

Abstract
Background
There has been little progress in adolescent health outcomes in recent decades. Researchers and youth-serving organizations struggle to accurately elicit youth voice and translate youth perspectives into health care policy.
Objective
Our aim is to describe the protocol of the MyVoice Project, a longitudinal mixed methods study designed to engage youth, particularly those not typically included in research. Text messaging surveys are collected, analyzed, and disseminated in real time to leverage youth perspectives to impact policy.
Methods
Youth aged 14 to 24 years are recruited to receive weekly text message surveys on a variety of policy and health topics. The research team, including academic researchers, methodologists, and youth, develop questions through an iterative writing and piloting process. Question topics are elicited from community organizations, researchers, and policy makers to inform salient policies. A youth-centered interactive platform has been developed that automatically sends confidential weekly surveys and incentives to participants. Parental consent is not required because the survey is of minimal risk to participants. Recruitment occurs online (eg, Facebook, Instagram, university health research website) and in person at community events. Weekly surveys collect both quantitative and qualitative data. Quantitative data are analyzed using descriptive statistics. Qualitative data are quickly analyzed using natural language processing and traditional qualitative methods. Mixed methods integration and analysis supports a more in-depth understanding of the research questions.
Results
We are currently recruiting and enrolling participants through in-person and online strategies. Question development, weekly data collection, data analysis, and dissemination are in progress.
Conclusions
MyVoice quickly ascertains the thoughts and opinions of youth in real time using a widespread, readily available technology—text messaging. Results are disseminated to researchers, policy makers, and youth-serving organizations through a variety of methods. Policy makers and organizations also share their priority areas with the research team to develop additional question sets to inform important policy decisions. Youth-serving organizations can use results to make decisions to promote youth well-being.
Keywords: adolescents, text messaging, longitudinal study, mixed methods, health policy
Introduction
Youth are central to every major health problem today [1]. Addressing the health and well-being of youth can influence their attitudes, beliefs, and behaviors that ultimately impact health outcomes throughout their life span [2-8]. For example, behaviors that influence chronic disease such as diet and exercise are developed and reinforced during youth [9-11]. Further, symptoms of mental illness often manifest before age 25 [12,13], and sexual health issues are also prominent during adolescence. Despite the need to influence and improve youth health and behavior, there has been little progress in adolescent health outcomes in recent decades [1,14]. Initiatives to address poor health outcomes have largely been unsuccessful [15-18], likely because they are not informed by the adolescent perspective [1]. Instead, program and policy recommendations rely heavily on the perspectives of adults because youth often exert little autonomy in society and in health care settings [19-21].
Previous efforts to gather the perspectives of youth to investigate adolescent health have employed more traditional quantitative and qualitative data collection methods. For example, studies that have employed quantitative strategies, such as surveys, are challenged by a long turnaround time for collection, analysis, and dissemination [8,22,23]. In other studies, researchers have used qualitative focus groups and individual interviews to understand the contextual experiences of youth, or the how and why particular health problems and phenomena persist. However, sample sizes in qualitative studies are relatively small and therefore hard to scale or make inferences about the broader population that can inform policy [24,25]. Finally, many of these approaches rely on samples from secondary school, university, clinic, or community settings that underrepresent low-income, minority, and out-of-school individuals [3,4]. This suggests that adolescent health research has largely ignored the perspective of diverse groups of youth, limiting a full understanding of the issues facing adolescents and perpetuating health disparities [26,27]. In sum, the quality of data collected about this age group is lacking and translation into clinical practice or policy recommendations may be misguided. Research is needed that engages youth—particularly high-risk youth left out of traditional research—to understand their perspectives on health policies and practices that impact their lives to ultimately improve the health and well-being of youth.
One promising method for engaging youth in research is through text messaging. Studies that employ text messaging support the use of this novel strategy for data collection, concluding that the method is effective, easy to implement, and preferable among low-income communities [28,29]. This method seamlessly integrates into the day-to-day lives of youth, not adding the unnecessary burden of travel or time. In addition, text messaging has also been shown to result in more candid responses than voice interviews, even to sensitive questions [30]. As a result, text messaging offers an innovative, youth-friendly way to significantly increase access to and participation of low-income, high-risk, and otherwise excluded populations.
The use of text messaging can also address the problems with more traditional approaches (eg, interviews, surveys, school-based samples) to adolescent research described previously [28,31,32]. Text messaging is used by nearly all adolescents in the United States (97%) and is their preferred mode of communication due to its convenience and efficiency [33,34]. In contrast to quantitative survey methods, which have a long turnaround time and therefore can fail to influence critical or urgent policy decisions, text messaging has the potential to be used for real-time feedback on current health issues [35]. Unlike qualitative approaches such as interviews and focus groups, data collection via text messaging allows for rapid data collection and analysis for a large population-based sample allowing researchers to make generalizations that can inform policy and practice. Finally, rather than relying on school, clinical, or nonrepresentative community samples, text messaging is convenient and accessible to the vast majority of youth.
The MyVoice study was designed in response to calls for “strategic science,” defined as research that addresses gaps in knowledge important to policy decisions. Strategic science is research derived from the reciprocal flow of information between researchers and policy makers, and communicated not only in scholarly publications but also in forms relevant to policymakers [36].
MyVoice collects real-time data from youth via text messaging. The purpose of MyVoice is to harness youth perspectives to connect youth attitudes, beliefs, and behaviors to researchers and policymakers who can bridge the divide between youth and youth-centered policies. The aim of this paper is to describe the research protocol used to engage youth in an ongoing longitudinal research study to investigate youth perspectives on health and well-being. In addition, plans for dissemination of findings to inform policies that impact youth are described.
Methods
Overview
MyVoice uses a longitudinal mixed methods research design [37] to gain insight into youth perspectives on health, health care policy, and related issues important to the well-being of adolescents and young adults (see Figure 1). We seek to gain insight into matters that impact young people by gathering the voices of those directly affected by programs and policies—youth themselves. Each week, we will ask youth to respond to quantitative and qualitative survey questions via text message. The results will be quickly analyzed in real time and disseminated to youth, community members, academic researchers, and policymakers. In this way, the perspectives of youth can be central to the decisions made by community organizations, program directors, researchers, and lawmakers.
Figure 1.
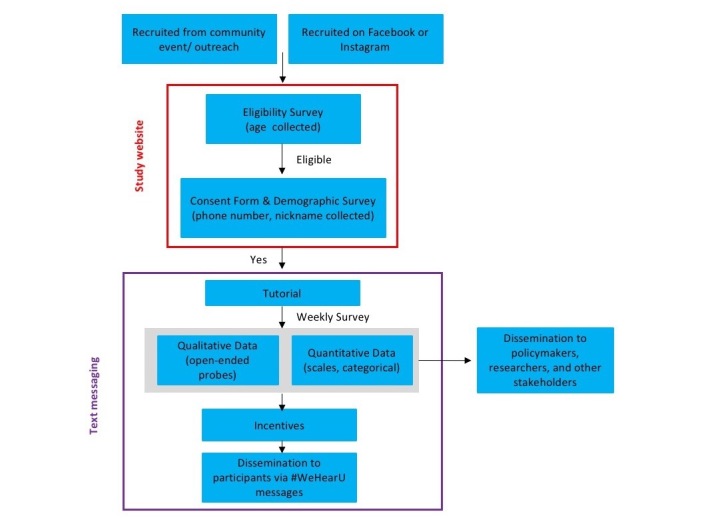
MyVoice research study design.
We assembled an interdisciplinary team of clinicians, academic investigators, methodologists, policymakers, and youth to bring together clinical, topical, methodological, and lived experiences relevant to youth health. The research team includes high school and college students to ensure that youth perspectives are incorporated into the full research process [38,39]. Youth research team members take on leadership roles, participate in decision-making processes, lead and support manuscript writing, generate research questions, support data collection and analysis, and create dissemination strategies. This study has been approved by the University of Michigan Institutional Review Board (HUM00119982).
Project Development and Timeline
The MyVoice study has been iteratively developed through a yearlong pilot study from June 2016 to June 2017. The first phase of pilot testing was used to understand how to recruit and maintain a racially and economically diverse sample, and how to maximize the user experience for participants. The first phase was tested with 114 individuals and revealed key insights that were applied to improve the project. For example, we collected quantitative and qualitative evaluation data about recruitment and consenting procedures, participant preferences for style and content of questions, and technical glitches encountered while participating in the pilot phase. Although the full findings of the pilot evaluation are beyond the scope of this protocol, results were used to make the following changes to the study design: (1) focusing questions on political topics and current events, (2) waiving parental consent for participants younger than age 18 years, (3) addressing technical issues with the text messaging platform, and (4) using targeted advertisement to meet sampling quotas for demographics.
The next phase aims to enroll a national population-based sample of approximately 1000 participants. To date, MyVoice has enrolled approximately 800 participants and is nearing quota goals for all demographics.
Recruitment
Youth are recruited in person, at community and youth-centered events, and online via Facebook and Instagram advertisements. Recruiting on Facebook and Instagram is an effective way to reach populations not traditionally reached through research because Facebook is used by 71% of adolescents and more likely to be used by teens that are from disadvantaged households [40]. Facebook and Instagram allows for targeted recruitment of specific populations, including low-income, minority youth, and youth not in high school or college. Eligibility criteria include age 14 to 24 years, ability to read and communicate in written English, and use of a phone with text messaging capabilities. Phones with text message capabilities from any operating system and carrier are able to participate. If eligible, consent is obtained from participants and parental consent is not required. Participants are only asked to report their nickname and their cell phone number, which is used only to send weekly surveys but are removed from the dataset before analysis to ensure confidentiality. At the time of enrollment, participants are sent a link to an online demographic survey (see Table 1). Demographic survey items include validated measures for gender, race, zip code, highest level of education, highest level of parent/guardian education, and an age-appropriate measure of socioeconomic status. Participants receive weekly surveys until they actively unenroll or when they reach age 25 years.
Table 1.
MyVoice demographic survey completed on enrollment.
| Question | Response options | ||
| What is your date of birth? Please enter it in the following format: mm/dd/yyyy. | Open-ended | ||
| What is your cell phone number? Please enter in the following format: 1 555 555 5555 | Open-ended | ||
| What is your gender? | Male; female; transgender (FTM); transgender (MTF); nonbinary; other (please specify) | ||
| What is your race? Check all that apply. | American Indian or Alaska Native; Asian; black or African American; Native Hawaiian or other Pacific Islander; white or Caucasian; other (please describe) | ||
| Are you Hispanic or Latino? | Yes; no | ||
| What zip code do you live in? | Open-ended | ||
| What is the highest level of education you have achieved? | Eighth grade or less; some high school; high school graduate; some vocational/technical training; completed vocational/technical training; some college; completed an associate’s degree; completed a bachelor’s degree; some graduate school; completed a master’s degree; some graduate training beyond a master’s degree; completed a doctoral degree | ||
| What is the highest level of education any parent/guardian has achieved? | Eighth grade or less; some high school; high school graduate; some vocational/technical training; completed vocational/technical training; some college; completed an associate’s degree; completed a bachelor’s degree; some graduate school; completed a master’s degree; some graduate training beyond a master’s degree; completed a doctoral degree | ||
| Who do you live with most of the time? | My parent(s)/guardian(s); my aunt/uncle; my kids; in a dorm; in apartment or house with other people, not family; in a fraternity/sorority; I live alone; other; my spouse, partner, or significant other | ||
| How many people are in your immediate family? (Include you, any parents/guardians, siblings, step-siblings, etc) | 1-3; 4-6; 7-10; ≥10 | ||
| What is your parent(s)/guardians’ current marital status? | Married; together but not married; separated; divorced; widowed; unsure | ||
| How did you hear about MyVoice? | From a family member; from a friend; Facebook; Instagram; other | ||
| Socioeconomic status measure for respondents under age 18 (version received determined by participant’s date of birth) | |||
| Thinking about the house you live in at the moment, do your parents own it or rent it? (If they have a mortgage, tick “they own it”) | They own it; they rent it; I don’t know | ||
| Do you have a car or van at home? | Yes, one car or van; yes, more than one car or van; no, we don’t own a car or van | ||
| Which of the following Internet technology devices do you have at home? | Desktop computer; laptop computer; iPad or other tablet; other (please specify) | ||
| When you were in middle/high school, did you receive free or reduced price school lunch? | Yes; no | ||
| Socioeconomic status measure for respondents age 18 and older (version received determined by participant’s date of birth) | |||
| What is your annual household income? (Just an estimate of the total amount of everyone in your household) | Open-ended | ||
Sampling
Quota sampling is used to achieve a population-based sample of youth participants. Recruited samples are matched with demographic characteristics of a national sample of youth aged 14 to 24 years. Facebook advertisements are created to target specific demographic characteristics, including age, gender, race/ethnicity, education, family income, and region of the country using weighted samples from the most recent American Community Survey. Creating a national sample of youth requires regular monitoring of participant demographics and tailoring online advertisements to meet predetermined quotas. Specifically, the study team is (1) opening recruitment on Facebook and Instagram and conducting weekly checks of participant demographics currently enrolled; (2) adjusting Facebook and Instagram recruitment advertisements to meet benchmarks, such as pausing advertisements targeting groups that have met the benchmark while increasing advertisements targeting populations that have not met the benchmark; and (3) continuing recruitment until all benchmarks are met and the sample is adequately powered for quantitative calculations.
Incentives
Modest incentives are provided for participation throughout the study. Participants receive a one-time US $5 incentive for completing the online demographic survey on the study website following enrollment in the study. For the weekly surveys, participants receive US $1 for each completed survey. Every 12 weeks, participants also receive a US $3 bonus if all 12 weekly surveys are completed (total incentive of US $15 every 12 weeks for completed surveys). MyVoice also offers occasional “bonus” questions to elicit perspectives on time-sensitive policy issues. Participants receive an additional US $1 for completion of each bonus survey.
Longitudinal Engagement
Based on our iterative pilot phases, we developed three primary strategies beyond the incentives described previously to promote participation and reduce attrition. First, the study design focuses on the perspectives of youth and asks youth to share their experiences. Second, with a goal to better understand and improve the health of youth, we actively generate weekly question sets that address topics that have real-world implications. Third, we regularly disseminate results to the youth participants, through infographics, summaries of findings, or select quotations (see Dissemination for more detail).
Question Development
Generating
In weekly MyVoice research team meetings, upcoming topics are identified and discussed. A research question is identified to structure each week’s question set. Each week of questions focuses on one topic or issue identified by the MyVoice team, external youth-serving organizations, researchers, or policy makers. Topics are selected that align with upcoming policy priorities or timely policy concerns specific to the health of youth. In pilot testing, topics that have been fielded included stress, weight, nutrition, substance use, health insurance, relationships, and sexual health education.
Writing
Weekly text message surveys consist of three to five questions. Although topics and question structure varied, we include closed- and open-ended questions that assess the knowledge, attitudes, and beliefs of study participants. During team meetings, we revise questions to maximize comprehension, appropriateness for youth, and adherence to the research question. The team also discusses how to structure the questions to optimize the use of the text messaging platform.
Piloting
Once written and edited by the research team, weekly surveys are sent to a pilot team of youth, community members, survey experts, methodologists, and topical experts. Participants in the pilot-testing sample provide feedback regarding topics, sentence structure, phrasing, and word choice. The research team makes modifications to weekly surveys in response to pilot feedback before data collection.
Data Collection
Tutorial
After participants provide consent/assent via the study website, they receive a text message tutorial that briefly describes the study process (see Figure 2). Participants are reminded that their participation is voluntary, responses are confidential, and any question can be skipped. In addition, the MyVoice tutorial provides a telephone number where study staff can be reached.
Figure 2.
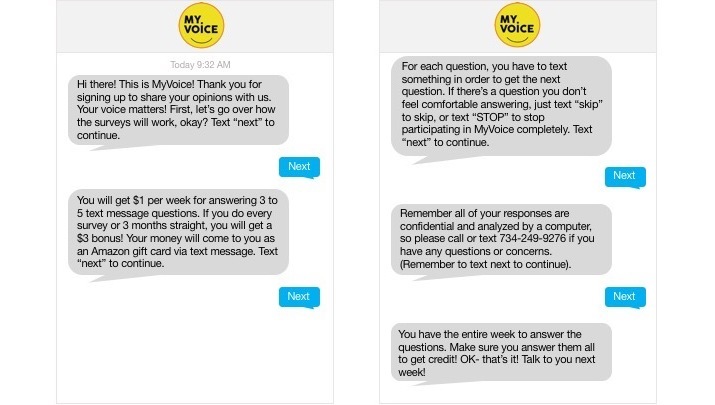
Screenshot of tutorial sent to new participants.
Weekly Survey
Questions are created in 12-week blocks. Textizen is the Web-based platform used to deliver surveys via text message. One-week delays are placed between each weekly question set. Weekly surveys are sent out to participants via Textizen on a consistent day and time.
Question Rating
Each week’s questions are rated by respondents on a scale of 1 to 5 “stars.” Ratings for questions are used to inform future surveys.
Data Analysis
All responses are downloaded as a comma-separated values file. Data analysis depends on the nature of the questions from each weekly survey. Closed-ended and categorical (quantitative) responses are cleaned for case mismatch, spelling variants, and typographic errors to prepare for analysis using descriptive statistics.
For open-ended (qualitative) responses, natural language processing (NLP) techniques are applied to cluster responses. Using NLP, responses are parsed and synonymous words are first grouped into word clusters. These word clusters are further grouped using word similarity measures resulting in semantic word clusters. Our initial analysis of these semantic word clusters shows sufficient agreement with traditional qualitative methods based on manual review and coding responses. Effectiveness of this approach will be reported in a future paper.
Results may be stratified by demographic characteristics to better understand differences and meet the needs of specific stakeholder organizations. For example, responses to surveys may be stratified by age to distinguish between younger (age 14-18 years) and older (age 19-24 years) respondents.
Dissemination
Results will be disseminated to multiple audiences, including academics, policymakers, and youth (see Figure 3). Dissemination products include media/online graphics or GIFs, presentations to community groups, one-page reports, policy briefs, academic presentations, and academic manuscripts. These products are determined by the audience and specific study and content area being disseminated. For example, a lawmaker interested in findings related to beliefs about sexually transmitted diseases may request a one-page infographic to be distributed during community town halls to influence local policy, whereas a study on eating behavior may be reported in a peer-reviewed manuscript.
Figure 3.
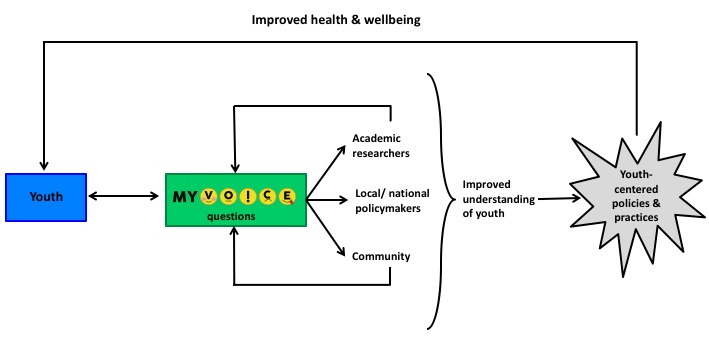
MyVoice dissemination model.
For youth, findings are shared via text message as #WeHearU messages (see Figures 4 and 5). Following data analysis, #WeHearU infographics or narratives are created to build engagement, encourage participation, and share the depth and breadth of responses. We also demonstrate the commitment of the MyVoice team to translate the words of youth into messages for lawmakers and youth-serving organizations by creating and distributing postcards featuring summaries of results or quotes from study participants (see Figure 5).
Figure 4.
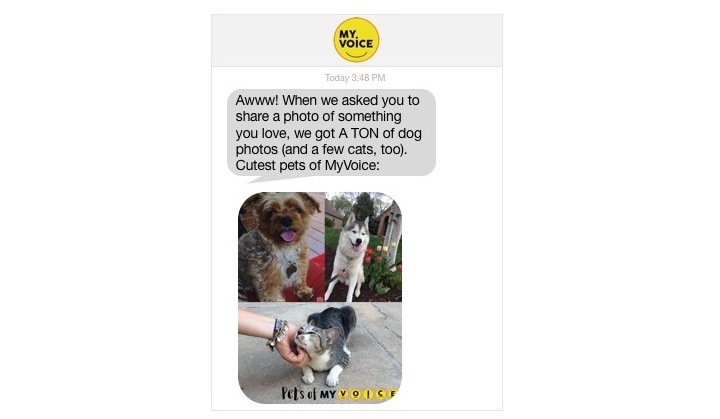
Example of #WeHearU sent to participants.
Figure 5.
Postcard distributed to lawmakers.
Results
We have launched the national study and are currently recruiting and enrolling participants through in-person and online strategies. The MyVoice website is live and enrollment (including consent) and demographic questionnaires are embedded (see Figures 6 and 7). Question development, weekly data collection, data analysis, and dissemination are in progress.
Figure 6.

Screenshot of home page for MyVoice website.
Figure 7.
Embedded enrollment (including consent) form in MyVoice website.
Through the first two phases of pilot testing, we have collected 56 weeks of data from 114 participants. See Textbox 1 for a selection of topics and corresponding question sets sent to participants.
Examples of MyVoice topics and questions.
Police
Intro: Hi, it’s MyVoice! Some people feel safer when police officers are around. Some people feel less safe. How do you feel when police officers are around you?
Q1: There has been news of unarmed people being shot by police. On a scale of 1 to 5 how big of a problem is this? (1=not a big prob; 5=a very big prob)
Q2: Why?
Q3: What are some things that police could do better to keep people safe?
Q4: What have your experiences with police been like?
Q5: Rate this week’s questions (1 through 5)! 1=one star, 5=five stars
Outro: That’s all for this week. Thank you!
Sexually transmitted diseases
Intro: Hi, {{name}}. We are interested in your thoughts about sexually transmitted infections (STIs). If you had an STI, would you tell your sexual partner(s)?
Q1: Why or why not?
Q2: Would it be hard for you to get TESTED for an STI? Why or why not?
Q3: Would it be hard for you to get TREATED for an STI? Why or why not?
Q4: Rate this week’s questions (1 through 5)! 1=one star, 5=five stars
Outro: You’re done for the week, {{name}}! Talk to you next week.
Student debt
Intro: Hi {{name}}! This week’s questions ask your thoughts about college. Whether you are in school or not, we want to hear your opinion. Type “next” to continue.
Q1: What are three things that might make it hard for you to go to college?
Q2: How much student loan debt is ok to have for a college education? Why?
Q3: Should college be free? Why or why not?
Q4: How much do you expect to earn per year in your first full-time job?
Q5: Rate this week’s questions (1-5)! 1=one star, 5=five stars
Outro: Alright, you are finished and made another dollar! We’ll talk to you next week! :)
Limitations
The MyVoice sample is not nationally representative; however, quota sampling allows MyVoice to recruit using a variety of methods while meeting national benchmarks for important demographic characteristics.
Question sets typically only include three to five questions per week and may require repeat longitudinal sampling to get in-depth knowledge (ie, fielding several weeks of questions on the same topic). However mixed methods techniques that integrate qualitative and quantitative data allow us to collect data with a deep understanding of context not attainable in traditional surveys of youth and are collected in a manner that may elicit more truthful responses [30].
Discussion
This study represents a novel example of strategic science that collects youth thoughts and opinions in real time with a goal of disseminating to appropriate change agents at the pace that policy decisions are being made [36].
This study protocol describes a youth-centered method of gathering the beliefs, attitudes, and behaviors of youth in their own words. We know that sustainability of interventions, programs, and policies is dependent on the buy-in of its users. Understanding youth perspectives can allow for the development of youth-centered policies that build on the needs, priorities, and recommendations of those who will be directly affected.
The Department of Health and Human Services Office of Adolescent Health currently lists no ongoing longitudinal qualitative or mixed methods study of youth [41]. As a result, our study is expected to make several methodological contributions. First, we will engage a national population-based sample of youth in a longitudinal mixed methods study of youth that includes voices that are traditionally excluded from research (ie, populations) and policy recommendations.
Second, we have developed a strategy to engage youth over time. Including youth in longitudinal research has been difficult, yet essential, to understanding the health problems we face today [1]. We employ text messaging as an inclusive, comfortable, low-burden mechanism for participation [42,43].
Third, our use of text messaging and NLP allows for real-time data collection, analysis, and dissemination of research findings. The timeline of research (months to years) is typically misaligned with the timeline of policy decision making (weeks to months) [44]. MyVoice bridges this gap by creating a method that better matches the needs of policy makers at all levels with the goal of informing youth-centered policies at all levels.
Finally, our project adds to the growing evidence that participation of advisory groups, peer leaders, and community researchers enhances the quality and reach of research [45-47]. Youth play an active role on our research team. They have an ongoing role in the development of the study, recruitment of participants, data collection and analysis, and dissemination to diverse audiences. Alongside academic researchers, community organizations, and clinicians, youth are encouraged to participate in decision-making processes and take on leadership roles.
Acknowledgments
This research was supported by the University of Michigan MCubed program and the Department of Family Medicine Building Blocks grant. We would like to thank Christina Czuhajewski for contributing design and visual communication expertise and Katie Grode for providing administrative support for this study.
Abbreviations
- NLP
natural language processing
Footnotes
Conflicts of Interest: None declared.
References
- 1.Patton GC, Ross DA, Santelli JS, Sawyer SM, Viner RM, Kleinert S. Next steps for adolescent health: a Lancet Commission. Lancet. 2014 Feb 01;383(9915):385–386. doi: 10.1016/S0140-6736(14)60039-8. [DOI] [PubMed] [Google Scholar]
- 2.Hanson MD, Chen E. Socioeconomic status and health behaviors in adolescence: a review of the literature. J Behav Med. 2007 Jun;30(3):263–285. doi: 10.1007/s10865-007-9098-3. [DOI] [PubMed] [Google Scholar]
- 3.Hawkins JD, Kosterman R, Catalano RF, Hill KG, Abbott RD. Promoting positive adult functioning through social development intervention in childhood: long-term effects from the Seattle Social Development Project. Arch Pediatr Adolesc Med. 2005 Jan;159(1):25–31. doi: 10.1001/archpedi.159.1.25. [DOI] [PubMed] [Google Scholar]
- 4.Irwin L, Siddiqi A, Hertzman C. Early Child Development: A Powerful Equalizer (Final Report) Vancouver, BC: Human Early Learning Partnership (HELP); 2007. [Google Scholar]
- 5.Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A, Currie C. Adolescence and the social determinants of health. Lancet. 2012 Apr 28;379(9826):1641–1652. doi: 10.1016/S0140-6736(12)60149-4. [DOI] [PubMed] [Google Scholar]
- 6.Satterwhite CL, Torrone E, Meites E, Dunne EF, Mahajan R, Ocfemia MC, Su J, Xu F, Weinstock H. Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. Sex Transm Dis. 2013 Mar;40(3):187–193. doi: 10.1097/OLQ.0b013e318286bb53. [DOI] [PubMed] [Google Scholar]
- 7.Decker MR, Peitzmeier S, Olumide A, Acharya R, Ojengbede O, Covarrubias L, Gao E, Cheng Y, Delany-Moretlwe S, Brahmbhatt H. Prevalence and health impact of intimate partner violence and non-partner sexual violence among female adolescents aged 15-19 years in vulnerable urban environments: a multi-country study. J Adolesc Health. 2014 Dec;55(6 Suppl):S58–S67. doi: 10.1016/j.jadohealth.2014.08.022. https://linkinghub.elsevier.com/retrieve/pii/S1054-139X(14)00354-1. [DOI] [PubMed] [Google Scholar]
- 8.Kann L, Kinchen S, Shanklin SL, Flint KH, Kawkins J, Harris WA, Lowry R, Olsen EO, McManus T, Chyen D, Whittle L, Taylor E, Demissie Z, Brener N, Thornton J, Moore J, Zaza S. Youth risk behavior surveillance--United States, 2013. MMWR Surveill Summ. 2014 Jun 13;63 Suppl 4:1–168. http://www.cdc.gov/mmwr/preview/mmwrhtml/ss6304a1.htm. [PubMed] [Google Scholar]
- 9.Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 1998 Mar;101(3 Pt 2):518–525. [PubMed] [Google Scholar]
- 10.Lau RR, Quadrel MJ, Hartman KA. Development and change of young adults' preventive health beliefs and behavior: influence from parents and peers. J Health Soc Behav. 1990 Sep;31(3):240–259. [PubMed] [Google Scholar]
- 11.Mahalik JR, Levine CR, McPherran LC, Doyle LA, Markowitz AJ, Jaffee SR. Changes in health risk behaviors for males and females from early adolescence through early adulthood. Health Psychol. 2013 Jun;32(6):685–694. doi: 10.1037/a0031658. [DOI] [PubMed] [Google Scholar]
- 12.Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry. 2003 Aug;60(8):837–844. doi: 10.1001/archpsyc.60.8.837. [DOI] [PubMed] [Google Scholar]
- 13.Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry. 1998 Jan;55(1):56–64. doi: 10.1001/archpsyc.55.1.56. [DOI] [PubMed] [Google Scholar]
- 14.Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, Arora M, Azzopardi P, Baldwin W, Bonell C, Kakuma R, Kennedy E, Mahon J, McGovern T, Mokdad AH, Patel V, Petroni S, Reavley N, Taiwo K, Waldfogel J, Wickremarathne D, Barroso C, Bhutta Z, Fatusi AO, Mattoo A, Diers J, Fang J, Ferguson J, Ssewamala F, Viner RM. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016 Jun 11;387(10036):2423–2478. doi: 10.1016/S0140-6736(16)00579-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zimmerman RS, Cupp PK, Donohew L, Sionéan CK, Feist-Price S, Helme D. Effects of a school-based, theory-driven HIV and pregnancy prevention curriculum. Perspect Sex Reprod Health. 2008 Mar;40(1):42–51. doi: 10.1363/4004208. [DOI] [PubMed] [Google Scholar]
- 16.Wiehe SE, Garrison MM, Christakis DA, Ebel BE, Rivara FP. A systematic review of school-based smoking prevention trials with long-term follow-up. J Adolesc Health. 2005 Mar;36(3):162–169. doi: 10.1016/j.jadohealth.2004.12.003. [DOI] [PubMed] [Google Scholar]
- 17.Wight D, Raab GM, Henderson M, Abraham C, Buston K, Hart G, Scott S. Limits of teacher delivered sex education: interim behavioural outcomes from randomised trial. BMJ. 2002 Jun 15;324(7351):1430. doi: 10.1136/bmj.324.7351.1430. http://europepmc.org/abstract/MED/12065268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.West SL, O'Neal KK. Project D.A.R.E. outcome effectiveness revisited. Am J Public Health. 2004 Jun;94(6):1027–1029. doi: 10.2105/ajph.94.6.1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.World Health Organization . Adolescent Friendly Health Services: An Agenda for Change. Geneva: World Health Organization; 2002. [Google Scholar]
- 20.Ambresin A, Bennett K, Patton GC, Sanci LA, Sawyer SM. Assessment of youth-friendly health care: a systematic review of indicators drawn from young people's perspectives. J Adolesc Health. 2013 Jun;52(6):670–681. doi: 10.1016/j.jadohealth.2012.12.014. [DOI] [PubMed] [Google Scholar]
- 21.Committee on Adolescence American Academy of Pediatrics Achieving quality health services for adolescents. Pediatrics. 2008 Jun;121(6):1263–1270. doi: 10.1542/peds.2008-0694. [DOI] [PubMed] [Google Scholar]
- 22.Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Hawkins J, Queen B, Lowry R, Olsen EO, Chyen D, Whittle L, Thornton J, Lim C, Yamakawa Y, Brener N, Zaza S. Youth risk behavior surveillance - United States, 2015. MMWR Surveill Summ. 2016 Jun 10;65(6):1–174. doi: 10.15585/mmwr.ss6506a1. [DOI] [PubMed] [Google Scholar]
- 23.Merikangas KR, He J, Brody D, Fisher PW, Bourdon K, Koretz DS. Prevalence and treatment of mental disorders among US children in the 2001-2004 NHANES. Pediatrics. 2010 Jan;125(1):75–81. doi: 10.1542/peds.2008-2598. http://europepmc.org/abstract/MED/20008426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research. 2nd edition. Thousand Oaks, CA: Sage; 2011. [Google Scholar]
- 25.Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001 Aug 11;358(9280):483–488. doi: 10.1016/S0140-6736(01)05627-6. [DOI] [PubMed] [Google Scholar]
- 26.National Research Council . Adolescent Health Services: Missing Opportunities. Washington, DC: National Academies Press; 2009. [PubMed] [Google Scholar]
- 27.Elgar FJ, Pförtner T, Moor I, De Clercq B, Stevens GWJM, Currie C. Socioeconomic inequalities in adolescent health 2002-2010: a time-series analysis of 34 countries participating in the Health Behaviour in School-aged Children study. Lancet. 2015 May 23;385(9982):2088–2095. doi: 10.1016/S0140-6736(14)61460-4. [DOI] [PubMed] [Google Scholar]
- 28.Chang T, Gossa W, Sharp A, Rowe Z, Kohatsu L, Cobb EM, Heisler M. Text messaging as a community-based survey tool: a pilot study. BMC Public Health. 2014;14:936. doi: 10.1186/1471-2458-14-936. http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-14-936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sharp AL, Chang T, Cobb E, Gossa W, Rowe Z, Kohatsu L, Heisler M. Exploring real-time patient decision-making for acute care: a pilot study. West J Emerg Med. 2014 Sep;15(6):675–681. doi: 10.5811/westjem.2014.5.20410. http://escholarship.org/uc/item/5zr8g21f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schober MF, Conrad FG, Antoun C, Ehlen P, Fail S, Hupp AL, Johnston M, Vickers L, Yan HY, Zhang C. Precision and disclosure in text and voice interviews on smartphones. PLoS One. 2015;10(6):e0128337. doi: 10.1371/journal.pone.0128337. http://dx.plos.org/10.1371/journal.pone.0128337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Vyas AN, Landry M, Schnider M, Rojas AM, Wood SF. Public health interventions: reaching Latino adolescents via short message service and social media. J Med Internet Res. 2012 Jul 12;14(4):e99. doi: 10.2196/jmir.2178. http://www.jmir.org/2012/4/e99/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Schnall R, Okoniewski A, Tiase V, Low A, Rodriguez M, Kaplan S. Using text messaging to assess adolescents' health information needs: an ecological momentary assessment. J Med Internet Res. 2013;15(3):e54. doi: 10.2196/jmir.2395. http://www.jmir.org/2013/3/e54/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lenhart A. Pew Research Center. 2015. Aug 06, [2017-07-10]. Teens, technology and friendships: video games, social media and mobile phones play an integral role in how teens meet and interact with friends http://www.pewinternet.org/2015/08/06/teens-technology-and-friendships/
- 34.Porath S. Text messaging and teenagers: a review of the literature. J Res C Educ Technol. 2011;7:86–99. [Google Scholar]
- 35.Park MJ, Paul MT, Adams SH, Brindis CD, Irwin CE. The health status of young adults in the United States. J Adolesc Health. 2006 Sep;39(3):305–317. doi: 10.1016/j.jadohealth.2006.04.017. [DOI] [PubMed] [Google Scholar]
- 36.Brownell KD, Roberto CA. Strategic science with policy impact. Lancet. 2015 Jun 20;385(9986):2445–2446. doi: 10.1016/S0140-6736(14)62397-7. [DOI] [PubMed] [Google Scholar]
- 37.Plano Clark VL, Anderson N, Wertz J, Zhou Y, Schumacher K, Miaskowski C. Conceptualizing longitudinal mixed methods designs. J Mix Method Res. 2014 Jul 21;9(4):297–319. doi: 10.1177/1558689814543563. [DOI] [Google Scholar]
- 38.Israel BA, Schulz AJ, Parker EA, Becker AB, Community-Campus Partnerships for Health Community-based participatory research: policy recommendations for promoting a partnership approach in health research. Educ Health (Abingdon) 2001;14(2):182–197. doi: 10.1080/13576280110051055. [DOI] [PubMed] [Google Scholar]
- 39.Jacquez F, Vaughn LM, Wagner E. Youth as partners, participants or passive recipients: a review of children and adolescents in community-based participatory research (CBPR) Am J Community Psychol. 2013 Mar;51(1-2):176–189. doi: 10.1007/s10464-012-9533-7. [DOI] [PubMed] [Google Scholar]
- 40.Lenhart A. Pew Research Center. 2015. Apr 09, [2017-07-10]. Teens, social media & technology overview http://www.pewinternet.org/2015/04/09/teens-social-media-technology-2015/
- 41.US Department of Health & Human Services Office of Adolescent Health. Evaluation and research https://www.hhs.gov/ash/oah/evaluation-and-research/index.html .
- 42.Maher JE, Pranian K, Drach L, Rumptz M, Casciato C, Guernsey J. Using text messaging to contact difficult-to-reach study participants. Am J Public Health. 2010 Jun;100(6):969–970. doi: 10.2105/AJPH.2009.188391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kew S. Text messaging: an innovative method of data collection in medical research. BMC Res Notes. 2010 Dec 20;3:342. doi: 10.1186/1756-0500-3-342. https://bmcresnotes.biomedcentral.com/articles/10.1186/1756-0500-3-342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lomas J. Words without action? The production, dissemination, and impact of consensus recommendations. Annu Rev Public Health. 1991;12:41–65. doi: 10.1146/annurev.pu.12.050191.000353. [DOI] [PubMed] [Google Scholar]
- 45.Balazs CL, Morello-Frosch R. The three R's: how community based participatory research strengthens the rigor, relevance and reach of science. Environ Justice. 2013 Feb;6(1) doi: 10.1089/env.2012.0017. http://europepmc.org/abstract/MED/24260590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ozer EJ. Youth-led participatory action research: developmental and equity perspectives. Adv Child Dev Behav. 2016;50:189–207. doi: 10.1016/bs.acdb.2015.11.006. [DOI] [PubMed] [Google Scholar]
- 47.Suleiman A, Soleimanpour S, London J. Youth action for health through youth-led research. J Commun Pract. 2006 Jan;14(1-2):125–145. doi: 10.1300/J125v14n01_08. [DOI] [Google Scholar]