

Abstract
Objectives:
The objective was to evaluate the effects of virtual reality versus conventional physiotherapy on upper extremity function in children with obstetric brachial plexus injury.
Methods:
Forty children with Erb’s palsy were selected for this randomized controlled study. They were assigned randomly to either group A (conventional physiotherapy program) or group B (virtual reality program using Armeo® spring for 45 min three times/week for 12 successive weeks). Mallet system scores for shoulder function and shoulder abduction, and external rotation range of motion (ROM) were obtained; shoulder abductor, and external rotators isometric strength were evaluated pre-and post-treatment using Mallet scoring system, standard universal goniometer, and handheld dynamometer.
Results:
The results of this study indicate that the children in both groups showed improvement in shoulder functions post-treatment with greater improvements in group B. The abduction muscle strength after treatment was 8.53 and 11.3 Nm for group A and group B, respectively. The external rotation muscle strength after treatment was 5.88 and 7.45 Nm for group A and group B, respectively.
Conclusions:
The virtual reality program is a significantly more effective than conventional physiotherapy program in improving the upper extremity functions in children with obstetric brachial plexus injury.
Keywords: Obstetric Brachial Plexus Injury, Virtual Reality, Conventional Physiotherapy, Upper Extremity Function
Introduction
Obstetric brachial plexus injury (OBPI) is a flaccid paralysis of the arm at birth, resulting from a complicated delivery. It is caused by injury to the nerves from the cervical roots C5 to T1. The prevalence of OBPI has been reported to be 1.6 to 5.1 per 1000 live births in population-based studies[1,2].
Motor disorders and loss of functional movements are common consequences of OBPI[3], related to muscle contractures, impairment movements, and motor weakness following brachial plexus damage and compromising quality of life. Many rehabilitation programs for the upper extremity in children with OBPI have been proposed, not only to increase the active range of movement of involved limb but also to improve the functional recovery[4].
Yang et al.[5], provide further support for neural plasticity (the general ability of the brain to reorganize neural pathways based on new experiences) in children with OBPI by investigating limb preference - because the majority of the population prefers to use the right upper limb, a shift to left upper limb preference by the majority of the children would be consistent with plastic adaptation of neural pathways to perinatal deafferentation injury. Recent evidence suggests that many children with neurological disabilities may improve motor performance if provided with sufficient opportunities to practice[6,7].
Obstetric brachial plexus injury has important repercussion for the child as structural deficits that interfere with the use of the upper extremity can result in limitations to the performance of activities of daily living and restrict participation of the child at school and community[8].
Management of OBPI includes both conservative and surgical interventions. Optimal rehabilitation of OBPP requires a multidisciplinary team of specialists including a pediatrician, an expert physical therapist, a pediatric surgeon, an orthopedic surgeon, an electro physiologist, an occupational therapist and a psychosocial therapist. In all cases of OBPI, initial management is conservative. The goals of therapy include maintaining a passive range of motion, supple joints and muscle strengthening; specific therapy includes stretching potentially contracting muscle groups[9]. Nevertheless, the available literature regarding the functional rehabilitation of children with OBPI is remarkably scarce[10].
Virtual Reality (VR) may have something to offer in that it allows individuals to interact and train with or within interesting and relatively realistic three-dimensional (3D) environments[11]. VR and its simulated environments are already well accepted in the guise of entertainment and computer games applications. However, what is not as well recognized is that VR offers the opportunity for intensive repetition of meaningful task-related activities (such as reaching for a utensil in a kitchen environment) necessary for effective rehabilitation[12-16], in a manner that can be more interesting and conducive to self-direction than conventional therapy[17].
Virtual reality as an intervention for motor rehabilitation is a promising tool[18], in order to improve upper limb function in children with neurological impairment. VR systems offer the capability to achieve rehabilitative goals through the use of real-time feedback and adaptive strategy with varying degrees of difficulty. Using attractive, game-like environments, VR is a motivating and entertaining way to engage children in the therapy[19], while providing an opportunity for practice and repetition of movements[20]. However, no studies to date have focused on the effects of VR on the upper extremity function in children with OBPI. Therefore, the aim of this study was to evaluate the clinical effectiveness of VR versus conventional therapy on the upper extremity functional movements in children with OBPI.
Materials and methods
This randomized controlled study was approved by the ethical committee of the Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia. Parents signed a consent form for their children’s participation in this study.
Participants
Forty children with OBPI, with ages ranged from five to eight years from both sexes, participated in this study. To avoid a type II error, a preliminary power analysis (power= 0.8, α=0.05, effect size=0.5) determined a sample size of 40 for this study. They were recruited from the Maternity and Children Hospital, Makkah, Saudi Arabia. The participated children should have a confirmed diagnosis of OBPI in the form of Erb’s type (C5, C6) injuries obtained from medical records. The degree of nerve severance was within the second and third degrees of injury, according to Sunderland classification of nerve injuries[21]. Children were cognitively competent and able to understand and follow instructions. They were medically free with no serious medical complications. There were no fixed contractures or stiffness in the shoulder, elbow, wrist and finger joints and no major rotational mal-alignments in their upper limbs. Children were excluded from the study if they had visual problems that would prevent them from performing the intervention, uncontrolled seizures, shoulder subluxation or dislocation, and fixed contractures or stiffness in the affected upper extremity that would limit activity engagement.
Randomization
Forty eight children were approached for participation in the study. Five children failed to meet the inclusion criteria, and the parents of three children refused to participate in this study. The recruitment process and the flow of participants throughout the study are illustrated in Figure 1. Children were assigned randomly into two groups of equal numbers by using the sealed envelopes. The therapist prepared the sealed envelopes, which contained a piece of paper indicating whether each child was in group A (conventional physiotherapy program) or group B (virtual reality program). Assignment performed before the initial assessment by blinded person who asked to pick up one sealed envelope that contained numbers of participating children.
Figure 1.

Flow diagram of the study.
Outcomes
Mallet scoring system
All children were evaluated pre-treatment and after 12 successive weeks of treatment by evaluating video recordings of standardized movements of the Mallet System to index active shoulder movements. It is a reliable method for evaluating children with OBPI based on the ability to perform functional positioning of the affected limb[22]. This scale assesses the function of the shoulder, and it is based on five criteria: The ability to actively abduct the arm, the ability to externally rotate the arm, the ability to place the hand behind the neck as well as behind the back or spine, and the ability to place the hand over the mouth. A total Mallet score is calculated from the scores gained in the performance of the former tasks with a grading scale of I to V giving a maximum score of 25[23]. Mallet scoring system was considered the primary outcome of this study.
Shoulder ROM
Shoulder abduction active range of motion (ROM) was measured using the standard universal goniometer. Measurement procedures performed while the child in sitting position, with fixing the trunk to prevent the compensatory movements. The arm was actively elevated in the strict coronal plane with the thumb pointed up toward the ceiling to allow the required external rotation necessary to avoid impingement of the greater tuberosity on the acromion process. Once the active end range was achieved the measurements were documented[24].
External rotation active ROM was measured in the supine position with the hips and knees flexed to approximately 45°. The tested arm was supported on the table in 90° of abduction, elbow flexed to 90°, and the wrist in neutral position. A towel roll was placed under the humerus to ensure neutral horizontal positioning; which required the humerus to be in level to the acromion process based on visual inspection. Once positioned, the child was asked to rotate his arm back into external rotation to his end available range without discomfort. The child was instructed not to lift his lower back during this measurement. Once active end-range was achieved the measurement was recorded[25].
Shoulder muscle strength
Shoulder abductors and external rotators strength were measured using a handheld dynamometer (HHD), which allows for a relatively quick measurement of isometric strength in various positions. Shoulder abduction strength was measured from supine position with the shoulder in 0° flexion, 0° abduction, and neutral rotation while the elbow in extension and the hand facing down. HHD located above the lateral epicondyles of the elbow and the child asked to push the arm laterally. Shoulder external rotation strength was measured from supine position with the shoulder in 0° flexion, 0° abduction, and neutral rotation while the elbow in flexion 90° and the hand facing medially. HHD located above the wrist and the child asked to push the arm laterally then measurement was recorded[26,27].
Interventions
Conventional physical therapy program
Group A received the conventional physiotherapy program, which aimed to improve arm function and shoulder abduction and external rotation. It includes a range of functional, daily living and play activities similar to those they usually practice in any given day of their life to maintain the child’s interest and attention[28].
The conventional program consisted of: (1) weight-bearing exercises for 10 min: shifting body weight on a fully extended and externally rotated upper extremity from sitting, weight bearing on an extended arm from quadruped position and push up from prone; (2) joint approximation technique: manually applied compression force to wrist, elbow, and shoulder of the affected side in rapid, jerky and dysrythmic manner from a comfortable sitting position; (3) proprioceptive neuromuscular facilitation: reinforcement of weak muscles through overflow of neural excitation from strong muscles acting in the same pattern. Flexion, adduction, external rotation pattern and flexion, abduction, and external rotation pattern were used; (4) scapulothoracic mobilization; from side lying with the affected side in the uppermost, cephalocaudal, and mediolateral gliding of the scapula was performed; (5) strengthening exercises with graduated manual resistance for shoulder abductors and external rotators; (6) facilitation of arm-hand exercises include; throw ball toward target from standing position either above or below the head level, bouncing ball from standing position and catch ball from standing position, either catching ball thrown from different directions or catching bounced ball; (7) stretching of tight muscles: internal rotators of the shoulder (subscapularis), pronators of the forearm, and flexors of the wrist and fingers were stretched for 20 seconds then released for 20 seconds with 5 repetitions each session. Each exercise other than weight-bearing and stretching exercises was conducted for approximately 5 min with a total treatment time of 45 min three times/week for 12 successive weeks
Virtual reality program
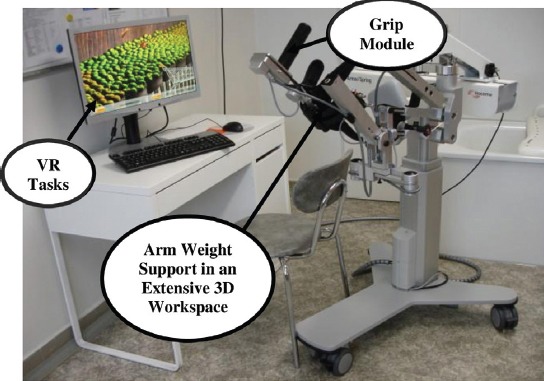
Group B received practice in a virtual environment by using Armeo® spring Pediatric (Hocoma, AG, Switzerland). The Armeo® spring is a novel tool that combines robotic assistance and virtual reality to provide a new, unique way to engage children in the required repetitive motions required for motor learning. This exoskeleton device provides an engaging environment to achieve the required repetitive practice the upper extremity needs for improved function. There is great adjustability to the Armeo® spring, allowing the therapist to customize the device to the needs of the individual child. Armeo® equipment is based on the product “T-WREX”. This product is a passive upper limb orthosis, which lightens the weight of the upper limb in 3D space using an ergonomic and adjustable backrest upper limb (antigravity effect) and allows natural movement in the workspace (Figure 2). This makes it easier for users with moderate to severe disabilities to achieve greater range of motion[29].
Figure 2.
Armeo® Spring System.
Armeo® system has five different degrees of freedom; shoulder flexion/extension, shoulder abduction/adduction, elbow flexion and extension, forearm pronation/supination and grip strength. The therapist can choose to lock out different motions or work on all motions at the same time depending on the needs of the individual child. In addition, adjustments can be made to the amount of gravity assistance the exoskeleton provides depending on the strength of the upper extremity. Several virtual reality games for each desired range of motion are available for the child to choose[30].
The therapist adjusts the electric lifting column according the child height during sitting and the length of the orthosis for upper arm and forearm to avoid compensatory movement and to set the three dimension workspace with adjusting the amount of weight support, after introducing the child data to the device the therapist select the children appropriate program according to difficulty level, the computer used sense the joint angle to give visual movement feedback and track the therapy process. Children practiced the VR program for 45 min three times/week for 12 successive weeks. This provided the high level of repetition required to promote change in the upper extremity[31,32].
Statistical analysis
Data analysis was performed using SPSS software (version 16.0, Chicago, IL). Descriptive statistics including mean and standard deviation were calculated for all variables at baseline and after 12-weeks of interventions. Data of shoulder functions measured by the Mallet scoring system were statistically analyzed by nonparametric statistical procedures, including Wilcoxon and Mann-Whitney tests. While the data of shoulder ROM and strength was statistically analyzed using an unpaired t-test. The level of significance for all statistical tests was set at P<0.05.
Results
Forty children with Erb’s palsy (27 males and 13 females) were included in this study. The children were randomly assigned to one of two equal-sized groups (A & B) (n=20 each). The demographic and clinical characteristics of the children were similar in both groups (Table 1).
Table 1.
Demographic and clinical characteristics of the participating children at baseline.
| Item | Group A (n= 20) | Group B (n= 20) | T-Value | P-Value | |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| Age (Years) | 6.6±1.05 | 6.35±0.93 | 0.79 | 0.43* | |
| Weight (Kg) | 22.2±1.51 | 21.65±1.76 | 1.06 | 0.29* | |
| Height (Cm) | 119.41±5.41 | 116.95±5.62 | 1.18 | 0.25* | |
| Sex | Male | 14 | 13 | 67.5℅ | |
| Female | 6 | 7 | 32.5℅ | ||
| Affected Side | Right | 13 | 12 | 62.5℅ | |
| Left | 7 | 8 | 37.5℅ | ||
Level of significance at P<0.05;
Nonsignificant; SD: standard deviation.
Before treatment, there were no significant differences in the mean values of Mallet scores for the shoulder function in both groups (Table 2). In contrast, there was a significant difference between the mean values of Mallet scores at baseline and after treatment. These findings showed that children in the group B showed distinct improvement in shoulder function when compared with the children in the group A (Table 2).
Table 2.
Mallet system scores pre and post treatment mean values for group A and B.
| Item | Abduction | External rotation | Hand to neck | Hand to spine | Hand to mouth | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Group A | 3.2±0.77 | 4.00±0.46 | 2.65±0.49 | 3.25±0.44 | 2.65±0.49 | 3.25±0.44 | 2.35±0.49 | 3.15±0.59 | 2.40±0.50 | 3.00±0.46 |
| Group B | 3.00±0.56 | 4.35±0.49 | 2.35±0.59 | 4.00±0.65 | 2.45±0.51 | 3.85±0.49 | 2.40±0.50 | 3.90±0.55 | 2.65±0.49 | 4.00±0.73 |
| P-value | 0.31* | 0.29* | 0.98* | <0.001** | 0.21* | <0.001** | 0.75* | <0.001** | 0.12* | <0.001** |
| Effect size | Cohen’s d= 0.74 | Cohen’s d= 1.35 | Cohen’s d= 1.29 | Cohen’s d= 1.31 | Cohen’s d= 1.64 | |||||
Level of significance at P<0.05;
Nonsignificant;
Significant.
At baseline, no significant differences were noted in the mean values of shoulder abduction and external rotation ROM (degrees) between group A and B (Table 3). After treatment, a significant difference was observed when comparing the post-treatment results of the two groups in favor of group B (Table 3).
Table 3.
Pre and post treatment mean values of abduction and external rotation range of motion (degrees) for group A and B.
| Item | Abduction ROM | External rotation ROM | ||
|---|---|---|---|---|
| Pre-treatment | Post-treatment | Pre-treatment | Post-treatment | |
| Group A | 70.1±4.24 | 88.1±4.11 | 34.75±2.61 | 48±3.71 |
| Group B | 71.25±2.88 | 110.8±6. 00 | 35.55±2.11 | 62.4±4.84 |
| P-Value | 0.32* | <0.001** | 0.29* | <0.001** |
| Effect size | Cohen’s d= 4.41 | Cohen’s d= 3.34 | ||
Level of significance at P<0.05;
Nonsignificant;
Significant.
No significant difference was noted in the mean values of shoulder muscle strength (Nm) at baseline between group A and B (Table 4). There was a significant difference between the mean values of shoulder muscle strength (Nm) obtained during the baseline and after treatment in both groups. These results indicated that the children in both groups showed distinct improvement in shoulder muscle strength post-treatment in favor of the group B (Table 4).
Table 4.
Pre and post treatment mean values of abduction and external rotation isometric strength (Nm) for group A and B.
| Item | Abduction muscle strength | External rotation muscle strength | ||
|---|---|---|---|---|
| Pre-treatment | Post-treatment | Pre-treatment | Post-treatment | |
| Group A | 6.49±0.51 | 8.53±0.68 | 4.23±0.57 | 5.88±0.48 |
| Group B | 6.68±0.89 | 11.3±1.08 | 4.4±0.64 | 7.45±0.81 |
| P-Value | 0.41* | <0.001** | 0.37* | <0.001** |
| Effect size | Cohen’s d= 3.06 | Cohen’s d= 2.35 | ||
Level of significance at P<0.05;
Nonsignificant;
Significant.
Discussion
This study compared the effects of virtual reality and conventional therapy on upper extremity function in children with OBPI. The findings of the present study demonstrated that children of group B (virtual reality program), showed greater improvement in the Mallet scores, ROM, and strength of the affected upper extremity than children in group A (conventional physiotherapy program).
Based on the above, results from studies comparing VR with conventional therapy, given the same type and intensity of exercises, are inconclusive[33-35]. According to some authors, benefits from VR are at least as effective as those from conventional therapy regimens. Other authors affirm that VR systems deliver better results than conventional therapy. For example, Lum et al.[36], compared a control group treated with conventional therapy to a group treated with VR. They concluded that the latter presented better clinical results and biomechanical measurements. Other authors believe that VR training combined with conventional therapy is probably better than either regimen by itself, for both kinematic and function[37]. The preference for VR systems over conventional therapies is probably based on the uniformity, velocity, and intensity of the VR exercises[33].
In group B, the association with different virtual realities provides the tasks with functional significance and increased visual feedback. The Armeo® system allows the therapist to adjust the level of difficulty to match the child’s condition, which is also a relevant concern in motor learning strategies. On the other hand, it is interesting to note that the most frequently repeated tasks with the Armeo® system are reaching/grasping tasks[38]. These movements are commonly used in activities of daily life, and interjoint arm coordination needed to complete this task is often impaired in children with OBPI.
Intense motor activity can re-establish and reinforce neuronal pathways and enhance neuronal plasticity in children with congenital or acquired motor deficits, caused disorders of the central or peripheral nervous system. Besides intensive motor training, another requirement for successful rehabilitation is a goal-oriented and task-specific training program[39]. Motor function in children with motor dysfunction can be improved using targeted functional training. Variations in repeated movements and enriched environments play an important role in affecting child motivation and thus the intensity and efficacy of training[40,41].
Use of virtual environment in this study allowed manipulation of all exercise characteristics such as duration, intensity, and type of feedback based on treatment aims and individual ability. Therefore, children can perform activities and tasks repeatedly and with increased motivation, and in addition, therapists can also monitor the results of their movements, and if inappropriate, correct them[42].
Practice in virtual environment produces active participation instead of passive practice during the training[42], which is recommended for motor learning and cortical reorganization. Passive exercises have been shown not to enable maximum improvement in the affected upper extremity in children with OBPI. It is also necessary to provide and strengthen new motor skills, provide functional and duty- focused practices and increase motivation for learning and recovery after a lesion. Although motor learning is quite different in children with OBPI compared to patients with stroke and spinal cord injury, focusing on the activity and task is one of the most important aspects of the treatment in children[43,44].
The major goal of rehabilitation of children with OBPI in this study is to restore the basic functional abilities of their arms. Recovery after neural damage usually depends on various factors such as the nature and amount of the rehabilitation. Conventional rehabilitation programs are shorter and less intensive to ensure optimal therapeutic results. They cannot adequately increase the motivation of the child or support activity participation[45].
Immediate augmented feedback in virtual environment makes the learning easier through eliminating time lags between children and therapist[46]. During this study intervention, Sensorimotor, visual, and auditory feedbacks were presented concurrently with the performance of exercises, or after the end of practice period.
The findings of this study are consistent with previous studies[42,47], that used a virtual reality intervention to improve upper-extremity control in children with cerebral palsy (CP). These studies showed positive effects of practice in a virtual environment on upper limb functions of children with CP.
The results of this study agree with previous studies[48,49], used robot assisted upper extremity therapy in adult stroke patients and in children with CP. They have proven that, the robot assisted upper extremity therapy was effective due to the patient’s active involvement is a factor with its effectiveness. However, this demands focused attention during training sessions, which can be a challenge for children.
Another important aspect of the VR training was, the virtual environments can provide an opportunity to practice and learn without the fear of losing or injury, which can result in a sense of personal control or self-efficacy. Sense of control and efficacy in activities may enhance motivation in children[50]. There was no evidence that the level of compliance with study protocol affected study outcomes.
There are some limitations of this study, one of them is the literature does not provide conclusive data about whether VR intervention in children with OBPI is superior to other rehabilitation therapies. This is the first study to use a VR intervention in OBPI. This lack of data limited the ability of the researcher to compare among different virtual reality protocols and used only studies done on children with CP and stroke. The lack of follow-up for several months post-treatment to evaluate the long-lasting effects of virtual reality interventions might be considered another limitation of this study. Therefore, future studies with a long-term follow-up are warranted.
Therefore, we can conclude that the virtual reality program is a significantly more effective than conventional physiotherapy program in improving the upper extremity functions in children with OBPI.
Acknowledgement
The author would like to express his appreciation to the participating children and their parents to make this study possible.
Footnotes
The authors have no conflict of interest.
Edited by: F. Rauch
References
- 1.Andersen J, Watt J, Olson J, Van Aerde J. Perinatal brachial plexus palsy. Pediatr Child Health. 2006;11:93–100. doi: 10.1093/pch/11.2.93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hoeksma AF, ter Steeg AM, Nelissen RG, van Ouwerkerk WJ, Lankhorst GJ, de Jong BA. Neurological recovery in obstetric brachial plexus injuries: an historical cohort study. Dev Med Child Neurol. 2004;46(2):76–83. doi: 10.1017/s0012162204000179. [DOI] [PubMed] [Google Scholar]
- 3.Zafeiriou DI, Psychogiou K. Obstetrical brachial plexus palsy. Pediatr Neurol. 2008;38:235–242. doi: 10.1016/j.pediatrneurol.2007.09.013. [DOI] [PubMed] [Google Scholar]
- 4.Santamato A, Panza F, Ranieri M, Fiore P. Effect of botulinum toxin type A and modified constraint-induced movement therapy on motor function of upper limb in children with obstetrical brachial plexus palsy. Childs Nerv Syst. 2011;12(27):2187–2192. doi: 10.1007/s00381-011-1609-4. [DOI] [PubMed] [Google Scholar]
- 5.Yang LJ, Anand P, Birch R. Limb preference in children with obstetric brachial plexus palsy. Pediatr Neurol. 2005;33(1):46–49. doi: 10.1016/j.pediatrneurol.2005.01.011. [DOI] [PubMed] [Google Scholar]
- 6.Duff SV, Gordon AM. Learning of grasp control in children with hemiplegic cerebral palsy. Dev Med Child Neurol. 2003;45(11):746–757. doi: 10.1017/s0012162203001397. [DOI] [PubMed] [Google Scholar]
- 7.Shumway-Cook A, Hutchinson S, Kartin D, Price R, Woollacott M. Effect of balance training on recovery of stability in children with cerebral palsy. Dev Med Child Neurol. 2003;45(9):591–602. doi: 10.1017/s0012162203001099. [DOI] [PubMed] [Google Scholar]
- 8.Strömbeck C, Krumlinde-Sundholm L, Remahl S, Sejersen T. Long-term follow-up of children with obstetric brachial plexus palsy I: functional aspects. Dev Med Child Neurol. 2007;49:198–203. doi: 10.1111/j.1469-8749.2007.00198.x. [DOI] [PubMed] [Google Scholar]
- 9.Dodds SD, Wolfe SW. Perinatal brachial plexus palsy. Curr Opin Pediatr. 2000;12(1):40–47. doi: 10.1097/00008480-200002000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Vaz DV, Mancini MC, do Amaral MF, de Brito Brandão M, de França Drummond A, da Fonseca ST. Clinical changes during an intervention based on constraint-induced movement therapy principles on use of the affected arm of a child with obstetric brachial plexus injury: a case report. Occup Ther Int. 2010;17(4):159–167. doi: 10.1002/oti.295. [DOI] [PubMed] [Google Scholar]
- 11.Sisto SA, Forrest GF, Glendinning D. Virtual reality applications for motor rehabilitation after stroke. Top Stroke Rehabil. 2002;8(4):11–23. doi: 10.1310/YABD-14KA-159P-MN6F. [DOI] [PubMed] [Google Scholar]
- 12.Nelles G, Jentzen W, Jueptner M, Müller S, Diener HC. Arm training induced plasticity in stroke studied with serial positron emission tomography. Neuroimage. 2001;13:1146–1154. doi: 10.1006/nimg.2001.0757. [DOI] [PubMed] [Google Scholar]
- 13.Small S, Solodkin A. Review: The neurobiology of stroke rehabilitation. Neuroscientist. 1998;4:426–434. [Google Scholar]
- 14.Liepert J, Bauder H, Wolfgang HR, Miltner WH, Taub E, Weiller C. Treatment-induced cortical reorganization after stroke in humans. Stroke. 2000;31(6):1210–1216. doi: 10.1161/01.str.31.6.1210. [DOI] [PubMed] [Google Scholar]
- 15.Broeren J, Bjorkdahl A, Pascher R, Rydmark M. Virtual reality and haptics as an assessment device in the post acute phase after stroke. Cyber Psychol Behav. 2002;25:207–211. doi: 10.1089/109493102760147196. [DOI] [PubMed] [Google Scholar]
- 16.Cramer S C, Bastings E P. Mapping clinically relevant plasticity after stroke. Neuropharmacology. 2000;39:842–851. doi: 10.1016/s0028-3908(99)00258-0. [DOI] [PubMed] [Google Scholar]
- 17.Crosbie JH, Lennon S, Basford JR, McDonough SM. Virtual reality in stroke rehabilitation: Still more virtual than real. Disabil Rehabil. 2007;29(14):1139–1146. doi: 10.1080/09638280600960909. [DOI] [PubMed] [Google Scholar]
- 18.Galvin J, McDonald R, Catroppa C, Anderson V. Does intervention using virutal reality improve upper limb function in children with neurological impairment: A systematic review of the evidence. Brain injury. 2011;25(5):435–442. doi: 10.3109/02699052.2011.558047. [DOI] [PubMed] [Google Scholar]
- 19.Snider L, Majnemer A, Darsaklis V. Virtual reality as a therapeutic modality for children with cerebral palsy. Dev Neurorehabil. 2010;13(2):120–128. doi: 10.3109/17518420903357753. [DOI] [PubMed] [Google Scholar]
- 20.Dinomais M, Veaux F, Yamaguchi T, Richard P, Richard I, Nguyen S. A new virtual reality tool for unilateral cerebral palsy rehabilitation: two single-case studies. Dev Neurorehabil. 2013;16(6):418–422. doi: 10.3109/17518423.2013.778347. [DOI] [PubMed] [Google Scholar]
- 21.Sunderland SA. Classification of peripheral nerve injuries producing loss of function. Brain. 1951;74:491–516. doi: 10.1093/brain/74.4.491. [DOI] [PubMed] [Google Scholar]
- 22.Bae DS, Waters PM, Zurakowski D. Reliability of three classification systems measuring active motion in brachial plexus birth palsy. J Bone Joint Surg Am. 2003;85-a(9):1733–1738. doi: 10.2106/00004623-200309000-00012. [DOI] [PubMed] [Google Scholar]
- 23.de Luna Cabrai JR, Crepaldi BE, de Sambuy MTC, da Costa AC, Abdouni YA, Chakkour I. Evaluation of upper-limb function in patients with obstetric palsy after modified Sever-L'Episcopo procedure. Rev Bras Ortop. 2012;47(4):451–454. doi: 10.1016/S2255-4971(15)30127-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Levangie PK, Norkin CC. Joint structure and function: A Comprehensive Analysis. 5th Edition. Philadelphia, PA: F.A. Davis Company; 2011. [Google Scholar]
- 25.Kilber MJ, Hanney WJ. The Reliability and concurrent validity of shoulder mobility measurements using a digital inclinometer and goniometer. A technical report. Ant J Sports Phys Ther. 2012;7(3):306–313. [PMC free article] [PubMed] [Google Scholar]
- 26.Brochard S, Alter K, Damiano D. Shoulder strength profiles in children with and without brachial plexus palsy. Muscle Nerve. 2014;50(1):60–66. doi: 10.1002/mus.24099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hébert LJ, Maltais DB, Lepage C, Saulnier J, Crête M. Hand-Held Dynamometry Isometric Torque Reference Values for Children and Adolescents. Pediatr Phys Ther. 2015;27(4):414–423. doi: 10.1097/PEP.0000000000000179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ibrahim AI, Hawamdeh ZM, Alsharif AA. Evaluation of bone mineral density in children with perinatal brachial plexus palsy: effectiveness of weight bearing and traditional exercises. Bone. 2011;49:499–505. doi: 10.1016/j.bone.2011.05.015. [DOI] [PubMed] [Google Scholar]
- 29.HOCOMA. Armeo®user manual [CD-ROM] Hocoma AG: 2008. [Google Scholar]
- 30.Klobucka S, Kralovicova M, Ziakova E. A functionally robot-assisted therapy upper limb. Rehabilitation and Physical Medicine. 2010;17:164–168. [Google Scholar]
- 31.Sladekova N, Kresanek J. Case report of a patient with cerebral palsy using non-robotic equipment for re-education movements of paretic upper limb. Prz Med Uniw Rzesz Inst Leków. 2014;1:115–118. [Google Scholar]
- 32.Padyšaková H, Repková A, Sládeková N, Žiaková E, Pacek O, Musilová E, Klobucka S. Re-Education Movements of the Paretic Upper Extremity in Children age by Using Non-robotic Equipment. European Journal of Medicine. 2015;8(2):106–114. [Google Scholar]
- 33.Kahn LE, Zygman ML, Rymer WZ, Reinkensmeyer DJ. Robot assisted reaching exercise promotes arm movement recovery in chronic hemiparetic stroke: a randomized controlled pilot study. J Neuroeng Rehabil. 2006;3:12. doi: 10.1186/1743-0003-3-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lo AC, Guarino PD, Richards LG, Haselkorn JK, Wittenberg GF, Federman DG, et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N Engl J Med. 2010;362:1772–1783. doi: 10.1056/NEJMoa0911341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lum PS, Burgar CG, Van der Loos M, Shor PC, Majmundar M, Yap R. MIME robotic device for upper-limb neurorehabilitation in subacute stroke subjects: a follow-up study. J Rehabil Res Dev. 2006;43:631–642. doi: 10.1682/jrrd.2005.02.0044. [DOI] [PubMed] [Google Scholar]
- 36.Lum PS, Burgar CG, Shor PC, Majmundar M, Van der Loos M. Robot-assisted movement training compared with conventional therapy techniques for the rehabilitation of upper-limb motor function after stroke. Arch Phys Med Rehabil. 2002;83:952–959. doi: 10.1053/apmr.2001.33101. [DOI] [PubMed] [Google Scholar]
- 37.Fasoli SE, Krebs HI, Hogan N. Robotic technology and stroke rehabilitation: translating research into practice. Top Stroke Rehabil. 2004;11(4):11–9. doi: 10.1310/G8XB-VM23-1TK7-PWQU. [DOI] [PubMed] [Google Scholar]
- 38.Brokaw EB, Murray T, Nef T, Lum PS. Retraining of interjoint arm coordination after stroke using robot-assisted time-independent functional training. J Rehabil Res Dev. 2011;48:299–316. doi: 10.1682/jrrd.2010.04.0064. [DOI] [PubMed] [Google Scholar]
- 39.Damiano DL. Activity, activity, activity: Rethinking our physical therapy approach to cerebral palsy. Phys Ther. 2006;86:1534–1540. doi: 10.2522/ptj.20050397. [DOI] [PubMed] [Google Scholar]
- 40.Ketelaar M, Vermeer A, Hart H, van Petegem-van Beek E, Helders PJ. Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys Ther. 2001;81:1534–1545. doi: 10.1093/ptj/81.9.1534. [DOI] [PubMed] [Google Scholar]
- 41.Magill R, Anderson R. Motor Learning and Control: Concepts and Applications. 10th Edition. North Ryde: NSW McGraw-Hill; 2014. [Google Scholar]
- 42.You SH, Jang SH, Kim YH, Kwon YH, Barrow I, Hallett M. Cortical reorganization induced by virtual reality therapy in a child with hemiparetic cerebral palsy. Dev Med Child Neurol. 2005;47:628–635. [PubMed] [Google Scholar]
- 43.Lotze M, Braun C, Birbaumer N, Anders S, Cohen LG. Motor learning elicited by voluntary drive. Brain. 2003;126(4):866–872. doi: 10.1093/brain/awg079. [DOI] [PubMed] [Google Scholar]
- 44.Papavasiliou AS. Management of motor problems in cerebral palsy: a critical update for the clinician. European journal of pediatric neurology. 2009;13(5):387–396. doi: 10.1016/j.ejpn.2008.07.009. [DOI] [PubMed] [Google Scholar]
- 45.Brutsch K, Schuler T, Koenig A, Zimmerli L, Koeneke SM, Lunenburger L, et al. Influence of virtual reality soccer game on walking performance in robotic assisted gait training for children. Journal of Neuroengineering and Rehabilitation. 2010;7:15. doi: 10.1186/1743-0003-7-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Brooks BM. Route Learning in a Case of Amnesia: A Preliminary Investigation into the Efficacy of Training in a Virtual Environment. Neuropsychol Rehabil. 1999;9(1):63–76. [Google Scholar]
- 47.Chen YP, Kang LJ, Chuang TY, Doong JL, Lee SJ, Tsai MW, Jeng SF, Sung WH. Use of virtual reality to improve upper-extremity control in children with cerebral palsy: a single-subject design. Phys Ther. 2007;87:1441–1457. doi: 10.2522/ptj.20060062. [DOI] [PubMed] [Google Scholar]
- 48.Kwakkel G, Kollen BJ, Krebs HI. Effects of robot-assisted therapy on upper limb recovery after stroke: a systematic review. Neurorehabil Neural Repair. 2008;22(2):111–121. doi: 10.1177/1545968307305457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ladenheim B, Altenburger P, Cardinal R, Monterroso L, Dierks T, Mast J, Krebs HI. The effect of random or sequential presentation of targets during robot-assisted therapy on children. NeuroRehabil. 2013;33(1):25–31. doi: 10.3233/NRE-130924. [DOI] [PubMed] [Google Scholar]
- 50.Reid DT. Benefits of a virtual play rehabilitation environment for children with cerebral palsy on perceptions of self-efficacy: a pilot study. Pediatr Rehabil. 2002;5(3):141–148. doi: 10.1080/1363849021000039344. [DOI] [PubMed] [Google Scholar]