

Abstract
The B-HEX® Pupil Expander (Med Invent Devices) is a disposable 6.5 mm flexible hexagonal device with notches at corners and flanges at sides. Alternate flanges with positioning holes are tucked under the iris to engage the notches to the margin of the pupil to provide a 5.5 mm expanded pupil. Unlike devices with scrolls or pockets which require an injector to avoid snagging the incision, the preloaded B-HEX is inserted and removed through a 1 mm or larger incision using a manipulator or 23-gauge micro-forceps. The thin profile and uniplanar design allow unhindered instrument movement during phacoemulsification, cortical cleaning, and intraocular lens implantation. The B-HEX is safely used even after capsulorhexis since the thin uniplanar notches are directly visualized to avoid the capsule margin. It is useful in coaxial phacoemulsification, coaxial sub 2.00 mm micro incision cataract surgery (MICS), biaxial 1.5 mm MICS, femtosecond laser assisted cataract surgery (FLACS), small pupil pars plana vitrectomy, and shallow anterior chamber eyes.
Keywords: B-HEX, intraoperative floppy iris syndrome, iris retractor, non-dilating pupil, pupil expander, small pupil
Phacoemulsification in small pupil eyes is challenging due to reduced workspace and limited visibility. Intraoperative floppy iris syndrome (IFIS) often poses additional challenges. Eyes with preoperative dilated pupil of 7.0 mm or smaller are at risk for IFIS regardless of systemic α-1 adrenergic receptor antagonists treatment.[1] Mechanical devices achieve a consistently large pupil diameter that will not constrict regardless of the IFIS severity or the type of viscosurgical device or fluidic parameters used.[2] To deliver good outcomes, a surgeon should be conversant with the use of pupil expansion devices. This paper presents techniques for a pupil expander which employs a radically different principle from that of existing devices.
The B-Hex® Pupil Expander (Bhattacharjee Ring)
The B-HEX® Pupil Expander [Fig. 1] (Med Invent Devices, Kolkata, India), a third generation Bhattacharjee Ring,[3] is a flexible jointless hexagonal plastic (Polyimide) ring with a 0.075 mm profile having notches and flanges disposed in a single plane. Each disposable 6.5 mm B-HEX provides a 5.5 mm expanded pupil. It is preloaded in a transparent single-use carrier with an ergonomic handle which delivers the device sterile at the incision. The device is inserted, engaged to the pupil margin, and removed using a dull tip micro Sinskey hook manipulator provided in the pack. However, a 23-gauge DSEK forceps provides greater control and speed in all these maneuvers. The flexible notches allow maneuvrability while resilient flanges resist buckling under the compressive force of the nondilating pupil. It is ethylene oxide sterilized and intended for single use. Autoclaving or reuse alters the shape and flexibility affecting performance. Removing the device from the carrier may damage it or render it unsterile.
Figure 1.
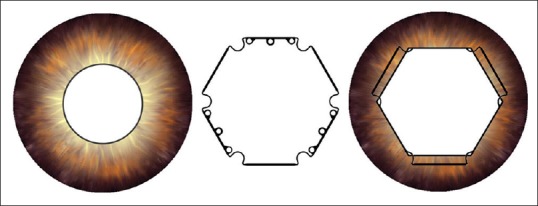
Schematic representation of small pupil, the B-HEX Pupil Expander with notches, flanges and positioning holes and expanded pupil with alternate flanges tucked
Surgical Technique [Videos 1 and 2]
Preparation
A 1.5 mm or larger incision is recommended though the B-HEX can pass through a 1 mm incision. Smaller than 4 mm nonelastic pupils are preferably bimanually stretched to 5 mm before placement of the device. This produces controlled micro-tears of the fibrosed pupil margin and minimizes the manipulations of the B-HEX. Viscoelastic is injected under the pupil margin, and the anterior chamber is kept underfilled. This anterior vaulting of the iris allows flanges to be easily tucked. Overfilling the anterior chamber pushes the iris against the lens rendering tucking of flanges difficult. Viscoelastic is also injected into the B-HEX housing.
Insertion
The apex of the triangular ramp of the carrier is snugly fit into the main incision. The manipulator tip is gently engaged in the positioning hole of the leading notch-flange junction and the B-HEX is advanced through the incision. The elongated configuration as a result of straightening of the notches facilitates easy passage. Pushing a flange across an incision may bend it at an acute angle and kink it. Pushing the manipulator forcefully results in the shaft slipping through the hole. Alternately, a Kuglen hook is engaged to the leading notch-flange junction or a notch-flange junction is held with a 23-gauge micro-forceps to slide the B-HEX through the incision. The slit in the ramp guides the device as it is carried through the incision into the anterior chamber in a single pass and placed on the iris. No attempt is made to tuck the flanges during insertion. The transparent housing allows uninterrupted visibility of the device during its passage through the incision [Fig. 2].
Figure 2.
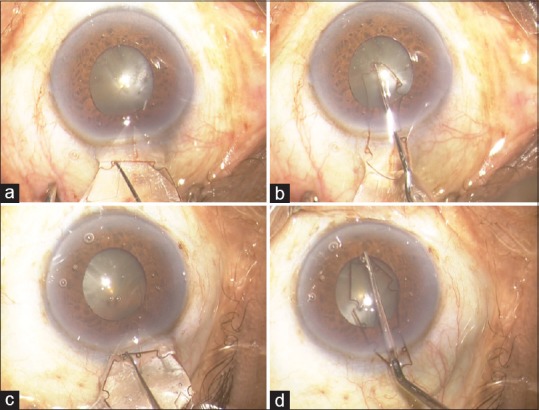
Insertion of B-HEX Pupil Expander; (a and b) with manipulator, (c and d) with Kuglen Hook engaged at the notch-flange junction
Engagement to the pupil margin
Alternate flanges bearing holes are tucked under the iris. The manipulator is engaged in a midflange hole or a 23-gauge forceps is used to draw the flange centrally and tuck it under the pupil margin. Main and side port incisions are used to gain access as required. Fixation of the globe with a forceps or an instrument snugly fit into the side port keeps the eye within the microscope field and provides counter traction. Flanges are drawn just enough to clear the pupil margin and tucked immediately or else entire notches and adjacent flanges go under the iris. After the second flange has been tucked, the partially engaged B-HEX is nudged to a side to bring the third flange centrally making it accessible. The first and second flanges may be initially partially tucked to allow easier access to the third flange. For an inadequately stretched pupil, a bimanual technique is used wherein a Kuglen hook passed between the flange and iris like a tire iron retracts the iris as the flange is tucked. A manipulator trapped between an engaged flange and iris is released by tapping the iris posteriorly with a second instrument. Two Sinskey hooks may be used bimanually to push notches closer or apart to attain a regular hexagon shape [Fig. 3].
Figure 3.
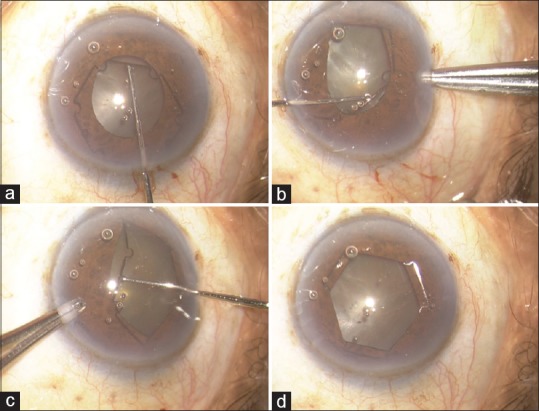
Engagement of B-HEX Pupil Expander; (a) first flange, (b) 2nd flange with fixation of eyeball, (c) 3rd flange with fixation of eyeball, (d) expanded pupil
B-HEX after capsulorhexis
The iris is lifted off the capsular rim with viscoelastic, and the flanges are carefully tucked avoiding the capsulorhexis margin. This is confirmed by pushing the engaged flange toward the periphery and visualizing the free capsulorhexis margin.
Phacoemulsification and intraocular lens implantation
A 5 mm capsulorhexis and nucleus disassembly into small fragments is recommended. Delivering a large hard fragment out of the capsular bag could tear the capsulorhexis or dislodge the ring. The anterior chamber is kept formed with viscoelastic when the phaco or I/A probes exit the eye. Implantation of intraocular lens (IOL) under balanced salt solution irrigation is not recommended as the B-HEX and iris may flutter significantly.
Removal
After IOL implantation, the anterior chamber is topped up with viscoelastic. A manipulator passed through an opposite incision, hooks the flange anterior to the iris and close to the main incision, and draws it centrally to disengage the notches on either side. This flange is held with a McPherson's forceps, and as the B-HEX is drawn out of the eye through the main incision, the trailing notches disengage from the pupillary margin spontaneously. Alternately, the notch-flange junction close to any incision is held with a 23-gauge forceps and moved centrally to disengage two notches and the device is gently pulled out of the incision. Catching the iris inadvertently is avoided as it could result in an iridodialysis. Untucking all flanges and then drawing out the B-HEX is also an option [Fig. 4].
Figure 4.
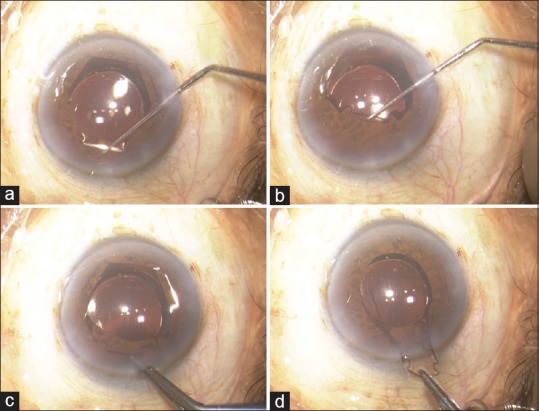
Removal of B-HEX Pupil Expander; (a) hooking the flange, (b) disengaging two notches, (c) flange held with McPherson's forceps, (d) B-HEX drawn out of the incision
Discussion
Increasing diabetic population, liberal use of α-1 antagonists, and other systemic conditions have increased incidence of nondilating pupils and IFIS. Increased patient expectations, surgeon's desire to consistently deliver good outcomes, use of toric and premium lenses, and the availability of user-friendly pupil expanders have reduced the surgeon's threshold to use one.
The scrolls or pockets of some pupil expanders are thick biplanar structures. They snag the self-sealing slit corneal incision during entry and exit and require an injector to circumvent this problem. The B-HEX with all bends at the corners and the supporting elements in a single plane has a thin profile. This is the inventive step.[4] The thin profile and uniplanar design allow it to glide through much smaller incisions without an injector. The B-HEX harmlessly bends the iris and the pupil margin straddles across the plane of the device whereas in other devices, a part of the device straddles across the plane of the pupil margin.
Bimanual stretching of a rigid pupil to 5 mm results in small controlled sphincter tears and helps in placement of a pupil expander. A stiff and bulky device may enlarge a rigid pupil but would be less maneuverable and cause uncontrolled disfiguring sphincter tears and glare.
A 5.5 mm pupil provided by a pupil expansion device is good enough for safe and effective phacoemulsification.[5] A larger expansion requires a larger device which is unwieldy.[5] With present technology and fluidics, an assurance that the expander would maintain a 5.5 mm pupil without collapsing would encourage most surgeons to proceed with phaco surgery. The usable enlarged pupil is usually smaller than the external dimensions of a device. It is important that manufacturers display the size of the expanded pupil achievable rather than the size of the device.
A square pupil produced by four iris hooks led innovators to believe that the square is the best shape for a pupil expander. However, size for size a hexagon is much more efficacious, safe, and practical. Geometrically, between an equal sized square and hexagon having equal incircles, the square has a larger circumcircle. A square device is more likely to injure the angle. Moreover, the space outside the capsulorhexis at the corners is wasted space. When inserted through a small incision, the longer diagonal of the elongated square precludes its complete insertion into the anterior chamber in a single pass.[3,6,7,8]
Through the microscope, the gaps in the scrolls of the Malyugin ring (MicroSurgical Technology, USA) or pockets of the I-Ring (Beaver-Visitec International, USA) are obscured posing difficulty in alignment with the pupil margin. The notches of B-HEX are easily aligned because they are directly visible and entirely in a single plane.[3] This is helpful when used after capsulorhexis.
The Malyugin ring is manually produced, has a glued joint, and requires a disposable injector which increases the cost of production. The B-HEX has a simple uniplanar design which is favorable for rapid and economical machine production.
Conclusion
The B-HEX Pupil Expander is a simple, versatile, safe, user-friendly, and economical device.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Videos Available on: www.ijo.in
Financial support and sponsorship
The study was financially supported by B-HEX Pupil Expanders provided by Med Invent Devices Pvt. Ltd. Kolkata.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Technical help from the following led to improvements in the design and usage techniques of B-HEX: Dr. Arup Bhaumik, Dr. Partha Biswas, Dr. Sri Ganesh, Dr. J S Titiyal, Dr. Mahipal S Sachdev, Dr. Rajesh Fogla, Dr. Ayan Mohanta, Dr. Suhas Haldipurkar, Dr. Rishi Swarup, Dr. Rajesh Joshi, Dr. D Ramamurthy, Dr. Kasu Prasad Reddy, Dr. Mathew Kurian, Dr. Minu Mathen. Dr. Soosan Jacob, Dr. A K Grover, Dr. Kumar Doctor, Dr. Keiki Mehta. Dr. Gaurav Luthra, Dr. Mohan Rajan, Dr. Ajoy Paul, Dr. Somdutt Prasad, Dr. Priya Narang, Dr. CM Wavikar, Dr. Vineet Ratra, Dr. Subhash Prasad, Dr. Saurabh Sanyal and Dr. Arulmozhi Varman.
References
- 1.Casuccio A, Cillino G, Pavone C, Spitale E, Cillino S. Pharmacologic pupil dilation as a predictive test for the risk for intraoperative floppy-iris syndrome. J Cataract Refract Surg. 2011;37:1447–54. doi: 10.1016/j.jcrs.2011.02.030. [DOI] [PubMed] [Google Scholar]
- 2.Chang DF. Use of Malyugin pupil expansion device for intraoperative floppy-iris syndrome: Results in 30 consecutive cases. J Cataract Refract Surg. 2008;34:835–41. doi: 10.1016/j.jcrs.2008.01.026. [DOI] [PubMed] [Google Scholar]
- 3.Bhattacharjee S. Pupil-expansion ring implantation through a 0.9 mm incision. J Cataract Refract Surg. 2014;40:1061–7. doi: 10.1016/j.jcrs.2014.05.003. [DOI] [PubMed] [Google Scholar]
- 4.Bhattacharjee S. Inventor; Device Providing Enlargement and Preventing Collapse of the Pupil of the Eye US Patent Application Publication US 20150351736 A1. [Last accessed on 2017 Jul 23]. Available from: https://www.google.com/patents/US20150351736 .
- 5.Bhattacharjee S. How Large is Just Large Enough. Presented at the XXXIV Congress of the ESCRS at Copenhagen, Denmark. [Last accessed on 2017 Jul 23]. Available from: http://www.escrs.org/Copenhagen2016/programme/posters-details.asp?id=25479 .
- 6.Math Open Reference. Circumcircle of a Polygon. [Last accessed on 2017 Jul 23]. Available from: http://www.mathopenref.com/polygoncircumcircle.html .
- 7.Pupil Expanders-Is Hexagon Better Than Square? [Last accessed on 2017 Jul 23]. Available from: http://www.medinventdevices.com/ophthalmic-surgeon/
- 8.Bhattacharjee S. Forthcoming. New Orleans, USA: 2017. Change the Mindset-Think Hexagon Instead of Square for Pupil Expanders. Accepted for American Academy of Ophthalmology Meeting. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.