

Abstract
Ascorbic acid is one of the most well-known nutritional supplement and antioxidant found in fruits and vegetables. Calcium ascorbate has been developed to mitigate the gastric irritation caused by the acidity of ascorbic acid. The aim of this study was to compare calcium ascorbate and ascorbic acid, focusing on their antioxidant activity and effects on gastric juice pH, total acid output, and pepsin secretion in an in vivo rat model, as well as pharmacokinetic parameters. Calcium ascorbate and ascorbic acid had similar antioxidant activity. However, the gastric fluid pH was increased by calcium ascorbate, whereas total acid output was increased by ascorbic acid. In the rat pylorus ligation-induced ulcer model, calcium ascorbate increased the gastric fluid pH without changing the total acid output. Administration of calcium ascorbate to rats given a single oral dose of 100 mg/kg as ascorbic acid resulted in higher plasma concentrations than that from ascorbic acid alone. The area under the curve (AUC) values of calcium ascorbate were 1.5-fold higher than those of ascorbic acid, and the Cmax value of calcium ascorbate (91.0 ng/ml) was higher than that of ascorbic acid (74.8 ng/ml). However, their Tmax values were similar. Thus, although calcium ascorbate showed equivalent antioxidant activity to ascorbic acid, it could attenuate the gastric high acidity caused by ascorbic acid, making it suitable for consideration of use to improve the side effects of ascorbic acid. Furthermore, calcium ascorbate could be an appropriate antioxidant substrate, with increased oral bioavailability, for patients with gastrointestinal disorders.
Keywords: Antioxidant, Ascorbic acid, Bioavailability, Calcium ascorbate, Gastric pH
INTRODUCTION
Vitamin C (ascorbic acid) is one of the elements required for the maintenance of human health and function [1,2]. As the main function of ascorbic acid is as an antioxidant for the removal of active oxygen, and it therefore has anti-aging, immune enhancement, drinking and smoking detoxification, gastric cancer prevention, vascular health protection, and atherosclerosis prevention effects [3,4,5]. Ascorbic acid is found in many vegetables and fruits, in particular, oranges, tomatoes, spinach, strawberries, potatoes, etc. The recommended daily intake of this vitamin is 90 mg for adults [1,2]. The lack of ascorbic acid in the human body inhibits the synthesis of collagen, causing swelling and bleeding of the gums, scurvy, chronic fatigue, nosebleeds, digestive disorders, and depression. Although excessive intake of ascorbic acid is not toxic, it could induce diarrhea, abdominal pain, acid indigestion, frequent urination, and headaches [6,7]. As mentioned above, the main effect of ascorbic acid is as an antioxidant for eliminating free radicals in the body and inhibiting various inflammatory conditions [8,9]. With its antioxidant activity, ascorbic acid plays an important role in the production of some major proteins, such as collagen, serotonin, and norepinephrine [10,11].
As humans cannot synthesize ascorbic acid in vivo, the vitamin has to be ingested from an external source. Although ascorbic acid can be from synthetic and natural sources, but the human body can accept either type, indicating that the body's absorption and utilization of this supplement is more important than the compound's origin. The oxidation product of ascorbic acid is dehydroascorbic acid, but high doses of ascorbic acid are metabolized to oxalate, where metabolism of accumulated oxalate can lead to urinary stone formation [12,13]. Excess intake of this supplement also causes diarrhea [14] and pyrolysis [15].
Gastritis or peptic ulcer is a disease that causes a change of the gastric mucosa, eliciting a variety of symptoms, such as indigestion, nausea, and heartburn. An excess intake of food or a sudden intake of high-acidity foods will lead to excessive secretion of gastric juices into the stomach and increased pepsin secretion in the mucous membrane chief cells. Pepsin represents active protein degradation at low pH (pH 1.8–2.0) [16,17], its activity and continuous exposure to gastric juice can induce damage of the stomach wall. The best known way to treat gastritis is to control the one's dietary life style; in other words, to avoid overeating and strong acidic foods, reduce stress and alcohol consumption [18]. Gastrointestinal disorders, such as gastritis or ulcers that result from consumption of high-acidity foods, increase the risk of gastric reflux into the esophagus [19]. Ascorbic acid has very high acidity and may induce these gastrointestinal side effects when ingested on an empty stomach [20]. Calcium ascorbate (neutralized vitamin C) has been developed to mitigate the epigastric adverse effects due to the low pH of ascorbic acid. A randomized, double-blind, crossover clinical trial with patients sensitive to acidic foods confirmed the lower occurrence of epigastric adverse effects with calcium ascorbate with ascorbic acid [15].
In this study, we hypothesized that calcium ascorbate could attenuate ascorbic acid-induced gastric high acidity and increase its oral bioavailability. To test this hypothesis, we compared the antioxidant activity, gastric juice pH, and total acid output in simulated gastric fluids (SGFs) treated with ascorbic acid and calcium ascorbate in vitro. Moreover, we examined the effect of calcium ascorbate on the gastric juice pH, total acid output, and pepsin activity in a rat model in vivo, as well as its pharmacokinetic parameters.
METHODS
Materials
Ascorbic acid (drug content 97%) and calcium ascorbate (drug content 76%) were obtained from PHARMCROSS Co., Ltd (Chuncheon, Korea). Methanol for high-performance liquid chromatography (HPLC) was purchased from SKYSOLTECH® (SK Chemicals, Ulsan, Korea). Acetonitrile for sample processing was purchased from Honeywell Burdick & Jackson Labs (Muskegon, MI, USA). Acetic acid (glacial, 99.5%) was purchased from Samchun Pure Chemical (Gyeonggi-do, Korea). All other chemicals were of reagent grade and were used without further purification. The distilled and deionized water (DW) was used after sterilization.
Animals
Male Sprague-Dawley rats (300 g) were purchased from Dae Han Laboratory Animal Research Co. (Eumsung, Korea) and were given free access to a normal standard chow diet (No. 322-7-1; Superfeed Co., Wonju, Korea) and tap water ad libitum. Throughout the experiments, the animals were housed (four per cage) in laminar flow cages maintained at 25±2℃ and 50–60% relative humidity under a 12 h light–dark cycle. The rats were acclimated under these conditions for at least 1 week. Each rat was fasted for at least 24 h prior to the experiment. The Committee for Ethical Usage of Experimental Animals in Chungnam National University (Daejeon, Korea) approved all animal study protocols (CNU-00605 and CNU-00609).
Preparation of simulated gastric fluid and determination of in vitro gastric acidity
SGF was prepared with 0.2 g of NaCl, 0.7 ml of HCl, and 100 ml of DW. To prepare SGF with pepsin (SGFw/P), 0.32 g of pepsin was added to the same SGF composition described above. The prepared gastric fluids were used to simulate the mean volume of gastric juice for human (hSGF & hSGFw/P) [21] and rat (rSGF & rSGFw/P) [22], and ascorbic acid was treated at the recommended daily intake dose. To compare the effects of ascorbic acid and calcium ascorbate on the pH and acidity of the gastric fluids, the changes in pH and acidity of SGFs mixed with DW (as the control), ascorbic acid, or calcium ascorbate were determined. The pH was measured with a pH meter (Orion 3-Star Plus; Thermo Fisher Scientific, Waltham, MA, USA). For acidity determination, 500 µl of SGF or SGFw/P was placed in a beaker with 10 µl of 0.1% phenolphthalein solution according to the method of Raoa and Vijayakumar [23], as the acidity was calculated as the volume of 0.01 N NaOH required to change the solution from colorless to rose color.
Pylorus ligation-induced ulcer model and measurement of gastric volume and pH
The animals were fasted for 24 h before the experiment and then anesthetized by intraperitoneal injection of 60 mg/kg of pentobarbital sodium (Hanlim Pharm. Co., Ltd, Seoul, Korea). Then, ascorbic acid (105.96 mg/kg) and calcium ascorbate (135.24 mg/kg) were orally administered to the rats, respectively. The ascorbic acid and calcium ascorbate doses for the rats (equivalent to 102.78 mg/kg as ascorbic acid) were converted from the human dose (1,000 mg/60 kg). For pylorus ligation, a 2 cm abdominal laparotomy was performed, and the pyloric region was tied using silk thread. After suture, the animals were relieved in the recovery chamber and transferred to their cages.
Experiments were carried out according to the method of Rao and Vijayakumar [23]. The animals were sacrificed after a certain period of time and the gastric juice was collected from the stomach. After centrifugation of the gastric juice at 3,000 rpm for 15 min, the exact volume of the supernatant was measured. This volume of gastric contents from the animals was converted to the kilogram weight of the experimental animals, using following equation:
The pH of the collected supernatant was measured with a pH meter (Thermo Fisher Scientific). The acidity obtained from the titration method was converted to total acid output (µEq) using the following equation.
| Total acid output (µEq)=titratable acidity (ml)×2×10 |
Measurement of pepsin secretion
According to the method of Sairam et al. [24], 250 µl of substrate (2.0 [w/v] hemoglobin solution) was added to the blank and sample tubes, and pretreated for 10 min in at 37℃ water bath. Then, 50 µl of the supernatant from the rat stomach sample was added to the pretreated tube. After gentle vortex-mixing, the solution was incubated for 10 min in the 37℃ water bath. Thereafter, 500 µl of 5% trichloroacetic acid was added to the solution, and the tube was gently vortexed and then incubated for 5 min in the 37℃ water bath. The solution was centrifuged at 6,000 × g for 30 min at 25℃ and the supernatant was collected. The supernatant of the sample and blank tubes was diluted four times with 0.1 N HCl and the absorbance was measured at 280 nm wavelength using a UV spectrometer (UV1800; Shimadzu, Tokyo, Japan).
To prepare the standard solution, pepsin was dissolved in 0.1 N NaOH and the solution was diluted to the concentrations of 0, 12.5, 25, 50, 100, 200, and 400 µg/ml. All reactions were carried out twice using the sample and blank solutions. After completion of the reaction, the absorbance of the supernatant was measured without dilution at 280 nm wavelength using a UV spectrometer (Shimadzu).
Determination of oxygen radical antioxidant capacity
The oxygen radical antioxidant capacity (ORAC) values for ascorbic acid and calcium ascorbate were determined using the OxiSelect™ Oxygen Radical Antioxidant Capacity (ORAC) Activity Assay Kit (Cell Biolabs, Inc., San Diego, CA, USA) according to the manufacturer's instructions. In brief, the area under curve (AUC) of each Trolox concentration (0, 2.5, 5, 10, 20, 30, 40, and 50 µM) was calculated using the standard curve for ORAC activity. Ascorbic acid and calcium ascorbate were calculated as the mmol Trolox equivalents (TE) by comparison against the standard curve. The ORAC values were expressed as TE/L.
Pharmacokinetics of ascorbic acid after oral administration
Using an animal feeding needle (oral zonde needle, stainless, 7 cm), ascorbic acid (105.96 mg/kg) or calcium ascorbate (135.24 mg/kg) was administered to the rats. An orbital blood sample (1.0 ml) was collected at 0.5, 1, 2, 4, 6, and 24 h post ingestion [25]. The plasma was separated by centrifugation of the blood sample at 12,000 rpm, 4℃, for 10 min, and then 100 µl was stored in the deep freezer at −70℃ prior to HPLC analysis. The HPLC method used was a modification of previous HPLC quantification methods [26]. To determine the concentration of ascorbic acid in the plasma, standard solutions were prepared by mixing the stock solution with blank plasma. For plasma deproteination, the collected plasma (30 µl) was mixed with acetonitrile (90 µl) by vortex mixing, and the mixture was then separated by centrifugation at 12,000 rpm, 4℃, for 10 min (Micro 17TR, Hanil Science, Korea). To remove impurities, the solutions were filtered through a polytetrafluoroethylene syringe filter (pore size 0.45 µm, diameter 13 mm; Whatman, Maidstone, UK). The concentration of ascorbic acid was determined using an SP-LC model HPLC system (PeakmanSP, Seoul, Korea) equipped with two SP 3101 pumps, an SP 3002 UV/Vis detector, an SP 3004 column oven, an SP 3010 switching valve and a 3023 SI-2 autosampler (Shiseido, Tokyo, Japan). The separation was performed on a Shiseido Capcell Pak MGII column (4.6 mm i.d.×150 mm, 5 µm) maintained at 30℃. The mobile phase was prepared by mixing distilled water, methanol, and acetic acid (91.9:8:0.1, v/v/v) and eluted at a flow rate 0.5 ml/min. After 10 µl samples were injected onto the column, the signals were monitored at a UV wavelength of 240 nm.
Statistical analysis
All data were expressed as the mean±SEM of three or more independent experiments. Analysis of variance was used to compare parameters among multiple groups (GraphPad, San Diego, CA, USA). If a significant difference between treated groups was found, Dunnett's test was applied. Differences with p<0.05 were considered statistically significant.
RESULTS
Comparison of the antioxidant activities of ascorbic acid and calcium ascorbate
It is well known that ascorbic acid aids cell growth and helps the body to stay healthy because of its antioxidant activity, which potentially offers protection from some diseases and degenerative aspects of aging [27]. To ascertain whether the antioxidant activity of calcium ascorbate was still functional, the antioxidant activities of calcium ascorbate and ascorbic acid were evaluated by measuring the fluorescence decrease rate from the production and decay of the peroxy radical by 2, 2′-azo-bis-2-methyl-propanimidamide, dihydrochloride (AAPH) using ORAC assay. Table 1 shows that with the antioxidant activity of ascorbic acid (25.24 mmol TE/L) was not significantly different from that of calcium ascorbate (25.65 mmol TE/L), and their relative percentages of antioxidant activity were also not significantly different (100% vs 101%, Table 1). These data show that calcium ascorbate and ascorbic acid have similar antioxidant activities.
Table 1. Antioxidant activity of calcium ascorbate measured by oxygen radical absorbance capacity (ORAC) assay (n=4).
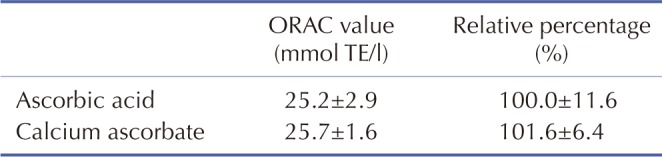
TE, trolox equivalent.
Effect of calcium ascorbate on gastric juice pH and total acid output in human and rat simulated gastric fluids in vitro
Previously, several studies reported that ascorbic acid could induce gastrointestinal disorders such as indigestion, heartburn, nausea, diarrhea, abdominal cramps/pain, and esophagitis [15,28,29]. Because ascorbic acid is highly acidic and could stimulate the secretion of stomach acids such as pepsin, these excess acids may trigger these gastrointestinal symptoms. To determine the effect of calcium ascorbate on the pH and total acid output of gastric juice, the differences in pH and total acid of SGFs following treatment with calcium ascorbate and ascorbic acid were compared. When treated with ascorbic acid, the gastric fluid pH was not different to that of the DW control in both hSGF and rSGF (Figs. 1A and 2A). In contrast, the pH of SGFs treated with calcium ascorbate was significantly higher than that of fluids treated with ascorbic acid (Figs. 1A and 2A). However, the total acid output was significantly higher in ascorbic acid-treated SGFs than in the DW control (Figs. 1B and 2B), whereas calcium ascorbate treatment resulted in no significant changes relative to the control (Figs. 1B and 2B). These results indicate that calcium ascorbate could act to increase gastric pH without increasing the total acid output, thereby attenuating gastric symptoms.
Fig. 1. Effect of calcium ascorbate on the pH and total acid output of human simulated gastric fluid (hSGF).

After the addition of ascorbic acid or calcium ascorbate to the hSGF, the changes in hSGF pH and total acid were measured until 240 min. pH (A) and total acid (B) of hSGF; pH (C) and total acid (D) of hSGFw/P (hSGF with pepsin). Data are expressed as the mean±SEM (n=5). ***p<0.001 vs. distilled water (DW).
Fig. 2. Effect of calcium ascorbate on the pH and total acid output of rat simulated gastric fluid (rSGF).

After the addition of ascorbic acid or calcium ascorbate to the rSGF, the changes in rSGF pH and total acid were measured until 240 min. pH (A) and total acid (B) of rSGF; pH (C) and total acid (D) of rSGFw/P (rSGF with pepsin). Data are expressed as the mean±SEM (n=5). ***p<0.001 vs. distilled water (DW).
Because pepsin is one of the major enzymes in gastric fluid and is stimulated by low pH and acid [30], its effect on gastric pH and total acid output was investigated in the SGFs treated with calcium ascorbate or ascorbic acid. The gastric pH and total acid output were not affected by pepsin in the hSGFw/P and rSGFw/P (Figs. 1C, 1D, 2C, and 2D).
Effect of calcium ascorbate on gastric juice pH and total acid output in the in vivo rat pylorus ligation-induced ulcer model
The reduction of gastric pH and the secretion of gastric juices both work to exacerbate damage to the gastric wall in gastric disorders [30]. Therefore, the effect of calcium ascorbate was further confirmed in the rat pylorus ligation-induced ulcer model. Although the secreted volume of gastric juice was not significantly different between ascorbic acid and calcium ascorbate treatments (Fig. 3A), the gastric juice pH was significantly increased by calcium ascorbate as compared with ascorbic acid until 30 min after administration (Fig. 3B). In contrast, the total acid output was not significantly increased by calcium ascorbate (Fig. 4A).
Fig. 3. Effect of calcium ascorbate on gastric juice volume and pH in the rat pylorus ligation-induced ulcer model.

After oral administration of distilled water (DW; as a control), ascorbic acid (105.96 mg/kg), or calcium ascorbate (135.24 mg/kg) to rats processed by pylorus ligation, the stomach was removed immediately following animal sacrifice and the gastric contents were collected at designated times. After the centrifugation of the gastric contents (1,800×g for 5 min), the volume (A) and pH (B) were measured. Data are expressed as the mean±SEM (n=5). **p<0.01, ***p<0.001 vs. distilled water (DW); ##p<0.01, ###p<0.001 vs. ascorbic acid.
Fig. 4. Effect of calcium ascorbate on total acid output and pepsin secretion in the rat pylorus ligation-induced ulcer model.

After oral administration of distilled water (DW; as a control), ascorbic acid (105.96 mg/kg), or calcium ascorbate (135.24 mg/kg) to rats processed by pylorus ligation, the stomach was removed immediately following animal sacrifice and the gastric contents were collected at designated times. After centrifugation of the gastric contents (1,800×g for 5 min), the total acid output (A) and amount of secreted pepsin (B) were measured. Data are expressed as the mean±SEM (n=5). **p<0.01, ***p<0.001 vs. distilled water (DW); ##p<0.01, ###p<0.001 vs. ascorbic acid.
Pepsin, secreted by the mucous membrane chief cells, is also present in the gastric juice and shows proteolytic activity at low pH (1.8–2.0) [31]. It is also known that the high activity of pepsin induces gastric damage [32]. Therefore, we evaluated whether the secretion of pepsin was affected by calcium ascorbate treatment. Fig. 4B shows that pepsin secretion was not induced by dosing with calcium ascorbate in the rat pylorus ligation-induced ulcer model, whereas it was immediately induced after ascorbic acid administration. Taken together, these results demonstrate that calcium ascorbate is effective in attenuating ascorbic acid-induced gastric symptoms by increasing the gastric pH and preventing pepsin secretion in the rat pylorus ligation-induced ulcer model.
Pharmacokinetics of calcium ascorbate after oral administration to rats
To investigate whether calcium ascorbate could improve the oral bioavailability of ascorbic acid, a pharmacokinetic study was carried out. Calcium ascorbate administration resulted in significantly higher plasma concentrations of ascorbic acid than dosing of ascorbic acid, at 0.5, 1, 2, 4, 6, and 24 h post oral administration (Fig. 5). The AUC0-24h value from calcium ascorbate (1277.0 ng/ml) was 1.5-fold higher than that from ascorbic acid (705.7 ng/ml), and the AUCinf value from calcium ascorbate (5769.6 ng/ml) was 2.8-fold higher than that from ascorbic acid (2024.7 ng/ml). The Cmax value of calcium ascorbate (91.0 ng/ml) was also higher than that of ascorbic acid (74.8 ng/ml). However, the Tmax values were similar (Table 2). After 24 h post dose, the plasma concentration of calcium ascorbate (45.3 ng/ml) was two times higher than that of ascorbic acid (22.6 ng/ml) (Fig. 5). Therefore, calcium ascorbate was obviously better absorbed and hence present in higher plasma levels than ascorbic acid.
Fig. 5. Blood concentration of ascorbic acid after oral administration.
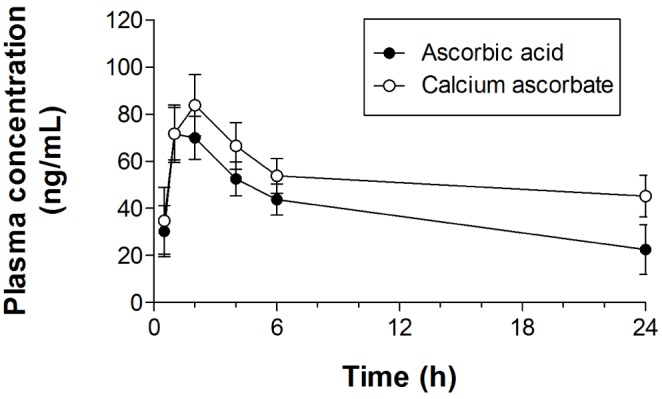
Plasma concentration versus time profiles obtained after the administration of ascorbic acid (105.96 mg/kg) and calcium ascorbate (135.24 mg/kg). Values for each time point are expressed as the mean±SEM (n=6).
Table 2. Pharmacokinetic parameters of ascorbic acid and calcium ascorbate after oral administration to rats (mean±SEM, n=6).
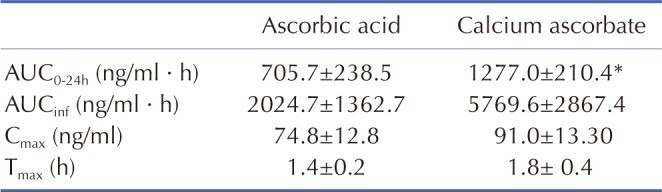
*Means p<0.05 compared with the results of ascorbic acid.
DISCUSSION
This study had two major findings: (1) calcium ascorbate could act as an antioxidant substrate without acid-induced gastric high acidity, and (2) the rate of absorption and the maintenance of calcium ascorbate in the body were higher than those of ascorbic acid in vivo. Our observations suggest that calcium ascorbate could be used as an antioxidant substrate for individual health maintenance without gastric high acidity particularly for people with sensitive stomachs and illnesses such as indigestion, diarrhea, abdominal cramps/pain, and other gastric diseases.
Gastric acid is one of the most important factors causing gastritis and reflux esophagitis [33]. Control of the stomach pH is an essential method to protect the gastric mucosa against damage [30]. Ascorbic acid is known to have an adverse effect by decreasing the gastric pH in patients with gastrointestinal disorders [34]. In the present study, we found that ascorbic acid increased the total acid outputs in vitro and in vivo (Figs. 1B, 1D, 2B, 2D, and 4A). However, calcium ascorbate increased the gastric pH without changing the total acid output (Figs. 1A, 1C, 2A, 2C, and 4A). Because pepsin activity could induce gastric wall damage, the lower activity of pepsin at a higher pH in the stomach could suppress the deterioration of the stomach [35]. Therefore, the inhibition of pepsin secretion and activity would be a most important target in the treatment of gastric disorders from gastric acid [19]. We found that pepsin did not affect the gastric pH and total acid output in vitro (Figs. 1C, 1D, 2C, and 2D); however, its secretion was increased by ascorbic acid in vivo, but not by calcium ascorbate (Fig. 4A). Moreover, we found that the antioxidant activity of calcium ascorbate was similar to that of ascorbic acid (Table 1). Thus, the findings from the present study provide compelling evidence of the protective role of calcium ascorbate against gastric high acidity in vitro and in vivo.
In rats with pylorus ligation-induced ulcer, the volume of gastric juice was increased gradually because of the pylorus ligation, but the changes in pH within 30 min were not significant since gastric juice was not secreted until 30 min (Fig. 3A). Moreover, pH reduction was observed after 60 min because of the increase of gastric juice secretion over time. The values of total acid output within 30 min were measured as the acidity of ascorbic acid, because the volumes of gastric juices were not significantly increased until 30 min (Fig. 4A). However, the total acid output seemed to be reduced at 240 min by dilution of the secreted gastric juices. Similar results were observed for pepsin output (Fig. 4B), which was increased with ascorbic acid dosing but inhibited by calcium ascorbate.
Moreover, it was found that the oral bioavailability of calcium ascorbate was higher than that of ascorbic acid [25]. The AUC0-24h values of calcium ascorbate were greater than ascorbic acid with significant difference (p<0.05). The reason for the increased absorption of calcium ascorbate was likely due to the neutralizing effect of the calcium salt. However, the AUCinf values were not significantly different in those two groups. Since the general dosage regimen of ascobate preparation is once daily and water-soluble vitamins are easy to be excreted in urine, it is meaningful to show the higher AUC0-24h values instead of AUCinf values.
In conclusion, our results demonstrate that calcium ascorbate has the same antioxidant activity as ascorbic acid, but can alleviate the side effects of the vitamin C, such as gastric high acidity. Furthermore, calcium ascorbate could be an appropriate antioxidant substrate, with increased oral bioavailability, for patients with gastrointestinal disorders.
ACKNOWLEDGEMENTS
This research was supported by a grant of PHARMCROSS (Chuncheon, Korea) and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Korean government, MOE (No 2009-0093815).
Footnotes
Author contributions: J.S.P. and C.S.M. designed the study, analyzed the data, and wrote the manuscript. J.K.L., S.H.J., S.E.L., J.H.H., E.J., and H.S.P. performed the experiments, and K.S.H. analyzed the data. D.K. helped with the calcium ascorbate preparation and data analysis.
CONFLICTS OF INTEREST: The authors declare no conflicts of interest.
References
- 1.Valdes F. Vitamin C. Actas Dermosifiliogr. 2006;97:557–568. doi: 10.1016/s0001-7310(06)73466-4. [DOI] [PubMed] [Google Scholar]
- 2.Naidu KA. Vitamin C in human health and disease is still a mystery? An overview. Nutr J. 2003;2:7. doi: 10.1186/1475-2891-2-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Padayatty SJ, Katz A, Wang Y, Eck P, Kwon O, Lee JH, Chen S, Corpe C, Dutta A, Dutta SK, Levine M. Vitamin C as an antioxidant: evaluation of its role in disease prevention. J Am Coll Nutr. 2003;22:18–35. doi: 10.1080/07315724.2003.10719272. [DOI] [PubMed] [Google Scholar]
- 4.Carr A, Frei B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999;13:1007–1024. doi: 10.1096/fasebj.13.9.1007. [DOI] [PubMed] [Google Scholar]
- 5.Martin A, Frei B. Both intracellular and extracellular vitamin C inhibit atherogenic modification of LDL by human vascular endothelial cells. Arterioscler Thromb Vasc Biol. 1997;17:1583–1590. doi: 10.1161/01.atv.17.8.1583. [DOI] [PubMed] [Google Scholar]
- 6.Padayatty SJ, Levine M. New insights into the physiology and pharmacology of vitamin C. CMAJ. 2001;164:353–355. [PMC free article] [PubMed] [Google Scholar]
- 7.Johnston CS. Biomarkers for establishing a tolerable upper intake level for vitamin C. Nutr Rev. 1999;57:71–77. doi: 10.1111/j.1753-4887.1999.tb06926.x. [DOI] [PubMed] [Google Scholar]
- 8.Anderson JW, Gowri MS, Turner J, Nichols L, Diwadkar VA, Chow CK, Oeltgen PR. Antioxidant supplementation effects on low-density lipoprotein oxidation for individuals with type 2 diabetes mellitus. J Am Coll Nutr. 1999;18:451–461. doi: 10.1080/07315724.1999.10718883. [DOI] [PubMed] [Google Scholar]
- 9.Kim YY, Ku SY, Huh Y, Liu HC, Kim SH, Choi YM, Moon SY. Antiaging effects of vitamin C on human pluripotent stem cell-derived cardiomyocytes. Age (Dordr) 2013;35:1545–1557. doi: 10.1007/s11357-012-9457-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hamrick I, Counts SH. Vitamin and mineral supplements. Prim Care. 2008;35:729–747. doi: 10.1016/j.pop.2008.07.012. [DOI] [PubMed] [Google Scholar]
- 11.Wilson JX. Regulation of vitamin C transport. Annu Rev Nutr. 2005;25:105–125. doi: 10.1146/annurev.nutr.25.050304.092647. [DOI] [PubMed] [Google Scholar]
- 12.Chen X, Shen L, Gu X, Dai X, Zhang L, Xu Y, Zhou P. High-dose supplementation with vitamin C-induced pediatric urolithiasis: the first case report in a child and literature review. Urology. 2014;84:922–924. doi: 10.1016/j.urology.2014.07.021. [DOI] [PubMed] [Google Scholar]
- 13.Sestili MA. Possible adverse health effects of vitamin C and ascorbic acid. Semin Oncol. 1983;10:299–304. [PubMed] [Google Scholar]
- 14.Bush MJ, Verlangieri AJ. An acute study on the relative gastro-intestinal absorption of a novel form of calcium ascorbate. Res Commun Chem Pathol Pharmacol. 1987;57:137–140. [PubMed] [Google Scholar]
- 15.Gruenwald J, Graubaum HJ, Busch R, Bentley C. Safety and tolerance of ester-C compared with regular ascorbic acid. Adv Ther. 2006;23:171–178. doi: 10.1007/BF02850358. [DOI] [PubMed] [Google Scholar]
- 16.Ozeki T, Mizuno S, Ohuchi H, Iwaki K, Watanabe S, Ueda H, Kawahara H, Masuda H, Sanefugi H. The effects of prostaglandin E1 on the pepsin activities in gastric mucosa and juice. Br J Exp Pathol. 1987;68:521–526. [PMC free article] [PubMed] [Google Scholar]
- 17.Guldvog I, Berstad A. Opposite effects of H2-receptors on parietal cells and chief cells. Gastric acid and pepsin secretion stimulated by histamine and food combined in dogs: the role of vagal innervation. Eur Surg Res. 1984;16(Suppl 2):55–61. doi: 10.1159/000128622. [DOI] [PubMed] [Google Scholar]
- 18.Sipponen P, Maaroos HI. Chronic gastritis. Scand J Gastroenterol. 2015;50:657–667. doi: 10.3109/00365521.2015.1019918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Katz PO. Lessons learned from intragastric pH monitoring. J Clin Gastroenterol. 2001;33:107–113. doi: 10.1097/00004836-200108000-00003. [DOI] [PubMed] [Google Scholar]
- 20.Heimer KA, Hart AM, Martin LG, Rubio-Wallace S. Examining the evidence for the use of vitamin C in the prophylaxis and treatment of the common cold. J Am Acad Nurse Pract. 2009;21:295–300. doi: 10.1111/j.1745-7599.2009.00409.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vertzoni M, Dressman J, Butler J, Hempenstall J, Reppas C. Simulation of fasting gastric conditions and its importance for the in vivo dissolution of lipophilic compounds. Eur J Pharm Biopharm. 2005;60:413–417. doi: 10.1016/j.ejpb.2005.03.002. [DOI] [PubMed] [Google Scholar]
- 22.McConnell EL, Basit AW, Murdan S. Measurements of rat and mouse gastrointestinal pH, fluid and lymphoid tissue, and implications for in-vivo experiments. J Pharm Pharmacol. 2008;60:63–70. doi: 10.1211/jpp.60.1.0008. [DOI] [PubMed] [Google Scholar]
- 23.Rao CV, Vijayakumar M. Effect of quercetin, flavonoids and alphatocopherol, an antioxidant vitamin, on experimental reflux oesophagitis in rats. Eur J Pharmacol. 2008;589:233–238. doi: 10.1016/j.ejphar.2008.04.062. [DOI] [PubMed] [Google Scholar]
- 24.Sairam K, Rao ChV, Babu MD, Kumar KV, Agrawal VK, K Goel RK. Antiulcerogenic effect of methanolic extract of Emblica officinalis: an experimental study. J Ethnopharmacol. 2002;82:1–9. doi: 10.1016/s0378-8741(02)00041-7. [DOI] [PubMed] [Google Scholar]
- 25.Pancorbo D, Vazquez C, Fletcher MA. Vitamin C-lipid metabolites: uptake and retention and effect on plasma C-reactive protein and oxidized LDL levels in healthy volunteers. Med Sci Monit. 2008;14:CR547–CR551. [PubMed] [Google Scholar]
- 26.Spinola V, Llorent-Martinez EJ, Castilho PC. Determination of vitamin C in foods: current state of method validation. J Chromatogr A. 2014;1369:2–17. doi: 10.1016/j.chroma.2014.09.087. [DOI] [PubMed] [Google Scholar]
- 27.Chatterjee IB, Majumder AK, Nandi BK, Subramanian N. Synthesis and some major functions of vitamin C in animals. Ann N Y Acad Sci. 1975;258:24–47. doi: 10.1111/j.1749-6632.1975.tb29266.x. [DOI] [PubMed] [Google Scholar]
- 28.Levine M, Rumsey SC, Daruwala R, Park JB, Wang Y. Criteria and recommendations for vitamin C intake. JAMA. 1999;281:1415–1423. doi: 10.1001/jama.281.15.1415. [DOI] [PubMed] [Google Scholar]
- 29.Masri OA, Chalhoub JM, Sharara AI. Role of vitamins in gastrointestinal diseases. World J Gastroenterol. 2015;21:5191–5209. doi: 10.3748/wjg.v21.i17.5191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hunt RH. Importance of pH control in the management of GERD. Arch Intern Med. 1999;159:649–657. doi: 10.1001/archinte.159.7.649. [DOI] [PubMed] [Google Scholar]
- 31.Goldberg HI, Dodds WJ, Gee S, Montgomery C, Zboralske FF. Role of acid and pepsin in acute experimental esophagitis. Gastroenterology. 1969;56:223–230. [PubMed] [Google Scholar]
- 32.Kwiecien S, Jasnos K, Magierowski M, Sliwowski Z, Pajdo R, Brzozowski B, Mach T, Wojcik D, Brzozowski T. Lipid peroxidation, reactive oxygen species and antioxidative factors in the pathogenesis of gastric mucosal lesions and mechanism of protection against oxidative stress - induced gastric injury. J Physiol Pharmacol. 2014;65:613–622. [PubMed] [Google Scholar]
- 33.DeMeester TR, Wernly JA, Bryant GH, Little AG, Skinner DB. Clinical and in vitro analysis of determinants of gastroesophageal competence. A study of the principles of antireflux surgery. Am J Surg. 1979;137:39–46. doi: 10.1016/0002-9610(79)90008-4. [DOI] [PubMed] [Google Scholar]
- 34.Rood JC, Ruiz B, Fontham ET, Malcom GT, Hunter FM, Sobhan M, Johnson WD, Correa P. Helicobacter pylori-associated gastritis and the ascorbic acid concentration in gastric juice. Nutr Cancer. 1994;22:65–72. doi: 10.1080/01635589409514332. [DOI] [PubMed] [Google Scholar]
- 35.Wang C, Hunt RH. Precise role of acid in non-erosive reflux disease. Digestion. 2008;78(Suppl 1):31–41. doi: 10.1159/000151253. [DOI] [PubMed] [Google Scholar]