .159 |
| AN-bp | PD vs. AN | Body dissatisfaction | EDI-body dissatisfaction | .28 | .12 | .023 | |
| AN-bp | PD vs. AN | Body dissatisfaction | EDI-drive for thinness | .08 | .12 | .512 | |
| AN-bp | PD vs. AN | Depression | PAI-depression | −.30 | .12 | .016 | |
| AN-bp | PD vs. AN | Duration of illness | Months | −.04 | .12 | .745 | |
| AN-bp | PD vs. AN | Eating psychopathology | EDI-bulimia | −.39 | .12 | .001 | |
| AN-bp | PD vs. AN | Perfectionism | EDI-perfectionism | −.22 | .12 | .070 | |
| AN-bp | PD vs. AN | Substance abuse | Alcohol problems | .26 | .12 | .035 | |
| AN-bp | PD vs. AN | Suicidality | Suicidal ideation | −.08 | .12 | .494 | |
| AN-bp | PD vs. AN | Treatment outcome | Treatment outcome (no binge purge symptoms for final 4 weeks of program, >=11 weeks of treatment, BMI ≥20) | .27 | .14 | .050 | |
| AN-r | PD vs. AN | Anxiety | PAI-anxiety | .34 | .13 | .007 | |
| AN-r | PD vs. AN | Body dissatisfaction | EDI-body dissatisfaction | .89 | .13 | <.001 | |
| AN-r | PD vs. AN | Body dissatisfaction | EDI-drive for thinness | .66 | .13 | <.001 | |
| AN-r | PD vs. AN | Depression | PAI-depression | .35 | .13 | .005 | |
| AN-r | PD vs. AN | Duration of illness | Months | .43 | .12 | <.001 | |
| AN-r | PD vs. AN | Eating psychopathology | EDI-bulimia | 1.17 | .13 | .000 | |
| AN-r | PD vs. AN | Perfectionism | EDI-perfectionism | .07 | .12 | .589 | |
| AN-r | PD vs. AN | Substance abuse | Alcohol problems | .46 | .13 | <.001 | |
| AN-r | PD vs. AN | Suicidality | Suicidal ideation | .48 | .13 | <.001 | |
| AN-r | PD vs. AN | Treatment outcome | % achieving ’good outcome’ defined by article | .35 | .14 | .011 | |
| PD vs. BN | Anxiety | PAI-anxiety (BN-p) | .21 | .10 | .038 | ||
| PD vs. BN | Body dissatisfaction | EDI-body dissatisfaction (BN-p) | −.05 | .10 | .594 | ||
| PD vs. BN | Body dissatisfaction | EDI-drive for thinness (BN-p) | .03 | .10 | .766 | ||
| PD vs. BN | Depression | PAI-depression (BN-p) | .20 | .10 | .051 | ||
| PD vs. BN | Duration of illness | Months (BN-p) | .09 | .10 | .381 | ||
| PD vs. BN | Eating psychopathology | EDI-bulimia (BN-p) | −1.49 | .11 | .000 | ||
| PD vs. BN | Perfectionism | EDI-perfectionism (BN-p) | .20 | .10 | .058 | ||
| PD vs. BN | Substance abuse | Alcohol problems (BN-p) | −.02 | .11 | .812 | ||
| PD vs. BN | Suicidality | Suicidal ideation (BN-p) | .06 | .11 | .580 | ||
| PD vs. BN | Treatment outcome | % achieving ’good outcome’ defined by article | −.20 | .14 | .152 | ||
| Tobin, Griffing, and Griffing (1997) | PD vs. BED | Anxiety | SCL-90 anxiety (BN-np) | .64 | .27 | .017 | |
| PD vs. BED | Body dissatisfaction | EDI-body dissatisfaction | −.52 | .26 | .043 | ||
| PD vs. BED | Body dissatisfaction | EDI-drive for thinness | .58 | .26 | .023 | ||
| PD vs. BED | Depression | SCL-90 depression | .23 | .26 | .386 | ||
| PD vs. BED | Eating psychopathology | EDI-bulimia | −.69 | .26 | .008 | ||
| PD vs. BED | Perfectionism | EDI-perfectionism | .33 | .25 | .188 | ||
| PD vs. BN | Anxiety | SCL-90 anxiety (BN-np) | −.07 | .29 | .814 | ||
| PD vs. BN | Anxiety | SCL-90 anxiety (BN-p) | .09 | .21 | .655 | ||
| PD vs. BN | Body dissatisfaction | EDI-body dissatisfaction (BN-np) | −.44 | .28 | .119 | ||
| PD vs. BN | Body dissatisfaction | EDI-body dissatisfaction (BN-p) | −.03 | .20 | .887 | ||
| PD vs. BN | Body dissatisfaction | EDI-drive for thinness (BN-np) | −.06 | .28 | .838 | ||
| PD vs. BN | Body dissatisfaction | EDI-drive for thinness (BN-p) | −.09 | .20 | .654 | ||
| PD vs. BN | Depression | SCL-90 depression (BN-np) | −.12 | .29 | .669 | ||
| PD vs. BN | Depression | SCL-90 depression (BN-p) | −.03 | .21 | .875 | ||
| PD vs. BN | Eating psychopathology | EDI-bulimia (BN-np) | −1.18 | .30 | <.001 | ||
| PD vs. BN | Eating psychopathology | EDI-bulimia (BN-p) | −1.04 | .20 | .000 | ||
| PD vs. BN | Perfectionism | EDI-perfectionism (BN-np) | −.07 | .28 | .791 | ||
| PD vs. BN | Perfectionism | EDI-perfectionism (BN-p) | −.10 | .20 | .625 | ||
| Wade (2007) | PD vs. AN | Self-esteem | RSE (unpublished data) | .44 | .27 | .096 | |
| PD vs. BN | Depression | Lifetime depression | −.44 | .29 | .128 | ||
| PD vs. BN | Impulsivity | BIS-11 | −.42 | .25 | .094 | ||
| PD vs. BN | Perfectionism | MPQ-concern over mistakes | −3.10 | .36 | <.001 | ||
| PD vs. BN | Self-esteem | RSE | 1.84 | .29 | <.001 | ||
| PD vs. BN | Suicidality | SSAGA | −5.34 | .50 | <.001 | ||
| PD vs. Control | Impulsivity | BIS-11 | 1.39 | .15 | <.001 | ||
| PD vs. Control | Perfectionism | MPQ-concern over mistakes | 4.10 | .18 | <.001 | ||
| PD vs. Control | Self-esteem | RSE | −5.19 | .20 | <.001 | ||
| PD vs. Control | Suicidality | SSAGA | 6.06 | .21 | <.001 | ||
| Wade, Bergin, Tiggemann, Bulik, and Fairburn (2006) | PD vs. BED | Age of onset | .04 | .23 | .857 | ||
| PD vs. BED | Body dissatisfaction | EDE-shape concern | −.28 | .23 | .229 | ||
| PD vs. BED | Body dissatisfaction | EDE-weight concern | −.29 | .23 | .209 | ||
| PD vs. BED | Eating psychopathology | EDE-eating concern | −.55 | .23 | .018 | ||
| PD vs. BED | Natural course | % asymptomatic | .16 | .26 | .535 | ||
| PD vs. BED | Purging frequency | (unpublished data) | .27 | .26 | .311 | ||
| PD vs. BED | Restraint | EDE-restraint | −.45 | .23 | .051 | ||
| PD vs. BED | SBE frequency | (unpublished data) | −.14 | .26 | .583 | ||
| PD vs. BN | Age of onset | .20 | .25 | .421 | |||
| PD vs. BN | Body dissatisfaction | EDE-shape concern (BN-p) | −.15 | .23 | .515 | ||
| PD vs. BN | Body dissatisfaction | EDE-weight concern (BN-p) | −.29 | .23 | .212 | ||
| PD vs. BN | Eating psychopathology | EDE-eating concern (BN-p) | −.84 | .24 | <.001 | ||
| PD vs. BN | Natural course | % asymptomatic (BN-p) | .36 | .30 | .241 | ||
| PD vs. BN | Purging frequency | (unpublished data) | .04 | .25 | .875 | ||
| PD vs. BN | Restraint | EDE-restraint (BN-p) | −.52 | .23 | .025 | ||
| PD vs. BN | SBE frequency | (unpublished data) | −1.39 | .28 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE-shape concern | .79 | .14 | <.001 | ||
| PD vs. Control | Body dissatisfaction | EDE-weight concern | .75 | .14 | <.001 | ||
| PD vs. Control | Eating psychopathology | EDE-eating concern | .26 | .14 | .068 | ||
| PD vs. Control | Restraint | EDE-restraint | .50 | .14 | <.001 | ||
| n.s. | PD vs. AN | Age of onset | 1.00 | .28 | <.001 | ||
| n.s. | PD vs. AN | Body dissatisfaction | EDE-shape concern (unpublished data for full criteria AN group) | .16 | .26 | .536 | |
| n.s. | PD vs. AN | Body dissatisfaction | EDE-weight concern (unpublished data for full criteria AN group) | .12 | .26 | .645 | |
| n.s. | PD vs. AN | Eating psychopathology | EDE-eating concern (unpublished data for full criteria AN group) | .11 | .26 | .685 | |
| n.s. | PD vs. AN | Purging frequency | (unpublished data) | .24 | .29 | .414 | |
| n.s. | PD vs. AN | Restraint | EDE-restraint (unpublished data for full criteria AN group) | .37 | .27 | .168 | |
| n.s. | PD vs. AN | SBE frequency | (unpublished data for full criteria AN group) | −.08 | .29 | .783 | |
| Watson et al. (2013) | PD vs. BED | Natural course | % with no ED diagnosis at follow-up- training sample | .98 | .26 | <.001 | |
| PD vs. BED | Natural course | % with no ED diagnosis at follow-up - validation sample | .98 | .25 | <.001 | ||
| PD vs. BN | Natural course | % with no ED diagnosis at follow-up - BN-p training sample | .90 | .28 | .001 | ||
| PD vs. BN | Natural course | % with no ED diagnosis at follow-up - BN-p validation sample | .97 | .26 | <.001 | ||
| Wolfe, Jimerson, Smith, and Keel (2011) | PD vs. BN | Duration of illness | Months | −.36 | .33 | .270 | |
| PD vs. BN | Purging frequency | .77 | .34 | .022 |
Note. PD = Purging Disorder; AN = Anorexia Nervosa; BN = Bulimia Nervosa; BN-p = BN purging subtype; BN-np = BN nonpurging subtype; BED = Binge Eating Disorder; AN-bp = AN binge-purge subtype; AN-r = AN restricting subtype; N.S.=Not specified; EDE = Eating Disorder Examination; BDI = Beck Depression Inventory; RSE = Rosenberg Self-Esteem Questionnaire; K-SADS = Kiddie Schedule for Affective Disorders and Schizophrenia; BAI = Beck Anxiety Inventory; EDI = Eating Disorder Inventory; SCL-90 = Symptom Checklist 90; BSQ = Body Shape Questionnaire; TFEQ = Three Factor Eating Questionnaire; IDS-SR = Inventory of Depressive Symptoms-Self Report; PHQ = Patient Health Questionnaire; EAT = Eating Attitudes Test; SATAQ = Sociocultural Attitudes Towards Appearance Scale; MPS = Multidimensional Perfectionism Questionnaire; SAS-SR = Social Adjustment Scale-Self Report for Youth; PAI = Personality Assessment Inventory; CPRS = Comprehensive Psychiatric Rating Scale; MASC Multidimensional Anxiety Scale for Children-10; CDI = Children’s Depression Inventory; DEBQ = Dutch Eating Behavior Questionnaire; Barratt Impulsiveness Scale-11; IBS = Impulsive Behavior Scale; MRFS-IV = McKnight Risk Factors Survey IV; PAI = Personality Assessment Inventory; SSAGA = Semi-structured Assessment for the Genetics of Alcohol; AUDIT = Alcohol Use Disorders Identification Test; PTSD = Post-traumatic Stress Disorder; DAST = Drug Abuse Screening Test; MAST = Michigan Alcoholism Screening Test; EDDS = Eating Disorder Diagnostic Scale.
BED data were not coded from Eddy et al. (2008) because of the presence of subclinical BED within this group.
Other diagnostic groups were not included from Fink et al. (2009) because of the presence of subclinical disorders within these groups.
Goldschmidt et al. (2016) differentiated between PD with and without loss of control (LOC) eating groups.
PD group was coded from “SBN” group in Keel et al. (2001).
Data for the PD group in Nakai et al. (2013) were unpublished information sent by the first author.
PD Versus Controls
Compared with control groups, PD groups reported higher levels of suicidality, depression, anxiety, impulsivity, substance use, dietary restraint, body dissatisfaction, and eating psychopathology. Large effect sizes were observed for all comparisons with the exception of a small effect for differences in substance use. Although the comparison of suicidality yielded a marginal significance value (p = .050), the effect size was large in magnitude (g = 1.94) and associated with a robust fail-safe N of 583. No comparisons of mortality were available, and limited data were found for comparisons of medical morbidity, quality of life, and functional impairment. Method of diagnosis and purging frequency criteria were investigated as potential moderators of eating psychopathology comparisons, but these variables did not account for significant variability in the effect size.
PD Versus AN
PD groups evidenced a later age of onset, better treatment outcomes, and less treatment history compared with AN groups, with small to medium effects for these comparisons; conversely, PD and AN groups did not differ in duration of illness. PD groups evidenced higher levels of substance use and self-esteem, representing small and medium effects sizes, respectively. With respect to ED constructs, PD groups reported more frequent purging behavior (medium effect size), less frequent SBEs (small effect size), and higher levels of dietary restraint (small effect size). There were no significant differences in suicidality, depression, anxiety, perfectionism, eating psychopathology, or body dissatisfaction. No comparisons of PD and AN on levels of medical morbidity, quality of life, or impulsivity were available, and very few studies were found comparing AN and PD in mortality, impairment, or outcome over the natural course of illness.
PD Versus AN Moderations
Although the overall PD/AN differences in eating psychopathology and body dissatisfaction were nonsignificant, there was a high degree of variability in these effect sizes that warranted investigation of moderators. Differences in eating psychopathology and body dissatisfaction were moderated by the inclusion of SBEs in PD diagnostic criteria, such that the direction of the effect was positive (and statistically significant in the case of body dissatisfaction) when PD criteria allowed SBEs, but negative (and not significant) when SBEs were not specified. Thus, when SBEs were included in the PD diagnostic criteria, PD groups reported significantly greater body dissatisfaction than AN groups.
PD Versus BN
Compared with BN groups, PD groups evidenced a later age of onset and better outcomes over the natural course of illness, with small to medium effects; however, groups did not differ in duration of illness, treatment outcome, or treatment history. With respect to non-ED validators, PD was lower in depression (small effect), impulsivity (medium effect), and perfectionism (small to medium effect), and higher in self-esteem (small to medium effect); however, groups did not differ significantly in suicidality, substance use, or anxiety. Regarding ED-related constructs, compared with BN groups, PD groups evidenced lower frequencies of purging (small effect) and lower levels of eating psychopathology (large effect) and body dissatisfaction (small effect); group differences for restraint and SBE frequencies were nonsignificant. No comparisons of PD and BN in terms of medical morbidity were available, and limited data were found regarding mortality, quality of life, and functional impairment. Although moderators were investigated for comparisons of SBE frequency, depression, anxiety, eating psychopathology, self-esteem, and perfectionism, no moderator emerged as significant for these effects.
PD Versus BED
Compared with BED groups, PD groups evidenced a shorter duration of illness and better natural course outcome, with small to medium effect sizes, but groups did not differ in age of onset. In regards to non-ED domains, groups did not differ in suicidality, depression, anxiety, or perfectionism. In terms of ED-related domains, there were not significant group differences in SBE frequency, eating psychopathology, or body dissatisfaction, though PD groups were higher in restraint (medium effect). Comparisons of PD and BED in mortality, medical morbidity, and quality of life were unavailable, and there were insufficient data for comparisons of impairment, impulsivity, treatment outcome, treatment history, and self-esteem. Moderators were explored for PD/BED comparisons of eating psychopathology, though none emerged as significant.
Publication Bias
We investigated possible publication bias (i.e., the file drawer problem) by calculating the fail-safe N (Rosenthal, 1979) for significant overall effect sizes (see Table 3), which indicates the number of studies with a null effect that would render the observed overall effect nonsignificant; thus, higher values indicate more robust effects. Given the results of these calculations, it is likely that all PD/Control comparisons (fail-safe N’s ranging from 102 to 1,131) are robust. Fail-safe N analyses also demonstrated robust PD/BN differences in eating psychopathology, body dissatisfaction, purging frequency, perfectionism, self-esteem, depression, impulsivity, and age of onset, with fail-safe Ns ranging from 25 to 3,585; however the difference in natural course outcome appeared less reliable (fail-safe N = 10). Fail-safe N analyses for PD/AN comparisons appeared most stable for differences in age of onset, treatment history, treatment outcome, and purging frequency (fail-safe N: 18 to 59), but less so for substance use (fail-safe N = 5) and restraint (fail-safe N = 4), which is likely related to the small number of studies that contributed to these effects (substance use: k = 4; restraint: k = 5). Regarding significant PD/BED effects, the difference in duration of illness appeared more robust (fail-safe N = 23) than the difference in natural course outcome (fail-safe N = 11). Although there is not a clear threshold at which fail-safe N values deem effects uninterpretable because of bias, these values provide perspective regarding the likelihood that publication bias may have influenced results. Thus, interpretations regarding PD/BN and PD/BED differences in natural course outcome, and the PD/AN differences in substance use and restraint, should be made more cautiously.
Discussion
This meta-analysis compared PD with established DSM–5 EDs (i.e., AN, BN, BED) and non-ED controls on indicators of course of illness and severity, including both general and ED-related psychopathology. Specifically, we sought to (a) evaluate the clinical significance of PD, (b) examine the validity of its categorization as an ED, and (c) provide evidence to inform its conceptualization as a distinct ED diagnosis by assessing domains related to predictive and concurrent validity.
PD as a Clinically Significant ED
Although limited data were found on general severity indicators (i.e., mortality, medical morbidity, quality of life, impairment), results provided robust support for the clinical significance of PD, as evidenced by higher levels of suicidality and psychiatric morbidity (i.e., depression, anxiety, substance use, impulsivity) in PD compared with controls. However, the dearth of data on mortality, medical morbidity, quality of life, or impairment in PD highlights the need for future comparisons in these domains. Findings also supported the inclusion of PD in a class of psychiatric disorders that are characterized by ED psychopathology, as demonstrated by higher levels of ED-related psychopathology (i.e., eating psychopathology, restraint, body dissatisfaction) in PD compared with controls. These findings are consistent with previous research (Keel & Striegel-Moore, 2009; Keel et al., 2011) and extend the current literature by providing comprehensive empirical support for conceptualizing PD as a clinically significant ED.
PD Versus Other EDs: Are There Significant Differences in Trajectories of Illness?
In addition, we reported evidence regarding the predictive validity of PD. One question that arises with respect to predictive validity is whether PD has a different trajectory of illness than the full-threshold disorders of AN, BN, and BED. Though the effect sizes were small to medium, findings suggest meaningful differences from AN regarding the trajectory or course of illness, in that AN appears to be associated with an earlier onset, more treatment history, and poorer treatment prognosis. Such findings are in line with prior research documenting low efficacy of treatment (Bulik, Berkman, Brownley, Sedway, & Lohr, 2007) and chronic course (Steinhausen, 2009) in AN. Thus, AN appears to represent a more pernicious ED, which is consistent with the high degree of mortality and medical complications in AN (Arcelus, Mitchell, Wales, & Nielsen, 2011; Mitchell & Crow, 2006).
PD was associated with a better prognosis over the natural course of illness compared with BN and BED, though these effects were based on a relatively small number studies and are in need of further replication. PD groups also had a later age of onset than BN groups and a shorter duration of illness than BED. It may be that the presence of OBEs is related to a more chronic course, as studies have found that upward of 20% of BN cases demonstrate chronicity (Steinhausen & Weber, 2009). With respect to the PD/BED comparisons, the presence of OBEs may be particularly powerful in maintaining the cycle of eating psychopathology for BED as well; furthermore, the presence of purging in PD may be experienced as comparatively more aversive, enhancing the desire to cease such behavior, and potentially contributing to the shorter duration of illness observed in PD versus BED. Interestingly, there were not significant differences between PD and BN with respect to treatment history or treatment outcome, suggesting that these groups may respond similarly to interventions targeting bulimic psychopathology.
PD Versus Other EDs: Are There Significant Differences in Severity of Non-ED and ED-Related Constructs?
This meta-analysis also addressed whether PD differed from AN, BN, and BED on various constructs related to concurrent validity, specifically general and ED-related psychopathology. Results suggested that overall and with a few exceptions, BN groups demonstrated greater severity on these dimensions. Specifically, PD groups experienced lower levels of depression, impulsivity, perfectionism, and higher levels of self-esteem than BN groups; PD groups also evidenced lower levels of eating psychopathology, body dissatisfaction, and less frequent purging. These findings could suggest that these specific domains are more severe in the presence of the OBEs that characterize BN. This is in line with a recent study of BN and PD that found the size of binge episodes explained additional variance in general and ED-related features beyond loss of control, and the relationship between loss of control eating, purging frequency, and depressive symptoms was stronger with larger binge sizes (Forney, Bodell, Haedt-Matt, & Keel, 2016). Furthermore, given suggestions that purging behavior may function to temporarily reduce aversive affective experiences associated with binge eating (Haedt-Matt & Keel, 2011), the lack of OBEs in PD may mitigate one of the primary functions of purging that serves to maintain and potentially exacerbate the behavior in other EDs characterized by OBEs.
Notably, the nonsignificant differences in restraint and SBE frequency provides evidence that individuals with PD and BN do not differ in the degree to which they attempt to restrict their intake and experience episodes of loss of control over eating normal amounts of food. A useful area for future studies would be to assess possible similarities in the antecedents and consequences of purging in PD and BN, as understanding the potential functional nature of purging in PD may further inform its conceptualization in diagnostic systems, as well as its treatment. More specifically, although PD and BN may differ in severity, as the current results suggest, there may be commonalities in the functions of their overlapping symptomatology (e.g., affect regulation).
There were far fewer significant differences between PD and AN and between PD and BED, respectively. PD groups demonstrated significantly higher levels of restraint than both AN and BED groups, though these effects were based on a small number of studies, and thus should interpreted with caution. Nevertheless, the finding that PD was higher in restraint than AN is notable in light of theoretical (Lowe, 1993; Polivy & Herman, 1985) and empirical literature (Elran-Barak et al., 2015; Stice, Davis, Miller, & Marti, 2008) documenting the relationship between restraint, dieting, and binge eating, possibly suggesting those with PD may be more predisposed to develop loss of control eating behavior than those with AN.
At the same time, though based on a limited number of studies, it is also interesting that PD groups reported more frequent purging but less frequent SBEs than AN groups. One possible explanation is that regular purging provides a sense of control over one’s caloric intake, whereas those with AN who do not purge have a stronger or more frequent sense of loss of control associated with eating. However, given that there was an insufficient number of studies to assess AN subtype as a potential moderator of this effect, it is unclear how SBEs and purging in PD compare to AN-r and AN-bp (which is also characterized by purging behavior). With respect to PD/BED differences in restraint, it may be that individuals with PD are more successful in attempting to limit their intake, given the objectively large quantities of food characterizing OBEs in BED.
Implications of Moderators
Although there were insufficient data to assess many of the coded moderators, it is notable that moderations were observed in PD/AN comparisons for which overall effects were nonsignificant. When PD diagnoses allowed for the inclusion of SBEs, PD groups evidenced significantly higher body dissatisfaction and higher (albeit nonsignificant) levels of eating psychopathology than AN groups; however when the inclusion of SBEs was not specified the direction of the effect was reversed, though nonsignificant. Thus, when PD includes loss of control eating behavior, it appears there is a trend for PD to be associated with greater severity in some eating-related symptoms compared with AN.
This finding is interesting in light of previous research documenting that the presence of loss of control eating is associated with impairment regardless of overeating (Forney et al., 2014; Goldschmidt et al., 2008); however, a recent study has suggested that PD was generally similar in psychopathology to other EDs characterized by purging (i.e., AN-bp and BN), regardless of loss of control eating (Goldschmidt et al., 2016). Therefore, the extent to which loss of control eating or purging behavior accounts for differences in degrees of severity between PD and other EDs such as AN is unclear, and future research is needed to assess possible variations in PD/AN differences according to AN subtypes.
Clinical and Theoretical Implications
The aforementioned results regarding general and ED-related validators are clinically meaningful in that they provide information about the course of illness and degree of severity in AN, BN, and BED compared with PD. In line with the Three-Dimensional Model (Williamson, Gleaves, & Stewart, 2005), differences in general and ED-related validators may represent variations along a continuum of psychopathology associated with EDs, though EDs may also differ categorically in some domains (e.g., the presence of OBEs). Notably, a recent factor mixture analysis of bulimic syndromes indicated a single latent severity dimension in combination with three distinct classes, but did not support clear distinctions between BN, PD, and AN-bp. Rather, the majority of PD cases were subsumed with BN and AN-bp cases in a class characterized by purging, weight phobia, and a higher level of comorbidity (Keel et al., 2013). Taken together with the present results, PD may exist along a dimension of severity within bulimic spectrum disorders characterized by loss of control eating and purging behavior. Importantly, the qualitative differences in symptoms characterizing these ED diagnoses and the approach to examining dimensional constructs in this review preclude the ability to make any firm conclusions about categorical diagnostic differences. Thus, the varying degrees of general and ED-related severity across ED diagnoses in the present meta-analysis should be considered in conjunction with inherent qualitative differences in the topography of symptoms and clinically meaningful differences in severity of EDs, both of which are fundamental to establishing diagnostic validity.
Although the analytic approach of this meta-analysis could not evaluate possible taxonic distinctions between PD and other EDs, the present results nevertheless have clinical utility and provide information that may inform future classification research. First, it is clear that PD is a clinically significant ED that warrants intervention, though little research thus far has focused on the treatment of PD. Second, there are meaningful differences in severity indicators (i.e., predictive and concurrent validity) that could suggest there is clinical utility in distinguishing PD from other EDs. Specifically, PD was associated with a better prognosis compared with other EDs and lesser severity of symptoms compared with BN. This information may allow clinicians to more clearly conceptualize PD, and thus may provide guidance for interventions and treatment planning.
Results also highlighted the potential importance of loss of control eating (both SBEs and OBEs) and purging as possible indicators of severity as well as qualitative differences in symptomatology among EDs. Given that SBEs were evidenced by all ED groups, loss of control over eating could be a transdiagnostic symptom that varies in frequency but not in presence. Thus, SBEs may be a general indicator of severity, which has been supported by previous research (Forney et al., 2014). This was evidenced by PD/AN moderation analyses in the present study, as well as research documenting associations between loss of control eating and indicators of general and ED-related severity (Forney et al., 2014).
It is also notable that PD was associated with more frequent purging than AN but less than BN, which is likely related to the inclusion of both AN-r (which is not associated with purging) and AN-bp in AN comparison groups. Although the presence of regular purging behavior signifies a qualitative difference between some diagnoses (i.e., PD and BED, and PD and AN-r), the frequency of purging, like SBE frequency, may also be an indicator of severity across purging-type disorders, which is in line with previous empirical classifications (Keel et al., 2013) and findings demonstrating associations between loss of control eating and purging frequency (Forney et al., 2016). However, because it was not possible to assess AN subtypes as moderators of differences in purging frequencies in the present study, further research is needed to compare AN-bp, PD, and BN in purging frequency and its relationship to the severity of associated symptoms.
Given the finding that BN was associated with more severe general and ED-related symptoms than PD, the presence of OBEs (i.e., the qualitatively distinct symptom in BN compared to PD) could also be conceptualized as an indicator of severity. Therefore, the binge size criterion may be important to retain in diagnostic systems to distinguish among EDs, as it appears to yield clinically useful information regarding the severity of symptomatology. Furthermore, given that the frequency of purging was higher in BN than in PD in the present study, this suggests that the combination of OBEs and more frequent purging together may signify a more severe clinical presentation. It is also notable that in previous research, larger binge size was related to more frequent purging among individuals with BN and PD who experienced relatively higher frequencies of loss of control eating, while at lower frequencies of loss of control this relationship was not observed (Forney et al., 2016). This may seem somewhat inconsistent with the present finding that BN and PD groups did not differ in SBE frequencies, though loss of control in the previous study included both SBEs and OBEs. Thus, given that individuals with BN can experience both OBEs and SBEs, it is possible they experience relatively more frequent loss of control compared with PD, which appears to be associated with both more purging and larger binge episodes.
Limitations
The current study represents the most comprehensive meta-analysis of PD studies to date. However, although the meta-analytic approach was a particular strength of this investigation, the findings are not without limitations. There were limited data on moderators and several validators, particularly for important variables (e.g., mortality, medical morbidity) that could potentially distinguish PD from other EDs. There were not sufficient data to systematically assess the PD diagnostic criteria, which would be beneficial for future studies to explore in greater depth. There is a clear need for future research to be more explicit when defining PD, which may allow for subsequent evaluation of these criteria, particularly those proposed within the literature (e.g., see Keel & Striegel-Moore, 2009). It should also be noted that many of the analyses were conducted using a limited number of studies; thus, these interpretations should be made cautiously. In addition, the majority of studies included samples consisting of only Caucasian women, and therefore the present findings may not generalize to men or other ethnic groups. Although we compared PD with established DSM–5 ED diagnoses, the majority of studies reviewed were based on DSM–IV diagnoses, which raises questions as to whether diagnostic groups were consistent across studies. Furthermore, we were not able to include newly introduced DSM–5 diagnostic categories, such as Avoidant/Restrictive Food Intake Disorder, other types of OSFED (e.g., atypical AN, BN with low frequency and/or duration), or UFED.
Conclusions and Future Directions
Despite the aforementioned limitations, the present meta-analysis revealed that the literature on PD continues to grow. The present findings support PD as a clinically significant ED characterized by substantial comorbidity and severity that is on par with some full-threshold ED diagnoses (i.e., AN and BED), but is less severe than BN in most domains. With respect to the predictive validity of PD as a diagnostic category, PD appears to be associated with a better prognosis compared with full-threshold EDs. Our findings also suggest that the frequency of SBEs could be investigated as a severity indicator across ED diagnoses, whereas purging frequency and the presence of OBEs warrant consideration as severity indicators within bulimic spectrum disorders, though further research is necessary to evaluate this conceptualization.
Notably, the differences observed between PD and other EDs in terms of severity and course of illness may have clinical utility in characterizing PD in relation to other ED diagnoses. However, given that the statistical approach of this meta-analysis precluded evaluation of categorical differences, it is yet unclear whether PD is a qualitatively distinct disorder from BN and other bulimic spectrum disorders such as AN-bp that are characterized by loss of control eating and purging behaviors, as both of these symptoms were observed in PD to varying degrees. As such, future taxometric and factor mixture analyses are needed to assess the categorical and dimensional nature of symptoms seen in PD and other EDs, particularly with respect to SBEs and purging behaviors. Doing so could inform revisions to future classification systems that account for both categorical and dimensional heterogeneity in EDs, as both of these domains are important to consider when characterizing diagnostic entities. Such classification approaches may provide clinicians with diagnostic conceptualizations that have greater clinical utility. Finally, the lack of data for many validators examined here also demonstrated a clear need for continued investigation of constructs related to course, outcome, and etiology in PD.
General Scientific Summary.
This review compared Purging Disorder (PD), an eating disorder characterized by purging in the absence of objective binge eating episodes, to other established eating disorder diagnoses. Results showed that there appear to be differences between PD, Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder regarding prognosis, and PD was less severe than Bulimia Nervosa on dimensional measures of general and eating disorder psychopathology. Taken together, thus far evidence suggests that while PD is a clinically significant disorder, it is yet unclear as to whether PD is categorically distinct eating disorder, and research is necessary to more fully address this question.
Acknowledgments
We thank Ross Crosby for assistance with consultation and revisions.
Footnotes
Part of the results of the present study were presented as a poster presentation at the 2014 Association for Behavioral and Cognitive Therapies convention
Both studies reported data on the same sample.
Evidence for etiological validity was also considered as potentially informative of diagnostic validity, but was not included in the present study because of the current lack of such research in PD samples.
The “*” allows for the identification of terms that begin with the same stem but have multiple endings in the PsycINFO search engine.
Contributor Information
Kathryn E. Smith, Neuropsychiatric Research Institute, Fargo, North Dakota
Janis H. Crowther, Department of Psychological Sciences, Kent State University
Jason M. Lavender, Neuropsychiatric Research Institute, and Department of Psychiatry and Behavioral Science, University of North Dakota School of Medicine and Health Sciences
References
*Indicates studies included in meta-analyses.
- *.Allen KL, Byrne SM, Oddy WH, Crosby RD. DSM-IV-TR and DSM-5 eating disorders in adolescents: Prevalence, stability, and psychosocial correlates in a population-based sample of male and female adolescents. Journal of Abnormal Psychology. 2013a;122:720–732. doi: 10.1037/a0034004. [DOI] [PubMed] [Google Scholar]
- *.Allen KL, Byrne SM, Oddy WH, Crosby RD. Early onset binge eating and purging eating disorders: Course and outcome in a population-based study of adolescents. Journal of Abnormal Child Psychology. 2013b;41:1083–1096. doi: 10.1007/s10802-013-9747-7. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th. Washington, DC: Author; 2000. text rev. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- Arcelus J, Mitchell AJ, Wales J, Nielsen S. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Archives of General Psychiatry. 2011;68:724–731. doi: 10.1001/archgenpsychiatry.2011.74. http://dx.doi.org/10.1001/archgenpsychiatry.2011.74. [DOI] [PubMed] [Google Scholar]
- *.Binford RB, le Grange D. Adolescents with bulimia nervosa and eating disorder not otherwise specified-purging only. International Journal of Eating Disorders. 2005;38:157–161. doi: 10.1002/eat.20167. http://dx.doi.org/10.1002/eat.20167. [DOI] [PubMed] [Google Scholar]
- Borenstein M, Hedges L, Higgins J, Rothstein H. Comprehensive meta-analysis: Version 3.0. Englewood, NJ: Biostat; 2014. [Google Scholar]
- *.Brown TA, Haedt-Matt AA, Keel PK. Personality pathology in purging disorder and bulimia nervosa. International Journal of Eating Disorders. 2011;44:735–740. doi: 10.1002/eat.20904. http://dx.doi.org/10.1002/eat.20904. [DOI] [PubMed] [Google Scholar]
- Bulik CM, Berkman ND, Brownley KA, Sedway JA, Lohr KN. Anorexia nervosa treatment: A systematic review of randomized controlled trials. International Journal of Eating Disorders. 2007;40:310–320. doi: 10.1002/eat.20367. http://dx.doi.org/10.1002/eat.20367. [DOI] [PubMed] [Google Scholar]
- Bulik CM, Sullivan PF, Kendler KS. An empirical study of the classification of eating disorders. American Journal of Psychiatry. 2000;157:886–895. doi: 10.1176/appi.ajp.157.6.886. [DOI] [PubMed] [Google Scholar]
- Crowther JH, Armey M, Luce KH, Dalton GR, Leahey T. The point prevalence of bulimic disorders from 1990 to 2004. International Journal of Eating Disorders. 2008;41:491–497. doi: 10.1002/eat.20537. http://dx.doi.org/10.1002/eat.20537. [DOI] [PubMed] [Google Scholar]
- *.Darcy AM, Fitzpatrick KK, Manasse SM, Datta N, Klabunde M, Colborn D, Lock J. Central coherence in adolescents with bulimia nervosa spectrum eating disorders. International Journal of Eating Disorders. 2015;48:487–493. doi: 10.1002/eat.22340. [DOI] [PubMed] [Google Scholar]
- *.Davis HA, Holland LA, Keel PK. A preliminary examination of a nonpurging compensatory eating disorder. International Journal Of Eating Disorders. 2014;47:239–243. doi: 10.1002/eat.22191. http://dx.doi.org/10.1002/eat.22191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Eddy KT, Doyle AC, Hoste RR, Herzog DB, le Grange D. Eating disorder not otherwise specified in adolescents. Journal of the American Academy of Child & Adolescent Psychiatry. 2008;47:156–164. doi: 10.1097/chi.0b013e31815cd9cf. [DOI] [PubMed] [Google Scholar]
- Edler C, Haedt AA, Keel PK. The use of multiple purging methods as an indicator of eating disorder severity. International Journal of Eating Disorders. 2007;40:515–520. doi: 10.1002/eat.20416. http://dx.doi.org/10.1002/eat.20416. [DOI] [PubMed] [Google Scholar]
- *.Ekeroth K, Clinton D, Norring C, Birgegard A. Clinical characteristics and distinctiveness of DSM-5 eating disorder diagnoses: Findings from a large naturalistic clinical database. Journal of Eating Disorders. 2013;1:31. doi: 10.1186/2050-2974-1-31. http://dx.doi.org/10.1186/2050-2974-1-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elran-Barak R, Sztainer M, Goldschmidt AB, Crow SJ, Peterson CB, Hill LL, Le Grange D. Dietary restriction behaviors and binge eating in anorexia nervosa, bulimia nervosa and binge eating disorder: Trans-diagnostic examination of the restraint model. Eating Behaviors. 2015;18:192–196. doi: 10.1016/j.eatbeh.2015.05.012. http://dx.doi.org/10.1016/j.eatbeh.2015.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairburn CG. Cognitive-behavioral treatment for bulimia. In: Garner DM, Garfinkel PE, editors. Anorexia and bulimia. New York, NY: Guilford Press; 1985. pp. 160–192. [Google Scholar]
- Fairburn CG, Bohn K. Eating disorder NOS (EDNOS): An example of the troublesome “not otherwise specified” (NOS) category in. DSM–IV. Behaviour Research and Therapy. 2005;43:691–701. doi: 10.1016/j.brat.2004.06.011. http://dx.doi.org/10.1016/j.brat.2004.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Favaro A, Ferrara S, Santonastaso P. The spectrum of eating disorders in young women: A prevalence study in a general population sample. Psychosomatic Medicine. 2003;65:701–708. doi: 10.1097/01.psy.0000073871.67679.d8. http://dx.doi.org/10.1097/01.PSY.0000073871.67679.D8. [DOI] [PubMed] [Google Scholar]
- *.Fink EL, Smith AR, Gordon KH, Holm-Denoma JM, Joiner TE., Jr Psychological correlates of purging disorder as compared with other eating disorders: An exploratory investigation. International Journal of Eating Disorders. 2009;42:31–39. doi: 10.1002/eat.20556. http://dx.doi.org/10.1002/eat.20556. [DOI] [PubMed] [Google Scholar]
- *.Flament MF, Buchholz A, Henderson K, Obeid N, Maras D, Schubert N, Goldfield G. Comparative distribution and validity of DSM-IV and DSM-5 diagnoses of eating disorders in adolescents from the community. European Eating Disorders Review: The Journal of the Eating Disorders Association. 2015;23:100–110. doi: 10.1002/erv.2339. http://dx.doi.org/10.1002/erv.2339. [DOI] [PubMed] [Google Scholar]
- Forney KJ, Bodell LP, Haedt-Matt AA, Keel PK. Incremental validity of the episode size criterion in binge-eating definitions: An examination in women with purging syndromes. International Journal of Eating Disorders. 2016;49:651–662. doi: 10.1002/eat.22508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forney KJ, Haedt-Matt AA, Keel PK. The role of loss of control eating in purging disorder. International Journal of Eating Disorders. 2014;47:244–251. doi: 10.1002/eat.22212. http://dx.doi.org/10.1002/eat.22212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fu R, Gartlehner G, Grant M, Shamliyan T, Sedrakyan A, Wilt TJ, Trikalinos TA. Conducting quantitative synthesis when comparing medical interventions: AHRQ and the Effective Health Care Program. Journal of Clinical Epidemiology. 2011;64:1187–1197. doi: 10.1016/j.jclinepi.2010.08.010. http://dx.doi.org/10.1016/j.jclinepi.2010.08.010. [DOI] [PubMed] [Google Scholar]
- *.Garcia-Campayo J, Sanz-Carrillo C, Ibañez JA, Lou S, Solano V, Alda M. Validation of the Spanish version of the SCOFF Questionnaire for the screening of eating disorders in primary care. Journal of Psychosomatic Research. 2005;59:51–55. doi: 10.1016/j.jpsychores.2004.06.005. [DOI] [PubMed] [Google Scholar]
- *.Goldschmidt AB, Accurso EC, O’Brien S, Kara Fitzpatrick K, Lock JD, Le Grange D. The importance of loss of control while eating in adolescents with purging disorder. International Journal of Eating Disorders. 2016;49:801–804. doi: 10.1002/eat.22525. http://dx.doi.org/10.1002/eat.22525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldschmidt AB, Jones M, Manwaring JL, Luce KH, Osborne MI, Cunning D, Taylor CB. The clinical significance of loss of control over eating in overweight adolescents. International Journal of Eating Disorders. 2008;41:153–158. doi: 10.1002/eat.20481. http://dx.doi.org/10.1002/eat.20481. [DOI] [PubMed] [Google Scholar]
- *.Haedt AA, Keel PK. Comparing definitions of purging disorder on point prevalence and associations with external validators. International Journal of Eating Disorders. 2010;43:433–439. doi: 10.1002/eat.20712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haedt-Matt AA, Keel PK. Revisiting the affect regulation model of binge eating: A meta-analysis of studies using ecological momentary assessment. Psychological Bulletin. 2011;137:660–681. doi: 10.1037/a0023660. http://dx.doi.org/10.1037/a0023660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedges LV. Distribution theory for glass’s estimator of effect size and related estimators. Journal of Educational Statistics. 1981;6:107–128. http://dx.doi.org/10.3102/10769986006002107. [Google Scholar]
- Hedges LV, Pigott TD. The power of statistical tests for moderators in meta-analysis. Psychological Methods. 2004;9:426–445. doi: 10.1037/1082-989X.9.4.426. http://dx.doi.org/10.1037/1082-989X.9.4.426. [DOI] [PubMed] [Google Scholar]
- *.Helverskov JL, Lyng B, Clausen L, Mors O, Frydenberg M, Thomsen PH, Rokkedal K. Empirical support for a reclassification of eating disorders NOS. European Eating Disorders Review. 2011;19:303–315. doi: 10.1002/erv.1067. [DOI] [PubMed] [Google Scholar]
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in Medicine. 2002;21:1539–1558. doi: 10.1002/sim.1186. http://dx.doi.org/10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychological Methods. 2006;11:193–206. doi: 10.1037/1082-989X.11.2.193. http://dx.doi.org/10.1037/1082989X.11.2.193. [DOI] [PubMed] [Google Scholar]
- Keel PK. Eating disorders. Upper Saddle River, NJ: Pearson Prentice Hall; 2005. [Google Scholar]
- Keel PK, Crosby RD, Hildebrandt TB, Haedt-Matt AA, Gravener JA. Evaluating new severity dimensions in the DSM–5 for bulimic syndromes using mixture modeling. International Journal of Eating Disorders. 2013;46:108–118. doi: 10.1002/eat.22050. http://dx.doi.org/10.1002/eat.22050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keel PK, Fichter M, Quadflieg N, Bulik CM, Baxter MG, Thornton L, Crow SJ. Application of a latent class analysis to empirically define eating disorder phenotypes. Archives of General Psychiatry. 2004;61:192–200. doi: 10.1001/archpsyc.61.2.192. [DOI] [PubMed] [Google Scholar]
- *.Keel PK, Haedt A, Edler C. Purging disorder: An ominous variant of bulimia nervosa? International Journal of Eating Disorders. 2005;38:191–199. doi: 10.1002/eat.20179. http://dx.doi.org/10.1002/eat.20179. [DOI] [PubMed] [Google Scholar]
- *.Keel PK, Holm-Denoma JM, Crosby RD. Clinical significance and distinctiveness of purging disorder and binge eating disorder. International Journal of Eating Disorders. 2011;44:311–316. doi: 10.1002/eat.20821. http://dx.doi.org/10.1002/eat.20821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Keel PK, Mayer SA, Harnden-Fischer JH. Importance of size in defining binge eating episodes in bulimia nervosa. International Journal of Eating Disorders. 2001;29:294–301. doi: 10.1002/eat.1021. http://dx.doi.org/10.1002/eat.1021. [DOI] [PubMed] [Google Scholar]
- Keel PK, Striegel-Moore RH. The validity and clinical utility of purging disorder. International Journal of Eating Disorders. 2009;42:706–719. doi: 10.1002/eat.20718. http://dx.doi.org/10.1002/eat.20718. [DOI] [PubMed] [Google Scholar]
- *.Keel PK, Wolfe BE, Gravener JA, Jimerson DC. Co-morbidity and disorder-related distress and impairment in purging disorder. Psychological Medicine. 2008;38:1435–1442. doi: 10.1017/S0033291707001390. http://dx.doi.org/10.1017/S0033291707001390. [DOI] [PubMed] [Google Scholar]
- *.Keel PK, Wolfe BE, Liddle RA, De Young KP, Jimerson DC. Clinical features and physiological response to a test meal in purging disorder and bulimia nervosa. Archives of General Psychiatry. 2007;64:1058–1066. doi: 10.1001/archpsyc.64.9.1058. http://dx.doi.org/10.1001/archpsyc.64.9.1058. [DOI] [PubMed] [Google Scholar]
- Kendell RE. Clinical validity. Psychological Medicine. 1989;19:45–55. doi: 10.1017/s0033291700011016. [DOI] [PubMed] [Google Scholar]
- *.Knoph C, Von Holle A, Zerwas S, Torgersen L, Tambs K, Stoltenberg C, Reichborn-Kjennerud T. Course and predictors of maternal eating disorders in the postpartum period. The International Journal of Eating Disorders. 2013;46:355–368. doi: 10.1002/eat.22088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Koch S, Quadflieg N, Fichter M. Purging disorder: A comparison to established eating disorders with purging behaviour. European Eating Disorders Review: The Journal of the Eating Disorders Association. 2013;21:265–275. doi: 10.1002/erv.2231. [DOI] [PubMed] [Google Scholar]
- Koch S, Quadflieg N, Fichter M. Purging disorder: A pathway to death? A review of 11 cases. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity. 2014;19:21–29. doi: 10.1007/s40519-013-0082-3. [DOI] [PubMed] [Google Scholar]
- *.Le Grange D, Binford RB, Peterson CB, Crow SJ, Crosby RD, Klein MH, Wonderlich SA. DSM-IV threshold versus subthreshold bulimia nervosa. International Journal of Eating Disorders. 2006;39:462–467. doi: 10.1002/eat.20304. [DOI] [PubMed] [Google Scholar]
- Lipsey MW, Wilson DB. Practical meta-analysis. Thousand Oaks, CA: SAGE Publications; 2001. [Google Scholar]
- Lowe MR. The effects of dieting on eating behavior: A three-factor model. Psychological Bulletin. 1993;114:100–121. doi: 10.1037/0033-2909.114.1.100. http://dx.doi.org/10.1037/0033-2909.114.1.100. [DOI] [PubMed] [Google Scholar]
- *.MacDonald DE, Trottier K, McFarlane T, Olmsted MP. Empirically defining rapid response to intensive treatment to maximize prognostic utility for bulimia nervosa and purging disorder. Behaviour Research and Therapy. 2015;68:48–53. doi: 10.1016/j.brat.2015.03.007. [DOI] [PubMed] [Google Scholar]
- *.Marino J. A multi-site comparison of purging-type disorders. Dissertation Abstracts International, Section B: The Sciences and Engineering. 2011:72. [Google Scholar]
- *.Meltzer-Brody S, Zerwas S, Leserman J, Von Holle A, Regis T, Bulik C. Eating disorders and trauma history in women with perinatal depression. Journal of Women’s Health [Serial Online] 2011;20:863–870. doi: 10.1089/jwh.2010.2360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell JE, Crow S. Medical complications of anorexia nervosa and bulimia nervosa. Current Opinion in Psychiatry. 2006;19:438–443. doi: 10.1097/01.yco.0000228768.79097.3e. http://dx.doi.org/10.1097/01.yco.0000228768.79097.3e. [DOI] [PubMed] [Google Scholar]
- Mitchell JE, Pyle RL, Hatsukami D, Eckert ED. What are atypical eating disorders? Psychosomatics: Journal of Consultation and Liaison Psychiatry. 1986;27:21–28. doi: 10.1016/S0033-3182(86)72739-4. http://dx.doi.org/10.1016/S0033-3182(86)72739-4. [DOI] [PubMed] [Google Scholar]
- *.Nakai Y, Fukushima M, Taniguchi A, Nin K, Teramukai S. Comparison of DSM–IV versus proposed DSM–5 diagnostic criteria for eating disorders in a Japanese sample. European Eating Disorders Review. 2013;21:8–14. doi: 10.1002/erv.2203. [DOI] [PubMed] [Google Scholar]
- *.Pisetsky EM, Thornton LM, Lichtenstein P, Pedersen NL, Bulik CM. Suicide attempts in women with eating disorders. Journal of Abnormal Psychology. 2013;122:1042. doi: 10.1037/a0034902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polivy J, Herman CP. Dieting and binging. A causal analysis. American Psychologist. 1985;40:193–201. doi: 10.1037//0003-066x.40.2.193. http://dx.doi.org/10.1037/0003-066X.40.2.193. [DOI] [PubMed] [Google Scholar]
- *.Roberto CA, Grilo CM, Masheb RM, White MA. Binge eating, purging, or both: Eating disorder psychopathology findings from an internet community survey. The International Journal of Eating Disorders. 2010;43:724–731. doi: 10.1002/eat.20770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Roberto CA, Haynos AF, Schwartz MB, Brownell KD, White MA. Calorie estimation accuracy and menu labeling perceptions among individuals with and without binge eating and/or purging disorders. Eating and Weight Disorders. 2013;18:255–261. doi: 10.1007/s40519-013-0035-x. [DOI] [PubMed] [Google Scholar]
- *.Rockert W, Kaplan AS, Olmsted MP. Eating disorder not otherwise specified: The view from a tertiary care treatment center. International Journal of Eating Disorders. 2007;40:S99–S103. doi: 10.1002/eat.20482. [DOI] [PubMed] [Google Scholar]
- Rosenthal R. The ‘file-drawer problem’ and tolerance for null results. Psychological Bulletin. 1979;86:638–641. http://dx.doi.org/10.1037/0033-2909.86.3.638. [Google Scholar]
- Rosenthal R. Writing meta-analytic reviews. Psychological Bulletin. 1995;118:183–192. http://dx.doi.org/10.1037/0033-2909.118.2.183. [Google Scholar]
- *.Smith KE, Crowther JH. An exploratory investigation of purging disorder. Eating Behaviors. 2013;14:26–34. doi: 10.1016/j.eatbeh.2012.10.006. [DOI] [PubMed] [Google Scholar]
- *.Solmi F, Hotopf M, Hatch SL, Treasure J, Micali N. Eating disorders in a multi-ethnic inner-city UK sample: prevalence, comorbidity and service use. Social Psychiatry and Psychiatric Epidemiology. 2016;51:369–381. doi: 10.1007/s00127-015-1146-7. [DOI] [PubMed] [Google Scholar]
- Steinhausen HC. Outcome of eating disorders. Child and Adolescent Psychiatric Clinics of North America. 2009;18:225–242. doi: 10.1016/j.chc.2008.07.013. http://dx.doi.org/10.1016/j.chc.2008.07.013. [DOI] [PubMed] [Google Scholar]
- Steinhausen HC, Weber S. The outcome of bulimia nervosa: Findings from one-quarter century of research. The American Journal of Psychiatry. 2009;166:1331–1341. doi: 10.1176/appi.ajp.2009.09040582. http://dx.doi.org/10.1176/appi.ajp.2009.09040582. [DOI] [PubMed] [Google Scholar]
- Stice E, Davis K, Miller NP, Marti CN. Fasting increases risk for onset of binge eating and bulimic pathology: A 5-year prospective study. Journal of Abnormal Psychology. 2008;117:941–946. doi: 10.1037/a0013644. http://dx.doi.org/10.1037/a0013644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Marti CN, Rohde P. Prevalence, incidence, impairment, and course of the proposed DSM–5 eating disorder diagnoses in an 8-year prospective community study of young women. Journal of Abnormal Psychology. 2013;122:445–457. doi: 10.1037/a0030679. http://dx.doi.org/10.1037/a0030679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Stice E, Marti CN, Shaw H, Jaconis M. An 8-year longitudinal study of the natural history of threshold, subthreshold, and partial eating disorders from a community sample of adolescents. Journal of Abnormal Psychology. 2009;118:587–597. doi: 10.1037/a0016481. http://dx.doi.org/10.1037/a0016481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Støving RK, Andries A, Brixen KT, Bilenberg N, Lichtenstein MB, Hørder K. Purging behavior in anorexia nervosa and eating disorder not otherwise specified: A retrospective cohort study. Psychiatry Research. 2012;198:253–258. doi: 10.1016/j.psychres.2011.10.009. [DOI] [PubMed] [Google Scholar]
- Striegel-Moore RH, Franko DL, Thompson D, Barton B, Schreiber GB, Daniels SR. An empirical study of the typology of bulimia nervosa and its spectrum variants. Psychological Medicine. 2005;35:1563–1572. doi: 10.1017/S0033291705006057. [DOI] [PubMed] [Google Scholar]
- Sullivan PF, Bulik CM, Kendler KS. The epidemiology and classification of bulimia nervosa. Psychological Medicine. 1998;28:599–610. doi: 10.1017/s0033291798006576. [DOI] [PubMed] [Google Scholar]
- *.Tasca GA, Maxwell H, Bone M, Trinneer A, Balfour L, Bissada H. Purging disorder: Psychopathology and treatment outcomes. The International Journal of Eating Disorders. 2012;45:36–42. doi: 10.1002/eat.20893. [DOI] [PubMed] [Google Scholar]
- Thomas JJ, Vartanian LR, Brownell KD. The relationship between eating disorder not otherwise specified (EDNOS) and officially recognized eating disorders: Meta-analysis and implications for DSM. Psychological Bulletin. 2009;135:407–433. doi: 10.1037/a0015326. http://dx.doi.org/10.1037/a0015326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Tobin DL, Griffing A, Griffing S. An examination of subtype criteria for bulimia nervosa. International Journal of Eating Disorders. 1997;22:179–186. doi: 10.1002/(sici)1098-108x(199709)22:2<179::aid-eat10>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- Valentine JC, Pigott TD, Rothstein HR. How many studies do you need? A primer on statistical power for meta-analysis. Journal of Educational and Behavioral Statistics. 2010;35:215–247. http://dx.doi.org/10.3102/1076998609346961. [Google Scholar]
- *.Wade TD. A retrospective comparison of purging type disorders: Eating disorder not otherwise specified and bulimia nervosa. International Journal of Eating Disorders. 2007;40:1–6. doi: 10.1002/eat.20314. http://dx.doi.org/10.1002/eat.20314. [DOI] [PubMed] [Google Scholar]
- *.Wade TD, Bergin JL, Tiggemann M, Bulik CM, Fairburn CG. Prevalence and long-term course of lifetime eating disorders in an adult Australian twin cohort. Australian and New Zealand Journal of Psychiatry. 2006;40:121–128. doi: 10.1080/j.1440-1614.2006.01758.x. http://dx.doi.org/10.1080/j.1440-1614.2006.01758.x. [DOI] [PubMed] [Google Scholar]
- Wade TD, Crosby RD, Martin NG. Use of latent profile analysis to identify eating disorder phenotypes in an adult Australian twin cohort. Archives of General Psychiatry. 2006;63:1377–1384. doi: 10.1001/archpsyc.63.12.1377. [DOI] [PubMed] [Google Scholar]
- *.Wade TD, Fairweather-Schmidt AK, Zhu G, Martin NG. Does shared genetic risk contribute to the co-occurrence of eating disorders and suicidality? International Journal of Eating Disorders. 2015;48:684–691. doi: 10.1002/eat.22421. http://dx.doi.org/10.1002/eat.22421. [DOI] [PubMed] [Google Scholar]
- *.Watson HJ, Von Holle A, Hamer RM, Knoph Berg C, Torgersen L, Magnus P, Bulik CM. Remission, continuation and incidence of eating disorders during early pregnancy: A validation study in a population-based birth cohort. Psychological Medicine. 2013;43:1723–1734. doi: 10.1017/S0033291712002516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williamson DA, Gleaves DH, Stewart TM. Categorical versus dimensional models of eating disorders: An examination of the evidence. International Journal of Eating Disorders. 2005;37:1–10. doi: 10.1002/eat.20074. http://dx.doi.org/10.1002/eat.20074. [DOI] [PubMed] [Google Scholar]
- *.Wolfe BE, Jimerson DC, Smith A, Keel PK. Serum amylase in bulimia nervosa and purging disorder: Differentiating the association with binge eating versus purging behavior. Physiology & Behavior. 2011;104:684–686. doi: 10.1016/j.physbeh.2011.06.025. [DOI] [PMC free article] [PubMed] [Google Scholar]