

Abstract
Surgical removal of impacted mandibular third molar is a routine procedure in oral surgery. Various iatrogenic complications related to the procedure has been discussed well in the literatures before. Some of these complications are related to the wrong usage of instruments and techniques. Here we discuss a rare complication on a 42-year-old male, related to the use of high-speed handpiece drill in mandibular third molar removal in a general dental office setting. He was referred when a high speed tungsten carbide bur was accidentally broken and displaced into the mandibular bone during surgical procedure. It is not common to use a high-speed handpiece in impacted third molar removal. This iatrogenic complication could have been totally avoided with the use of proper equipment and technique; therefore raising awareness regarding wrong usage of instrument is vital to avoid similar incidents in the future.
Keywords: oral and maxillofacial surgery, dentistry and oral medicine
Background
This case report highlights a rare complication in a routinely done procedure due to wrong selection of instruments and poor technique. Reporting possible complications from the use of high-speed handpiece drills in mandibular third molar removal can raise awareness among clinicians to avoid similar unnecessary incidents.
Case presentation
A 42-year-old male was referred to our oral and maxillofacial surgery clinic for removal of an embedded fractured bur fragment at right mandibular bone. On initial presentation, he was having right-sided facial swelling together with pain and severe trismus. For the history of presenting complain, his right mandibular third molar was removed earlier that day in a procedure lasting more than 3 hours. He was informed that a fragment from a rotary instrument was left in situ in the wound and could not be removed by the clinician. He was referred to our centre for further management. He brought in some panoramic view radiographs which were taken during the procedure at the clinic. The series of radiographs showed incomplete transverse sectioning of the tooth and attempt by the operator to separate the crown from the roots. This followed by the removal of root fragments first, then followed by removal of the remaining crown segment(figure 1). On the last radiograph, a thin radio opaque material resembling a tip of a bur is seen embedded in the mandibular bone, distal to the tooth 47 (figure 1). Vertically, it was inferior to the apex of tooth 47 and located superior to upper cortical margin of right inferior alveolar canal (figure 2). Clinically, blood clot was seen within the extraction socket and no metal fragment were visible. There was minimal hypoesthesia reported by the patient at right lower lip. He was able to differentiate sharp and blunt stimulation and could do two point discriminations on the affected area. Clinically, the neurosensory deficit was diagnosed as neuropraxia. Sensory function at right lateral border of tongue was normal. A cone beam CT was done to identify the size and exact position of the bur segment in a three-dimensional view. The bur segment was later removed under general anaesthesia on the following day.
Figure 1.
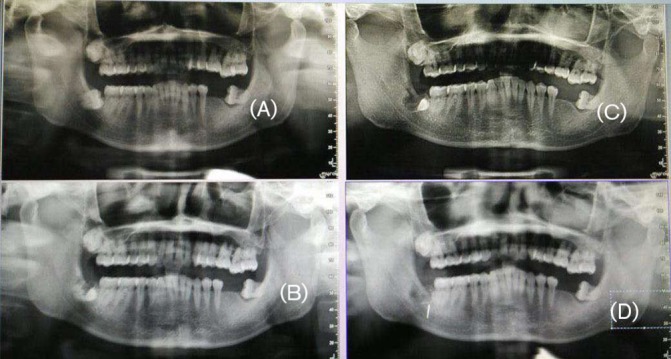
Sequence of panoramic view radiographs showing sectioning of tooth.
Figure 2.

Panoramic view showing displacement of bur segment into mandible.
Investigations
Cone Beam CT was done to get a three-dimensional location of the bur fragment. The bur fragment was found fully embedded in the outer cortex of mandibular bone, lateral to the previously removed crown of tooth 48 (figure 3). In relation to the inferior alveolar canal, the bur was positioned close to the superior cortex of the canal. Size of the bur segment was 9 mm in length.
Figure 3.
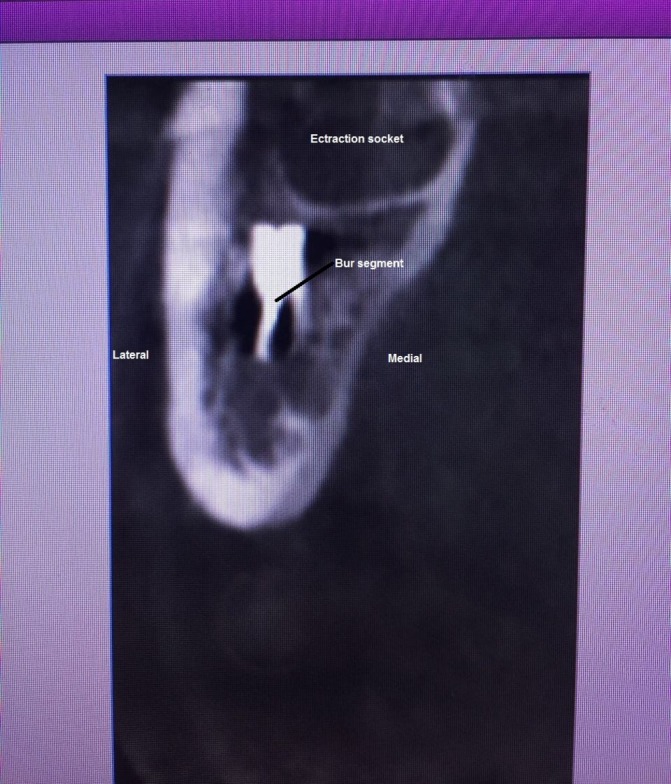
Coronal view of cone beam CT scan showing the position of bur segment in three-dimensional view.
Differential diagnosis
Iatrogenic displacement of high-speed bur to mandibular bone.
Treatment
Removal of fractured displaced bur was done under general anaesthesia. The previous surgical incision was extended to increase the access. The mesial relieving incision which was done at midbuccal of 47, extended inferiorly and anteriorly to the vestibule. The distal relieving incision was extended laterally to the external oblique ridge. Cortical bone lateral to the extraction socket was carefully removed to expose the bur fragment. Once the bur segment was clinically visible, it was secured with an artery forceps and carefully removed. The removed segment was measuring 9 mm (figure 4). Inferior alveolar nerve was not visible after the removal of the bur fragment.
Figure 4.

Removed bur segment.
Outcome and follow-up
Postoperative panoramic view radiograph showed complete removal of the bur fragment (figure 5). The wound healing was good without any infection or tissue breakdown. On postoperative 2 weeks review, the neurosensory disturbance had resolved completely and the patient was discharged from follow-up.
Figure 5.

Postoperative panoramic view showing complete removal of the bur segment.
Discussion
Only one similar case has been published so far in the literature regarding accidental displacement of a high-speed handpiece bur during mandibular third molar surgery.1 In that case, a 20 mm long bur was displaced to the submandibular space during sectioning of the tooth. The bur segment retrieved 3 weeks later via intraoral approach by using a lingual flap. Recovery was uneventful.
Usage of a high-speed handpiece in third molar surgery is not recommended and is not a common practice. High-speed handpiece is a rotary instrument powered by compressed air, rotates at a speed of around 200 000–800 000 rotations per minute. Usually, thin burs made of steel with tungsten carbide or diamond coating are typically used with this handpiece for general dental works. These burs used with high-speed handpiece are comparatively thinner than the burs used with slow-speed handpiece in surgical cases. These thin high-speed burs are not designed to cut hard cortical bone, therefore the risk of fracture is higher when used anappropriately if it is used for bone removal.
Besides the risk of bur fracture, surgical emphysema is another well-documented complication associated with the use of high-speed handpiece in surgical cases.2 3 Subcutaneous emphysema associated with dental extraction usually results from using air-water cooled high-speed dental handpieces, which let the air penetrate the soft tissue through the reflected flap and invade the adjacent tissues.2 It usually invades the spaces around the tooth, but sometimes it may spread along the fascial planes to distant areas. Emphysema usually resolves spontaneously but in severe cases it can cause complications like secondary infection, obstruction of airway, pneumomediastinum and tension pneumothorax.4 In relation to this case, fortunately the patient did not develop any emphysema after the usage of high-speed handpiece.
In the literature, the incidence of inferior alveolar nerve injury following removal of third molars has been reported to be around 0.26%–8.4%5 and most of the injuries are transient. In this case, the nerve injury sustained by the patient can be classified as neuropraxia, or Sunderland first-degree injury, which is a problem caused by conduction blockade following mild compression. Radiographically, there was no direct injury seen but the position of the bur was close to the superior margin of the inferior alveolar canal, which may have caused indirect pressure to the nerve. Once the bur was removed, the neuropraxia resolved and patient regained normal sensation within 2 weeks.
This iatrogenic complication could have been totally avoided with the use of proper equipment and technique. This case emphasizes the importance of avoiding the use of high-speed handpiece drills during minor oral surgery.
Learning points.
High-speed handpiece drills should not be used in surgical cases.
Displacement of bur and surgical emphysema are potential complications from the use of high-speed handpiece drill in surgical removal of impacted third molars.
Slow-speed handpiece with tungsten carbide surgical burs are recommended for impacted third molar removal and osteotomy cases.
Footnotes
Handling editor: Seema Biswas
Contributors: The case was managed by JRR under the supervision of MNAJ and RKR. All the authors contributed equally in the thought process and writing of this paper.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Yalcin S, Aktas I, Emes Y, et al. Accidental displacement of a high-speed handpiece bur during mandibular third molar surgery: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e29–e31. 10.1016/j.tripleo.2007.09.017 [DOI] [PubMed] [Google Scholar]
- 2.Olate S, Assis A, Freire S, et al. Facial and cervical emphysema after oral surgery: a rare case. Int J Clin Exp Med 2013;6:840–4. [PMC free article] [PubMed] [Google Scholar]
- 3.Wong C, Collin J, Hughes C, et al. Surgical emphysema and pneumomediastinum after coronectomy. Br J Oral Maxillofac Surg 2015;53:763–4. 10.1016/j.bjoms.2015.05.008 [DOI] [PubMed] [Google Scholar]
- 4.Ali A, Cunliffe DR, Watt-Smith SR. Surgical emphysema and pneumomediastinum complicating dental extraction. Br Dent J 2000188:589–90. 10.1038/sj.bdj.4800547a [DOI] [PubMed] [Google Scholar]
- 5.Leung YY, Fung PP, Cheung LK. Treatment modalities of neurosensory deficit after lower third molar surgery: a systematic review. J Oral Maxillofac Surg 2012;70:768–78. 10.1016/j.joms.2011.08.032 [DOI] [PubMed] [Google Scholar]