

Keywords: nerve regeneration, fingertip replantation, neurological function, microsurgery, hand surgery, anatomy, plastic surgery, blood vessels, neural regeneration
Abstract
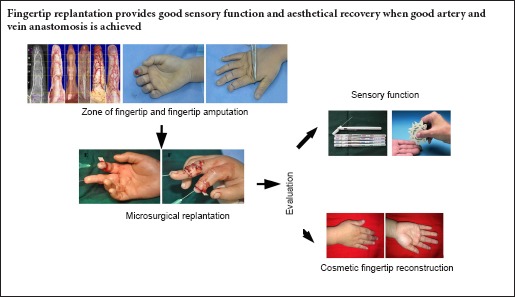
Sensory function is the most significant criterion when evaluating the prognosis of replanted fingers. Current clinical research has focused on surgical techniques and indications for finger replantation; however, few studies have focused on recovery of finger sensory function after replantation. This study retrospectively assessed data of eight patients who had undergone nine Zone I replantations of the fingertips in the First Affiliated Hospital of Sun Yat-sen University of China from July 2014 to January 2016. Variations in the extent of damage, with the residual vessels or nerves in some fingers being too short or even missing, prevented tension-free suture repair in some patients. Thus, repair of four of the nine fingertips included arteriovenous anastomosis, the remaining five undergoing arterial anastomosis during replantation of the amputated fingers. Three patients underwent nerve repair, whereas the remaining six cases did not. Fingertip replantations were successful in all eight patients. Compared with the patients without vascular anastomosis, no obvious atrophy was visible in the fingertips of patients who did undergo vascular anastomosis during replantation and their sensory function did recover. Fingertip replantation provides good sensory function and cosmetic outcomes when good artery and vein anastomoses have been created, even when digital nerves have not been repaired.
Introduction
Komatsu et al. and Tamai et al. reported the first successful digital replantation in 1965 (Masuhara et al., 1967; Komatsu and Tamai, 1968). Over the past 50 years, the limits of digital replantation have been extended by improved instrumentation and establishment of more methodical approaches to teaching microsurgical techniques (Dadaci et al., 2016; Idrissi et al., 2016; Wen et al., 2017). Recent studies have shown high survival rates and excellent functional and aesthetic results. Thus, when managing distal digit injury, most doctors prefer replantation to direct closure or flap transfer (Jazayeri et al., 2013). The survival rate is reportedly 93.3% (Lima et al., 2015; Brown et al., 2017). The replantation procedure represents the pinnacle in the field of hand surgery because the decision to replant a severed part is influenced by many factors, including the importance of the part, the severity of the injury, the expected recovery of function, and the mechanism of injury (Yu et al., 2015). Of these factors, the severity of injury is the most important in determining survival of the replanted digit (Ma et al., 2016). The anatomical structures involved in amputated finger are important in determining the digital replantation strategy. Different sections of human fingers have different anatomical structures and characteristics. To aid in the analysis and study of digital replantation, each digit is divided into six zones on the basis of anatomical details and clinical considerations. Zones I, III, and V involve the bony segments, whereas Zones II, IV, and VI involve the joints of the hand (Figure 1) (Ding and Wang, 2007; Zhu, 2008). Zone I is defined as the fingertip region beyond the proximal 1/5 of the distal phalanx including Zone Ia, which involves the region beyond 1/2 of the distal phalanx, and Zone Ib, which includes the region from the proximal 1/5 to 1/2 of the distal phalanx. Zone Ib harbors the volar digital arteries on the side of the phalanx and the matrix of the fingernail on its back.
Figure 1.
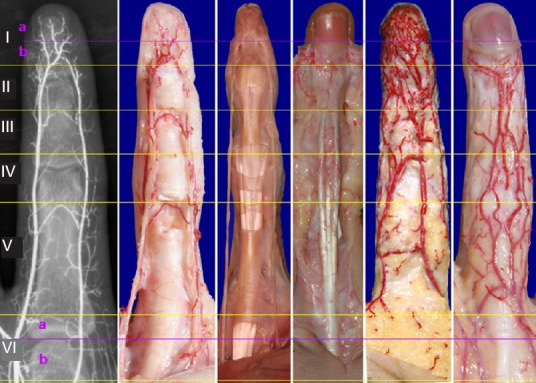
Surgical zones of the fingertip.
On the basis of anatomical features and clinical considerations, each digit is divided into six zones to aid in the analysis and study of digital replantation. Zones I, III, and V include the bony segments, whereas Zones II, IV, and VI include the joints of the hand (Zhu, 2008).
Surgical technique and indications for finger replantation have been discussed (De Frenne and Dhooghe, 1983; Barbary et al., 2013; Engdahl and Morrison, 2015); however, few researchers have focused on cosmetic outcomes and sensory function after replantation of fingers. In this study, the surgical zones of the fingertip (Zone Ia and Zone Ib) were discussed. The aim of this study was to evaluate cosmetic outcomes and sensory function after fingertip replantations at or distal to the nail base and to evaluate the clinical outcomes.
Subjects and Methods
Patients
From July 2014 to August 2015, eight patients (average age, 6.8 years; range, 2–18 years) were included in this study. Patients were included if they met the following criteria: (1) age < 18 years; (2) complete amputation of fingertip; (3) duration of injury < 8 hours; and (4) provision of informed consent by the patient's legal guardians. Exclusion criteria were: (1) age > 18 years; (2) incomplete amputations of fingertips; (3) duration of injury > 8 hours; and (4) inability to comply with treatment, postoperative rehabilitation and follow-up. The eight patients underwent a total of nine Zone I replantations of the fingertip (five boys with six replantations and three girls with one replantation each). Eight amputations were caused by crushing or crushing–avulsion and one by cutting. All injuries were complete amputations involving two thumbs, four index fingers, one middle finger, and two ring fingers. The replantation surgeries were all carried out within 8 hours of injury. The average duration of follow-up period was 9.3 ± 3.5 months (range, 6–15 months).
This study was approved by the Institutional Review Board of the First Affiliated Hospital of Sun Yat-sen University of China (Approval No. [2009]99). Written informed consent was provided by the patients or their legal guardians prior to their participation in the study.
Surgical procedure
Careful debridement of the amputated digit was performed under general anesthesia and with microscopic guidance (magnification of 25× to 30×). The neurovascular bundle was dissected to locate an available vessel in the proximal stump and one artery in the distal stump was identified and tagged for later anastomosis. The bone ends were shortened slightly, or left intact in cases of clean-cut amputations, and the bony fragments fixed with a 5-mL syringe needle (Shanghai Kindly Enterprise Development Group, Shanghai, China) or Kirschner Wire (Yutong Medical Instrument Company, Tianjin, China). Stabilization was achieved by directly suturing the skin where the amputated fingers had very small bone fragments. The selected artery was anastomosed using a 12-0 nylon suture. The vein was also anastomosed with a 12-0 nylon suture (Crownjun KONO, Tokyo, Japan) if a vein had been identified. Otherwise, a fish-mouth incision, either at the pulp tip or opposite to the artery repair side of the pulp, was made to enable controlled bleeding to relive venous congestion.
If possible, neurorrhaphy was performed using one to two sutures. The skin was closed using 5-0 nylon. Heparin (Wanbang Biochemical Pharmaceutical, Jiangsu, China) was continually administered intravenously (6250 IU every 24 hours) for ~3–5 days. After skin closure and wound dressing, a dorsal long-arm splint was used to immobilize the affected extremity.
Cosmetic evaluation
Finger atrophy was evaluated on the basis of the fullness of the injured finger pulp by comparing the appearance of the pulp with that of the contralateral uninjured finger. Finger atrophy was defined as less pulp in the replanted fingertip than the healthy side according to naked eye observation. JHL and YJH were responsible for follow-up of patients.
Evaluation of sensory function
Evaluation of sensory functional included static two-point discrimination (s2PD) tests, which were performed using a Touch-TestTM Two-Point Discriminator (Alimed, Dedham, MA, USA), and Semmes-Weinstein (SW) monofilament examination by a Touch-Test™ Sensory Evaluator (Alimed) (with specifications such as 6.65, 4.56, 4.31, 3.61, and 2.83) (He et al., 2015; Murphy et al., 2017). The evaluation criteria for SW and s2PD used to interpret sensory recovery are shown in Tables 1 and 2, respectively. s2PD was defined as: excellent, ≤ 6 mm; good, 7–15 mm; and poor, ≥ 16 mm (Weber et al., 2000; Meek, 2001; He et al., 2015; Murphy et al., 2017).
Table 1.
Interpretation of monofilament testing of pressure threshold (Weinstein, 1993)
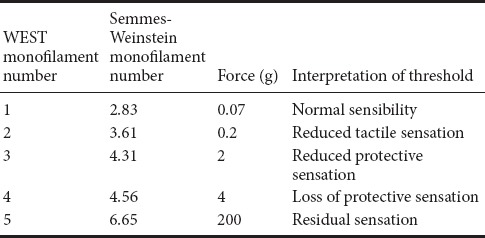
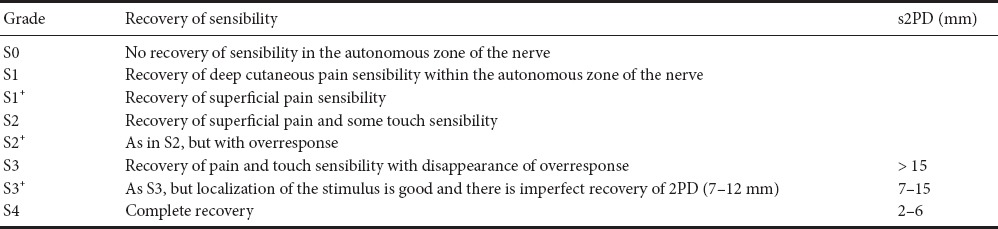
Table 2.
Classification of sensory recovery assessed by static 2-point discrimination (s2PD) test (Glickman and Mackinnon, 1990)
Statistical analysis
Measurement data are presented as mean values. Statistical analysis was performed using SPSS 13.0 software (SPSS, Chicago, IL, USA). Comparisons were performed using the chi-square test. A value of P < 0.05 was considered to denote statistical significance.
Results
Survival rate and functional evaluation
Because the amputated fingertips had been subjected to different severities of trauma, some veins or nerves were either too short or lost to allow repair. Therefore, four of nine fingertips were repaired with vein anastomosis; nerve repair was also performed in three of these. All nine fingertip replantations in the eight patients were successful. All patients reported satisfactory return of sensation based on monofilament examination. In addition, patients 1, 2, and 5 achieved excellent outcomes based on s2PD tests on each finger. The remaining patients were too young to undergo the s2PD sensation test and thus did not undergo this assessment. The results of s2PD and SW monofilament testing are shown in Table 3.
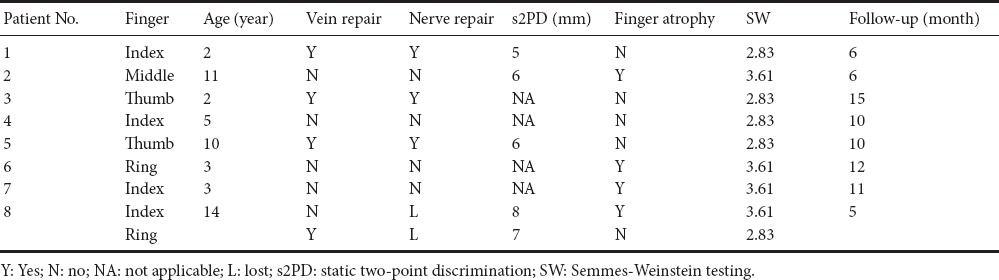
Table 3.
Sensory recovery by s2PD and SW monofilament testing at the last follow-up
Evaluation of cosmetic outcomes
Compared with fingertips without post-injury vein anastomoses (n = 5), replantations reconstructed with such anastomoses (n = 4) showed no obvious atrophy. The difference between these two groups was significant according to the chi-square test (P < 0.05). Two of the four fingertips without vein repair had obvious atrophy. Venous drainage was constructed in three of them to improve blood circulation. However, the fourth had no suitable vein for repair because of the severity of the injury, which was a deep longitudinal cleft in the amputated fingertip. In this case, blood supply we re-established on the radial side. Three months after surgery, the blood circulation of the whole fingertip was adequate. However, the ulnar side of the tip had an insufficient blood supply, resulting in inevitable atrophy of this part. However, the chi-square test showed no significant differences in SW scores between fingertips with (n = 3) or without (n = 6) nerve repair (P > 0.05). Thus, whether or not nerves were repaired, there was satisfactory recovery of sensation according to SW monofilament examination in all replanted fingertips.
Representative cases
Case 1: A 2-year-old boy (No. 7 in Table 3) presented with a twisting injury to the right hand caused by a wheeled machine, resulting in complete amputation at Zone Ib of the index finger. There was rupture of the extensor tendons of the middle finger and a laceration on the dorsal surface of the ring finger and the wound was severely contaminated with machine oil. After thorough debridement, the amputated fingertip was reduced to Zone Ia. An artery distal to the arterial arch of the distal phalanx and one vein were anastomosed to the index finger using 12-0 non-absorbable sutures. A plastic strip (Figure 2E, F) was placed on the anastomosed site. In addition, the extensor tendon rupture of the middle finger was repaired, and the ring finger debrided and stitches inserted (Figure 2). Six months after the procedure, the repaired finger looked good, its pulp lacking any obvious atrophy. The s2PD test showed 5-mm when the SW test result was 2.83.
Figure 2.
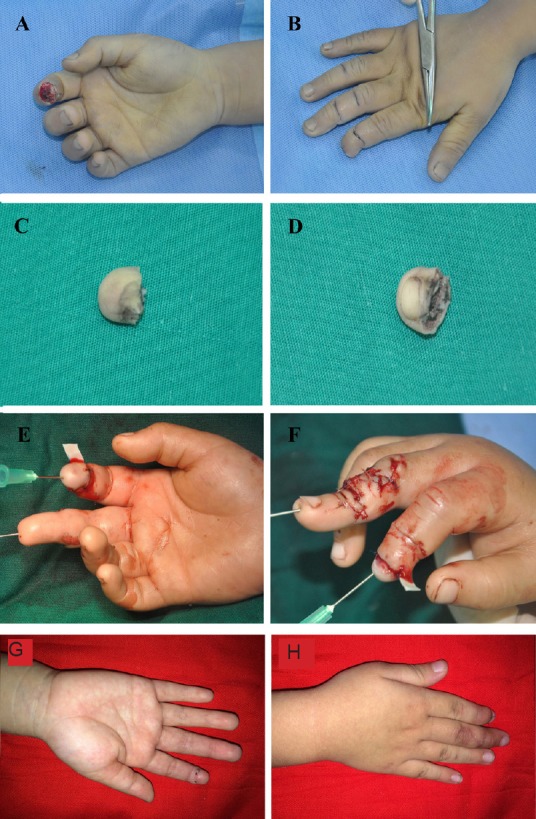
A 2-year-old boy presented with a twisting injury of the right hand caused by a wheeled machine, resulting in complete amputation at Zone Ib of the index finger.
(A) Pre-replantation, ventral view; (B) pre-replantation, dorsal view; (C) ventral view of amputated index; (D) dorsal view of amputated index; (E) post-replantation, ventral view; (F) post-replantation, dorsal view; (G) ventral view six months post-replantation; (H) dorsal view six months post-replantation.
Case 2: A 14-year-old boy (No. 8 in Table 3) presented with an injured left hand caused by a cutting machine, the fingertips of the index and ring fingers having been completely amputated. The wound was contaminated with dark cotton-like fabric and a small amount of an oily substance. After thorough debridement, a single artery distal to the arterial arch of index finger was anastomosed, and one artery distal to the arterial arch and one vein were anastomosed in the ring finger using 12-0 non-absorbable sutures (Figure 3). Six months postoperatively, the pulp of the index finger had atrophied whereas the pulp of the ring finger looked good. s2PD tests of the second and fourth fingers were 8 mm and 7 mm, respectively and SW test results were 3.61 and 2.83, respectively.
Figure 3.

A 14-year-old boy presented with an injured left hand caused by a cutting machine, resulting in amputation of the index and ring fingertips at Zone Ia.
(A) Dorsal view of amputated index fingertip; (B) X-ray film of left hand; (C) dorsal view of left hand 5 months post-operation; (D) ventral view of left hand 5 months post-operation.
Discussion
Reconstruction of the fingertip distal to the flexor tendon insertion by replantation remains controversial and technically challenging although the anatomy of the fingertip has been well-described for surgical planning purposes (Dadaci et al., 2015; Butler et al., 2016; Regmi et al., 2016).
The digital arteries anastomose as palmar arches three times and at least three vessels then radiate longitudinally out from the rounded distal transverse palmar arch to supply the pulp, the central vessel usually having the largest caliber (Scheker and Becker, 2011; Wang et al., 2014). Scholars have classified fingertip injuries into two zones (Yamano, 1985; Kim et al., 2013): (1) the terminal branches from the arcade being classified as Zone I vessels; and (2) Zone II starting proximal to Zone I and continuing to the distal interphalangeal joint. In contrast, Ishikawa et al. (1990) have divided the distal phalanx into four zones.
Although the above classifications have previously been widely used, they have some limitations. The classification by Yamano (1985) and Kim et al. (2013) focuses primarily on arterial damage in a specific plane without considering the level of damage to other severed structures such as the bones and joints. When digital amputations involve a joint structure, there is often poor functional recovery of the severed joint. We consider that Ishikawa et al.'s classification (1990) is overly detailed. Therefore, we here propose a classification based on the amputation level that takes whether the injury involved the finger joints into consideration. On the basis of the anatomical features of the severed fingers, we divide the digits into six zones, Zones I, III, and V including the phalanges and Zones II, IV, and VI including the digital joints. Because Zone I harbors the distal arterial arch, we have further classified it into Zone Ib, which includes the distal arterial arch and the fingernail matrix, and Zone Ia, which begins at a point beyond the distal arterial arch. The surgical strategies and requirements for vascular anastomosis different between Zones Ia and Ib because the arterial arches in Zone Ib are of significantly greater diameter than those of the radiating branches in Zone Ia.
As the digital arteries divide at the level of the distal transverse palmar arch, they inevitably decrease in size from approximately 0.8 mm to as small as 0.3 mm in the radiating branches (Ishikawa et al., 1990; Barbary et al., 2013; Epameinondas et al., 2016). For the same reason, within Zone VI the common palmar digital artery splits into two proper palmar digital arteries at the metacarpophalangeal junction. This is subclassified as Zones VIa and VIb on the basis of the vascular anatomy, which for Zone VIa includes the common palmar digital artery at the metacarpophalangeal junction, and for Zone VIb the dorsal branch of the proximal phalanges.
As previously mentioned, Yamano's classification of finger amputation (1985) does not consider the impact of damage involving the interphalangeal joints, whereas Ishikawa et al.'s classifications (1990) and the similar one of Park et al. (2013) contain excessive detail of little clinical relevance. Our schema provides a digital amputation classification based on the level and extent of digital injury and can facilitate consideration of the options for phase II digital replantation.
Elsewhere, we have presented our approach to restoring a cosmetically pleasing appearance of the reconstructed thumbs or fingers while preserving the function and cosmetic appearance of the donor foot, including detailed discussion of the reconstructive procedures for each degree of digit defect and pitfalls and technical tips (Wang and Sun, 2014; Sun et al., 2015; Balan, 2016).
The most important factor in determining the stratagem for digital replantation surgery is reconstruction and recovery of normal blood circulation in the replanted fingertip (Fakin et al., 2015; Kim and Lee, 2015; Saha et al., 2015; Efanov et al., 2016). Unfortunately, the relevant venous anatomy is variable. At the level of the eponychium, 63% of fingers have a vein measuring at least 0.8 mm; however, the location of these veins is unpredictable (Scheker and Becker, 2011).
Various methods have been described for maintaining blood flow until internal circulation is achieved when an adequate venous anastomosis cannot be constructed (Chen et al., 2013; Kim et al., 2014; Streit et al., 2014; Huan et al., 2016). Anastomosis of a single artery in a digit will not provide adequate resumption of the fingertips. However, the procedure may still be successful if the problem of venous return is solved. When venous anastomoses cannot be constructed, close postoperative monitoring of the replanted digit for adequate circulation is essential (Sunil, 2006; Beris et al., 2010; Nazerani et al., 2011; Cigna et al., 2015). Our team adopts an adjunct treatment involving venous drainage from the nail bed or by fingertip incision (Hirase, 1997; Yabe et al., 2001; Jeon et al., 2016). In addition, we routinely introduce a plastic strip at the anastomosed sites that has the functions of (1) readily allowing venous drainage and thus reducing the risk of excessive pressure at the anastomosed site as a result of edema; and (2) because the wound is typically covered with a blood clot 2–3 days post-digital replantation, a small fraction of the strip can be withdrawn each day to induce bleeding and achieve a similar effect as venous drainage. We did not perform manual venous drainage by fingertip incision in Patient 1; rather, successful replantation was achieved by using a plastic strip to induce bleeding. In Patient 2, the plastic strip was partially withdrawn on day 3 and completely removed on day 4. By day 5, the reattached digit remained bruised and was subsequently treated by the fingertip incision bleeding method. In this group, replantations reconstructed with a vein supply showed no obvious atrophy compared with fingertips without anastomosing veins. Our experience of treating a considerable number of cases indicates that there is characteristically a lesser degree and shorter duration of obstruction of venous return following replantation in younger than in older children (Boyraz and Sayger, 2011); the rate of successful replantation of the fingertips is therefore higher in younger than in older children. Unlike adults, children have immense potential for adaptability (Frykman, 1976) and re-innervation is consequently often close to normal, especially in the younger ones (Barbary et al., 2013). Distal amputations often achieve very good results with replantation, including recovery of sensation (Kotkansalo, 2012; Ciclamini et al., 2013; Ozcanli et al., 2013; Peraut et al., 2015).
Barbary et al. (2013) showed that nerve suturing is not necessary in amputations in Zones I to III, because there is adjacent and spontaneous neurotization. Shi et al. (2010) reported excellent restoration of finger motion and appearance after an average of 26 months (range, 6 to 36 months) of follow-up, with the parents and children expressing satisfaction with the final results. When performing monofilament testing of pressure thresholds, we define 2.83, 4.31, and 3.61 as satisfactory and 4.56 and 6.65 as unsatisfactory results. In our group, the regained s2PDs ranged from 5.0 to 8.0 mm (mean, 6.4 ± 1.14 mm). In this study, differences in SW scores between fingertips with or without nerve repair were not significant, which is in accordance with Barbary et al.'s conclusions (2013). Additionally, we found that replanted digits atrophy if veins have not been anastomosed.
Sensory re-education is very important after replantation of fingers (Dellon, 1986; Piza-Katzer and Estermann, 2007; Cong et al., 2010). In the present study, although not all patients received sensory re-education and the average follow-up was 9.7 months, according to monofilament examination recovery of sensation was satisfactory in all the patients. Patients 2 and 5 achieved excellent results according to the s2PD test. The s2PD test was not performed on the other patients because they were too young.
We believe that our results would have been better if we had provided sensory re-education and prolonged our duration of follow-up. Good outcomes regarding fingertip sensation and restoration of length and cosmetic appearance have been reported by many researchers (Buntic and Brooks, 2010; Kantarci et al., 2010; Barbary et al., 2013).
In conclusion, fingertip replantation in children provides good sensory function and cosmetic outcomes and the procedure should be attempted, if technically feasible.
Acknowledgments
We would like to thank Zeng-tao Wang from Department of Hand and Foot Surgery, Shandong Provincial Hospital, Shandong University, China, for providing anatomical details and figures of fingers.
Footnotes
Funding: This study was supported by a grant from the Department of Health of Guangdong Province of China, No. A2016018; the Specialized Research Fund for the Doctoral Program of Higher Education, No. 20120171120075; a grant from the Science and Technology Project of Guangdong Province of China, No. 2014A020212479; a grant from the Science and Technology Program of Guangzhou City of China, No. 201300000174; a grant from the Science and Technology Project of Guangdong Province of China, No. 2016A010103012; a grant from the Doctoral Start-up Project of the Natural Science Foundation of Guangdong Province of China, No. 2017A030310302.
Conflicts of interest: None declared.
Research ethics: The study protocol was approved by the Institutional Review Board of the First Affiliated Hospital of Sun Yat-sen University of (approval No. (2009)99). The study followed the Declaration of Helsinki and relevant ethical principles.
Declaration of patient consent: The authors certify that they have obtained all appropriate patient consent forms. In the form, patients or their legal guardians have given their consent for the images and other clinical information of patients to be reported in the journal. The patients or their legal guardians understand that the names and initials of patients will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Plagiarism check: Checked twice by iThenticate.
Peer review: Externally peer reviewed.
Copyedited by Yu J, Li CH, Qiu Y, Song LP, Zhao M
References
- 1.Balan JR. Free toe pulp flap for finger pulp and volar defect reconstruction. Indian J Plast Surg. 2016;49:178–184. doi: 10.4103/0970-0358.191319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Barbary S, Dap F, Dautel G. Finger replantation: surgical technique and indications. Chir Main. 2013;32:363–372. doi: 10.1016/j.main.2013.04.012. [DOI] [PubMed] [Google Scholar]
- 3.Beris AE, Lykissas MG, Korompilias AV, Mitsionis GI, Vekris MD, Kostas-Agnantis IP. Digit and hand replantation. Arch Orthop Trauma Surg. 2010;130:1141–1147. doi: 10.1007/s00402-009-1021-7. [DOI] [PubMed] [Google Scholar]
- 4.Boyraz G, Sayger TV. Psychological well-being among fathers of children with and without disabilities: the role of family cohesion, adaptability, and paternal self-efficacy. American journal of men's health. 2011;5:286–296. doi: 10.1177/1557988310372538. [DOI] [PubMed] [Google Scholar]
- 5.Brown M, Lu Y, Chung KC, Mahmoudi E. Annual Hospital Volume and Success of Digital Replantation. Plast Reconstr Surg. 2017;139:672–680. doi: 10.1097/PRS.0000000000003087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Buntic RF, Brooks D. Standardized protocol for artery-only fingertip replantation. J Hand Surg Am. 2010;35:1491–1496. doi: 10.1016/j.jhsa.2010.06.004. [DOI] [PubMed] [Google Scholar]
- 7.Butler DP, Murugesan L, Ruston J, Woollard AC, Jemec B. The outcomes of digital tip amputation replacement as a composite graft in a paediatric population. J Hand Surg Eur Vol. 2016;41:164–170. doi: 10.1177/1753193415613667. [DOI] [PubMed] [Google Scholar]
- 8.Chen YC, Chan FC, Hsu CC, Lin YT, Chen CT, Lin CH. Fingertip replantation without venous anastomosis. Ann Plast Surg. 2013;70:284–288. doi: 10.1097/SAP.0b013e3182321b81. [DOI] [PubMed] [Google Scholar]
- 9.Ciclamini D, Tos P, Magistroni E, Panero B, Titolo P, Da Rold I, Battiston B. Functional and subjective results of 20 thumb replantations. Injury. 2013;44:504–507. doi: 10.1016/j.injury.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 10.Cigna E, Lo Torto F, Maruccia M, Ruggieri M, Zaccheddu F, Chen HC, Ribuffo D. Postoperative care in finger replantation: our case-load and review of the literature. Eur Rev Med Pharmacol Sci. 2015;19:2552–2561. [PubMed] [Google Scholar]
- 11.Cong H, Sui H, Wang C, Wang Z, Yang Q, Wang B. Ten-digit replantation with seven years follow-up: A case report. Microsurgery. 2010;30:405–409. doi: 10.1002/micr.20757. [DOI] [PubMed] [Google Scholar]
- 12.Dadaci M, Ince B, Altuntas Z, Bitik O, Uzun H, Bilgen F. A novel technique for distal fingertip replantation: Polypropylene suture guided interpositional vein graft. J Plast Surg Hand Surg. 2015 doi: 10.3109/2000656X.2015.1041968. doi: 10.3109/2000656X.2015.1041968. [DOI] [PubMed] [Google Scholar]
- 13.Dadaci M, Ince B, Altuntas Z, Bitik O, Kamburoglu HO, Uzun H. Assessment of survival rates compared according to the Tamai and Yamano classifications in fingertip replantations. Indian J Orthop. 2016;50:384–389. doi: 10.4103/0019-5413.185602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.De Frenne H, Dhooghe P. Experience with 46 cases of digital replantation and revascularization. Acta Chir Belg. 1983;83:284–287. [PubMed] [Google Scholar]
- 15.Dellon AL. Sensory recovery in replanted digits and transplanted toes: a review. J Reconstr Microsurg. 1986;2:123–129. doi: 10.1055/s-2007-1007013. [DOI] [PubMed] [Google Scholar]
- 16.Ding ZH, Wang ZT. Atlas of Clinical Anatomy of the Hand. Ji’nan: Shandong Science and Technology Press Co. Ltd; 2007. [Google Scholar]
- 17.Efanov JI, Rizis D, Landes G, Bou-Merhi J, Harris PG, Danino MA. Impact of the number of veins repaired in short-term digital replantation survival rate. J Plast Reconstr Aesthet Surg. 2016;69:640–645. doi: 10.1016/j.bjps.2015.12.001. [DOI] [PubMed] [Google Scholar]
- 18.Engdahl R, Morrison N. Traumatic thumb amputation: case and review. Eplasty. 2015;15:ic18. [PMC free article] [PubMed] [Google Scholar]
- 19.Epameinondas K, Christos A, Petros K, Avraam D, Othon P, Vincent C. Predictable Pattern Digital Artery Perforator Flap: An Alternative Concept in Digital Reconstruction. Hand (N Y) 2016;11:88–96. doi: 10.1177/1558944715614839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fakin R, Gazzola R, Calcagni M, Giovanoli P, Giesen T. Replantation by palmar arteriovenous anastomosis in complex finger amputations. Chir Main. 2015;34:240–244. doi: 10.1016/j.main.2015.08.003. [DOI] [PubMed] [Google Scholar]
- 21.Frykman GK. Peripheral nerve injuries in children. Orthop Clin North Am. 1976;7:701–716. [PubMed] [Google Scholar]
- 22.Glickman LT, Mackinnon SE. Sensory recovery following digital replantation. Microsurgery. 1990;11:236–242. doi: 10.1002/micr.1920110311. [DOI] [PubMed] [Google Scholar]
- 23.He B, Zhu Q, Chai Y, Ding X, Tang J, Gu L, Xiang J, Yang Y, Zhu J, Liu X. Safety and efficacy evaluation of a human acellular nerve graft as a digital nerve scaffold: a prospective, multicentre controlled clinical trial. J Tissue Eng Regen Med. 2015;9:286–295. doi: 10.1002/term.1707. [DOI] [PubMed] [Google Scholar]
- 24.Hirase Y. Salvage of fingertip amputated at nail level: new surgical principles and treatments. Ann Plast Surg. 1997;38:151–157. doi: 10.1097/00000637-199702000-00009. [DOI] [PubMed] [Google Scholar]
- 25.Huan AS, Regmi S, Gu JX, Liu HJ, Zhang WZ. Fingertip replantation (zone I) without venous anastomosis: clinical experience and outcome analysis. Springerplus. 2016;5:1835. doi: 10.1186/s40064-016-3394-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Idrissi ME, Elibrahimi A, Shimi M, Elmrini A. Digital replantation, results and complications: study of a series of 18 cases. Pan Afr Med J. 2016;24:184. doi: 10.11604/pamj.2016.24.184.8718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ishikawa K, Ogawa Y, Soeda H, Yoshida Y. A new classification of the amputation level for the distal part of the finger. J Jpn Soc Reconstr Microsurg. 1990;3:54–62. [Google Scholar]
- 28.Jazayeri L, Klausner JQ, Chang J. Distal digital replantation. Plast Reconstr Surg. 2013;132:1207–1217. doi: 10.1097/PRS.0b013e3182a3c0e7. [DOI] [PubMed] [Google Scholar]
- 29.Jeon BJ, Yang JW, Roh SY, Ki SH, Lee DC, Kim JS. Lateral nail fold incision technique for venous anastomosis in fingertip replantation. Ann Plast Surg. 2016;76:67–71. doi: 10.1097/SAP.0000000000000297. [DOI] [PubMed] [Google Scholar]
- 30.Kantarci U, Cepel S, Buldu H. Successful replantation in ten-digit amputation. Acta Orthop Traumatol Turc. 2010;44:76–78. doi: 10.3944/AOTT.2010.2109. [DOI] [PubMed] [Google Scholar]
- 31.Kim JH, Lee YM. Fingertip replantation using Y-shaped vein graft to pulp artery. Ann Plast Surg. 2015;75:424–429. doi: 10.1097/SAP.0000000000000196. [DOI] [PubMed] [Google Scholar]
- 32.Kim JS, Yang JW, Lee DC, Ki SH, Roh SY. Challenges in fingertip replantation. Semin Plast Surg. 2013;27:165–173. doi: 10.1055/s-0033-1360583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kim SW, Han HH, Jung SN. Use of the mechanical leech for successful zone I replantation. ScientificWorldJournal. 2014;2014:105234. doi: 10.1155/2014/105234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Komatsu S, Tamai S. Successful replantation of a completely cut-off thumb. Plast Reconstr Surg. 1968;42:374–377. [Google Scholar]
- 35.Kotkansalo T. Fingertip injuries. Duodecim. 2012;128:399–407. [PubMed] [Google Scholar]
- 36.Lima JQ, Jr, Carli AD, Nakamoto HA, Bersani G, Crepaldi BE, de Rezende MR. Prognostic factors on survival rate of fingers replantation. Acta Ortop Bras. 2015;23:16–18. doi: 10.1590/1413-78522015230101026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ma Z, Guo F, Qi J, Xiang W, Zhang J. Effects of non-surgical factors on digital replantation survival rate: a meta-analysis. J Hand Surg Eur Vol. 2016;41:157–163. doi: 10.1177/1753193415594572. [DOI] [PubMed] [Google Scholar]
- 38.Masuhara K, Tamai S, Fukunishi H, Obama K, Komatsu S. Experience with reanastomosis of the amputated thumb. Seikei Geka. 1967;18:403–404. [PubMed] [Google Scholar]
- 39.Meek MF. A randomized prospective study of polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg. 2001;108:1087–1088. doi: 10.1097/00006534-200109150-00056. [DOI] [PubMed] [Google Scholar]
- 40.Murphy AD, Keating CP, Penington A, McCombe D, Coombs CJ. Paediatric fingertip composite grafts: Do they all go black? J Plast Reconstr Aesthet Surg. 2017;70:173–177. doi: 10.1016/j.bjps.2016.11.002. [DOI] [PubMed] [Google Scholar]
- 41.Nazerani S, Motamedi MH, Ebadi MR, Nazerani T, Bidarmaghz B. Experience with distal finger replantation: a 20-year retrospective study from a major trauma center. Tech Hand Up Extrem Surg. 2011;15:144–150. doi: 10.1097/BTH.0b013e31820504c9. [DOI] [PubMed] [Google Scholar]
- 42.Ozcanli H, Coskunfirat OK, Bektas G, Cavit A. Innervated digital artery perforator flap. J Hand Surg Am. 2013;38:350–356. doi: 10.1016/j.jhsa.2012.10.019. [DOI] [PubMed] [Google Scholar]
- 43.Park HC, Bahar-Moni AS, Cho SH, Kim SS, Park HS, Ahn SC. Classification of distal fingertip amputation based on the arterial system for replantation. J Hand Microsurg. 2013;5:4–8. doi: 10.1007/s12593-012-0086-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Peraut E, Mirous MP, Chammas M. Secondary restoration of fingertip sensation with Littler's heterodigital neurovascular island flap after ring avulsion injury: report of two cases. Chir Main. 2015;34:49–54. doi: 10.1016/j.main.2014.12.001. [DOI] [PubMed] [Google Scholar]
- 45.Piza-Katzer H, Estermann D. Cognitive re-education and early functional mobilisation in hand therapy after bilateral hand transplantation and heterotopic hand replantation--two case reports. Acta Neurochir Suppl. 2007;100:169–171. doi: 10.1007/978-3-211-72958-8_35. [DOI] [PubMed] [Google Scholar]
- 46.Regmi S, Gu JX, Zhang NC, Liu HJ. A systematic review of outcomes and complications of primary fingertip reconstruction using reverse-flow homodigital island flaps. Aesthetic Plast Surg. 2016;40:277–283. doi: 10.1007/s00266-016-0624-y. [DOI] [PubMed] [Google Scholar]
- 47.Saha SS, Pandey A, Parwal C. Arterial segments as microvascular interposition grafts in venous anastomosis in digital replantations. Indian J Plast Surg. 2015;48:166–171. doi: 10.4103/0970-0358.163055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Scheker LR, Becker GW. Distal finger replantation. J Hand Surg Am. 2011;36:521–528. doi: 10.1016/j.jhsa.2010.12.017. [DOI] [PubMed] [Google Scholar]
- 49.Shi D, Qi J, Li D, Zhu L, Jin W, Cai D. Fingertip replantation at or beyond the nail base in children. Microsurgery. 2010;30:380–385. doi: 10.1002/micr.20743. [DOI] [PubMed] [Google Scholar]
- 50.Streit L, Dvořák Z, Novák O, Stiborová S, Veselý J. The use of medicinal leeches in fingertip replantation without venous anastomosis - case report of a 4-year-old patient. Acta Chir Plast. 2014;56:23–26. [PubMed] [Google Scholar]
- 51.Sun G, Nie K, Jin W, Wei Z, Qi J, Wang D. Composite tissue flap at perforating branches of saphenous artery: a new design for repairing composite tissue defects in anterior knee. Int J Clin Exp Med. 2015;8:21448–21453. [PMC free article] [PubMed] [Google Scholar]
- 52.Sunil TM. A technique for postoperative cooling after composite grafting of the fingertip. Tech Hand Up Extrem Surg. 2006;10:118–119. doi: 10.1097/00130911-200606000-00012. [DOI] [PubMed] [Google Scholar]
- 53.Wang ZT, Sun WH. Cosmetic reconstruction of the digits in the hand by composite tissue grafting. Clin Plast Surg. 2014;41:407–427. doi: 10.1016/j.cps.2014.03.001. [DOI] [PubMed] [Google Scholar]
- 54.Wang ZT, Wang YB, Ding ZH. Clinical Anatomic Atlas of Microsurgery. Ji’nan: Shandong Science and Technology Press Co. Ltd; 2014. [Google Scholar]
- 55.Weber RA, Breidenbach WC, Brown RE, Jabaley ME, Mass DP. A randomized prospective study of polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg. 2000;106:1036–1045. doi: 10.1097/00006534-200010000-00013. discussion 1046-1048. [DOI] [PubMed] [Google Scholar]
- 56.Weinstein S. Fifty years of somatosensory research: from the Semmes-Weinstein monofilaments to the Weinstein Enhanced Sensory Test. J Hand Ther. 1993;6:11–22. discussion 50. [PubMed] [Google Scholar]
- 57.Wen G, Xu J, Chai YM. Fingertip replantation with palmar venous anastomoses in children. Ann Plast Surg. 2017;78:692–696. doi: 10.1097/SAP.0000000000000948. [DOI] [PubMed] [Google Scholar]
- 58.Yabe T, Muraoka M, Motomura H, Ozawa T. Fingertip replantation using a single volar arteriovenous anastomosis and drainage with a transverse tip incision. J Hand Surg Am. 2001;26:1120–1124. doi: 10.1053/jhsu.2001.28939. [DOI] [PubMed] [Google Scholar]
- 59.Yamano Y. Replantation of the amputated distal part of the fingers. J Hand Surg Am. 1985;10:211–218. doi: 10.1016/s0363-5023(85)80107-6. [DOI] [PubMed] [Google Scholar]
- 60.Yu H, Wei L, Liang B, Hou S, Wang J, Yang Y. Nonsurgical factors of digital replantation and survival rate: A metaanalysis. Indian J Orthop. 2015;49:265–271. doi: 10.4103/0019-5413.156185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Zhu JK. Microsurgery. Beijing: People's Medical Publishing House Co, Ltd; 2008. [Google Scholar]